
Abstract
Objectives:
We assessed the 30-day readmission rate of a privately insured population diagnosed with colorectal cancer (CRC) who had primary tumor resection in rural and urban communities.
Methods:
Claims data of people aged <65 with a diagnosis of CRC between 2012 and 2016 and enrolled in a private health plan administered by BlueCross BlueShield of Nebraska were analyzed. Readmission was defined as the number of discharged patients who were readmitted within 30 days, divided by all discharged patients. Multivariate logistic regression was used to estimate the factors associated with readmission.
Results:
The urban population had a higher readmission rate (11%) than the rural population (8%). Although the adjusted odds ratio showed that there is no difference in readmission between rural and urban residents, patients with a Charlson Comorbidity Index (CCI) of >1 were more likely than those without CCI to be readmitted (OR 3.59, 1.41-9.11). Patients with open vs. laparoscopic surgery (OR 2.80, 1.39-5.63) and those with an obstructed or perforated colon vs. none (OR 7.17, 3.75-13.72) were more likely to be readmitted.
Conclusions:
Readmission after CRC surgery occurs frequently. Interventions that target the identified risk factors should reduce readmission rates in this privately insured population.
Keywords
Introduction
Colorectal cancer (CRC) is the third most common cancer and the third leading cause of cancer mortality in the United States (US) for both women and men, with an estimated 135,430 new cases and 50,260 deaths from CRC in 2017. 1 -4 With surgery being the primary treatment approach for CRC patients, superior oncological outcomes are crucial; nonetheless, postoperative hospital readmissions occur frequently in this patient population. 5 Hospital readmissions are associated with increased morbidity, mortality, and healthcare costs. 6 -8 Determinants of preventable readmissions suggest a lack of access to quality care during the index hospitalization, a characteristic more frequent in rural areas due to limited institutional resources and the adverse characteristics of the rural population. 9 -11
Rural-urban disparities in access to quality cancer care is a worldwide phenomenon. 12 Previous research showed that a rural population and those with lower socioeconomic status (SES) were less likely to be screened, less likely to receive treatment, and at an increased risk of death following CRC diagnosis. 13 -17 Factors that predispose rural residents to experience worse cancer outcomes include the characteristics of the rural population, the institutional resources, the health behavior of rural residents, and the availability of quality cancer services. For instance, rural residents tend to be elderly and poor, lack medical help-seeking behavior due to location barriers, a characteristic associated with low follow-up on initiated treatment, and little offered treatment options. 18 In addition to the aforementioned disparities, rural residents lack access to cancer specialists such as oncologists and surgeons. 19 -21
In the United States, the annual readmission rate for the 600,000 cases of colorectal surgery range between 9% and 25%. 5,8,22 Factors associated with readmissions are age, sex, race, SES, insurance type, deprivation score, comorbidities, immunosuppressant use, the severity of illness, surgical approach (open vs. laparoscopic), procedure type and urgency, operation time, length of stay (LOS), complications, non-home discharge, blood transfusion around the time of surgery, postoperative steroids and stoma. 5 Most prior research related to hospital readmission rates for patients receiving surgery for CRC has not examined differences between rural and urban populations. Of those that considered rurality, some did not investigate patients <65 or privately insured population, and others instead were limited to a single institution or used a Medicare population. 23 -29 There is a paucity of population-based studies of rural-urban differences that include people under 65 years of age. In contrast to the overall US population, where 20%-25% of people live in rural areas, 35% of the population of Nebraska lives in rural areas. 10
The objective of the study was to measure the rate of hospital readmission of patients after surgical resection of CRC, using data from a privately insured population of people <65 years of age. BlueCross BlueShield of Nebraska data captures information about patients’ diagnoses and procedures, which can be used to derive comorbidities and complications. We wanted to compare the frequency of readmissions following CRC surgery between rural and urban populations and identify factors associated with a higher likelihood of readmission after CRC. Therefore, we hypothesized that rural patients, those with higher comorbidities, underwent open surgery, presented with an obstructed or perforated colon, discharged with a stoma, and with a higher length of stay at the hospital were more likely to get readmitted within 30 days of their index surgery compared to their counterparts.
Methods
Data Sources
We designed a retrospective cohort study using data from BlueCross BlueShield of Nebraska (BCBSNE). BCBSNE is a large private health insurer covering more than 700,000 individuals in Nebraska. 30 Data consists of claims from inpatient, professional and outpatient services. The data also contains members’ demographic information that includes age, gender, member, and provider 5-digit ZIP codes. BCBSNE captures the member’s enrollment information, which consists of the beginning and ending date of coverage and the beginning and ending date of services. Diagnosis and procedural codes for inpatient, outpatient, and professional services were all available from their claims data warehouse.
Study Population
Participants included in this study were members of BCBSNE between January 1st, 2012, and June, 30th 2016, who were 19-64 years old, enrolled with BCBSNE for the entire year, and who were diagnosed with CRC. The International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis codes, and ICD-10-CM diagnosis codes were used (See supplementary material S1 for the codes used to identify the diagnosis of CRC). 31 Figure 1 shows eligibility criteria. Patients were diagnosed with CRC if they had at least one inpatient or 2 outpatient claims with a primary diagnosis of CRC at 2 different visits. 32 We excluded members >65 since BCBSNE data did not contain claims for all of their Medicare-covered health services. We also excluded members with no surgery claims 1 month before CRC diagnosis or within 6 months after the diagnosis. See supplementary material S2 for the codes used to identify CRC surgery. Additionally, members with no admission or discharge records were also excluded.
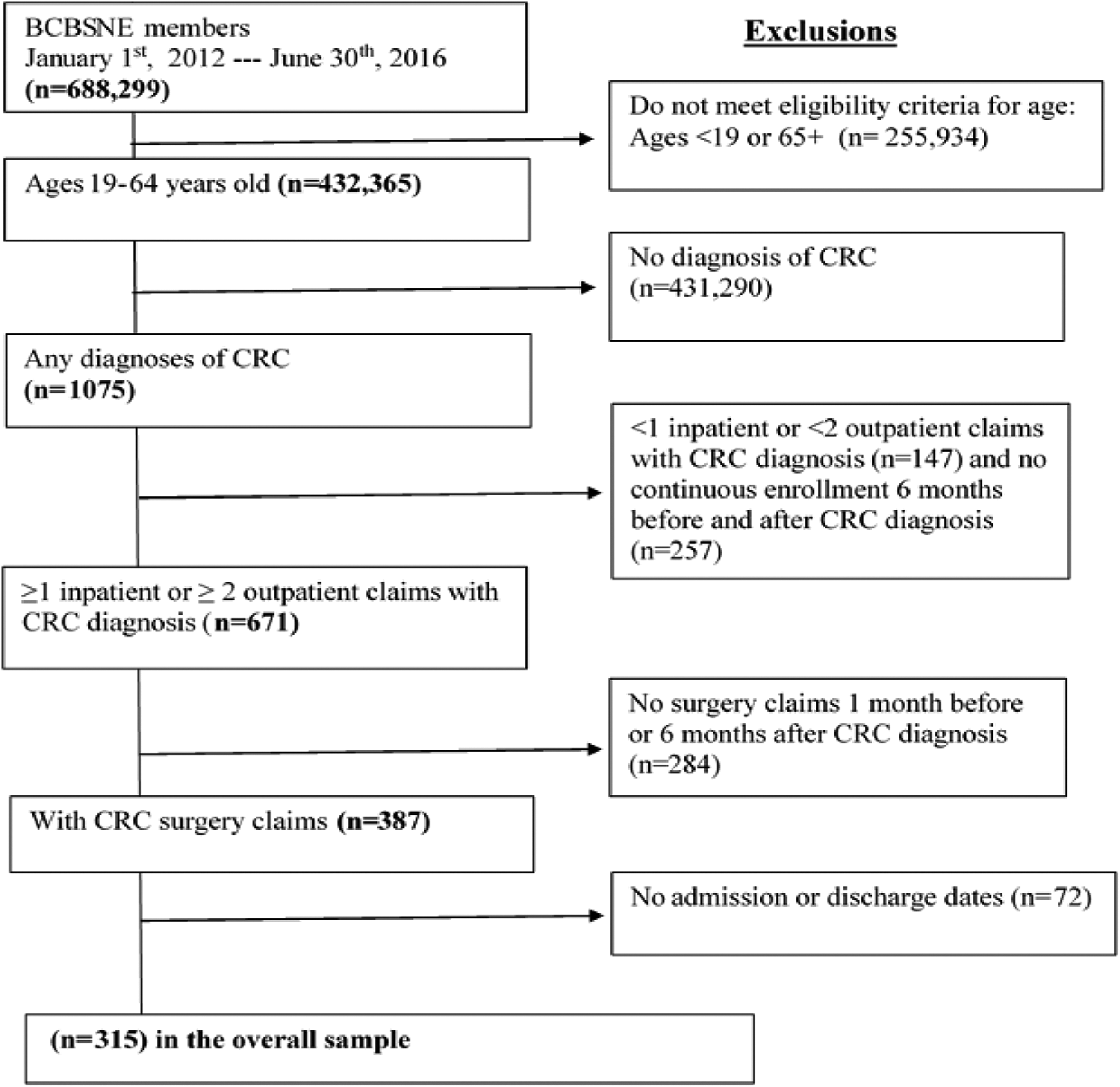
Eligibility criteria for the study population.
Study Variables
Patient characteristics
We used the enrollment file to extract the beginning and ending dates of coverage and services. Patient demographics, including age, gender, and 5-digit ZIP code of residence, were derived from the claims file. Utilization and clinical variables were extracted from the international classification of disease fields and current procedural terminology fields from the claims file.
The updated Charlson Comorbidity Index (CCI) was used to determine the burden of disease and case-mix. 33,34 The index contains a comprehensive list of 17 comorbid conditions developed by Charlson et al and recently updated by Quan et al.
Travel time measurements were described previously. 31 Briefly, travel time was computed by measuring the time in minutes between the member and provider ZIP codes at the date of surgery. The provider’s ZIP code was defined as the place where the operation took place on the date of the index surgery, and the member’s ZIP code as that for their place of residence when receiving the operation. Travel times to surgical treatment were obtained using an open-source SAS program that makes repeated calls to Google to get travel time information for any number of locations. 35,36 Studies have found a high correlation of Google maps with straight-line distance (r2 = 0.96) but with superior travel time estimates. We measured travel time as both continuous variable and as 4 categories based on quartile distribution.
Rural-Urban Status Measurement
A patient’s “index” surgery was designated as the first time a patient had surgery within 1 month before or 6 months after their CRC diagnosis. The surgery was the basis on which both members’ and providers’ ZIP codes were defined to calculate the travel time. The provider’s ZIP code was defined as that on the date of the index surgery, and the member’s ZIP code as that for their place of residence when receiving the index surgery.
For the rural-urban status definition, we used the Rural-Urban Commuting Area (RUCA) codes to assign each member’s residential status based on their residential ZIP code. Subsequently, we used these codes to classify members by rural-urban status using “Categorization C,” as suggested by the publisher. 37 This categorization combines RUCA codes into urban and rural codes. The urban codes consist of a metropolitan area core, micropolitan or small-town high-commuting areas, or rural areas with a secondary commuting flow of 30% to 49% within an urban area. The rural codes consist of a micropolitan area core with a secondary flow of 10% to 29% to an urban area, small-town, low-commuting areas, or rural areas with commuting to urban cluster areas.
Outcome Variables
CRC surgery was defined as the resection of the primary tumor with or without stoma creation within 1 month before or 6 months after the CRC diagnosis. We applied this definition to patients with 6 months of continuous enrollment before and after CRC diagnosis (1 year of continuous enrollment) to ensure that we are not missing surgeries conducted after systemic therapy according to guidelines (i.e., surgery after neoadjuvant therapy). 38 The codes used to identify surgeries (Appendix A) were selected in consultation with a surgeon and a trained coder, as well as previous publications. 5,29,39 -41 The 30-day readmission was defined as the number of discharged patients who were readmitted within 30 days, divided by the number of people discharged. Operationally, we used the inpatient records and admission and discharge dates to measure hospital readmission. The same definition has been used in previous publications. 8,24,25,29,39,40,42 -44
Data Analysis
Patient characteristics including age, gender, rural-urban status, travel time, LOS, and CCI were compared between readmitted and non-readmitted groups using a student t-test for continuous variables and the Chi-square (X2) test for categorical variables. The same tests were used to compare readmitted and non-readmitted patients according to the surgery characteristics, including tumor location, surgery site, and approach, whether a patient has an intestinal obstruction or perforation and whether a patient required a stoma. Wald tests were used to assess the predictors’ significance. The fractional polynomial method was used to examine non-linear relationships between the log odds of readmission and the continuous variables. 45 We inspected the curves of the predictors against the dichotomous response and used the likelihood ratio test for improvement in fit against the assumed linear relationship. We performed univariate analysis to assess the relationship between each independent variable and readmission rates, with variables that have P-value <0.25 added to the multivariate model. At the multivariate analysis, were performed backward elimination to eliminate non-significant variables (P > 0.05) with the final model adjusting for the surgical approach, the presence of intestinal obstruction or perforation, and CCI. There were no interactions between rural-urban status and independent variables. All tests were 2-sided and using α = 0.05. SAS statistical software version 9.4 (SAS Institute Inc. Cary, NC) was used to conduct all analyses. This study, with its fully anonymized data, was approved by the University of Nebraska Medical Center Institutional Review Board (IRB# 366-1).
Results
The application of the inclusion and exclusion criteria resulted in a cohort of 315 patients with CRC surgery claims (Figure 1).
Table 1 shows the characteristics of the study members who had CRC surgery by their hospital readmission status. The urban population (11%) had a higher readmission rate than the rural population (8%). Readmitted patients presented with more comorbidities compared to non-readmitted patients. Mean travel times were very similar between the readmitted (mean = 27.69 min) and non-readmitted (mean = 27.92 min) groups. Overall, 25% traveled a maximum distance of 7.5 miles, 50% traveled a maximum of 19 miles, and 75% traveled a maximum of 35 miles. While the median distance traveled by rural patients was 33.02 miles, urban patients traveled a median of 10.16 miles to get to a hospital.
Patient Characteristics by 30-Days Readmission Status, BCBSNE 2012-2016 (N = 315).
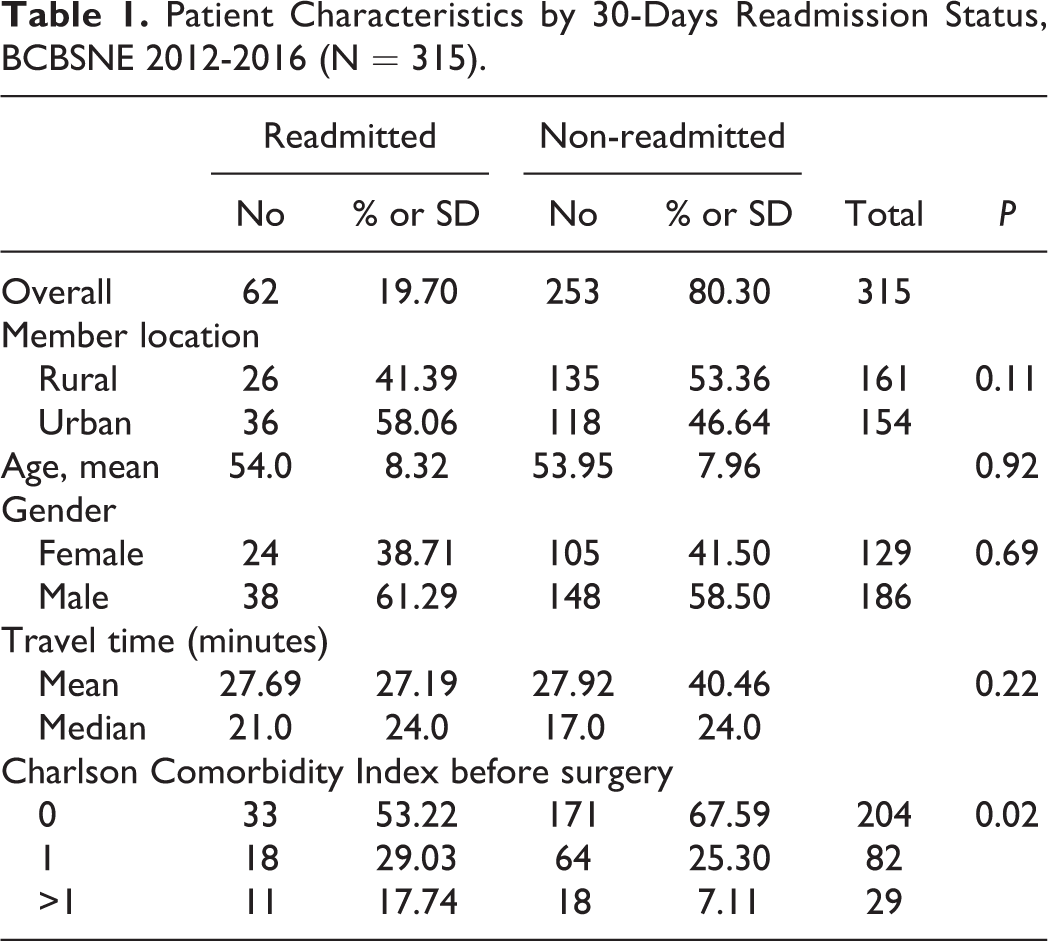
Table 2 displays the surgery characteristics according to readmission status. The majority of the surgical procedures (77%) of readmitted patients were open surgery, compared to half of the surgical procedures of the non-readmitted patients. The majority of surgical procedures among readmitted patients were performed on patients who had intestinal obstruction or perforation before surgery and who had no stoma.
Index Surgery Characteristics by 30-Days Readmission Status, BCBSNE 2012-2016 (N = 315).

Table 3 shows the results of the multivariate analysis for the association between rural-urban status and 30-day readmission rates. Compared with patients who had no comorbidities, patients with >1 comorbid condition had 3.59 (95% CI, 1.41-9.11) higher odds of being readmitted within 30-day of the index surgery. Patients who had open surgery during the index admission had 2.80 (95% CI, 1.39-5.63) higher odds of being readmitted within 30-days compared to patients who had laparoscopic surgery. Patients who presented with intestinal obstruction or perforation during their index admission had 7.17 (95% CI, 3.75-13.72) higher odds of getting readmitted within 30-day of the index surgery compared with those without such symptoms. We found no significant difference in 30-day readmission between BCBSNE members who live in rural vs. urban areas.
Univariate and Multivariate Analysis of Risk Factors for 30-Day Readmission, BCBSNE 2012-2016.
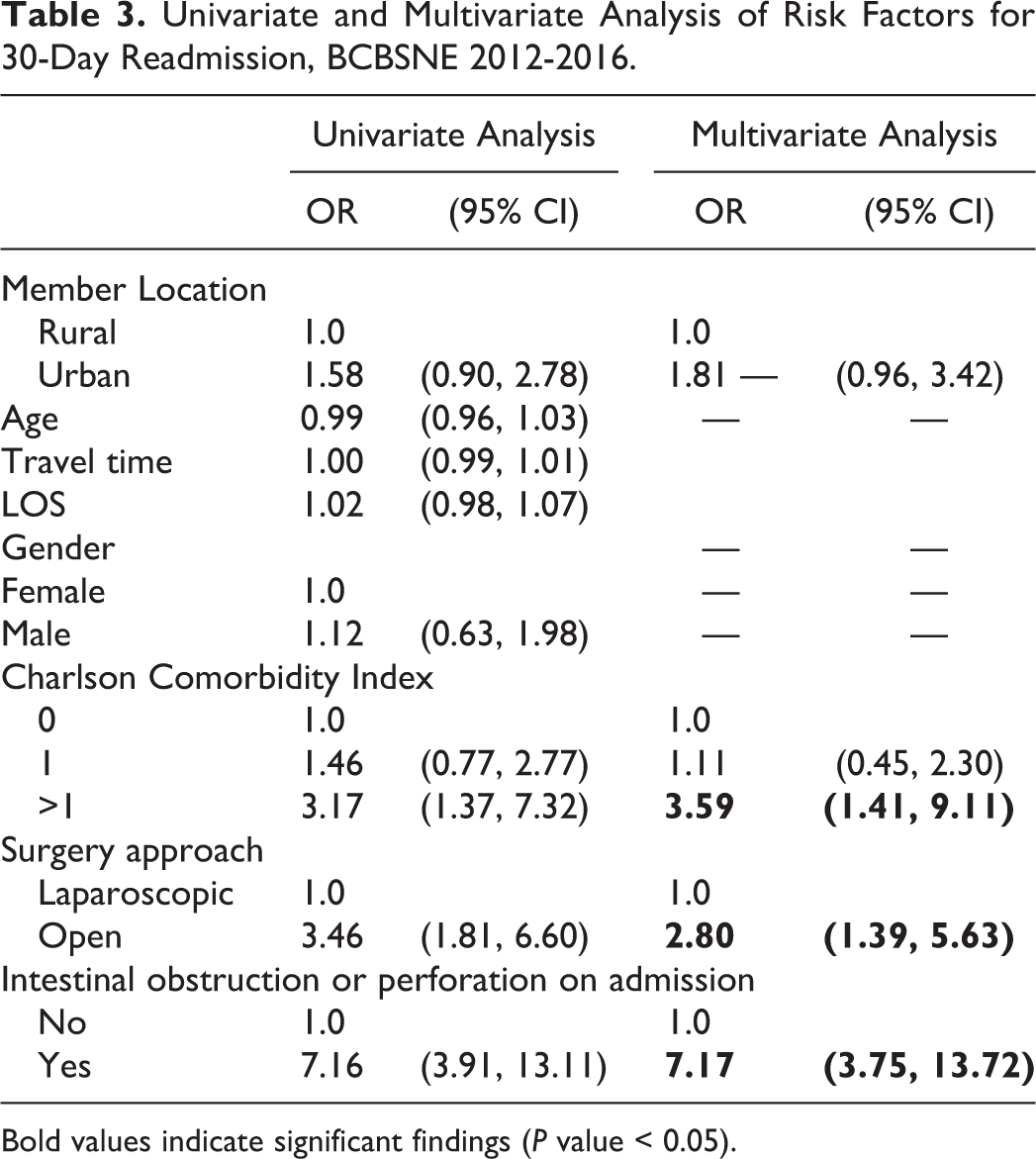
Bold values indicate significant findings (P value < 0.05).
Discussion
The retrospective cohort study of the privately insured adults who had CRC and treated surgically from January 2012 to June 2016 resulted in a readmission rate of 11% in urban population and 8% in the rural population. The consequences of readmission can be detrimental since patients who are readmitted within 30 days of the index surgery have 2.44 increased odds of mortality than those who were not readmitted. 40 Our finding is comparable to previous studies that reported readmission rates ranging between 9% and 25%. 8,22,41 The discrepant results in readmission rates, evidenced by a wide readmission range, could be because of the differences in the time of surgical complications (e.g., complications that occurred during the index surgery or postdischarge) or differences in the time of readmission. 42 Alternatively, differences in readmission rates could also be partly due to different definitions used for hospital readmission. For example, the National Surgical Quality Improvement Program (NSQIP) uses a clinical reviewer to check medical records for postoperative complications derived from readmission and handles phone calls to follow up with patients. However, the University Health System Consortium (UHC) database is a discharge billing data set that is limited to inpatient records. 5 Another difference is that the NSQIP defines readmission starting from the date of surgery, while UHC uses the day after discharge. 5
In the current study, the rural-urban status was not a predictive factor for 30-day hospital readmission. This finding is similar to a study conducted with the Medicare population that found no differences between the rural and urban populations in the 30-day readmission rate. 40 Still, it is dissimilar to others, which found that the rural population is more likely to get readmitted. 43 , 46 For instance, a study conducted with the Veteran Affairs (VA) patients 65 years and older found that rural patients were more likely to be readmitted within 30-days and indicated that the findings reflect the low quality of care for patients treated at rural hospitals. Additionally, a study conducted in Nebraska found that the rural population is 40% less likely than urban to receive a laparoscopic colectomy, a procedure associated with improved postoperative patient outcomes. 11
Since the introduction of laparoscopic CRC surgery in 1991, 47,48 the association between laparoscopic CRC surgery vs. open approach and the decreased readmission rates has been controversial. The impact of the surgical approach on the risk of hospital readmission after CRC surgery is somewhat anticipated. Although the laparoscopic procedure is associated with a longer operation time, several studies have found that the minimally invasive laparoscopic approach is associated with favorable outcomes, including lower readmission rates. 41,49 As a result, there has been an increase in the utilization of laparoscopy during CRC surgery (37% in 2008 and 44% in 2011). 50 Additional favorable outcomes associated with laparoscopy use are lower postoperative pain, shorter duration of ileus, improved pulmonary function, better overall quality of life during the 30 days postoperatively, and lower postoperative LOS. 49 The latter is associated with lower 30-day hospital readmission; in the current study, we found near-significant higher LOS among readmitted patients (P = 0.07).
The risk factors of 30-day readmission identified in this study include the use of an open surgery approach. Our research found that patients who had open surgery had 2.8 the odds of being readmitted to the hospital within 30 days of the index surgery compared to those who had laparoscopic surgery, 2.8 (95% CI: 1.39, 5.63). Congruent with our findings, Damle et al assessed the association between the surgery approach and 30-day readmission and found that patients who had open surgery to be 24% more likely to get readmitted compared to those with laparoscopic surgery, 1.24 (95% CI: 1.17, 1.31). 39 Likewise, Bartlett et al found that patients who had laparoscopic surgery to be less likely to be readmitted, 0.90 (95% CI: 0.85, 0.96). 42 However, other studies reported non-significant findings. 24,51,52 Accordingly, given that the higher the use of laparoscopy, the lower the LOS, and subsequently, the lower the hospital readmission, the evidence suggests an association between laparoscopic use and lower readmission rate.
Another risk factor that has been identified in this study was poor baseline health or comorbidities. We found that patients with >1 CCI score to be 3.59 more likely to be readmitted to the hospital within 30 days after the index surgery. Several studies from diverse populations found that the higher the comorbidity, the higher the likelihood of readmission. 42,43,53,54 Comorbidity is associated with higher mortality, lower quality of life, and higher complications of treatment. 55 For instance, Greenblatt and colleagues found that patients with comorbidities were 14% more likely to be readmitted within 30 days of discharge and were 27% more likely to die within 1 year of discharge. 40
We also found that 24% of readmitted patients had an obstructed or perforated bowel at the time of the index surgery. This finding is slightly higher than some studies. 56 but similar to others. 57,58 Part of the differences could be different age groups among these studies. Patients with obstructed or perforated bowel were 7.17 more likely to be readmitted to the hospital within 30 days after the index surgery, which is similar to some studies that found worse outcomes associated with patients presented with an obstructed or perforated tumor. 29,40
Previous studies showed a positive association between surgical outcomes and undergoing surgery at high surgery volume hospitals or by high volume surgeons. 21,59 -64 While we did not measure surgery volume in this privately insured young population, we noticed that travel time was not significantly different between the readmitted and non-readmitted patients, and the majority of patients (75%) did not exceed 35 miles. Given the higher frequency of colon cancer surgeries (less complex surgery) in the state than rectal cancer surgery (supplementary materials, S3 and S4), the lack of differences in travel time and readmission could be related to more frequent colon cancer surgery in the state. Future studies should elaborate on the surgery volume and its impact on cancer outcomes. This result is consistent with previous findings, 6,21,64 which showed that the distance traveled for CRC surgeries ranges between 1.9 and 9.3 miles among medium-volume hospitals. At high-volume hospitals, the distance was between 2.9 and 24.5 miles. Accordingly, among this rural population, some of the patients did not mind traveling more than 35 miles to undergo surgery and, therefore, did not consider traveling as a barrier to receiving surgery. Although having surgeries at high volume hospitals is associated with better outcomes, especially among rectal cancer patients, referral patterns are strong contributing factors to surgical outcomes. 65
A strength of the current study is the use of privately insured populations who are less represented in prior studies. For instance, despite its nationwide representation, limitations of Medicare data include restricting the population to adults over 65 years of age and including only fee-for-service Medicare beneficiaries. On the other hand, some limitations should be considered when interpreting the findings. First, our sample is relatively small compared with some prior publications. Second, hospital surgery volumes were not measured in the current study, and therefore we were unable to adjust for it in the analysis. Although hospital volume was associated with mortality, it is not associated with readmission rates. 66 Third, the studied population is limited to patients with private insurance from Nebraska. Therefore, our results may not be generalized to communities located in different states or with different types of insurance, those underinsured or uninsured. Nevertheless, Nebraska residents resemble the population of other rural states. 9,10 Fourth, prior studies show that SES is proportionally associated with access to health services use. 67 Our privately insured population tends to be of higher SES compared to populations without private insurance, so while we could not examine SES as a predictor variable, we could minimize the impact of the access to insurance component of SES on our results. Fifth, our data lacks detailed information about patients’ complications and disposition postdischarge; therefore, they were not investigated in this study. Moreover, we acknowledge the lack of data regarding postoperative complications and surgical infection in this privately insured population. Lastly, it is possible that the study is underpowered to find an association between rural-urban status and hospital readmission.
Considering our findings, a state-wide quality initiative should be implemented. First, access to care during the postdischarge period among patients with a high risk of readmission should be facilitated. For example, in our study, we found that patients with ≥2 comorbidities were more likely to be readmitted. Accordingly, payers should waive copayments for outpatient visits during 30-60 days of discharge for patients with ≥2 comorbidities, even among out-of-network providers. Second, providers should prioritize appointments for the said patients to facilitate timely treatment, avoid delayed appointments, and possibly prevent readmission. Third, access to multidisciplinary quality care is essential to monitor patients during the postdischarge period. For instance, patients with comorbidities are usually prescribed polypharmacy (e.g., anticoagulants, antihypertensive, or treatment to other chronic diseases) and thus in need of postdischarge medications’ management.
Conclusions
The rate of readmission after CRC surgery is common among the young privately insured population. To reduce readmission in a privately insured population, the identified risk factors should be targeted for interventions. For instance, patients present with comorbidities or those admitted with an obstructed colon at the index hospitalization should undergo frequent outpatient follow up after discharge to minimize the chance of readmission. Additionally, enhanced use of laparoscopic surgery, especially in rural areas, should be implemented. It is also possible that the rural population who are privately insured might have more access to quality care compared to the rural population with no private insurance.
Supplemental Material
Supplemental Material, sj-pdf-1-ccx-10.1177_10732748211027169 - Comparison of Urban-Rural Readmission Rates After Colorectal Cancer Surgery: Findings From a Privately Insured Population
Supplemental Material, sj-pdf-1-ccx-10.1177_10732748211027169 for Comparison of Urban-Rural Readmission Rates After Colorectal Cancer Surgery: Findings From a Privately Insured Population by Mesnad Alyabsi, Mary Charlton, Jane Meza, K. M. Monirul Islam, Amr Soliman and Shinobu Watanabe-Galloway in Cancer Control
Footnotes
Authors’ Note
Mesnad Alyabsi, Mary Charlton, Jane Meza, K. M. Monirul Islam, Amr Soliman, and Shinobu Watanabe-Galloway contributed equally to this work. Our study was approved by The University of Nebraska Medical Center Institutional Review Board (IRB# 366-1). All patients provided written informed consent prior to enrollment in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
ICD/CPT Codes Used in Identifying the Colorectal Cancer Surgery.

| ICD/CPT | Description |
|---|---|
| 4571/0dbe0zz,0dbe3zz,0dbe7zz, 0dbe8zz | Open Multi-Segment Resection of Large Intestine |
| 4572/0dth0zz, 0dth7zz, Dth8zz | Open Cecectomy Nec |
| 4573/0dtf0zz, 0dtf7zz, 0dtf8zz, 0dtk0zz | Open Right Hemicolectomy Nec |
| 4574/0dtl0zz, 0dtl7zz, 0dtl8zz | Open Transverse Colon Res Nec |
| 4575/0dtg0zz, 0dtg7zz, 0dtg8zz | Open Left Hemicolectmy Nec |
| 4576/0dtn0zz, 0dtn7zz, 0dtn8zz | Open Sigmoidectomy Nec |
| 4579 | Partial Large Intestine Excision NEC/NOS |
| 4581/0dte4zz | Laparoscopic Total Intra-Abdominal Colectomy |
| 4582/0dte0zz | Open Total Intrabdominal Colectomy |
| 4583/0dte7zz, 0dte8zz | Total Abdominal Colectomy Nec/Nos |
| 1731/0dbe4zz | Laparoscopic Multi-Segment Resection Large Intestine |
| 1732/0dth4zz | Laparoscopic Cecectomy |
| 1733/0dtf4zz | Laparoscopic Right Hemicolectomy |
| 1734/0dtl4zz | Laparoscopic Resection Transverse Colon |
| 1735/0dtg4zz | Laparoscopic Left Hemicolectomy |
| 1736/0dtn4zz | Laparoscopic Sigmoidectomy |
| 1739/0dbe4zz | Laparoscopic Partial Excision Large Intestine Nec |
| 44140 | Colectomy Partial W/Anastomosis |
| 44141 | Colectomy Partial W/Skin Level Cecostomy/Colostomy |
| 44143 | Colectomy Partial W/End Colostomy & Closure of Distal Segment |
| 44144 | Colectomy Partial W/ Colostomy /Ileostomy & Mucofistula |
| 44145 | Colectomy Partial W/Coloproctostomy |
| 44146 | Colectomy Partial W/Coloproctostomy & Colostomy |
| 44147 | Colectomy Partial Abdominal & Transanal Approach |
| 44150 | Colectomy Total Abdominal W/O Proctectomy W/ Ileostomy |
| 44151 | Colectomy Total Abdominal W/O Proctectomy W/Continent Ileostomy |
| 44155 | Colectomy Total Abdominal W/Proctectomy W/Ileostomy |
| 44157 | Colectomy Total Abdominal W/Proctectomy Ileoanal Anastomosis |
| 44158 | Colectomy Total Abdominal W/ Proctectomy Ileoanal Anastomosis & Reservoir |
| 44160 | Colectomy Partial W/Removal Terminal Ileum & Ileocolostomy |
| 44204 | Laparoscopic Colectomy Partial W/Anastomosis |
| 44205 | Laparoscopic Colectomy Partial W/ Removal Terminal Ileum |
| 44206 | Laparoscopic Colectomy Partial W/End Colostomy & Closure of Distal Segment |
| 44207 | Laparoscopic Colectomy Partial W/Coloproctostomy Low Pelvic Anastomosis |
| 44208 | Laparoscopic Colectomy Partial W/ Coloproctostomy Low Pelvic Anastomosis W/Colostomy |
| 44210 | Laparoscopic Colectomy Total W/O Proctectomy W/Ileostomy/Ileoproctostomy |
| 44211 | Laparoscopic Colectomy Total Abdominal W/Proctectomy Ileoanal Anastomosis |
| 44212 | Laparoscopic Colectomy Abdominal W/Proctectomy W/Ileostomy |
| 44145 | Colectomy Prtl W/Coloproctostomy |
| 44146 | Colectomy Prtl W/Coloproctostomy & Colostomy |
| 44147 | Colectomy Prtl Abdominal & Transanal Approach |
| 44155 | TPC—Total Proctocolectomy, Ileostomy Includes Stoma |
| 44156 | TPC—Total Proctocolectomy, Continent Ileostomy Includes Stoma |
| 44157 | TPC, IAA—Ileo-Anal Anastomosis, Straight With or Without Stoma, Code Stoma Separately When Done |
| 44158 | TPC, IPAA—Ileal Pouch-Anal Anastomosis |
| 44207 | Laps Colectomy Prtl W/Colopxtstmy Lw Anast |
| 44208 | Laps Colectomy Prtl W/Colopxtstmy Lw Anast W/Clst |
| 44211 | Laps Colct Ttl Abd W/Prctect Ileoanal Anastomosis |
| 44212 | Laparoscopic TPC—Total Proctocolectomy, Includes Stoma |
| 44238 | Unlisted Laparoscopy Procedure, Intestine |
| 45499 | Unlisted Laparoscopy Rectum |
| 45110 | Proctectomy, APR, Colostomy Includes Stoma |
| 45111 | Prctect Prtl Rescj Rectum Tabdl Appr |
| 45112 | Prctect Cmbn Abdominoprnl Pull-Thru Px |
| 45113 | Prctect Prtl W/Mucosec Ileoanal Anast Rsvr |
| 45114 | Proctectomy, Combined Abdominal And Transsacral Approach With or Without Stoma |
| 45116 | Proctectomy, Partial, Parasacral (Kraske or York-Mason Approach) Anorectal Procedures Transanal Excision |
| 45119 | Prctect Cmbn Pull-Thru W/Rsvr W/Ntrstm |
| 45120 | Prctect Compl W/Pull-Thru Px & Anastomosis |
| 45121 | Proctocolectomy, For Congenital Megacolon, Including Total Colectomy With Pull-Through (Eg, Swenson, Duhamel, or Soave) With or Without Stoma, Code Stoma Separately When Done |
| 45123 | Prctect Prtl W/O Anast Prnl Appr |
| 45126 | Pelvic Exenteration For Colorectal Malignancy, With Proctectomy (With or Without Colostomy), With Removal of Bladder And Ureteral Transplantations, And Hysterectomy, or Cervicectomy, With or Without Removal of Tube(S), With or Without Removal of Ovary(S), |
| 45160 | Exc Rct Tum Proctotomy Transsac/Transcoccyge |
| 45170 | Excision of Rectal Tumor, Transanal Approach CPT Expanded |
| 45171 | Exc Rct Tum Not Incl Muscularis Propria |
| 45172 | Exc Rct Tum Incl Muscularis Propria |
| 45190 | Destruction Rectal Tumor Transanal Approach |
| 45395 | Proctectomy, APR, Colostomy, Laparoscopic Includes Stoma |
| 45999 | Unlisted Procedure, Rectum (Open) |
| 45397 | Laps Proctectomy Combined Pull-Thru W/Reservoir |
| 483 | Local Excision or Destruction of Lesion or Tissue of Rectum |
| 4831 | Radical Electrocoagulation of Rectal Lesion or Tissue |
| 4832, 0d5p0zz, 0d5p3zz,0d5p4zz, 0d5p7zz, 0d5p8zz | Other Electrocoagulation of Rectal Lesion or Tissue |
| 4833 | Destruction of Rectal Lesion or Tissue By Laser |
| 4834 | Destruction of Rectal Lesion or Tissue By Cryosurgery |
| 4835, 0dbp3zz, 0dbp7zz, 0dbp8zz | Local Excision of Rectal Lesion or Tissue |
| 4836, 0dbp4zz, 0dbp8zz | [Endoscopic] Polypectomy of Rectum |
| 4840,0dtp0zz, 0dtp4zz | Pull-Through Resection of Rectum, Not Otherwise Specified |
| 4841 | Soave Submucosal Resection of Rectum |
| 4842, 0dtp4zz | Laparoscopic Pull-Through Resection of Rectum |
| 4843, 0dtp0zz | Open Pull-Through Resection of Rectum |
| 4849, 0dtp0zz, 0dtp4zz | Other Pull-Through Resection of Rectum |
| 4850, 0dtp0zz, 0dtp4zz, 0dtp7zz, 0dtp8zz, 0d1n0z4 | Abdominoperineal Resection of the Rectum, Not Otherwise Specified |
| 4851, 0dtp4zz, 0d1n0z4 | Laparoscopic Abdominoperineal Resection of the Rectum |
| 4852, 0dtp0zz, 0d1n0z4 | Open Abdominoperineal Resection of the Rectum |
| 4859, 0dtp7zz, 0dtp8zz, 0d1n0z4 | Other Abdominoperineal Resection of the Rectum |
| 486 | Other Resection of Rectum |
| 4861 | Transsacral Rectosigmoidectomy |
| 4862, 0dtp0zz, 0dtp4zz, 0d1n0z4, 0d1n4z4 | Anterior Resection of Rectum With Synchronous Colostomy |
| 4863, 0dtp0zz, 0dtp4zz | Other Anterior Resection of Rectum |
| 4864 | Posterior Resection of Rectum |
| 4865 | Duhamel Resection of Rectum |
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.