
Abstract
Background
Radon is a predominant indoor air pollutant and second leading cause of lung cancer in radon-prone areas. Despite the gravity of the health risk, residents in Canada have inadequate perception and taken minimal protective actions. Better perception of a risk motivates people to take preventive measures. Scholarship about radon health risk perception is lacking in Canada. We applied a mixed methods population health approach to explore the determinants shaping perception and actions of a resident population in Canada.
Methods
We conducted mixed surveys (n = 557) and qualitative bilingual interviews (n = 35) with both homeowners and tenants of Ottawa–Gatineau areas. The study explored residents' risk perception and adaptations factors. Descriptive, correlational and regression analyses described and established associations between quantitative variables. Thematic, inductive analyses identified themes in the qualitative data. A mixed methods analysis triangulated both results to draw a holistic perception of the health risk.
Results
Residents’ quantitative perceptions of radon health risk, smoking at home, synergistic risk perception, social influence and care for family were associated significantly with their intention to test for radon levels in their home, actual testing and mitigation. These results were explained further with the qualitative findings. Residents who had dual cognitive and emotional awareness of the risk were motivated enough to take preventive actions. Caring for family, knowing others who contracted lung cancer and financial capability were enablers, whereas lack of awareness and homeownership, cost of mitigation and stigma were obstacles to preventive actions. We also explored the dual subjective and objective aspects of risk perception that are influenced by micro- and macro-level determinants.
Conclusions
Inducing protective action to reduce risk requires comprehensive population-level interventions considering dual perceptions of the risk that can modify the risk determinants. Future research can explore the dual aspects of risk perception and unequal distribution of the risk factors.
Introduction
Indoor air quality is vital for the health of people in cold countries as they pass over 90% of time indoors. 1 Having the largest uranium reserve, 2 Canadian land produces much radon gas that enters home mainly through tiny gaps in foundations. 3 Radon accumulates indoors during the long winter months and further decays to emit radioactive alpha particles; once inhaled, these induce DNA mutations and can lead to lung cancer.4,5 Radon is the major (> 80%) source of lifetime radiation exposure 6 that has confirmed causative link to lung cancer.7-9 In 2019, about 40% cancer related deaths were from lung cancer and 1 out of 5 in non-smokers who suffer all the unjust stigmatization as smokers do. 10 Thus, radon is the leading cause of lung cancer mortality among non-smokers and second among smokers. 11 Children, women and smokers from lower socioeconomic groups are disproportionately affected by the exposure to indoor radon gas.7,12
Despite various efforts, the National Radon Program (NRP) lags the target public uptake. According to the Household and the Environment Survey, 55% of Canadian households have heard about radon; however, only 6% of them have taken any preventive action. 13 Bridging the gap between risk awareness and actual adoption of preventive behaviour presents a challenge for public health professionals. 14 So far, practitioners in different countries assumed that programmes offering better-communicated information, enforced guidelines and tax rebates would be among the best solutions for radon health risk management. However, studies in the United States, 15 the United Kingdom 16 and Ireland 17 showed that taking regulatory actions, offering rebates and even providing free test kits did not significantly improve the situations. Thus, a key issue – how to motivate the target population individually and collectively – remains unresolved.
Transdisciplinary research with psychology and neuroscience has described the subjective and objective understandings of risk and determined a dual cognitive and affective risk perception concept. 18 Social science research has identified that the success of any population-level awareness programme is contingent on the views and actions of key decision makers at the household level. 19 We assumed that attempts to reduce health risks would benefit from an understanding of people’s perception of the risk, as well as the views and actions related to its management. There is a dire shortage of scholarship on the public perception of radon health risk in Canada. We employed a Mixed Methods (MM) approach with theory-based tools to understand the determinants related to residents’ perceptions of the risk as well as the micro and macro level factors that motivate residents to adopt preventive actions.
Objectives
The objective of this study was to explore radon health risk perception of Ottawa–Gatineau residents applying a mix of research methodologies (qualitative and quantitative) and thereby generate evidence to inform radon health risk prevention policy.
Conceptual Framework
Population Health Approach
Population health is an approach that encompasses the broadest aspect of human health aiming to improve the overall health status by reducing health inequities among the subgroups. To achieve these objectives, it addresses the determinants that contribute to the health. These are the broad range of personal, familial, occupational, social, organizational, economic and environmental determinants that impact health. 20 Among these, there is a specific group relating to the social and economic aspects, often called social determinants of health. The latter group pertains to an individual’s place in society, such as education, employment and income. Addressing these determinants of health means generating changes in the systems which in turn can support healthy behaviours conducive to positive health and well-being. 11
Pragmatic Worldview
Pragmatism is a problem-oriented philosophy that acknowledges the importance of the strategic application of research methods to get the most useful answer to a research question. This paradigm advocates using of MM in research and bypassing the argumentative issues. 21 It focuses on what works and considers that as the reality concerning the research questions under scrutiny. 22
The population health approach as described above assumes that interrelated conditions and determinants impact health throughout the life course, and there is a systematic pattern through which these impacts occur and are perceived. 23 This approach is in accord with the pragmatic philosophical worldview that employs diverse and systematic ways to find how things happen, what works and what does not, by valuing both the objective and subjective knowledge. 24 Applying these approach and worldview, we aimed to explore the determinants of radon health risk that can support evidence-informed policy.
Protection Motivation Theoretical Lens
Exposure to a health risk communication message initiates 2 appraisal processes: (a) threat appraisal and (b) coping appraisal.
25
Threat appraisal is the evaluation of the chance (susceptibility) of contracting a disease and its seriousness (severity). A coping appraisal comprises response efficacy and self-efficacy. Response efficacy is the anticipation that carrying out recommendations would remove the threat effectively. Self-efficacy is the confidence in one’s personal ability to implement the recommended courses of action (Figure 1).
25
Theoretical lens: Protection motivation theory.
Consequently, the more one believes in the susceptibility and severity of a risk, the more would one engage in the coping appraisal. PMT specifies how these 2 perception processes guide a person to either adopt an active adaptive or maladaptive coping mechanism in response to a health risk.26,27 These understandings, in turn, control the intention and ultimately shape the behaviour of a person (testing for radon) that is called protection motivation. 28 On the contrary, maladaptive response puts an individual at further risk and leads to behave in a way (not testing for radon) that has negative consequences and ends up with inaction. This eventually results in unfavourable health outcomes (lung cancer).
Hence, protection motivation has 4 dynamics: (a) perceived probability or susceptibility of an outcome (lung cancer), (b) perceived severity of a threatening event (death), (c) response efficacy (perceived effectiveness of the test and mitigation measures) and (d) self-efficacy (confidence to successfully undertake a recommended action). Thus, protection motivation is the outcome of an educated threat appraisal and coping appraisal, and as a mediating variable, it motivates and maintains the protective health behaviour. 28
Methodology
We adopted a mixed methodology that is conducive to the achievement of the objectives of this study. As per Creswell et al, 24 we defined MMR as a methodology that focuses on research questions and seeks to understand multilevel influences on radon health risk perception in a Canadian context by employing different perspectives and methods.
Justification. The relevance of using such methods was that radon health risk is influenced by a complex set of determinants interacting with each other in different ways (63) that are hard to explore either by quantitative or qualitative method alone. Both methods have their strengths and limitations; so, we assumed that the combined outcome would provide us with a holistic picture of risk perception, and the understanding of which would be useful for guiding policy.
There are examples in health research that focus group discussions and interviews are used to gather insight to design a survey instrument or to identify the relevant variables for a subsequent study. 29 In other instances, qualitative work follows a large-scale survey to explore the mechanisms in further details and find out where the variables are linked. 30 Thus, we assumed that an early qualitative pilot study would provide an understanding of the risk variables and insights to design the survey questionnaires. Similarly, the survey outcomes would guide developing the core qualitative interview protocol. We expected to illustrate the contexts through identified patterns of risk perception and to discover any new theme from residents’ experience to support or refute current evidence. 31 Such analysis has been beneficial to provide a ‘whole greater than the sum of the parts’ 30 (p. 40) and thus, helped drawing a holistic interpretation from the results to frame the complete story.
Methods
In an exploratory sequential mixed method design, we looked for the empirical evidence from both (a) qualitative interviews of residents with a mixed open and semi-structured interview protocol including some close-ended queries and (b) quantitative survey with a structured questionnaire including some open-ended questions.
Qualitative interview participants. We selected the interviewees purposefully (survey takers who showed some degree of knowledge about the issue) from the neighbourhoods of Ottawa–Gatineau CMA (census metropolitan area). We made efforts to reduce bias by including participants from the diverse sociodemographic subgroups such as homeowner and tenant, male and female, young adult and elderly, different ethnic groups, levels of education, income and occupation categories. The final number of interviewees was 35.
Qualitative measures and pilot study. Qualitative interviews explored themes and noted participants’ sociodemographic situations. The questions covered residents’ source of radon health risk information, level of radon health risk awareness, the perception of susceptibility and severity of the risk, enablers and barriers in the context of residents’ adoption of preventive actions or maladaptive risk behaviours. A mini-pilot study conducted earlier helped designing the main interview protocol. Two researchers (SMK and SC) jointly analysed data following Charmaz’s 32 coding procedures that gave initial ideas about the core constructs around the variables as well as about positive adaptations and maladaptive behaviours. These initial findings helped guide the development of the survey instrument to collect quantitative data.
Quantitative survey participants. In a cross-sectional, non-experimental design, we conducted a complex survey to assess perception of radon health risk between 2 independent groups of residents from Ottawa–Gatineau CMA. This is the only CMA that spans 2 provinces, and its area comprised the capital city of Canada. 33 This 6767 square kilometre area had an estimated resident population of 1,323,783 with 535,499 private dwellings in 2016. 33 We applied a stratified two-stage cluster design based on postcodes. Group I and group II were property owners and tenants, respectively. We had a stratified random sample of 140 participants from each of the 2 cities and 2 neighbourhoods (city centres and suburban areas). We selected homeowners (70%) randomly via public access property rolls. Tenants (30%) of the population who rent houses were chosen from the same city centres and neighbourhoods and selected randomly from the rental agency lists. Therefore, our final sample was assumed to be 560 (140×2×2).
The neighbourhoods were chosen keeping in mind the possible variability in (a) prevalence of the risk perception or radon awareness, (b) urban vs suburban population, (c) percentage of adult smokers (11.3% and 14.2%, respectively), (d) lung cancer incidence (1 in 4400 and 1 in 4300 respectively) and (e) average radon values.10,33-35 The selection criteria were living in a house that is in touch with the ground, spending at least 4 hours on the ground floor or in the basement for at least 1 year.
Study areas and sample. Radon-related lung cancer risk is particularly relevant in Ottawa–Gatineau areas as most of the houses are built over the Canadian Shield, and there is a radiological anomaly emanating from the Gatineau Park. Besides, there exist homes that are among the oldest in the country with porous basements and recent evidence of many radon-induced lung cancer cases, particularly among the non-smoking female population in the area (Figure 2).
10
Survey sample scheme.
Quantitative measures and variables. The survey consisted of multiple-choice closed ended as well as some open-ended questions. We measured independent variables – radon awareness, perceived susceptibility of the risk, perceived severity of the outcome, that is, lung cancer, social influence, synergistic risk (of radon with smoking) perception and smoking behaviour in home. As DiPofi, LaTour and Henthorne 36 identified, one of the most frequently cited reasons for taking action was the protection of children, and our pilot study also found that the presence of a child in the household influenced radon-related awareness and behaviour, we included this as a variable. The dependent or outcome variables were residents’ intention to test for radon and were measured in an ordinal scale, and residents’ actual testing and mitigation done or not were expressed in binary responses such as ‘yes’ or ‘no’.
We employed anchored relative scales rather than Likert scales as research has identified the former to be more sensitive than the latter. 37 The anchored relative scales had predetermined grading points unlike a range from 0 to 10 used by the Likert scale. This enabled having a clear idea about the distance between 2 measuring points (available on reasonable request).
The control variables at the individual level included the sociodemographic factors like age, gender, education, occupation, income, race/ethnicity and homeownership or tenancy. The socioeconomic status (SES) was estimated based on participants’ occupation and the total household income in the previous year. The race and ethnicity were considered synonymous, and we used the categories as per National Household and Environment Survey. These were European Canadian, Aboriginal Canadian and Visible Minority, but we kept option for those not willing to answer as ‘prefer not to respond’.
Data Collection Procedures
Quantitative data collection. Quantitative data were gathered through a mix of methods such as an online survey launched through a webpage and other social media (Twitter and Facebook), calling over phone and recording, and receiving the response by email. The online survey lodged by Qualtrics contained a link to the consent form. The selection criteria were set in a way that only people fulfilled the inclusion criteria could take the survey. However, as about 10% of residents have no access to the internet, 38 we conducted a similar face-to-face survey at the community settings using pen and paper or an iPad where appropriate. This ensured residents’ inclusive representation. Thus, a response rate of over 96% was achieved.
Qualitative data collection. We conducted face-to-face interviews following an interview protocol (available on reasonable reaquest) and recorded voice using a digital (Sony) recorder and took field notes simultaneously. Interviews lasted for 60 minutes on average that we continued until a thematic saturation was achieved. Interview data (verbal) were enhanced by adding observation (visual), field notes (written) and photographs collected or taken from the spot to develop a contextualized understanding of the risk perception. 39
We paid no monetary remuneration to the survey takers or interview participants, only a radon testing kit was available to the participants who agree to test their houses voluntarily. As the community is bilingual, surveys and interviews were conducted both in English and French.
Data Analysis
Quantitative data analysis. Descriptive and inferential analyses were conducted using SPSS 24 with 95% confidence intervals setting the alpha level at .01 and .05 (two-tailed) alternatively. After sensitivity analyses, the descriptive statistics included frequency distributions to summarize the data. Univariate and bivariate analyses were conducted for the whole sample, subgroups (depending on homeownership and demographic variables) and outcomes (those with and without testing intentions, actual testing and mitigation). The Chi-square test of association used to determine whether study variables were associated with the intention to test for radon. 40 Multivariate binary logistic and ordinal regression conducted to identify predictors for the intention to test as well as actual protective behaviours that included whether the homes were tested and mitigated for radon.
Qualitative data analysis. We transcribed verbatim all interview data, and for the pilot project, we followed Charmaz’s 32 procedure of line-by-line coding using the gerund. For the main qualitative interviews, we followed Miles et al 41 and Braun and Clarke’s 42 coding recommendations. First, we assigned initial descriptive codes to the transcribed texts that were followed by more focused codes. From the observation notes, we inserted memos to the texts as relevant. A code list was prepared to show the codes and subcodes with their descriptions and illustrations. A contact summary form was added at the end of each interview outlining the important themes associated with participant’s perceptions and reported behaviours. Considering the large volume of qualitative data, we used Atlas.ti for the focused coding and further analysis. We followed Braun and Clarke’s 42 thematic analysis procedures to find, refine, organize and categorize codes and ultimately determined the patterns and final themes ( 43 Ref. published qualitative article).
Mixed Methods Analysis
As per Creswell and Plano-Clark’s 24 MM approach, we corroborated the qualitative and quantitative findings to find links and relations between them. We identified points where one outcome complemented another and triangulated the results to come up with themes supported by both parts of the research outcomes. Besides the data generated through surveys and interviews, we collected some secondary data related to the existing building laws and regulations, the latest development in building codes, ongoing programmes related to radon management policy in Canada and around the globe, policy proposals designed by different organizations and initiatives taken or under process with various agencies and levels of governments. These were from credible sources like the latest published peer-reviewed literature, government agencies, private, intergovernmental or non-governmental organizations and from interactions with the key informants and researchers in the field. Consultation with the principal radon stakeholders, scientists, homebuilders and health professionals on the research objectives helped to get a broader insight into the current state of affair regarding radon research, policy and programmes. The interpretation of conducted research findings and integration of ideas from experts in the field and linking them to the latest development in the area helped to understand residents’ radon risk perception and preventive actions in a comprehensive manner.
Point of Interface
The point of interface or mixing in this MMR was made intentionally and systematically throughout the cycle of this project rather than keeping the quantitative and qualitative aspects separate to combine only at the end. The aim was to maximize the diversity and minimize the introduction of bias that can compromise the study quality. Initially, mixing was done right from the conceptual and theoretical frameworks, and the process continued through the designing of interview protocols and survey questionnaires. It remained in the data collection phase, as mentioned above, some numeric data were gathered from the qualitative interviewees, and a few qualitative data were collected from the survey through open-ended questions. Besides, during data analysis, some of the qualitative data, for example, by counting the occurrence of themes (sources of information, average time passed or children sleeping in the basement), were converted into quantitative scores to compare with quantitative frequencies. Although these were not from a representative sample, such analysis helped to explain, corroborate and compare one finding with another while conducting the MM analysis as is customary in the field.
44
For example, we considered how many cases a resident was motivated to test by the sense of care for children and how this corresponded to the quantitative findings. Finally, mixing was done during the final data interpretation when the quantitative results were compared with the themes that emerge from the qualitative research.
45
A schematic of these sequences of mixing of concepts, methods, analyses, interpretations and the outcomes related to each of these processes is presented in Figure 3. Scheme of MMR and point of interface.
Results
While both the quantitative and qualitative outcomes are published in 2 separate articles, here, we present only the outcomes of MM analysis of combined data that relate the findings from both studies and enhance the explanation of radon health risk perception.
Demographics of Survey Participants.

The sample of the qualitative study consisted of 35 interviewees purposefully selected from the above cohort (Table 2). As our purpose was to collect more information, we selected survey takers who showed some degree of radon knowledge and either tested or mitigated their houses for radon. For this reason, the sample was under-represented by the tenants and people from the low-income groups.
Variations in the Source of Risk Information
Source of radon information. From the quantitative study (Figure 4), we knew that most residents (54%) learned something about radon from the mass media including television, newspaper and magazine, etc. Whereas the qualitative findings provided us with the breakdown of this information. Where we found that most residents (28%) learned about radon for the first time from local newspapers or magazines, not from the popular mass media – television that usually comes to mind at the first place. Source of randon information. ““There was a report in the Ottawa Residents, a local newspaper in the Kanata area that talked about radon gas.” (SP19). ““I read something about its years ago, in the Maclean’s magazine” (SP18).
Surprisingly, many residents (20%) got to know about radon for the first time in their lives from the current study. “You delivered a presentation in the community center, and I heard from that (SP3). “I had not heard of radon till I was contacted to participate in your survey” (SP10). “I heard about it from your study” (SP25).
Others heard from their friends and peers, only 8% came to know from the internet, 5% heard on the radio and 3% from other sources (Scientific article, NRC, etc.). It was noted only in one instance from the interviews where watching a story of a non-smoking woman on television who contracted lung cancer motivated a resident to test and mitigate the house for radon. There, a doctor was shown to indicate the possibility of exposure to radon for that lung cancer case (SP7). The same was manifested from the response to an open-ended question in the survey. When asked, what else you know about radon (Q. 29; Figure 5, most survey participants (52%) responded ‘nothing’ as shown in the word cloud. Word cloud: What else you know about radon?
Variations in radon health risk perception
From the survey, we found that many residents did not know much about radon whereas the qualitative study provided evidence that although most of them knew very little, some residents possessed in-depth knowledge about the health issue. We were able to explore the reasons behind the different level of knowledge and perception across population subgroups. These included (a) personal health consciousness, especially, if someone was a lung cancer survivor; (b) familial – being concerned about the health of children living in the basement; (c) social – interaction with friends and witnessing others in the community who were diagnosed with or suffering from lung cancer or visiting a home fair and (d) occupational – hearing about the risk from a colleague, taking part in training at one’s workplace or learning as a part of one’s job.
The in-vivo quotes from qualitative interviews supported these variations:
Personal
“I am health conscious; if I know something is a risk factor, I would go for fixing that. I learned that all homes have a certain level of radon” (SP7)
Familial
“My daughter does sleep there (basement) quite often. So, I am concerned about her sleeping in the basement and a buildup of radon” (SP23).
Social
“We had friends who live a few kilometres from here, who told us about radon. This increased our awareness” (SP1).
Occupational
“I was trained in hazardous materials operations, as part of the fire department but more for the knowledge but not exactly to be active but to understand what the risk may be and thus, I came across also to radon gas” (SP32).
Thereby, our qualitative study enhanced understanding of the information gathered from the survey; otherwise, our understanding would remain limited.
Variation of Perception Across Sociodemographic Characteristics
Sociodemographic Characteristics of Qualitative Study Participants.
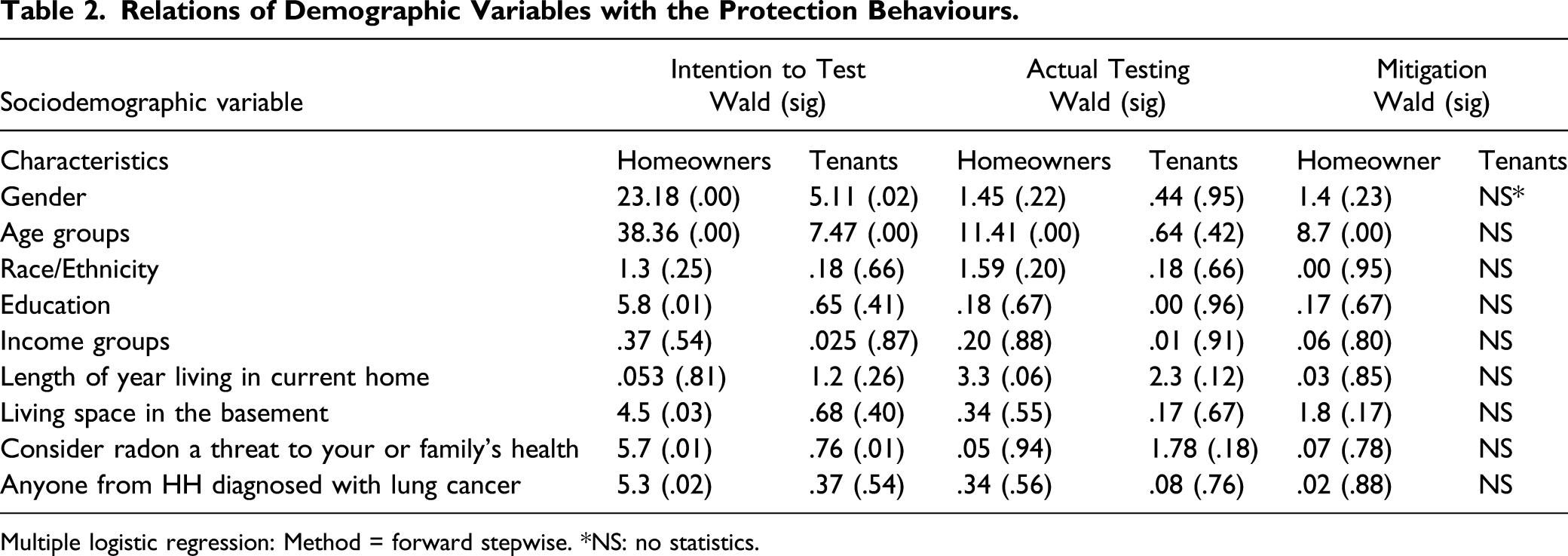
Age was associated with the intention to test for radon both for homeowners and tenants; when it came to test and mitigate homes, it was significant for the homeowners but not for the tenants. The reason also remained unclear until we got to know from the qualitative data that homeowners were comparatively older, had children and they cared for their health. We found no correlations of race or ethnicity with either intention to test or protection behaviours, neither for homeowners nor for tenants.
Education was significantly correlated with the intention to test for radon in the case of homeowners but not tenants. When we explored the qualitative data, we found that elder homeowners invested more times to study the health issue. On the other hand, among tenants who were generally not highly educated, could only know about the risk from their workplace and colleagues. Similarly, income group was correlated neither with the intention to test or protection behaviours in both homeowners and tenants. This finding contradicted the qualitative result as residents who tested and mitigated homes for radon were generally of higher SES.
Likewise, the length of living in the current home was not correlated with either intention to test or protection behaviours, neither for homeowners nor for tenants. Instead, we found this to act as the basis of maladaptive behaviour, as stated by 1 participant: ‘I’ve lived in my house for forty years, but I don’t yet know, and everybody is healthy’ (SP26).
Our quantitative analysis showed that tenants spent more time than homeowners in the basement (32% vs 27%) consistently with their type of dwelling. However, this variable had a significant correlation with the intention to test for radon by the homeowners but not for tenants. This result practically complemented our qualitative findings as most of the tenants in our small qualitative sample were living either on the ground floor or in the basement and obviously spending substantial time there.
However, when it came to testing homes for radon, homeowners remained ahead of the tenants for the reasons of authority or property ownership, financial ability and having children living in the basement, as we hinted above, and it would be clear from the analysis described in the next section.
Variations of Adopting Preventive Behaviours

Multiple logistic regression: Method = forward stepwise. *NS: no statistics.
Similarly, the finding of strong association between social influence and preventive behaviour matched with the qualitative finding. We identified instances of social influences where one witnessed a 60-year-old neighbour dying of lung cancer, who was not a smoker. Other participants mentioned hearing about the gravity of the risk from friends, peers and colleagues that motivated them to test for radon.
Compliance With the PMT
Differential Outcomes of Binary and Ordinal Regression Modeling.

aOrdinal regression model fit statistics. Likelihood for homeowner = 60.31, P < .00; 1, tenants =30.26, P < .00 and X2 for homeowners = 71.59, tenants = 42.79, df = 7.
bValues refer to the predictors that are significant in the model. SE = standard error of β; Std. β = standardized beta, χ2 = chi-square statistic, df = degree of freedom. NS: no statistics.
cBinary regression model. Cox and Snell R2 for homeowners = .224, tenants = .139; Nagelkerke R2 for homeowners =.300, tenants = .199; P < .00, df = 1.
Whereas quantitative study showed statistically significant associations of residents’ perception of the risk with their intention to test, actual testing and mitigating behaviours, the qualitative findings demonstrated response efficacy as those who thought radon as a real threat to themselves and their family members carried out recommendations with the expectation of eliminating the risk. Again, in terms of self-efficacy, those who had the knowledge and financial capability executed the recommended courses of action successfully. 25 Thereby, we found evidence of the constructs of PMT that the more residents believed they were susceptible to a serious threat, the more they engaged in the threat and coping appraisal. These comprehensions, in turn, determined the intention and ultimately the behaviour termed as protection motivation 28 (Figure 1). Thus, PMT was implicitly followed as these 2 perception processes led a small group of residents to adopt an active adaptive response, but another large group to deny the threat. The latter group either took no action or followed maladaptive coping mechanisms. 27
Maladaptive behaviours. We defined maladaptive behaviours as taking actions ignoring the recommended standard. We discerned some ideas residents held to be scientifically unfounded. Some installed alternate systems (ventilation) that have less to do with radon mitigation, but they thought they were safe. [We cannot provide here an in-vivo quotation as this study participant did not permit us to quote]. Others felt that they are safe because they live in a new house ‘I live in a new house, and I don’t think there is any risk” (SP2).
This is also against the latest scientific evidence that confirmed all houses have some amount of radon and new houses have it comparatively more than the older ones. 46 Although theoretically this is termed as maladaptive behaviour, for having a lower radon level, the study participants considered themselves under no serious threat of exposure from radon. Some others even took ignorance as a bliss: ‘I think, some people might be afraid of the fact that if there is radon and then, they have to spend money that they don’t want. The old saying ‘ignorance is bliss’ yeah, I don’t have a problem because I don’t see there is one’ (SP32).
Discussion
The objectives of this MMR were to understand the holistic aspects of radon health risk perceptions and how these might vary among residents’ subgroups. Another part was to explore the social antecedents determining differential radon health risk perceptions and motivations to take preventive actions. While cross-examined the quantitative and qualitative findings, we identified that the associations among the measured variables fluctuated across the population subgroups. We identified that the critical tool to raise public awareness, that is, the mass media has not been adequately and effectively used to disseminate radon health risk communication message to the target residents. Age might play a role in this, as most of our interviewers were elderly and retired people and they were not as much fond of social media as the new generations do. For them, the source of information was newspaper, radio and/or television. This finding matches that of the Environment and Household Survey of 2015 33 and agrees with the previous historical analysis of media coverage of radioactive gas in Canada. 47 We were surprised to notice that many residents became aware of radon health risk for the first time from our survey. 48 Besides, people of lower income groups, tenants renting house and people who live in rural and suburban areas have a comparatively lower level of awareness, and they have less access to radon health risk information and resources than the property owners and those living in the cities. These observations were also noted previously by researchers in the field. 14 Thus, we had to make the same conclusions as was made nearly 2 decades ago that the Canadian National Radon Program has not been highly effective in informing residents and prompting action. 49 Our finding of television show instance of lung cancer demonstrates the substantial impact of television. However, it also shows the lack of reach of such programmes to the greater population and underscores the importance of live campaigns using this and similar popular media.
Our collected evidence from both parts of the studies supported the constructs and dynamics of the protection motivation and psychological theory of risk perception. Although a few residents showed in-depth knowledge about the health risk, most others who came across radon information demonstrated misconceptions about the risk. This includes unrealistic optimism, low appreciation of the susceptibility and severity of the risk as were noted with past studies in the US 50 and Ireland 51 among residents of high radon areas where people exactly believed that radon was a threat to others, and they had no likelihood of getting lung cancer.
We also noted evidence that people got motivated and acted when driven by the emotional aspects of risk perception in addition to that of cognitive perception.43,48 Irrespective of homeownership, having children lived in the basement or on the ground floor was significantly correlated with residents’ intention to test for radon and actual testing behaviour. This signifies their universal care for children that is the emotional or affective aspect of risk awareness as explained by the psychological theory of risk perception. 18 This finding corresponds with those of previous studies.18,52
The varied adoption of protection behaviour by the tenants can be explained either by their lack of authority over the property to make any structural changes or by the financial capability as supported by qualitative findings. We also noticed that misconception of the risk is dissipated through either experiencing the harm by oneself or observing others directly to suffer as was evident from a resident who had a 60-year-old neighbour and another who watched women in a TV show – both were otherwise healthy and non-smokers but had contracted lung cancer. Availability of such instances of harm motivates people to be convinced about the health risk. 53 However, conversion of such conviction to a health protective behaviour has not been straightforward. Psychological studies in this area showed that translation of risk information and transforming that into a health behaviour followed complex stages and was influenced by various triggering factors both at the micro and macro levels.50,52,53
On the contrary, some maladaptive responses demonstrated in our study also supported the PMT constructs. At the micro-level, people develop mini theories that can make them defensive while confronting intimidating risk information. 54
Studies have showed that when a health message is personally threatening, people usually moderate their perception of severity about health risk, fabricate questions about the accuracy of the risk information and process it in a subjective manner.25,55
Besides, there are macro-level factors such as how the risk is viewed and who is considered responsible for managing the risk. 56 Such structural barriers cannot be overcome only through risk communication messages. As we can observe growing community action against drugs in Canada and gun control in the US developed over consensus, such established social norms, consensus and action groups for radon can help motivate more people to adopt protective actions, especially in high radon areas. Fortunately, we found residents who are much enthusiastic about going out and convening others to assemble and engage in collective social action on radon. Others suggested to engage various public and non-governmental agencies.
Recommendations. For radon intervention to have a measurable impact, mere transmission of frightening risk message, how much evidence-based it might be, we should take strategic approach by adding innovations to health message. Since people’s construction of mini theories vary in types, risk communication techniques must adopt novel tactics such as using diverse media, varied forms of messages with an appeal to both the cognitive and emotional aspects of risk perceptions and engaging the authentic agencies, professionals and celebrities in delivering the message. As per our findings, presenting the real-life scenarios can have positive impact. Such vivid communication helps people to link the situation to both their personal and family members’ health and acts as an incentive to engage in protective behaviours. Evidence from the UK showed better outcomes when radon health risk communication campaigns were made repeatedly 57 and engaged authentic agencies 58 in radon-prone areas. Moreover, public health inspectors and environmental health professionals could support people in remote rural areas with the necessary information and resources.
We came to know about a home inspector who alerted one (SP34) of our interviewees about the radon health risk while inspecting the house during a sale. Home inspectors can be an active stakeholder to engage in raising awareness and escalating discussions about testing during all real estate transactions. Public Health Inspectors can also promote access to the Canadian National Radon Protection Program’s online portal 59 where residents can get the contact information about certified radon professionals for radon testing and remediation. It is noticed that specific population subgroups who rent basements, reside or work in the ground- and basement-level facilities, children who spend most of their daytime in such daycare centres, people who live in long-term care homes or correctional facilities or social housing are particularly vulnerable and more at risk of exposure to radon than others. Evidence showed that the highest concentrations of radon are generally found in the lowest levels of a building; thus, these population subgroups should be paid special attention. Public health inspectors should visit and discuss radon health issue with the managers, operators of ground- and basement-level facilities. They should also talk to the residents and provide information about the health risk. 14
We identified some population health determinants like education, income, occupation, social connections, etc. to be crucial in getting access to radon health risk information. To this end, the issue of radon health risk can be included in the public health risk awareness curriculum. Federal plan to test workplaces covers only the government offices; this can be expanded to private offices and workplaces by making inclusions under the workplace safety and industrial hygiene laws and regulations. Education and training of people involved in construction, building and real estate industries are also important. As an example, the New Brunswick Real Estate Association 60 requires realtors to take a radon course that teaches them about the dangers of radon and different radon mitigation methods. Besides, such training currently requires that realtors of both the seller and buyer mention radon during a real estate transaction. 61
Limitations
Due to lack of adequate population-level data, we could not use health inequity toolkits to measure the difference in the level of risk perception between the subgroups. Both the quantitative and qualitative studies were limited by sample size and locations covered. The survey conducted online might have failed to include participants from diverse demographic and cultural backgrounds which might have skewed the results. Thus, future research would generate robust data from a representative sample and interviewing with participants from diverse socioeconomic backgrounds and covering high radon areas in Canada. Notably, similar studies in cities of active radon health communication interventions would generate noteworthy evidence to support or counter the findings of this study.
Conclusion
This MMR unfolded the intricate aspects of radon health risk perception of a resident population in Canada. The constructs and variables explored from the initial qualitative pilot helped developing the survey questionnaire to measure resident’s perception of radon health risk. The quantitative part applied the protection motivation theoretical lens and statistically determined that residents’ perceptions of the health risks of radon are a marker of intention to test their homes for radon and are a clear predictor of actual risk mitigation behaviours. However, the variables reflecting public perception of the radon health risk did not always resulted in the adoption of protection behaviours. To understand that aspect, we conducted a qualitative study that explored the vital aspects of residents’ knowledge and views of radon and perception of the risk. This study filled the scholarly gap on the perception of radon risk in Canada by providing a deeper understanding of residents’ experiences, thus generated evidence that explained and complemented the quantitative findings. We were able to identify the reasons behind the gap between risk awareness and actual adoption of preventive action. Our study underscores the importance of seriously considering how radon risk is understood and dealt with by residents. We identified that having mere cognitive risk awareness is not enough to prompt preventive action; instead, additional affective awareness motivates residents to act. Thereby, we conclude that the radon health communication program would be more effective through addressing both these aspects of risk perception along with plausible regulations and necessary incentives.
The MM analysis added further insight by clarifying the fact that residents who had children living in their basement and who had significant social influence became concerned and proactively tested as well as mitigated their houses for radon. We were also able to explore the social antecedents such as health consciousness, type of self-education, active social networks and financial capability that determine residents’ views and lead to adopting preventive behaviours.
Our study explored all 4 dynamics of the PMT: (a) Perceived probability, (b) perceived severity, (c) response efficacy and (d) self-efficacy. Thus, it was demonstrated that protection motivation was the result of an informed threat appraisal and coping appraisal, and as a mediating variable, these prompted, guided and in some cases helped to demonstrate the protective health behaviours. Thus, results obtained from the analyses of both methods validated the constructs described in the protection motivation theory as well as the psychological theory of risk perception.
Future research can explore the dual aspects of radon risk perception applying psychometric measurements. This will help discover the facets of cognitive and affective aspects of risk perception regarding radon-induced lung cancer risk. Adopting a health equity lens, future research can assess the distribution of radon health risks by considering stratification by age, gender, education, income, geographic location and other population subgroups.
Footnotes
Acknowledgements
Khan S. M. is grateful to Dr Daniel Krewski for extending financial support to this project and Dr Raywat Deonandan for his technical inputs. We would like to express our thanks to all survey takers and interview participants.
Author Contributions
S. M. Khan conceived, designed the study and developed survey instrument and qualitative interview protocols under guidance of J. Gomes and S. Chreim.
S. M. Khan conducted bilingual surveys and interviews, recorded data, translated French data to English and analysed quantitative data and performed statistical tests with J. Gomes.Qualitative data were analysed jointly by S. M. Khan and S. Chreim.
S. M. Khan prepared the first draft and the other two critically reviewed and added inputs.
S. M. Khan incorporated the inputs obtained from the other two co-authors and sent them the final manuscript.
All authors reviewed the final manuscript and agreed to send for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The McLaughlin Centre for Population Health Risk Assessment (389969) and Telfer School of Management, grant number, University of Ottawa (602733) supported this study.
Ethical approval
The University of Ottawa’s Health Sciences and Science Research Ethics Board (REB) approved the study and data collection protocols (file number: H10-17-03) on December 13, 2017.
Informed consent
We duly secured informed written consent for participation, voice recording and direct quoting. We assigned a number to each participant to maintain anonymity and excluded any identifying information from the quotes.