
Abstract
Objectives
Human papillomavirus (HPV)-associated cancers account for about 9% of the cancer mortality burden in the United States; however, survival differs among sociodemographic factors. We determine sociodemographic and clinical variables associated with HPV-associated cancer survival.
Methods
Data derived from the Surveillance, Epidemiology, and End Results 18 cancer registry were analyzed for a cohort of adult patients diagnosed with a first primary HPV-associated cancer (anal, cervical, oropharyngeal, penile, vaginal, and vulvar cancers), between 2007 and 2015. Multivariable Fine and Gray proportional hazards regression models stratified by anatomic site estimated the association of sociodemographic and clinical variables and cancer-specific survival.
Results
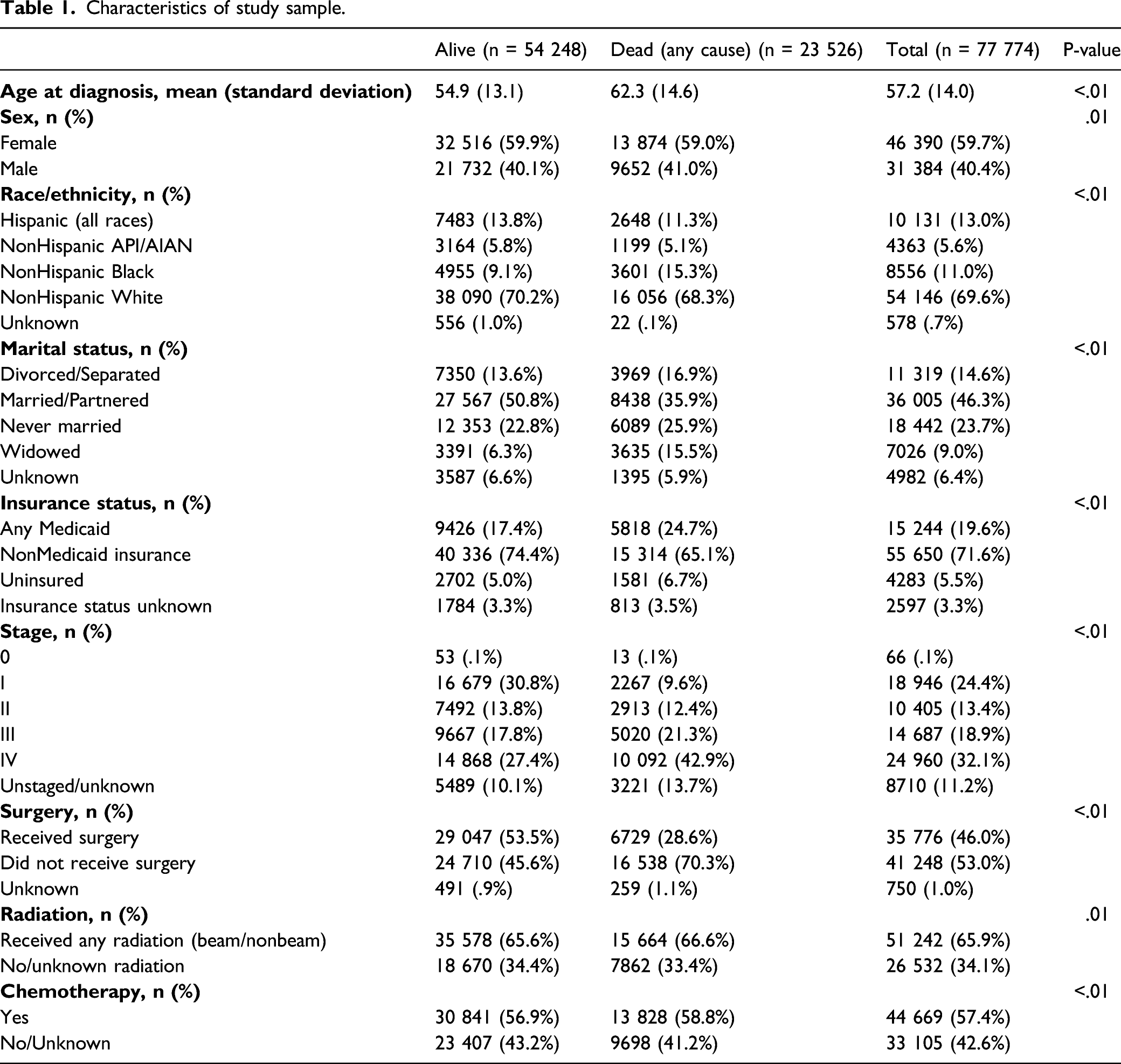
A total of 77 774 adults were included (11 216 anal, 27 098 cervical, 30 451 oropharyngeal, 2221 penile, 1176 vaginal, 5612 vulvar; average age = 57.2 years). The most common HPV-associated cancer was cervical carcinoma (58%) for females and oropharyngeal (81%) for male. Among patients diagnosed with anal/rectal squamous cell carcinoma (SCC), males had a higher risk of death than females. NonHispanic (NH) blacks had a higher risk of death from anal/rectal SCC, oropharyngeal SCC, and cervical carcinoma; and Hispanics had a higher risk of death from oropharyngeal SCC than NH whites. Marital status was associated with risk of death for all anatomic sites except vulvar. Compared to nonMedicaid insurance, patients with Medicaid and uninsured had higher risk of death from anal/rectal SCC, oropharyngeal SCC, and cervical carcinoma.
Conclusions
There exists gender (anal) and racial and insurance (anal, cervical, and oropharyngeal) disparities in relative survival. Concerted efforts are needed to increase and sustain progress made in HPV vaccine uptake among these specific patient subgroups, to reduce cancer incidence.
Keywords
Introduction
Eighty million individuals in the United States are currently infected with one or more types of the human papillomavirus (HPV), with 14 million new infections occurring each year. 1 Of the more than 150 HPV types, the nonavalent HPV vaccine covers the major oncogenic types (HPV 6, 11, 16, 18, 31, 33, 45, 52, and 58),2-4 which are responsible for most of the 44 000 new cases of HPV-associated cancers in the United States annually. These occur in a range of anatomic sites, including the oropharynx, the cervix, and other anogenital sites. 4 These diseases’ span many medical specialties resulting in research that is often siloed. The incidence of HPV-associated oropharyngeal cancer has dramatically increased, surpassing cervical cancer as the leading HPV-associated cancer in the United States.4,5
HPV-associated cancers account for about 9% of the cancer mortality in the United States; however, survival differs among racial/ethnic groups, 5 and is significantly lower among blacks than whites. 6 Whether significant clinical, biological, or sociodemographic differences underpin these racial differences in survival remains largely inconclusive. Given that eliminating cancer-related racial disparity is a principal objective of the Healthy People 2020 initiative, 7 it is important to understand the clinical/sociodemographic drivers of survival disparity in HPV-associated cancers. 5
The need to further understand correlates of HPV-associated cancer survival has become even more imperative, as data emerge describing the potential of therapeutic (rather than the current preventive) HPV vaccines.8-10 Therapeutic HPV vaccines (when they become available) would likely affect current efforts to reduce if not completely eliminate cervical cancer 11 responsible for over three-quarters of the global burden of HPV-associated cancers. 10 Unfortunately, current HPV-associated cancer literature is predominated by incidence rather than survival, and primarily for cervical or oropharyngeal cancers,6,12-16 creating a paucity of data on survival of the less prevalent HPV-associated cancers, anal, penile, vaginal, and vulvar malignancies. 5
The study aimed to determine sociodemographic variables associated with survival in patients diagnosed with HPV-associated cancers. Findings may identify specific, disparate subpopulations at increased risk of death from HPV-associated cancers.
Methods
Data Source
In 17 this retrospective analysis, we used data from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) 18 program. SEER is a leading source of population-based information on cancer incidence, staging, and survival, 18 and SEER 18 encompass approximately 27.8% of the United States population. 19 Because SEER is a publicly available database containing de-identified patient information, it was deemed exempt by the Saint Louis University Institutional Review Board.
Patient Population
Patients of 18–99 years diagnosed with a malignant first primary microscopically confirmed HPV-associated cancer were identified from SEER 18 between 2007 and 2015. HPV-associated cancer was defined using the National Program of Cancer Registries’ definition. 20 Six sites were defined by International Classification of Diseases-Oncology (ICD-O)-3 code: anal/rectal squamous cell carcinoma (SCC) (primary sites C20.9, C21.0-C21.8; ICD-O-3 histologic types 8050-8084, 8120-8131), cervical carcinoma (primary sites C53.0-C53.9; histologic types 8010-8671, 8940-8941), oropharyngeal SCC (primary sites C01.9, C02.4, C02.8, C05.1, C05.2, C09.0-C09.9, C10.0-C10.9, C14.0-C14.8), penile SCC (primary sites C60.0-C60.9), vaginal SCC (primary site C52.9), and vulvar SCC (primary sites C51.0-C51.9). Patients were excluded if they did not meet any of the previous criteria, if their cancer was only reported on their death certificate/autopsy, or were alive with no survival time. Also, SEER automatically excludes patients older than 99 for consistency with analyses that use expected survival tables, as these tables for ages 100 and older are unstable. 21
Measures and Statistical Analysis
The outcome of interest was death from first primary HPV-associated cancer. SEER provides a cause-specific death classification variable that considers patients’ number of tumors, site of first cancer, and comorbidities to reduce cause of death misclassification. 22 SEER also provides patients’ survival time in months from month of diagnosis to month of last contact. 23 Patients who were lost to follow-up or were alive through the last day of database collection were considered censored. Also, by default, SEER*Stat censors patients when they reach 100 years old for consistency with analyses that incorporate expected survival tables. 21
Sociodemographic variables included in the analyses were sex (female, male), marital status (married/partnered, divorced/separated, never married, unknown, widowed), age at diagnosis (continuous), race/ethnicity (Hispanic (all races), nonHispanic (NH) White, NH Black, NH Asian/Pacific Islander/Native American/Alaska Native (API/AIAN), and insurance type (nonMedicaid insurance; any Medicaid [includes Medicare with Medicaid eligibility]; uninsured; unknown). 24 Clinical factors included anatomic site, stage (I, II, III, IV, unstaged/unknown), surgery (yes, no), radiation (any radiation [beam/nonbeam], no/unknown), and chemotherapy (yes, no/unknown). For radiation and chemotherapy, SEER does not provide separated values for no and unknown receipt of treatment. 17
Preliminary associations between clinical and demographic patient characteristics and overall death were calculated using chi-squared tests and independent samples t-tests where appropriate. Cumulative incidence curves (all-cause death) were created to depict cancer-specific death for each HPV-associated cancer site, stratified by sex for anatomic consistency. Gray’s tests with Bonferroni adjustments were used to determine if significant death existed between each of the 6 sites. We also calculated cumulative incidence curves for each HPV-associated cancer site (cause-specific death) stratified by race/ethnicity, insurance, and stage at presentation (Figures A1, A2, A3 and Table A1). The overall Gray’s test was performed along with comparisons to a predetermined reference group. Multivariable Fine and Gray proportional hazards regression models 25 stratified by anatomic site estimated the association of sociodemographic and clinical variables on cancer-specific death. These associations were estimated using subdistribution hazard ratios (sdHR) and corresponding 95% confidence intervals (CI). SEER*Stat version 8.3.5 (Surveillance Research Program, National Cancer Institute) was used for data extraction and SAS version 9.4 (SAS Institute, Cary, NC) was used for analyses. Statistical significance was set at P < .05, and all tests were two-tailed.
Results
Characteristics of study sample.
HPV-associated cancer sites by sex.

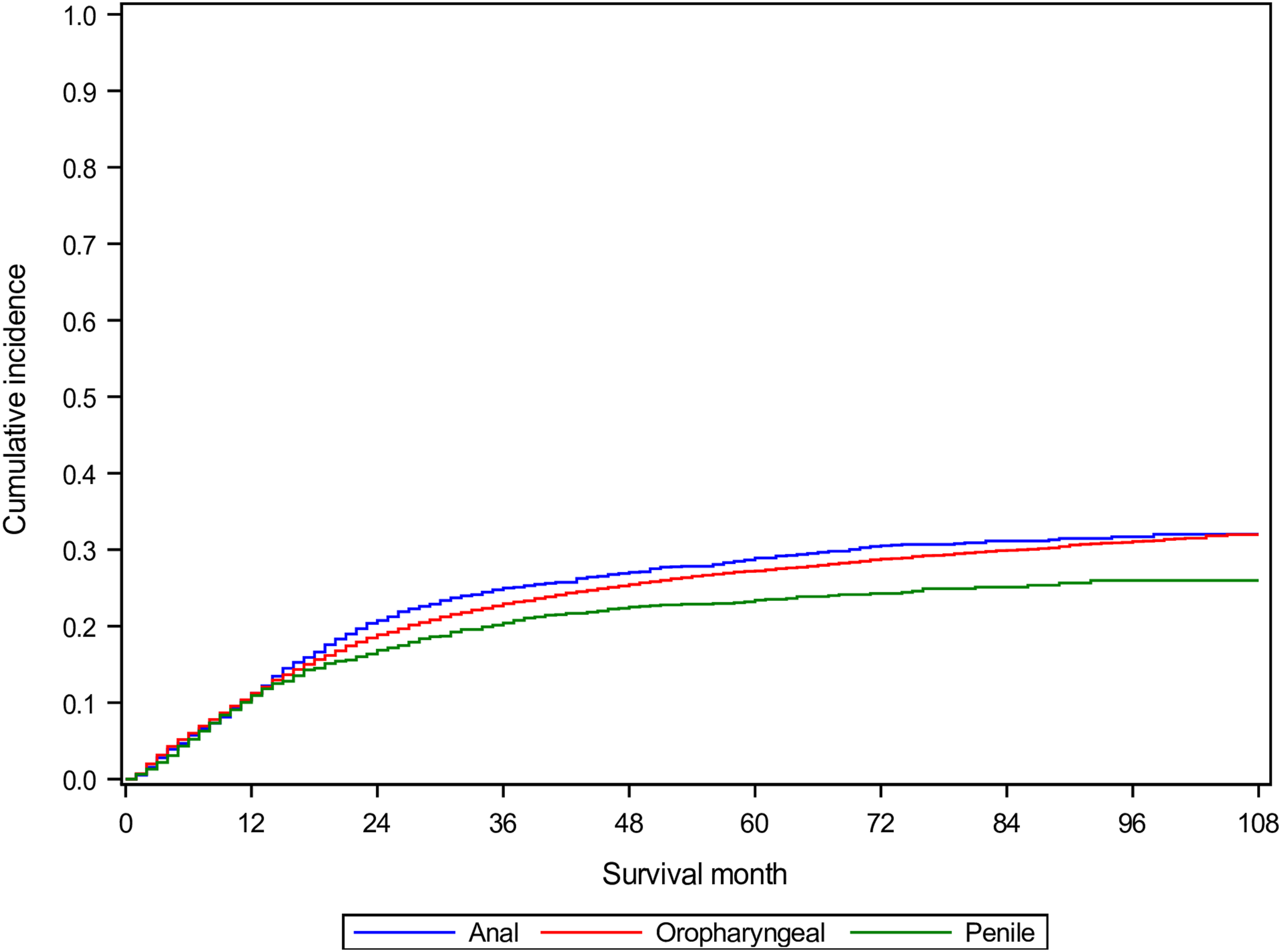
There were significant differences in cancer-specific death based on anatomic site for both males and females (Gray’s test P < .01). For females, vaginal SCC had the highest cancer-specific cumulative death (46%) compared with oropharyngeal SCC (37%), cervical carcinoma (32%), vulvar SCC (31%), and anal/rectal SCC (24%) [Bonferroni P < .05, Figure 1]. For males, penile SCC had the lowest cancer-specific cumulative death (26%) compared to anal/rectal SCC (32%) and oropharyngeal SCC (32%), while there was no significant difference between anal/rectal SCC and oropharyngeal SCC (Bonferroni P < .05, Figure 2). Cumulative incidence curves (outcome = cancer-specific death) of female study population by primary cancer site. SCC: Squamous cell carcinoma. Cumulative incidence curves (outcome = cancer-specific death) of male study population by primary cancer site. SCC: Squamous cell carcinoma.
Competing risks proportional hazards regression results

SCC = squamous cell carcinoma; sdHR = subdistribution hazard ratios; CI = confidence interval; bold values are statistically significant at P < .05.
Compared to married/partnered patients, divorced/separated patients had 46% increased risk of death from oropharyngeal SCC (sdHR = 1.46, 95% CI 1.36, 1.56) and 18% increased risk of death from cervical carcinoma (sdHR = 1.18, 95% CI 1.09, 1.27); never married patients had 24% increased risk of death from anal/rectal SCC (sdHR = 1.24, 95% CI 1.10, 1.39), 51% increased risk of death from oropharyngeal SCC (sdHR = 1.51, 95% CI 1.41, 1.61), 21% increased risk of death from cervical carcinoma (sdHR = 1.21, 95% CI 1.13, 1.30), and 35% increased risk of death from penile SCC (sdHR = 1.35, 95% CI 1.03, 1.76); and widowed patients had 36% increased risk of death from anal/rectal SCC (sdHR = 1.36, 95% CI 1.16, 1.58), and 45% increased risk of death from oropharyngeal SCC (sdHR = 1.45, 95% CI 1.31, 1.60).
Compared to nonMedicaid insurance patients, patients with any Medicaid had 46% increased risk of death from anal/rectal SCC (sdHR = 1.46, 95% CI 1.30, 1.64), 79% increased risk of death from oropharyngeal SCC (sdHR = 1.79, 95% CI 1.67, 1.91), 10% increased risk of death from cervical carcinoma (sdHR = 1.10, 95% CI 1.04, 1.17), and 23% increased mortality from vulvar SCC (sdHR = 1.23, 95% CI 1.04, 1.45). Also, compared to nonMedicaid insurance patients, uninsured patients had 71% increased risk of death from anal/rectal SCC (sdHR = 1.71, 95% CI 1.44, 2.04), 73% increased risk of death from oropharyngeal SCC (sdHR = 1.73, 95% CI 1.56, 1.91), 14% increased risk of death from cervical carcinoma (sdHR = 1.14, 95% CI 1.03, 1.25), and 103% increased risk of death from vaginal SCC (sdHR = 2.03, 95% CI 1.26, 3.25).
The multivariable models showed that for all HPV-associated cancer sites, stages II, III, and IV cancers had significantly increased cancer-specific death than stage I cancer. Also, patients who received surgery for all cancer sites had significantly decreased cancer-specific death than those who did not. Receiving any radiation (beam/nonbeam) was associated with significantly decreased cancer-specific death from anal/rectal SCC (sdHR = .71, 95% CI 0.62, .82), oropharyngeal SCC (sdHR = .41, 95% CI 0.38, .44), and cervical SCC (sdHR = .81, 95% CI 0.75, .88) compared to no/unknown radiation. Receiving chemotherapy was associated with significantly decreased cancer-specific death from anal/rectal SCC (sdHR = .68, 95% CI 0.59, .78), oropharyngeal SCC (sdHR = .83, 95% CI 0.78, .89), cervical SCC (sdHR = .75, 95% CI 0.69, .81), and vulvar SCC (sdHR = .82, 95% CI 0.69, .98) but was associated with significantly increased cancer-specific death from penile SCC (sdHR = 1.65, 95% CI 1.25, 2.18).
Discussion
Several previous SEER-based studies have examined prognostic factors related to survival of HPV-associated cancers, however most have focused on cervical and oropharyngeal cancer, and less so on rarer types of HPV-associated malignancies.14,15,13,26 Recently, Razzaghi et al 6 used 27 population-based cancer registries to assess the role of age, race, and gender on survival of HPV-associated cancer, but their study was mostly descriptive, and their data excluded marital status and insurance status. Our study examined survival outcomes of all HPV-associated cancers based on sociodemographic factors and build on the Razzaghi et al study. For a group of cancers with known survival disparity, social support, and health care access are well known patient variables predicting prognosis, and are integral for inclusion in cancer survival modeling.27-29
Our study found an overall survival rate of 54% at the end of follow-up. Razzaghi et al, 6 who reported 5-year survival rates ranging from as low as 47.4% (penile) to as high as 66% (vulvar), depending on primary cancer site. Considering 90% of anal and cervical cases are attributable to HPV types for which there is the nonavalent vaccine, a dramatic reduction in incidence should be achievable through primary prevention. 3 In fact in Australia, a recent disease modeling study revealed that the nation was on track to eliminate cervical cancer as a major public health threat by 2028, in part due to a highly successful HPV vaccination campaign. 30 The United States is similarly positioned to achieve such cancer prevention milestones, but success is largely contingent upon the ability to improve current HPV vaccination strategies and increase uptake rates. 31 It should be noted that individuals affected by HIV are disproportionately affected by HPV-associated cancers.32,33 For instance, a study found that although HIV-associated infections seemed to contribute minimally to the excess risk of death for women with HPV-associated cancers, women with HIV have a rapid progression of cervical cancer compared to HIV-uninfected women. 34 Similarly, survival among individuals with anal cancer is influenced by their HIV status especially among men with HIV. 12
We found gender disparities in survival of HPV-associated oropharyngeal and anal cancers. Interestingly, these HPV-associated cancers that occur in both sexes have continued to increase in incidence over the last two decades. 4 Previous studies have been inconclusive about gender differences in survival of oropharyngeal cancer.35-37 In the current study, males had a significantly elevated risk of death from anal cancer, but lower risk of death from oropharyngeal cancer, which is broadly consistent with the recent findings from Razzaghi and colleagues. 6 The lack of consensus in the literature highlights the need for studies that explore factors related to gender differences in cancer survival outcomes, including tumor biology, inequities in health care access, and risks from other competing causes of death.
The potential impact of health insurance on survival was evidenced among low-income individuals with Medicaid or uninsured, particularly for patients with anal or oropharyngeal cancer. Notably, those with Medicaid experienced worse survival outcomes than those with private coverage, particularly among oropharyngeal cancer patients. Individuals enrolled in Medicaid tend to be less healthier than those who are uninsured or privately insured—they experience a greater burden of health comorbidities due to generally lower socioeconomic status and higher rates of unemployment. 38 Oftentimes, individuals who suffer from a serious health event or disabling illness who should be the first to seek coverage do so retroactively rather than enrolling prior to health detriment, in a phenomenon known as adverse selection. 39 In addition, some patients may only qualify for Medicaid after a late stage diagnosis, or in some cases, after being admitted for cancer treatment. 40 These individuals are likely to sustain worse oncologic survival outcomes compared to their privately insured counterparts.40,41 Interestingly, there seems to be a complex interplay between health insurance status, stage of presentation, and race,29,42,43 and in the current study, blacks, who were also more likely to be uninsured or under Medicaid, were more likely to die from their HPV-associated cancers. 6 While studies have attempted to describe racial differences in cancer outcomes according to racial differences in tumor biology and treatment responses, most have concluded that stage of presentation and unequal access to quality cancer care play a greater role in cancer health disparities than do biological and tumor characteristics.5,43,44 Racial/ethnic minorities should be the target of future HPV-associated cancer interventions, since this population may likely continue to suffer worse outcomes if barriers to health care access are not addressed. 5
Interestingly, marriage positively impacted survival after penile, anal, and oropharyngeal cancers ⸺ all male-related HPV-associated cancers. In fact, unmarried patients with penile and oropharyngeal cancers had the most dramatic association with marital status (in both genders and across all HPV-associated cancers). However, among the female-only HPV-associated cancers, cervical, vaginal, and vulvar cancers, only cervical cancer had a statistically significant difference between the married and unmarried survivors. There is evidence that among cancer survivors, males might benefit from being married more than females. 45 Marriage may be a proxy measure for social support, which is critical among cancer survivors due to the huge psychosocial burden of cancer survivorship.46-48 It is therefore important to seek that better understanding of optimal support for these survivors. Critically, among sexual minorities, the impact of same-sex marriage on marital support deserves more attention, especially for oropharyngeal and anal cancers which have well-documented associations with sexual lifestyle and preferences.49-51
Limitations and Strengths
This study has important limitations. First, SEER files used for this study do not contain information on HPV-DNA tumor status, so cancers were classified based solely on histologic examination, or anatomic proxy (for HPV-associated oropharyngeal cancer). This introduces the potential for misclassification of etiologically associated HPV cancers as nonHPV-associated cancers (or vice versa), leading to biased results. For example, in oropharyngeal cancer where HPV-association has strong prognostic implications, some of the observed survival disparities may be explained by unmeasured differences in rates of HPV-associated tumors. Second, data on comorbidities was unavailable and therefore we were unable to control for them and these might affect our study findings. However, by focusing on cancer-specific mortality the impact of death directly from comorbid disease should be minimized. Third, other risk factors, such as tobacco use, might impact survival of HPV-associated cancers, especially oropharyngeal cancer, 52 but we were unable to control for this with the data available.
Notwithstanding these limitations, this is the first study of its kind to examine the association between marital status and health insurance status with survival of HPV-associated cancers in the United States and to assess cancer-specific survival on a population level across HPV-associated cancer sites. By design, the population-based nature of this study is an added strength, offering access to diverse population-level data and increased generalizability of our findings.
Clinical and Public Health Implications
As the number of HPV-associated cancer survivors continues to grow, a call to action for greater cancer survivorship surveillance is warranted. While the preventable nature of most HPV-associated cancers cannot be overstated, the lasting impact of HPV vaccination programs and screenings in potentially eliminating HPV-associated cancers hinges on concerted efforts to increase and sustain progress made in HPV vaccine uptake.
30
In 2019, 71.5% of adolescents aged 13–17 years received ≥1 dose of HPV vaccine (73.2% for girls and 69.8% for boys) and 54.2% completed the series (56.8% for girls and 51.8% for boys).
53
For young adults aged 18–26 years, this uptake is even lower, with national initiation rates of 40% for women and only 8% for men.
54
Recent news that vaccine coverage will include individuals through 27–45 years implies that millions of people who were previously deemed ineligible may qualify to receive the HPV vaccine in the future.
55
This new HPV vaccine-eligible age range coincides with the increased shift towards HPV-associated cancer among younger adults less than 50 years.12,56 Furthermore, because of the delay from HPV infection to cancer diagnosis, there is a large age cohort at risk who missed window for the preventative vaccination.
57
These patients are reliant on early diagnosis and treatment, which our study highlights still have large disparities. Our study provides additional support for targeted policy interventions addressing expanding health care access to help reduce health outcome disparities. Future studies may also explore the interaction of demographic and clinical characteristics on cancer-specific survival. Examples include determining if the associations of stage and treatment with cancer-specific survival are different based on marital status or insurance status, as patients who are unmarried or of lower socioeconomic status may have increased benefit of early stage at presentation or receiving treatment on their cancer-specific survival than those with better social support or of higher socioeconomic status. Cumulative incidence curves for cancer-specific mortality stratified by race/ethnicity for each HPV-related cancer site. Anal/rectal squamous cell carcinoma (SCC) overall Gray’s test p < 0.01; comparisons to Non-Hispanic White: Hispanic (All Races) p = 0.18, Non-Hispanic Asian/Pacific Islander or American Indian/Alaska Native (API/AIAN) p = 0.30, Non-Hispanic Black p < 0.01. Cervical carcinoma overall Gray’s test p < 0.01; comparisons to Non-Hispanic White: Hispanic (All Races) p < 0.01, Non-Hispanic API/AIAN p = 0.34, Non-Hispanic Black p < 0.01. Oropharyngeal SCC overall Gray’s test p < 0.01; comparisons to Non-Hispanic White: Hispanic (All Races) p < 0.01, Non-Hispanic API/AIAN p = 0.02, Non-Hispanic Black p < 0.01. Penile SCC overall Gray’s test p = 0.09; comparisons to Non-Hispanic White: Hispanic (All Races) p = 0.39, Non-Hispanic API/AIAN p = 0.09, Non-Hispanic Black p = 0.15. Vaginal SCC overall Gray’s test p = 0.97; comparisons to Non-Hispanic White: Hispanic (All Races) p = 0.95, Non-Hispanic API/AIAN p = 0.80, Non-Hispanic Black p = 0.72. Vulvar SCC overall Gray’s test p = 0.02; comparisons to Non-Hispanic White: Hispanic (All Races) p = 0.86, Non-Hispanic API/AIAN p = 0.33, Non-Hispanic Black p < 0.01. Cumulative incidence curves for cancer-specific mortality stratified by insurance status for each HPV-related cancer site. Cumulative incidence curves for cancer-specific mortality stratified by stage at presentation for each HPV-related cancer site. For all sites, the overall Gray’s test p < 0.01, and comparisons to stage I p < 0.01. Among cervical carcinoma patients, stage at presentation by age group.



Conclusion
We found marked sociodemographic disparities in HPV-associated cancer survival in the United States that often transcend specific sites. It is important that factors associated with survival, including the nonclinical factors described in this study, continue to be evaluated. In particular, the need for equal access to high-quality cancer care independent of race or health insurance status remains. Cancer survivors will continue to need social and emotional support as they progress in their cancer survivorship journey.
Footnotes
Author Note
Abstract of this paper was presented at the 2018 AACR Annual Meeting, Chicago, IL.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical review and approval was not required for the study because a publicly available data was used.