
Abstract
Background
This study aimed to determine the relationship of programmed death-ligand 1 (PD-L1) expression and standardized uptake values in fluorodeoxyglucose–positron emission tomography/computed tomography (FDG-PET/CT) with prognosis in non–small-cell lung cancer (NSCLC).
Methods
We retrospectively analyzed 328 NSCLC patients who underwent lobectomy/segmentectomy with lymph node dissection. PD-L1 expression was detected by immunohistochemically stained using the murine monoclonal antibody clone 22C3. The preoperative maximum standardized uptake value (SUVmax) of FDG-PET/CT at the primary lesion; pathological factors including histological type, microscopic lymphatic, venous, and pleural invasion; and lymph node metastases in resected specimens was determined. Significant prognostic clinicopathologic factors were analyzed by univariate and multivariate analyses.
Results
PD-L1 expression was higher in men, smokers, squamous cell carcinoma, advanced pathologic stages, positive venous invasion, positive pleural invasion, and high preoperative SUVmax (≥3). Postoperative survival analysis showed that both PD-L1 expression and preoperative SUVmax were significantly negative prognostic factors in univariate analysis for overall survival (OS) (P = 0.0123 and P < 0.0001) and relapse-free survival (RFS) (P = 0.0012 and P < 0.0001). Kaplan–Meier survival curves showed that the OS and RFS were the best in patients with negative PD-L1 expression and SUVmax < 3, intermediate in patients with positive PD-L1 expression and SUVmax < 3 and those with negative PD-L1 expression and SUVmax ≥ 3, and poor in patients with positive PD-L1 expression and SUVmax ≥ 3.
Conclusion
Combining PD-L1 expression and preoperative FDG-PET/CT SUVmax in primary tumor might help in accurate prediction of postoperative prognosis in NSCLC patients.
Introduction
Lung cancer is the leading cause of death by cancer in most developed countries. 1 Although multidisciplinary therapies are used for advanced non–small-cell lung cancer (NSCLC) patients, the overall survival (OS) rate is still poor. Recently, several humanized monoclonal antibodies that block immune checkpoints have been developed and have proven to be useful in selected patients with unresectable NSCLCs.2,3 The association between programmed cell death 1 (PD-1) and programmed death-ligand 1 (PD-L1) can be utilized to target these monoclonal antibodies. Inhibition of the PD-1/PD-L1 axis enhances antitumor immunity and prevents tumor cells from escaping from host immune responses, which provides a promising strategy for effective tumor immunotherapy. 4 Previous clinical trials reveal the treatment effect predictor of immune checkpoint inhibitor (ICI) such as PD-L1 expression5-7 and tumor mutation burden 8 as a positive correlation and SKT11 and KEAP1 mutations as a negative correlation. 9 However, the number of clinical studies remains limited, and the results are controversial. In contrast, pembrolizumab is an ICI that can be used for single agent administration in the first treatment for advanced stage NSCLC. The tumor proportion score (TPS) is the most highly correlated effect predictor of pembrolizumab.5,7,10
However, the relationship between PD-L1 expression and various clinicopathologic factors is still unclear. We previously have reported on the clinicopathological significances of PD-L1 expression in 90 resected NSCLC patients 11 and also shown that the preoperative maximum standardized uptake value (SUVmax) of FDG-PET/CT at the primary lesion is a more efficient index of nodal metastasis compared to tumor size. 12
Therefore, this study aimed to determine the relationship of PD-L1 expression and preoperative SUVmax in fluorodeoxyglucose–positron emission tomography/computed tomography (FDG-PET/CT) with prognosis in NSCLC.
Patients and Methods
We enrolled 328 NSCLC patients (179 men and 149 women; age range = 46–81 years; mean age = 67.1 years) who underwent lobectomy or segmentectomy, along with lymph node dissection, after preoperative FDG-PET/CT from January 2008 to December 2019 at our hospital. The exclusion criteria were preoperative induction therapy and multiple lung cancers. The histologic types were adenocarcinoma (Ad) in 258 patients, squamous cell carcinoma (Sq) in 48, large-cell neuroendocrine carcinoma (LCNEC) in 13, large-cell carcinoma (La) in 8, and adenosquamous carcinoma (AdSq) in 2. The pathological stages were 0 in 13 patients, IA (IA1–IA3) in 229, IB in 48, IIA in 13, and IIB in 25. The median postoperative follow-up period was 62 months; range = 2–135 months. Of 48 patients with stage IB, 29 patients (60.4%) received postoperative adjuvant therapy with oral uraciletegafur (UFT); of 38 patients with stage II, 13 (34.2%) received intravenous platinum doublet-based chemotherapy and 3 patients received pembrolizumab with or without platinum doublet as a clinical trial [MK3475-671]. On the other hand, 62 patients relapsed, then 37 patients (59.7%) received the standard anti-cancer therapy according to guidelines. Eleven (17.7%) patients received EGFR-TKI, and 9 (14.5%) patients received ICI as the treatment for relapse.
This study was approved by the Ethics Committee of St. Marianna University School of Medicine, Kanagawa, Japan (accession no. 1461), and written informed consent was obtained from all included patients.
FDG-PET/CT Imaging
FDG-PET/CT was performed using four integrated PET/CT scanners: Eminence-G SOPHIA 3000GCT/M (Shimazu, Tokyo, Japan), Biograph DUO LSO (Siemens, Berlin, Germany), ECAT ACCEL (Siemens), and Discovery IQ (GE Healthcare Japan, Tokyo, Japan), reported in detail in our previous study. 13 The patients were made to fast for 5 h and then were given 150–300 MBq FDG intravenously according to the body weight; PET testing was performed 1 h later. Patients with blood glucose levels >200 mg/dl at the time of PET testing were excluded. Image slices were obtained from the skull–midthigh vertex. PET scanning times per image slice were as follows: Eminence-G SOPHIA 3000GCT/M, 2.6 min; Biograph DUO LSO, 3.4 min; ECAT ACCEL, 5.1 min; and Discovery IQ, 3.8 min.
Region of interest (ROI) was manually set to the lung lesion determined by PET and CT. The border of the ROI was drawn based on CT, and SUVmax was used for the validation. The SUVmax for each suspicious lesion was automatically calculated after delineation of the area of interest on attenuation-corrected FDG-PET/CT images.
Pathologic Examination for Local Tumor Invasion
Pathologic examination of dissected lymph nodes was performed. In addition, we evaluated microscopic tumor invasion according to International Association for the Study of Lung Cancer (IASLC; Denver, CO, USA) criteria 13 as follows: absence of lymphatic invasion (Ly0), presence of lymphatic invasion (Ly1), absence of microscopic venous invasion (V0), presence of microscopic venous invasion (V1), and presence of macroscopic venous invasion (V2).
The pleural invasion status in resected lung specimens was evaluated as follows: tumor confined within the subpleural lung parenchyma or invading superficially into pleural connective tissue beneath the elastic layer (PL0), tumor invading beyond the elastic layer (PL1), tumor invading the pleural surface (PL2), and tumor invading any parietal pleura component (PL3).
Immunohistochemistry
Immunohistochemistry was performed using the PD-L1 IHC 22C3 pharmDX kit (Dako, Carpinteria, CA, USA) according to the manufacturer’s instructions. We selected PD-L1 because the Food and Drug Administration (FDA) has approved it for companion diagnostic testing to determine the applicability of pembrolizumab treatment. Briefly, serial 3-μm-thick sections were cut from formalin-fixed, paraffin-embedded tissue blocks, and the sections were deparaffinized in xylene and rehydrated using a graded series of ethanol concentrations. Next, antigen retrieval was done in Envition™ FLEX Target Retrieval solution (Dako) in a 97°C water bath for 20 min. Intrinsic peroxidase activity was blocked using hydrogen peroxide for 5 min. Subsequently, the sections were washed with a wash buffer (Dako), and primary antibodies were applied to cover them. The sections were then incubated for 30 min at room temperature, again washed thrice with the wash buffer for 5 min each time, incubated with an anti-mouse linker antibody specific to the primary antibody’s host species, and then again incubated with a ready-to-use visualization reagent comprising secondary antibody molecules and horseradish peroxidase molecules coupled to a dextran polymer backbone. Finally, the sections were counterstained with hematoxylin for 5 min and mounted under a coverslip.
PD-L1 Expression
We followed instructions given in the “PD-L1 Immunohistochemistry Testing in Lung Cancer” manual of the IASLC (https://www.iaslc.org/sites/default/files/wysiwyg-assets/pd-l1_atlas_book_lo-res.pdf). Briefly, the pathologists counted PD-L1-positive tumor cells, defined as complete circumferential or partial cell membrane staining. Cytoplasmic staining and tumor-associated immune cells, such as macrophages, were excluded from scoring. The tumor proportion score (TPS) was calculated as follows:
TPS (%) = (PD-L1-positive tumor cells/Total number of tumor cells) × 100.
The TPS was used to categorize the staining status as follows: <1% (negative staining), ≥1% and ≤49% (weakly positive staining), and ≥50% (highly positive staining); in other words, all tumors with TPS ≥1% were considered as showing positive PD-L1 expression.
On the basis of PD-L1 expression (negative or positive) and preoperative SUVmax (<3 or ≥3), the patients were divided into four groups: Group A: negative PD-L1 expression and preoperative SUVmax <3 Group B: positive PD-L1 expression and preoperative SUVmax <3 Group C: negative PD-L1 expression and preoperative SUVmax ≥3 Group D: positive PD-L1 expression and preoperative SUVmax ≥3
Statistical Analysis
Statistical analysis was performed using JMP software. Clinicopathologic characteristics by categorical variables were evaluated using the chi-square test. The OS and RFS were analyzed using the Kaplan–Meier method. Univariate analysis compared differences in survival rates using the log-rank test, and Cox regression analysis was used for multivariate analysis for survival. P < 0.05 was considered statistically significant.
Results
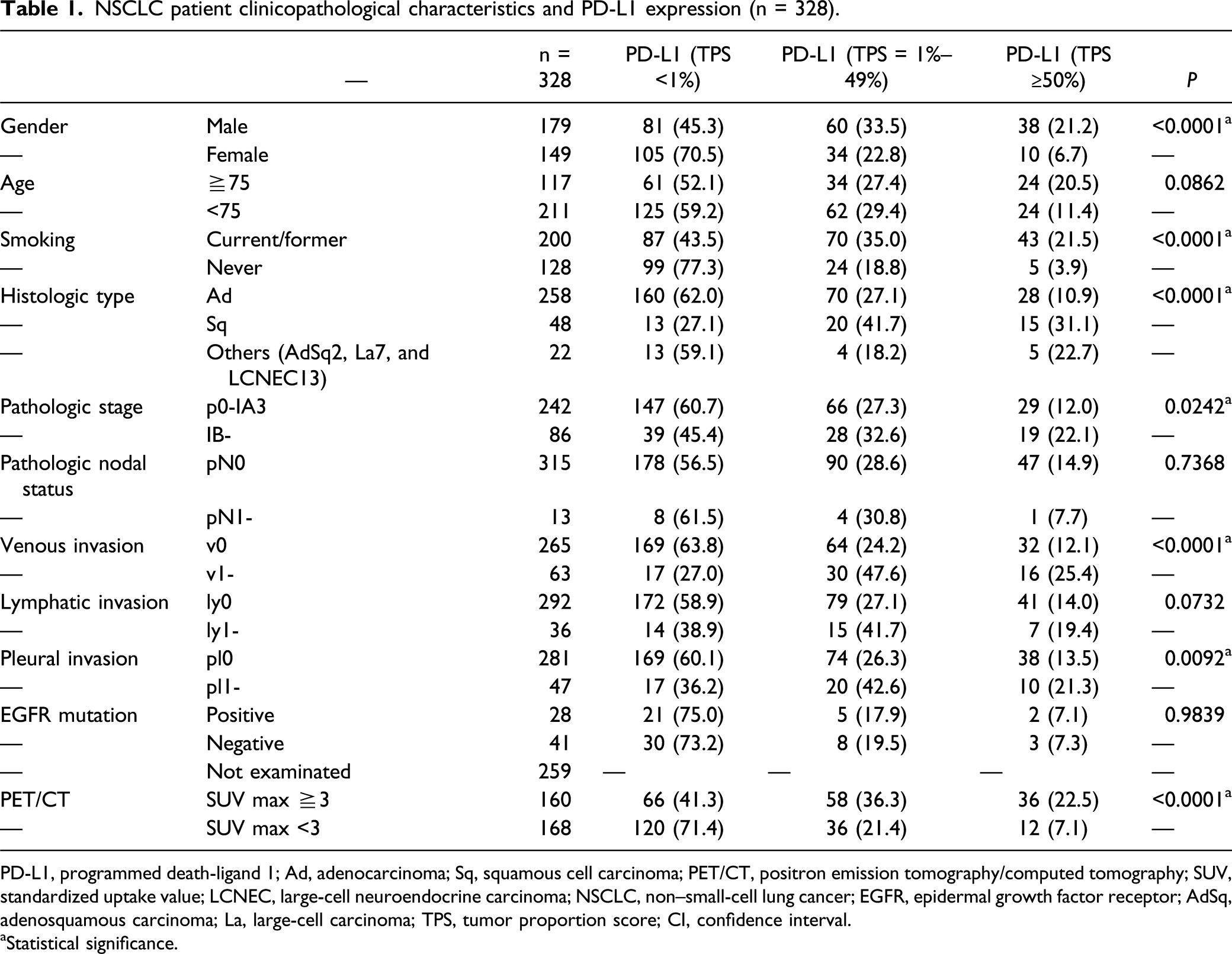
Figure 1 shows the staining of PD-L1-positive tumor cells: negative staining (TPS <1%) (Figure 1A), weakly positive staining (TPS ≥1% and <49%) (Figure 1B), and highly positive staining (TPS ≥ 50%) (Figure 1C). Table 1 shows all the patients’ clinicopathological characteristics and PD-L1 expression status. PD-L1 expression was higher in men (P ≤ 0.0001), smokers (P ≤ 0.0001), Sq (P ≤ 0.0001), advanced pathologic stages (≥IB; P = 0.0242), positive venous invasion (P = 0.0001), positive pleural invasion (P = 0.0092), and patients with SUVmax ≥3 (P = 0.0001). However, we found no relationship of age, pathologic nodal status, lymphatic invasion, and epidermal growth factor receptor (EGFR) mutation status with PD-L1 expression. Staining of PD-L1-positive tumor cells: negative staining (TPS<1%) (A), weakly positive staining (TPS ≥1% and <49%) (B), and highly positive staining (TPS ≥ 50%) (C). PD-L1, programmed death-ligand 1; TPS, tumor proportion score. NSCLC patient clinicopathological characteristics and PD-L1 expression (n = 328). PD-L1, programmed death-ligand 1; Ad, adenocarcinoma; Sq, squamous cell carcinoma; PET/CT, positron emission tomography/computed tomography; SUV, standardized uptake value; LCNEC, large-cell neuroendocrine carcinoma; NSCLC, non–small-cell lung cancer; EGFR, epidermal growth factor receptor; AdSq, adenosquamous carcinoma; La, large-cell carcinoma; TPS, tumor proportion score; CI, confidence interval. aStatistical significance.
Univariate and multivariate analysis of the OS.
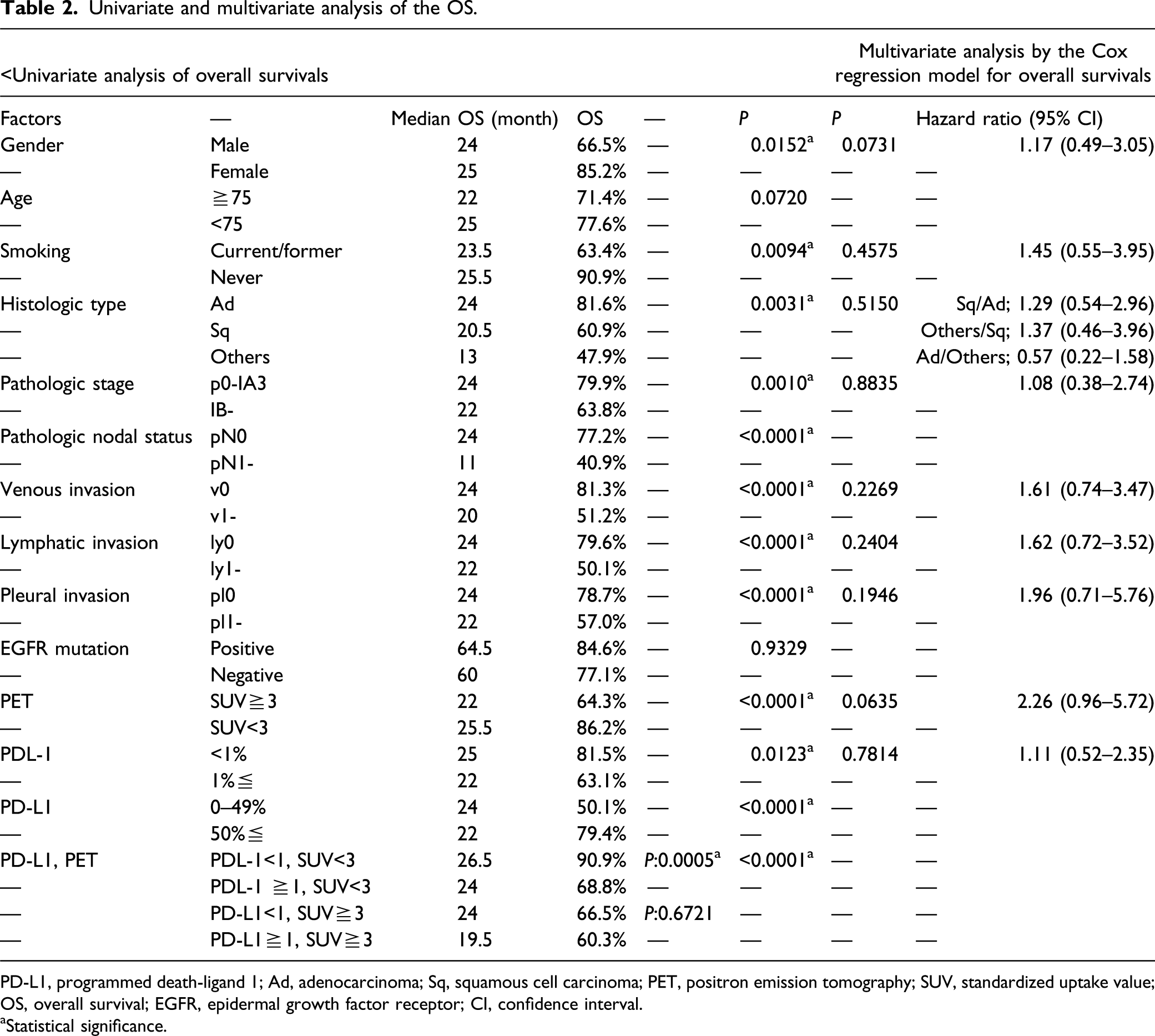
PD-L1, programmed death-ligand 1; Ad, adenocarcinoma; Sq, squamous cell carcinoma; PET, positron emission tomography; SUV, standardized uptake value; OS, overall survival; EGFR, epidermal growth factor receptor; CI, confidence interval.
aStatistical significance.
Univariate and multivariate analysis of the RFS.

RFS, relapse-free survival; PD-L1, programmed death-ligand 1; SUV, standardized uptake value; CI, confidence interval.
aStatistical significance.
When PD-L1 expression was defined by TPS ≥1%, PD-L1 was expressed in 58.8% of NSCLC patients with preoperative SUVmax ≥3 and in 28.5% of NSCLC patients with preoperative SUVmax <3.
And we perform subgroup analysis to investigate whether adjuvant therapy affects prognosis. There was no statistically significant difference both in the OS (P = 0.3607) and RFS (P = 0.2205) between the group received adjuvant therapy and not (data not shown).
Kaplan–Meier survival curves show there was a statistically significant difference both in the OS and RFS between the degree of PD-L1expression (P < 0.0001) (Figure 2A) and between preoperative SUVmax (P <0.0001) (Figure 2B). Kaplan–Meier survival curves. (A) The OS and RFS were the best in the PD-L1 negative group, intermediate in the weakly positive group, and poor in the highly positive group. (B) Preoperative SUVmax was lead to poor prognosis both on OS and RFS. (C) The OS and RFS were the best in group A, intermediate in groups B and C, and poor in group D. (D) The OS and RFS were the best in the double negative group, intermediate in group only one is positive, and poor in the double positive group. PD-L1, programmed death-ligand 1; OS, overall survival; RFS, relapse-free survival.
According to Kaplan–Meier survival curves, the OS and RFS were the best in group A, intermediate in groups B and C, and poor in group D. There was a statistically significant difference in the OS between group A and B (P = 0.0005) but not between groups C and D (P = 0.67212). There was no statistically significant difference in the RFS between groups A and B (P = 0.0693) and between groups C and D (P = 0.3975) (Figure 2C). In addition, we compare double negative (group A) vs intermediate (groups B and C) vs double positive (group D). There was a statistically significant difference both in the OS (P < 0.0001) and RFS (P < 0.0001) (Figure 2D).
Multivariate analysis showed preoperative SUVmax was the only independent negative prognostic factor for the RFS (Table 3) and that there was no independent negative prognostic factor for the OS (Table 2).
In addition, to evaluate utilities of combining positive PD-L1 expression and preoperative SUVmax, we perform logistic regression analysis of 3-year OS and RFS. Regarding 3-year OS, 118 patients were enrolled, we eliminate patients who is still alive, but the observation period has not been reached 3 years. Positive PD-L1 expression and preoperative SUVmax ≥3 (area under the curve (AUC) =0.716), positive PD-L1 expression (AUC=0.601), and preoperative SUVmax ≥3 (AUC=0.676). Regarding 3-year RFS, 131 patients were enrolled, and we eliminate patients who are still not relapse, but the observation period has not been reached 3 years. Positive PD-L1 expression and preoperative SUVmax ≥3 (AUC=0.798), positive PD-L1 expression (AUC=0.660), and preoperative SUVmax ≥3 (AUC=0.758).
Discussion
SUVmax of FDG-PET/CT has high reproducibility and availability, so it is used as a parameter for making diagnoses; performing tumor, node, and metastasis (TNM) staging; and monitoring for therapeutic effects. Bille et al. 14 (2013) reported the prognostic significance of SUVmax in both early and advanced NSCLC. In addition, a systematic review and meta-analysis showed that a high SUVmax is related to poor OS in NSCLC patients. 15 These findings are consistent with our results. We previously reported, when NSCLC patients are classified on the basis of an SUVmax cut-off of 3, preoperative SUVmax at the primary lesion is a more efficient index of nodal metastasis compared to tumor size. 12
Increased PD-L1 expression is significantly correlated with poor survival in NSCLC patients, 16 which is consistent with our results. This finding also supports the idea that increased PD-L1 expression enables tumor cells to evade host immune surveillance and promotes disease progression. 17 However, Kerr et al. 18 (2019) showed that positive PD-L1 expression is correlated with better OS in resected NSCLC. Therefore, increased PD-L1 expression is correlated with favorable and unfavorable prognoses in different studies. In this study, PD-L1 expression affects worse prognosis both on OS and RFS. However, in the near future, it is likely to be PD-L1 expression might affect better prognosis by ICI treatment, like EGFR mutation affects better prognosis by EGFR-TKI treatment, 19 despite EGFR mutation have no significant difference both on OS and RFS in this study.
Preoperative SUVmax is correlated with PD-L1 expression in NSCLC patients.20-23 SUVmax ≥8.6 is correlated with PD-L1 expression (TPS ≥ 11%) but is an independent prognostic factor for the OS in Sq patients. 20 In addition, increased PD-L1 expression (TPS ≥ 2%) and a high SUVmax (>11.2) are both independent risks factors for poor OS in Sq patients. 21 There is a statistically significant difference between the OS and RFS in Ad patients with SUVmax ≥2.9. A statistically significant difference in the OS was also seen in Ad patients with TPS ≥6% but not in the RFS. 22 SUVmax is significantly higher in Ad and Sq patients with positive PD-L1 expression compared to those without. 23 Most of these findings are consistent with our results. Limited to the cases of preoperative SUVmax<3, we find out the statistical significance between PD-L1 expression on OS (P = 0.0005) and marginal significance on RFS (P = 0.0693). This fact indicated that combining PD-L1 expression and preoperative SUVmax might be a factor in predicting prognosis in NSCLC because this study shows preoperative higher SUVmax was the independent prognostic factor for poor RFS by multivariate analysis.
In a near future, immune-PET imaging might be one of a standard clinical assessment tools in this field. 24 Niemeiger et al. showed that PET-CT with 18Fluor-labeled anti-PD-L1 adnectin, and 89zirconium-labeled nivolumab may be useful biomarker to non-invasively evaluate PD-1 and PD-L1 expression. 25 In the era of immune-PET, we could get more precise information about PD-L1 expression because immune-PET hampered unsolved issues we have, such as varying immunohistochemistry antibodies, tissue preparation and processing variabilities, oncogenic vs induced PD-L1 expression levels that changed over time, and staining of tumors vs immune cells. 24 Not only we obtain more precise information about PD-L1 expression, we could obtain SUVmax of primary site more routinely. So, toward the future, this study may have more importance.
This study had some limitations. First, the number of patients enrolled was relatively small to obtain reliable results. Second, this was a retrospective, not a prospective, multicenter study; therefore, bias might exist. Third, the postoperative observation period was relatively short. Further studies with a larger and external validation cohort are necessary in order to confirm our results.
Conclusion
This retrospective study assessed the clinicopathological significance of PD-L1 expression correlated with preoperative SUVmax in surgically resected NSCLC. PD-L1 detected by the monoclonal antibody 22C3 is differentially expressed in several clinicopathologic factors, such as sex, smoking status, histologic type, advanced pathologic stages, positive venous invasion, positive pleural invasion, and preoperative SUVmax. Positive PD-L1 expression and preoperative SUVmax ≥3 are correlated with poor OS and RFS in NSCLC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.