
Abstract
Background
Cancer is one of the leading causes of death within the United States. Adolescence remains a critical stage of development in which new cognitive skills and lifestyle factors related to cancer are acquired. It is critical to understand adolescents’ knowledge of cancer and preferences for receiving clear and easy-to-comprehend information about cancer and cancer prevention. The purpose of this study was to explore adolescents’ perceptions of cancer and cancer risk factors and identify their preferences for receiving cancer prevention education.
Methods
The survey used in this study was based on the Health Belief Model framework, the Youth Risk Behavior Survey, and the Cancer, Clear & Simple (CC&S) Curriculum. The survey evaluated adolescents’ knowledge, attitudes, and health-related behaviors regarding cancer and cancer prevention among adolescents. Three Midwestern middle and high schools were recruited, and 235 students completed the survey. Survey responses were analyzed using descriptive statistics.
Results
Study participants had some basic knowledge of cancer; however, only 66% recognized that individuals have control over their risk of developing cancer. Participants (95%) reported that cancer prevention was important, yet only 37.3% stated they knew how to lower their risk of getting cancer and 50% indicated that they currently try to make decisions that lower their chances of getting cancer. About 82% stated that an educational game would be a useful tool to learn about cancer and prevention.
Conclusion
Study findings indicate the need for an increase in adolescent knowledge of cancer, specifically how they can control their cancer risk, and prevention strategies through development of game-based education to teach adolescents about cancer-related topics.
Highlights
What do We Already Know About This Topic?
Cancer is the fourth leading cause of deaths for adolescents. The rise in cancer risk factors has created a significant increase of cancer diagnoses in the adolescent population. Current literature indicates there is a knowledge gap among adolescents and their cancer awareness, exposure to cancer risks and the correlations between health behaviors and cancer diagnoses.
How Does Your Research Contribute to the Cancer Control Field?
This study explored adolescents’ perceptions about cancer and risk factors and identified preferences for receiving cancer education in school settings. This research contributes to the Cancer Control field by aiming to advance cancer prevention though examining adolescents’ cancer awareness, decision-making and lifestyle choices, and preferences for cancer education and interventions.
What Are Your Research’s Implications Toward Theory, Practice, or Policy?
Findings from this study support the need for a cancer intervention, specifically in the form of a serious game, to increase adolescent knowledge of cancer, risk factors, and prevention strategies. Education on lifestyle habits such as eliminating tobacco use and alcohol consumption, promoting healthy eating habits, increasing exercise, and protection against sunlight exposure are necessary to inform adolescents on cancer prevention and how to practice health behaviors, which can assist in the reduction of the number of cancer diagnoses each year.
Introduction
According to the National Cancer Institute, in 2020 about 1.8 million new cancer cases were diagnosed in the United States and more than 60,6000 people were estimated to have died of cancer. 1 Despite improvements in survival rates, cancer remains one of the leading causes of death in the United States. 2 The rise in cancer risk factors has created a significant increase of cancer diagnoses among adolescents. 2 Cancer is the fourth leading cause of death in adolescents, followed by accidents, suicide, and homicide.3,4 Furthermore, members of racial/ethnic minorities, people living in rural areas with limited access to health care, and/or of lower socioeconomic status, report higher rates of cancer with worse outcomes. 5 Current literature indicates there is a knowledge gap among adolescents and their cancer awareness, exposure to cancer risks and the correlations between health behaviors and cancer diagnoses.6,7
It is critical to educate adolescents about cancer risk and prevention because they are at a transitional stage where development of new cognitive skills and behavioral factors related to a healthy lifestyle can be acquired.7-9 Adolescence is a stage where neurodevelopment and lifestyle practices are emerging and changing. 10 Risk-taking behaviors and susceptibility to social influence increase during adolescence, but this is also a time where adolescents become more independent in their decision-making.11,12 While there are individual differences in impulsivity and risk-taking during adolescence, studies show early interventions can reduce the severity and long-term impact of these actions by increasing control over behavior, especially when a valued goal is associated with the intervention. 13 Additionally, there is evidence that adolescents can learn to avoid harmful health-related behaviors, especially if they are given information that relates the consequences of those behaviors to potentially damaging outcomes. 14
Nearly half of all cancer diagnoses among adolescents are subject to 5 main lifestyle factors: tobacco use, alcohol consumption, eating habits, lack of exercise, and unprotected sunlight exposure.15-17 Adolescence is the period of greatest development for the lung, and tobacco carcinogens can make the early smoker more susceptible to damaging effects. 18 In addition, e-cigarette use has dramatically risen among middle and high school students in the United States, with a 900% increase in use from 2011 to 2015. 19 Furthermore, literature demonstrates a correlation between heavy alcohol consumption in late adolescence that persists into adulthood with an increase in cancer probability. 20 High body-mass index during adolescence has also been associated with an increased risk of mortality and morbidity for most cancers in adulthood. 21 Similarity, adolescents are considered an at-risk group for developing skin cancer later in life due to high reported rates of sunburn, ineffective use of sunscreen or other sun protectants, and overall low levels of knowledge of sun protective behaviors. 22 Findings from multiple studies suggest the need for a standardized way to provide adolescents with accurate information about tobacco, e-cigarette, and alcohol use, as well as sun exposure, diet, and exercise to curb the cancer epidemic.
It is important to consider adolescents’ perspectives and preferences in the development of an educational cancer intervention. However, there are a limited number of studies focused on how to best increase adolescents’ awareness and knowledge about cancer prevention and the effectiveness of educational interventions. 6 Tailored health education that builds on the understanding of current knowledge and beliefs of a targeted group is more successful than similar strategies that lack this foundation.23,24 The importance of rooting health education in existing knowledge and beliefs stems from a discrepancy in the way different people view health. 25 A more effective intervention can be created by understanding adolescents’ preexisting knowledge of cancer and identifying their preferences for receiving clear and easy-to-comprehend information about cancer risk and cancer prevention.
Increasing adolescents’ awareness of how modifiable lifestyle factors contribute to cancer risk may influence life-long patterns of healthy behavior and decrease the number of cancers diagnosed each year. Examining adolescents’ awareness of cancer risk factors and preferences for cancer education will lead to a collaborative and effective educational intervention. 2 This information will assist in creating educational interventions targeted at adolescents to decrease the risk of cancer over their lifetime. The objectives of this study were (1) to explore adolescents’ perceptions about cancer and cancer prevention, (2) examine adolescent behaviors that affect cancer risk, and (3) identify preferences for receiving cancer education.
Methods
Survey Design
The Health Belief Model (HBM) guided the conceptualization of the survey administered to study participants. The HBM is commonly used in health behavior research because it elucidates both the change and maintenance of health-related behaviors and serves as a strong foundation for health behavior interventions.
26
The HBM has been used extensively to understand predictors of preventative health actions, including individuals’ perceptions of cancer and their behaviors that avoid or reduce cancer risks.27,28 The HBM framework (Figure 1) is informed by primary concepts that predict what factors influence adolescents’ behavior to prevent, screen for, or control cancer conditions, including susceptibility, severity, benefits, barriers, self-efficacy, and cues to action.
26
Health Belief Model. The Health Belief Model was used in this study to explain individuals’ perceptions of cancer and their behaviors that avoid or reduce cancer risks.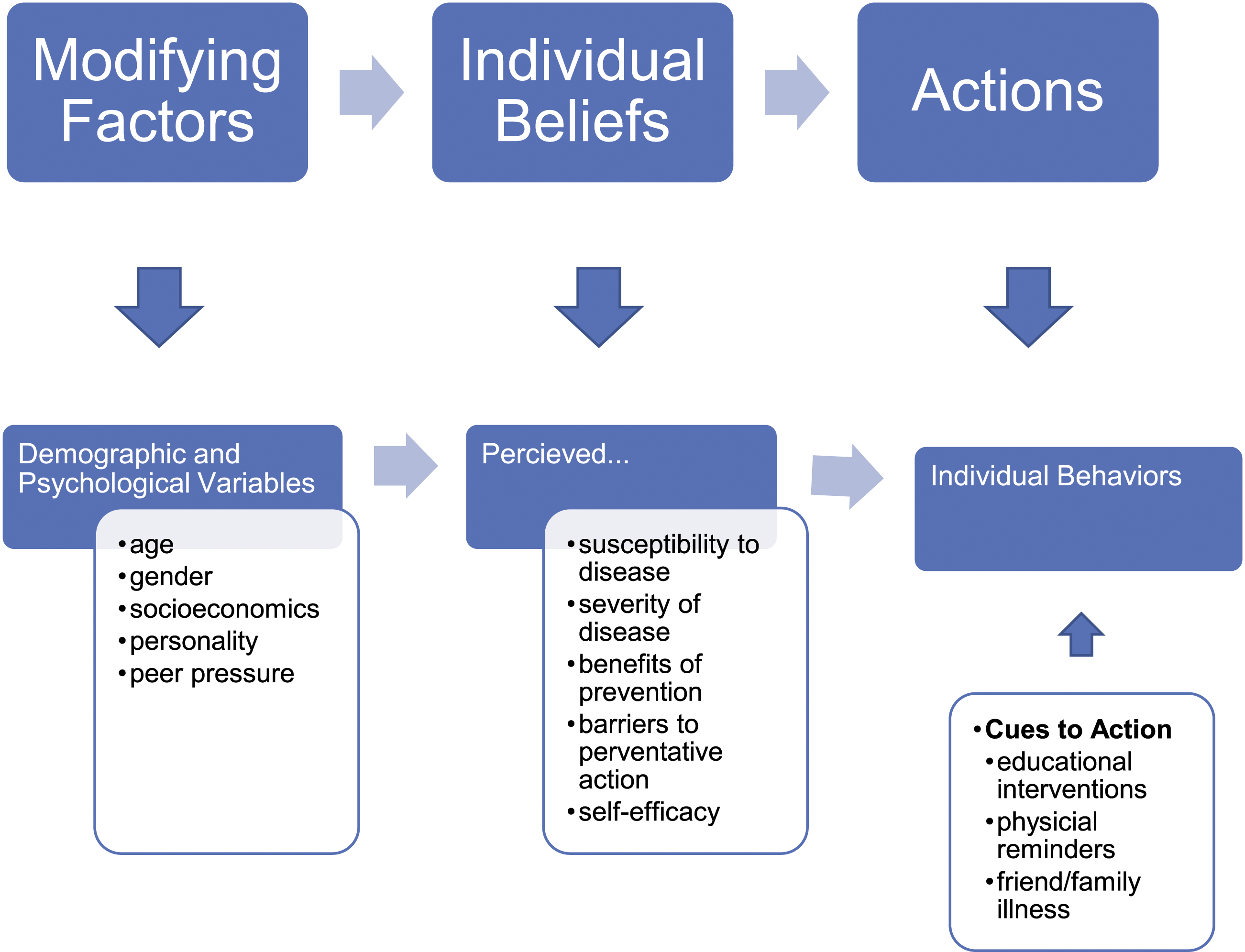
The study team developed an online survey consisting of closed-ended questions with “yes/no” or Likert scale response options and demographic questions (see Supplementary Material). Survey questions were designed to explore adolescents’ perceptions and knowledge of cancer and cancer prevention, including cancer-related health behaviors. Survey questions related to behavior were adapted from the Youth Risk Behavior Survey, a validated survey instrument. 29 Additional survey questions examined adolescents’ cancer knowledge, current information sources, experience with cancer, attitudes about cancer risk and prevention, and preferences for receiving cancer education and sharing learned information.30-32 These questions were adapted from previous studies that examined cancer awareness, as well as the Cancer, Clear & Simple (CC&S) curriculum created by the Midwest Cancer Health Disparities Initiatives.24-26 The CC&S curriculum is designed to enhance cancer knowledge and awareness to help persons by improving their health-related decision-making, specifically for rural, African American, and Latinx communities. 33 This study developed survey questions from the rural adaptation of the CC&S curriculum which includes topics on cancer basics, cancer prevention, and cancer screening. 32 The survey also collected participants’ demographic information, including age, grade, gender, race/ethnicity, zip code, and number of people under 18 in the participant’s household. The University Survey Center reviewed the survey and provided expert feedback on content and clarity. The revised study instrument and study protocol were approved by the University of Wisconsin-Madison Institutional Review Board (2019-0975).
Study Settings, Recruitment, and Participants
Participants were recruited from three Midwestern middle and high schools between January and March 2020. One school distributed recruitment materials to all eligible students enrolled in a required health course. Another school distributed recruitment materials to eligible students in a medical interventions elective class and eligible students in an alternative education class made up of 11th and 12th grade students. The third school distributed recruitment packets to all students. Eligible students were categorized as enrolled in middle or high school who could speak, read, and understand English, and whose parents could read English or Spanish. Students could participate in study activities if they gave written assent, and a parent or guardian gave written consent. Parental consent was not required for students 18 years of age or older. All consent documents were translated into Spanish and were available for participants whose parents or guardians preferred Spanish versions.
Data Collection
At two schools, the survey was administered through a link that was provided to students by school administrators or the study team. Students completed the survey in a private room at school, under supervision of the study team. A paper survey was utilized at one school and data were entered into Research Electronic Data Capture (REDCap) by study team members. Study data were collected and managed using REDCap electronic data capture tools. Research Electronic Data Capture is a secure, web-based software platform designed to support data capture for research studies.34,35 Research Electronic Data Capture provides (1) an intuitive interface for validated data capture; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for data integration and interoperability with external sources.34,35 The survey took approximately 10 minutes to complete, and participants received US$10 in cash upon verification of completion.
Data Analysis
Statistical analyses of survey responses were performed using SPSS version 26. Survey questions were divided into six categories to represent key themes: Basic Knowledge of Cancer, Knowledge of Cancer Risk Factors, Attitude Toward Cancer, Likelihood to Share Knowledge About Cancer Prevention, Potentially Helpful Sources of Cancer Information, and Sources of Cancer Information. Descriptive statistics were used for participant demographics and to explore cancer knowledge, behaviors, information sources, probability of sharing learned cancer information, and preferences for educational interventions. Missing data were moved into a separate category to maximize usable data.
Three of the themes (Potentially Helpful Sources of Cancer Information, Likelihood to Share Knowledge About Cancer Prevention, and Attitude Toward Cancer) consisted entirely of Likert questions (e.g., “strongly disagree” to “strongly agree”). The Likert scales were compressed from a 5-point scale to a 3-point scale to simplify response implications; “strongly agree” and “agree” were combined into “agree” and “disagree” and “strongly disagree” were combined into “disagree,” and “slightly” and “somewhat” were combined into one category and “very” and “extremely” were combined into another. Questions within each of these themes thus range from 1 to 3 rather than 1 to 5. Likelihood to Share Knowledge About Cancer Prevention and Attitude Toward Cancer were summarized into composite scores by mean and standard deviation. Potentially Helpful Sources of Cancer Information questions were categorized by the percent of participants who would find them to be useful tools for cancer education.
Two themes (Basic Knowledge of Cancer and Knowledge of Risk Factors for Cancer) consisted of “True/False” knowledge questions, with one correct answer. Questions within each of these themes were summarized by the percent correct answers and range from 0 to 1. Composite scores were described through means and standard deviation. One theme (Sources of Cancer Information) consisted of “Yes/No” questions, indicating if a source of cancer information had been used, and were categorized by the percent of participants who had used the tool(s) for cancer education.
Responses to behavior-based questions asking about fruit, vegetable, and water consumption were grouped into two categories: “eats/drinks fruit/vegetable/water less than 1 time/day” and “eats/drinks fruit/vegetable/water at least 1 time/day.” Physical exercise responses were broken down into exercising more or less than 5 days. Tobacco and e-cigarette use consisted of “Yes/No” questions to indicate if the substance had ever been used, and alcohol use responses were categorized as “none” or “used in the past 30 days” to signify if the person had ever drunk alcohol. Sunscreen use was broken down into “none” or “use most of the time/always.” Questions within each of these themes were summarized by the percent of use/consumption and range from 0 to 1. Scores were described through means and standard deviation.
Results
A total of 235 participants took the survey. Two were removed due to incompleteness, resulting in a total of 233 surveys included for final analysis.
Demographics
Participant Characteristics Who Completed the Survey.

aThree options were presenting to participants to select for their gender; “male,” “female,” and “other.” Thus, “male” is defined as selecting “male” while not selecting other choices, and “female” is defined as selecting “female” while not selecting other choices; “other” was defined as all other combination of choices that occurred.
bIf the participant lived in more than one home, they were asked to answer regarding the home they spent the most time in. The participant was asked to not include themselves in the total number of people living in their home, under the age of 18.
cSeven different categories were available to select from for race/ethnicity, including “Black or African American,” “Hispanic or Latino,” and “White.” Participants were defined as “Black,” “Hispanic,” or “White,” if they only selected the associated category and no other selection was made; all other combinations of selects were defined as “Other.”
Basic Knowledge of Cancer
Survey Responses to Basic Cancer Knowledge, Knowledge of Cancer Risk, Attitude Toward Cancer, Likelihood to Share Knowledge About Cancer Prevention, Sources of Cancer Information, and Potentially Helpful Sources of Cancer Information.

a N = 233 unless stated in the missing category.
Knowledge of Cancer Risk Factors
Most participants could recognize the behaviors that affect cancer risk (M = .81, SD = .15), and 93% acknowledged that regular physical exams, medical screening tests, and knowledge of changes in their body could help detect early signs of cancer. Awareness of cancer risk factors was highest for tobacco use (91%), poor diet (80%), and physical activity (80%). Less commonly perceived cancer risk factors included alcohol consumption (78%) and exposure to sunlight (71%).
Attitude Toward Cancer
Of the 233 respondents, most had positive attitudes toward cancer (M = 1.48, SD = .38) and 95% reported that cancer prevention was important. However, only 50% expressed that they currently try to make decisions that will lower their chances of getting cancer, and only 37.3% stated they knew how to lower their risk of getting cancer.
Sources of Cancer Information/Potentially Helpful Sources of Cancer Information
The most reported source of cancer information was Google or other websites (72%) followed by discussions with parents (68%), and doctors (58%). Online videos (41%), educational video games (37%), and educational websites (39%) were stated as being the most helpful sources to learn about cancer and cancer prevention. Only 7% of participants reported past use of an educational game to find information about cancer; however, 82% stated they would find educational video games to be a helpful tool to learn about cancer.
Likelihood to Share Knowledge About Cancer Prevention
Participants reported a high likelihood of sharing their knowledge of cancer prevention (M = 2.27, SD = .45). The majority (93%) of respondents stated they were likely to share knowledge about cancer prevention with their family, and 92% reported a likelihood of sharing the same knowledge with their friends.
Behaviors That Affect Cancer Risk
Adolescent Behaviors That Affect Cancer Risk.

a N = 233 unless stated in the missing category.
Discussion
There are few studies examining adolescents’ perceptions about cancer and their preferences for cancer education in school settings. Current literature supports that unhealthy lifestyle factors significantly contribute to cancer diagnoses among adolescents.7,15 This study found that adolescents recognized cancer-related topics, understood basic concepts about cancer, and recognized the importance of regular physical exams and medical screenings to detect cancer, but they were unable to identify some of the most common cancer risks factors and desired more information on prevention strategies. Overall, participants reported low alcohol, tobacco, and e-cigarette use and stated that they consume fruit, vegetables, and water at least once a day. About half of the sample said they got 60 minutes of exercise during a 7-day period; however, less than half indicated that they use sunscreen when they are outside for more than an hour. Most participants reported an interest in utilizing an educational game to gain cancer knowledge and awareness. Additionally, almost all participants were interested in sharing information learned about cancer prevention with friends and family.
Knowledge and Behaviors Toward Cancer
Adolescents’ awareness regarding cancer prevention strategies is lacking. Studies from multiple countries surveying adolescents’ lifestyle choices found high reported levels of smoking, alcohol consumption, tanning bed use, poor physical activity, and low awareness of healthy eating habits.36-40 One study found adolescents in rural areas use less sun protection behaviors than in urban areas. 36 Similarly, half of the participants in this study reported they do not currently implement strategies to prevent cancer in their daily life, and few recognized which of their daily behaviors could reduce their risk of cancer. Participants desired to learn more about cancer prevention, but a disconnect existed when asking about daily behaviors around preventing cancer. Social interactions around cancer-related topics were explored in this study as well. Current literature shows teachers are primary sources of cancer-related information for adolescents, along with parents and peers. 37 While this study found internet sources to be the most frequently identified way to learn about cancer information, parents and doctors were also highly reported sources as well. Almost all participants perceived they could discuss cancer-related topics with their peers and family members.
Educational Programs and Technology
This study establishes the need for the development of technology-driven cancer prevention education programs by utilizing search engines like Google, online videos, and educational games to learn more about cancer prevention. Currently, there are limited cancer prevention education programs designed and tailored for youth in the United States schools.41-43 Other countries have developed and implemented successful instructor-led programs designed to reach adolescents.10,44-46 For example, Cancer, Educate to Prevent (CEP) was successful and effective in both educating high school students on cancer prevention and preparing their biology teachers to utilize this curriculum in schools.10,45 The Australian-based Sun Smart program incorporates technological interventions such as a media campaign, two mobile video games, and a mobile app as a component of a robust set of educational materials. The program has successfully educated elementary, middle, and high school populations on UV-radiation risk factors for skin cancer.47-50 However, few studies have evaluated a technology-based educational tool to educate adolescents on cancer-related risks and prevention in the United States. There is a need for further development of technology platforms to educate adolescents about cancer-related topics.
The HBM and Educational Interventions
The HBM suggests that people are likely to engage in preventative action(s) if they are aware of the severity of a health risk. 26 Therefore, educational interventions are most effective if they address the individual’s specific perceptions about susceptibility, benefits, barriers, and self-efficacy. Interventions focusing on this model should involve risk calculation and projection, as well as personalized education. Based on the results from this study, lack of knowledge was a barrier to cancer prevention. An educational intervention that helps adolescents recognize the most common cancer risk factors, learn about proper sunscreen use and the effect alcohol has on cancer risk, and how to incorporate more physical exercise into their daily lives is needed. Additionally, the intervention should provide adolescents with general information on cancer prevention strategies and what resources are currently available to them.
Future Directions
Educational games, also known as serious games, are video games designed not only for entertainment but also to educate, change a behavior, or create awareness of a certain issue. 51 Serious games can encourage active engagement and foster positive health behaviors.52-54 Thus, researchers and educators have the potential to effect change with a well-designed serious game targeted for adolescents. Due to their frequent use and repetitive nature, serious games are an ideal educational tool for positive health impact. They have been shown to enhance learning and reinforce content by providing immediate feedback to the player.54,55 Since adolescents are highly engaged users of digital technology, and educational games can foster positive health behaviors, there is the potential to effect change to lifestyle behaviors and habits with a well-designed serious game for adolescents. 56 Serious games are digital tools that promote positive health behaviors by offering innovative learning methods for delivering health information. 57 Using health behavior change theories to design serious games has been shown to increase positive health behaviors, including management of diabetes, asthma, cystic fibrosis, depression, cancer medication adherence, and healthy eating.58-63 While serious games have been a successful tool used to promote cancer medication adherence and healthy lifestyle choices, there are few studies that have developed and examined the effects of a theory-driven serious game to educate adolescents about cancer and how to reduce cancer risk in a school setting. Findings from this study show adolescents would find serious games to be a helpful educational tool to learn about cancer.
Future research should examine the effectiveness of a serious game intervention that incorporates the HBM and is targeted toward adolescents. Studies should use a pre-post survey design that measures knowledge gained and qualitative measures, such as interview questions, that allow the adolescent to elaborate on what they learned from the game, what questions they have after playing the game, and what else they would like to see in the game. Additionally, the game should aim to promote conversations about cancer education between adolescents and their parent/guardian and/or healthcare team.
Limitations
While the survey used for this study was created from other validated surveys and cancer curriculum, it has not been validated as a standalone survey. Furthermore, the data collected were from a predominantly white, urban, Midwestern sample which is not representative of the adolescent population in the United States or other countries. Future studies should administer the survey to a diverse, national sample of adolescents and examine how demographic characteristics affect responses. Findings would help inform researchers of adolescents’ cancer awareness perceptions, and preferences for education, as well as the health disparities and cancer understanding among minorities. Additionally, the survey should be adapted into languages other than English. Once examined, these data will allow for researchers to gain better insight on adolescents’ perceptions about cancer and guide the development of adolescent specific interventions to combat the cancer epidemic. The validated survey could also be used in schools to assess adolescents’ perceptions and knowledge before offering a cancer education session in health class.
Conclusion
A knowledge gap exists between adolescents’ cancer awareness and exposure to cancer risks, which is contributing to the number of cancer diagnoses and deaths in the United States.1,6 Education on lifestyle habits, such as eliminating tobacco use and alcohol consumption, promoting healthy eating habits, increasing exercise, and protection against sunlight exposure are necessary to inform adolescents on cancer prevention. Few studies have focused on strategies that incorporate adolescent preferences for cancer prevention topics and learning modalities. Education is needed in adolescent populations on cancer knowledge, risk factors, and prevention strategies. Technology-based interventions were desired by participants and have been successful previously in preventing unhealthy behaviors that can cause cancer.58,61,63 Future directions include the development of a game-based learning platform to provide adolescents with information on general cancer-related topics and prevention.
Supplemental Material
sj-pdf-1-ccx-10.1177_10732748211036057 – Supplemental Material for Adolescents’ Perceptions About Cancer and Preferences for Cancer Education
Supplemental Material, sj-pdf-1-ccx-10.1177_10732748211036057 for Adolescents’ Perceptions About Cancer and Preferences for Cancer Education by Olufunmilola Abraham, Claire A. Rosenberger, Sarah M. LeMay, Sarah J. Bittner in Cancer Control
Footnotes
Acknowledgments
We appreciate Lisa Szela from the University of Wisconsin-Madison (UW) School of Pharmacy for her assistance with assisting with the IRB protocol, survey development, data collection, editing the manuscript, and providing feedback throughout the writing process. We express gratitude to Erin Bailey for her assistance with data collection and data entry and Laura Stephenson previously for assisting with data cleaning and analysis. We would also like to thank Cody Fredrick for assisting with study methods, survey design, and data collection.
Authors’ Note
Written assent was obtained from participants and written consent was obtained from their parent or guardian if under the age of 18, before the survey was conducted. Participants aged 18 or older could consent without parent or guardian consent. Prior to participant recruitment and data collection, the project was approved by the University of XXX Institutional Review Board (IRB). Due to the sensitive nature of the questions asked in this study, survey respondents were assured raw data would remain confidential and would not be shared. To facilitate openness, transparency, and reproducibility of our research, we attached the full survey used for this study in ![]() . We encourage other researchers to reach out to the corresponding author with any questions they may have when reproducing our work.
. We encourage other researchers to reach out to the corresponding author with any questions they may have when reproducing our work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by American Cancer Society (ACS) grant IRG-15-213-51 and the UWCCC (University of Wisconsin-Madison Carbone Cancer Center) and by the KL2 grant KL2 TR002374-03 and grant UL1TR002373 to UW ICTR by the Clinical and Translational Science Award (CTSA) program, through the NIH National Center for Advancing Translational Sciences (NCATS). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Ethical Approval
Ethical approval was obtained from the University of Wisconsin-Madison Institutional Review Board (2019-0975).
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the University of Wisconsin-Madison Institutional Review Board (2019-0975) approved protocol.
Statement of Informed Consent
Written informed consent was obtained from the study participants or obtained from their legally authorized representative(s) for their anonymized information to be published in this article.
Abbreviations
CC&S, Cancer, Clear & Simple; HMB, Health Belief Model; REDCap, Research Electronic Data Capture.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.