
Abstract
Background:
Colorectal cancer (CRC) disproportionately affects Vietnamese Americans, especially those with low income and were born outside of the United States. CRC screening tests are crucial for prevention and early detection. Despite the availability of noninvasive, simple-to-conduct tests, CRC screening rates in Asian Americans, particularly Vietnamese Americans, remain suboptimal. The purpose of this study was to evaluate the interplay of multilevel factors – individual, interpersonal, and community – on CRC screening behaviors among low-income Vietnamese Americans with limited English proficiency.
Methods:
This study is based on the Sociocultural Health Behavior Model, a research-based model that incorporates 6 factors associated with decision-making and health-seeking behaviors that result in health care utilization. Using a community-based participatory research approach, we recruited 801 Vietnamese Americans from community-based organizations. We administered a survey to collect information on sociodemographic characteristics, health-related factors, and CRC screening-related factors. We used structural equation modeling (SEM) to identify direct and indirect predictors of lifetime CRC screening.
Results:
Bivariate analysis revealed that a greater number of respondents who never screened for CRC reported limited English proficiency, fewer years of US residency, and lower self-efficacy related to CRC screening. The SEM model identified self-efficacy (coefficient = 0.092, P < .01) as the only direct predictor of lifetime CRC screening. Educational attainment (coefficient = 0.13, P < .01) and health beliefs (coefficient = 0.040, P < .001) had a modest significant positive relationship with self-efficacy. Health beliefs (coefficient = 0.13, P < .001) and educational attainment (coefficient = 0.16, P < .01) had significant positive relationships with CRC knowledge.
Conclusions:
To increase CRC screening uptake in medically underserved Vietnamese American populations, public health interventions should aim to increase community members’ confidence in their abilities to screen for CRC and to navigate associated processes, including screening preparation, discussions with doctors, and emotional complications.
Keywords
Introduction
Colorectal cancer (CRC) is a malignancy that originates in the colon or rectum 1 and that almost always develops from precancerous polyps in these tissues. 2 In the United States, of cancers that affect both men and women, CRC is the third most commonly diagnosed malignancy, excluding skin cancer, 3 and is the second leading cause of cancer death. 4 In 2020, the estimated incidence is 147,950 new CRC cases and 53,200CRC deaths were reported in the United States. 5 CRC screening tests are crucial in preventing CRC and in reducing CRC death, owing to their ability to: (1) detect precancerous polyps, enabling timely polyp removal, and (2) detect CRC in its early stages, when treatment is most effective. 2 The US Preventive Services Task Force (USPSTF) recommends CRC screening for adults ages 50 to 75. 2 The USPSTF recommends several types of CRC screening, including stool tests, colonoscopy, flexible sigmoidoscopy, and CT colonography (virtual colonoscopy). Stool tests, which check stool samples provided by patients for signs of cancer and which include guaiac-based fecal occult blood test (gFOBT), fecal immunochemical test (FIT), and FIT-DNA test, 6 are noninvasive and relatively straight-forward. 6 USPSTF recommends that gFOBT and FIT be performed annually, with FIT-DNA recommended once every 1 to 3 years. 6
Within the United States generally, CRC screening rates have increased progressively in recent years. National data indicate that 68.8% of adults aged 50 to 75 were up-to-date with CRC screening in 2018. 3 However, disparities still persist in racial and ethnic minority and medically underserved populations. 7 According to data from the 2015 National Health Interview Survey (NHIS), among adults age 50 or older, CRC screening rates were much lower for Asian (49%), Hispanic (50%), and American Indian/Alaska Native (AI/AN) (54%) adults compared to White (65%) and Black (62%) adults. Screening was lowest among the uninsured (25%) and among immigrants who had resided in the United States for fewer than 10 years (34%). 8
Asian Americans, particularly Vietnamese Americans, are disproportionately affected by CRC. 7 For Vietnamese Americans, CRC is the third highest cause of cancer-related mortality, accounting for 7.9% of all cancer-related deaths in men and 9.6% in women, according to data from the 2003–2011 National Center for Health Statistics (NCHS). 9 Among adults aged 50 to 79, only 52.7% of Asian Americans had any CRC test or procedure, much lower than the rate of 65.4% for non-Hispanic whites. 10 Regional studies found that CRC screening rates ranged from 33 to 61% in populations of community-dwelling Vietnamese Americans aged 50 to 79 in California (52%), 11 Washington (52% for men, 61% for women), 12 and Minnesota (33.1%). 13 These rates lag significantly behind the target CRC screening rate of 70.5% set by Healthy People 2020. 14 Among Asian American ethnicities, Vietnamese Americans had higher levels of unemployment (10.6%) and low levels of socioeconomic status in a 2013 report conducted by John Logan and Weiwei Zhang. 15 The previously conducted regional studies also identified low levels of educational attainment, English-speaking proficiency and self-rated health among Vietnamese American participants. 11 -13
Studies have attempted to identify individual-, interpersonal-, and community-level facilitators and barriers to CRC screening in Vietnamese American communities. In particular, CRC screening uptake in these communities is associated with individual-level demographic characteristics, social determinants of health (such as educational attainment), access to healthcare, and English proficiency. 12,16 -20 In addition, psychosocial factors, such as CRC-related knowledge or attitudes, perceived risks or susceptibility, and self-efficacy, 21 also have been found to be related to CRC screening behavior and other cancer prevention behaviors among Vietnamese Americans. 22 -27 Furthermore, research suggests that social support and social norms play an important role in motivation and intention for CRC screening. 12,17,28
Figure 1 represents the Sociocultural Health Behavior Model (SCHBM) that identifies and describes relationships and interactions between the various factors that guide health behavior. 29 -31 The SCHBM, a research-based model developed by the primary author (Grace X. Ma), incorporates 6 factors associated with decision-making and health-seeking behaviors that result in health care utilization. These factors include: (1) predisposition (e.g., educational attainment), (2) cultural influences (e.g., health beliefs), (3) needs (e.g., hierarchy of health care), (4) enabling influences (e.g., health insurance coverage), (5) environmental/health systems (e.g., availability of healthcare resources), and (6) family and community-level factors (e.g., social norms and social support). The SCHBM highlights the overarching significance of socio-cultural factors on health behaviors.

Sociocultural Health Behavior Model. Sociocultural Health Behavior Model, developed by the primary author was used in this study to explore factor impacting colorectal cancer screening among the target population. Note: Figure published in Ma GX, Wang MQ, Ma XS, Kim G, Toubbeh J, Shive S. The sociocultural health behavioral model and disparities in colorectal cancer screening among Chinese Americans. J Nurs Educ Pract. 2013;3(7):129-139. doi: 10.5430/jnep.v3n7p129. PMID: 25364475; PMCID: PMC4214268.
The purpose of this study was to examine the interplay of multilevel factors—individual, interpersonal, and community—on CRC screening behaviors. These multilevel factors form a complex mechanism affecting the behavior of individuals in seeking and receiving CRC screening. To the best of our knowledge, only a few studies have examined factors related to CRC screening among Vietnamese Americans; our understanding of the mechanisms through which multilevel factors interact to affect CRC screening remain limited. The goal of this community-based study was to apply the SCHBM to examine associations between individual-, cultural-, and community-level factors and lifetime CRC screening history specifically among medically underserved Vietnamese Americans in the greater Philadelphia area.
Materials and Methods
Study Design and Data Collection
From 2017 to 2019, we conducted a large-scale community-based randomized controlled trial of a culturally appropriate multilevel intervention to increase CRC screening among underserved Vietnamese Americans in the greater Philadelphia metropolitan area. The intervention components aimed to address individual-, interpersonal-, organizational-, and community-level barriers to CRC screening that Vietnamese Americans face. We used the community-based participatory research (CBPR) approach in the design and implementation of the study. Specifically, we worked closely with community-based organizations (CBOs) in the Vietnamese American community in the design of intervention components, the implementation of participant recruitment and intervention delivery strategies, and the design and collection of program evaluations. We actively engaged community leaders, stakeholders, and regular community members in the various stages of the project.
In collaboration with community leaders, the research team recruited 801 eligible participants from 20 CBOs in the Vietnamese American community in the greater Philadelphia metropolitan area. To be eligible, individuals needed to identify as being of Vietnamese descent and were required to be age 50 or above and accessible by cell phone. Eligible individuals were not enrolled in any CRC screening interventions, had no history of colorectal polyp or CRC, and had no family history of CRC. Enrolling only participants who had not enrolled in any CRC intervention was to prevent the contamination of other interventions on the outcome. Those with a history of colorectal polyp or CRC or had family history of CRC were considered at average risks, while those with such personal or family history were considered at higher risks. Including only the former group allowed us to test the efficacy of an intervention designed to promote CRC screening in the general community population. Participants had the option of answering the questions in either English or Vietnamese. Onsite language assistance from a trained bilingual community health educator was available for participants. All participants read and signed the informed consent forms to participate in the study. This described study was approved by the Institutional Review Board (IRB) of Temple University (IRB protocol #23693). This article only focused on the analysis and results of baseline data.
Measurements
The research team, working with community leaders and members, developed the survey questionnaire in English. Bilingual community health educators who were trained and experienced in community-based health research in the Vietnamese American community translated the questionnaire into Vietnamese; furthermore, our bilingual co-investigator conducted proofreading and edits. We conducted face and content validity of the questionnaire through involvement of a review panel composed of ten members including collaborating community leaders and health professionals. The questionnaire was revised based on comments from the review panel to ensure that the phrasing and terminologies used in the questionnaire were culturally appropriate, the questions were clearly stated, and the information was concise and familiar to the participants by using short direct sentences and common words or lay language as appropriate.
Outcome Measures
The primary outcome for this study was lifetime CRC screening. Respondents were asked if they had ever had a colonoscopy, FIT, or FOBT. The responses were coded as 0 for “no” and 1 for “yes.”
Enabling Factor
The enabling factor, health insurance coverage, was measured with the question: Do you currently have health insurance? The responses were coded as 0 for “no insurance,” 1 for “Medicare/Medicaid,” and 2 for “Private Insurance.”
Predisposing Factors
The predisposing factor, educational attainment, was measured as the highest level of educational degree obtained. The responses were coded as 0 for “high school degree or lower” and 1 for “college or advanced degree.”
Health Belief
Health belief was assessed with 5 questions related to perceptions of fatalism, health, and healthcare providers that were adapted from previous research of cancer screening behaviors in Asian Americans. 22 For instance, “Getting or not getting cancer is determined by the fate of a person. There’s not much people can do to avoid getting cancer” and “Most diseases, excluding external wounds, are caused by the imbalance between hot and cold in a person’s body.” We computed a health belief score by summing up participants’ responses to the 5 questions (Cronbach’s alpha = .79). The score ranged from 0 to 5, with a higher numeric value indicating greater endorsement of positive health beliefs.
Social Norms
Social norms were assessed with 8 community-based questions related to CRC screening that were adapted from previous research of cancer screening behaviors in Asian Americans. 22 The goal was to obtain a sense of communal views of CRC screening, which may have influenced previous screening uptake. The 8 social norm questions were asked using a 5-point Likert scale ranging from “strongly disagree” to “strongly agree.” Examples of social norm questions include: “people in my community talk about colorectal cancer screening,” “people in my community believe colorectal cancer screening can help prevent colorectal cancer,” and “talking about colorectal cancer and colorectal cancer screening is a comfortable topic in my community.” The average score, ranging from 0 to 5, was calculated for these 8 questions (Cronbach’s alpha = .87) to determine the overall level of social norm, with a higher numeric value indicating a greater presence of positive social norm toward CRC and CRC screening.
Self-Efficacy
Individual self-efficacy was assessed with 4 questions focused on individuals’ confidence in undergoing CRC screening, preparing for CRC screening, discussing CRC with their doctors, and their ability to control emotions that may be caused by CRC screening. The questions were adapted from previous research of cancer screening behaviors in Asian Americans, 22 and they had high reliability (Cronbach’s alpha = .89). The responses were on a 10-point Likert scale from “not at all confident” to “totally confident.”
Knowledge
Individual knowledge about CRC and CRC screening was assessed with 9 questions that were adapted from previous research in CRC-related knowledge among Asian Americans. 25,32 These questions covered a variety of areas concerning CRC more broadly and how it relates to the Vietnamese population. Coverage areas included appropriate screening age, risk factors for CRC, and the severity of risk for Vietnamese populations in the United States. A composite score was generated from individual responses for the 9 questions (Cronbach’s alpha = .73). The composite score ranged from 0 to 9.
Statistical Analysis
To test differences in sociodemographic and health-related factors between individuals who had ever received CRC screening and those who had never received screening, we conducted chi-square tests for categorical variables and t-test for continuous variables. We used structural equation modeling (SEM) for latent model analyses to examine how multilevel factors interact to affect lifetime CRC screening among Vietnamese Americans. Factors assessed included enabling factors, predisposing factors, cultural factors, self-efficacy, and knowledge. Results were constructed into a path model using tetrachoric correlations that depict relationships between exogenous variables (variables with both emanating paths and receiving paths) and endogenous variables (variables with mostly receiving paths). We estimated the model fit by computing the comparative fit indices (CFI) and Tucker-Lewis Index (TLI), along with the root mean square error of approximation (RMSEA). A CFI value of .90 or higher was considered acceptable; a TLI value of .90 or higher was considered acceptable; and a RMSEA value below 0.08 indicated a good fit. The total model R-Square indicates the percentage of explained variance in the dependent variable. 33 We conducted all analyses for this study in Stata 16. 34
Results
Sample Characteristics
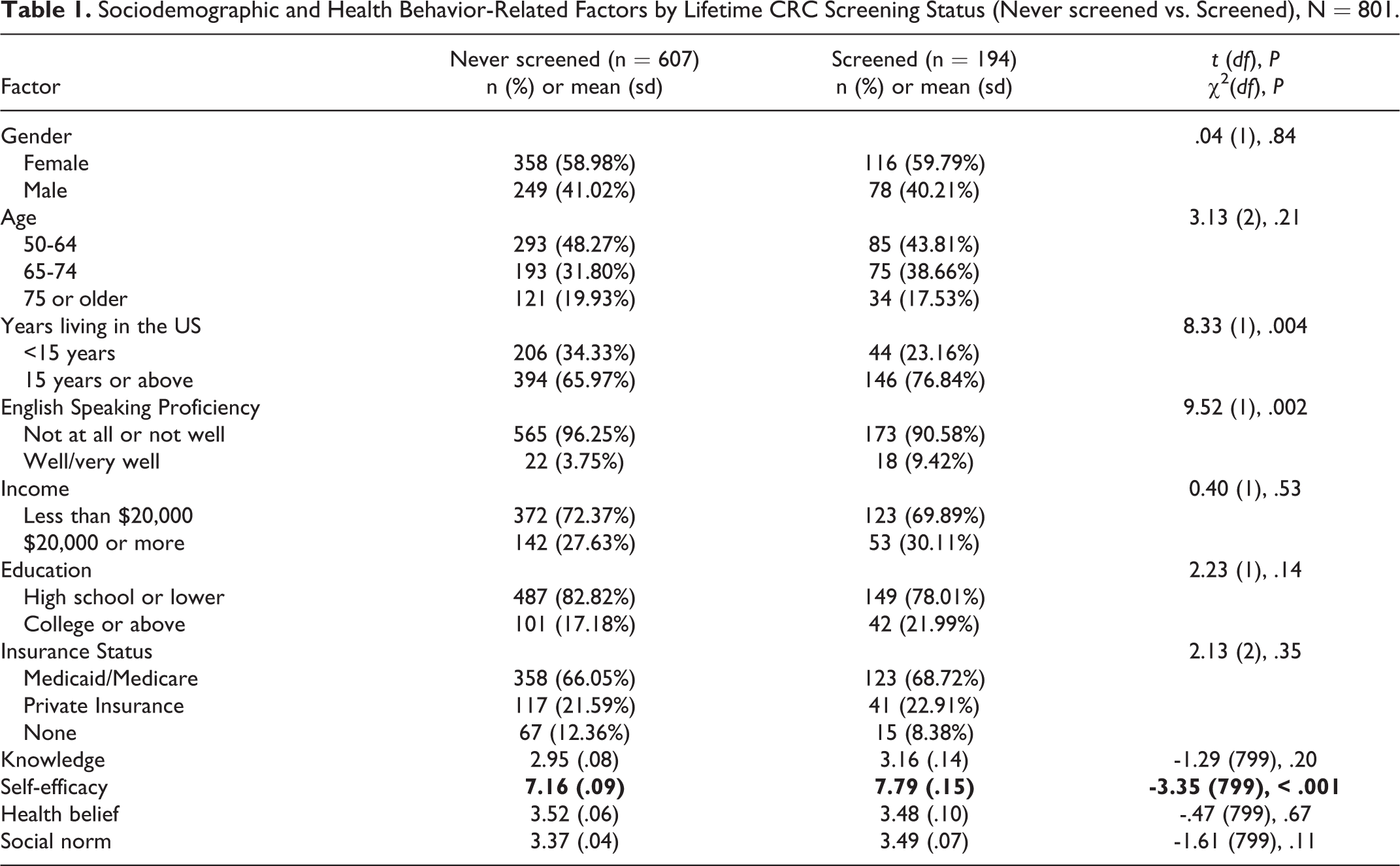
Table 1 shows the results for differences between participants who had previously received CRC screening (n = 194) and those who had never been screened for CRC (n = 607). Among those that previously received CRC screening when compared to participants who have never been screened, there were slightly more participants that reported living in the United States for 15 years or longer (76.84% vs. 65.97%) and slightly more participants reported well or very well English-speaking proficiency (9.42% vs. 3.75%). Average self-efficacy score was significantly higher among those who had received CRC screening (7.79) than among those who had not (7.16). Knowledge, health beliefs, and social norms did not differ significantly between the 2 groups. Knowledge was very low in both groups, with an average score of 2.95 among those who never been screened and 3.16 among those who had been screened for CRC, out of a total possible score of 9. The presence of positive perceptions of fatalism, health, and healthcare providers was modest for both groups, with an average score of 3.53 among those who had never been screened and 3.48 among those who had been screened for CRC, out of a total possible score of 5. Social norm was also at modest levels for both groups, with an average score of 3.37 among those have never been screened and 3.49 among those who had been screened for CRC, out of a total possible score of 5.
Sociodemographic and Health Behavior-Related Factors by Lifetime CRC Screening Status (Never screened vs. Screened), N = 801.
Structural Model
The hypothesized model and the standardized maximum likelihood estimates for parameters of the model are shown in Figure 2 . The path coefficients describe the direction and magnitude of associations between the parameters. Self-efficacy was the only factor that showed a positive and significant direct relationship with CRC screening (coefficient = .092, P < .01), which indicated that individuals with greater confidence in preparing for, receiving, and discussing CRC screening had a greater likelihood to have received CRC screening. In addition, predisposing factor, educational attainment (coefficient = .13, P < .01), and greater endorsement of positive health beliefs (perception toward fatalism, health, and healthcare providers) had a significant positive relationship (coefficient = .04, P < .001) with self-efficacy. Participants with higher levels of educational attainment and those with more positive health beliefs had a greater likelihood of demonstrating greater confidence in preparing for, receiving, and discussing CRC screening.

Path Coefficients and Their Significance From the Structural Equation Modeling Analysis (N = 801). *P <.**P < .01;***P < .001 RMSEA: 0.028; CFI: 0.969; TLI: 0.89.
In addition, we found that a higher educational attainment was significantly associated with higher levels of social norm scores at the community-level (coefficient = .03, P < .01), a higher likelihood of having health insurance coverage (coefficient = .13, P < .01), and a higher level of CRC-related knowledge (coefficient = .16, P < .001). Health belief was significantly associated with social norm scores at the community level (coefficient = .12, P < .001), with having health insurance coverage (coefficient = .032, P < .05), and with CRC-related knowledge (coefficient = .13, P < .001). This finding suggests that participants with more positive health beliefs had a greater likelihood of demonstrating positive social norms at the community-level and a greater likelihood of having greater levels of CRC-related knowledge, as well as a greater likelihood of reporting health insurance coverage. The R2 value explains the variance between the construct variables. Precisely 11.33% of CRC screening was explained by the constructs utilized in this structural model.
CFI for the structural equation model was 0.97, which meets the criteria for an acceptable model fit. TLI resulted in a value of 0.89. RMSEA compares the observed variances and covariances with those resulting from the model’s parameter estimates and is not sensitive to sample size. The model generated an RMSEA value of 0.028, which indicates a good fit of the measurement model.
Discussion
The purpose of this study was to apply the SCHBM to examine relationships between individual-, interpersonal-, and community-level factors and lifetime CRC screening history among limited English proficient, medically underserved Vietnamese Americans in the greater Philadelphia area. There were 4 main findings. First, we found that self-efficacy was the only factor with a significant direct association with lifetime CRC screening uptake. Participants who were more self-confident when preparing for and receiving CRC screening and discussing CRC screening test results had a greater likelihood of having received CRC screening, relative to less confident individuals. This finding adds to the growing body of literature that highlights the important role of self-efficacy in cancer prevention behaviors in Vietnamese Americans and other medically underserved Asian American populations. 22,35 -37
Second, we found that education was an indirect yet important factor in relation to CRC screening uptake. A higher level of educational attainment was significantly linked to individual CRC-related knowledge, health beliefs, and social norms and, via these associations, was linked to self-efficacy. These significant paths confirmed the critical role of upstream individual and social determinants of health. 38,39 Research has shown that the uneven distribution of educational resources and health disparities by socioeconomic status may be ameliorated through policy initiatives that give individuals of all ages improved access to health information and that inform individuals about how to use health information effectively. 40,41 Furthermore, this finding highlights the need for culturally competent, community-based educational outreach in underprivileged and underserved communities.
A third finding of this study is that health insurance coverage is a significant factor indirectly linked to lifetime CRC screening uptake. We observed direct paths to social norms and health beliefs in cancer prevention. The indirect paths to knowledge, self-efficacy and health insurance potentially afforded individuals’ access to health information and subscription to beliefs about cancer prevention. This in turn may have led to individuals feeling more comfortable and confident with CRC screening. This finding is consistent with observations from other studies in which health insurance coverage was identified as an important factor in promoting CRC screening behavior among Vietnamese Americans and other underserved Asian Americans. 23 -25,42 -45 Improving health insurance coverage, with linkage to culturally competent cancer prevention care for medically underserved populations, including those in which individuals have limited English proficiency and are affected by low socioeconomic standing, appears to be crucial for reducing cancer incidence and eliminating disparities in cancer mortality rates. 44,46 -48
The fourth major finding of this study centers on the identification of complex mechanisms through which individual-level factors, education, and health insurance coverage are related to psychosocial factors and knowledge. These factors, acting through self-efficacy, were linked to lifetime CRC screening uptake. This multilevel pathway indicates the need for efforts to reduce structural, cultural, community, and individual-level barriers. Individual-level education and empowerment should be accompanied by destigmatization of cancer and by a more open community cultural norm toward cancer prevention. A more positive cultural norm could be achieved by the engagement of community leaders, lay community health educators, and patient representatives, and the adoption of ethnic-specific traditional and social media platforms to raise awareness and combat misinformation. In underprivileged and underserved communities, these measures have the potential to significantly increase awareness of CRC prevention and early CRC detection.
Collectively, the findings of this community-based study shed light on the interplay of multilevel factors—encompassing individuals, culture, and community—that ultimately affect CRC screening participation. This study is not without limitations. We excluding individuals with any personal or family history of colorectal polyps or CRC, we were focussing on population that might be slightly healthier than the general population. Future research should examine the awareness of and screening behaviors among individuals with personal or family history of colon polyps or CRC, a group at a higher risk for CRC. Being cross-sectional in nature, our study design did not permit us to ascertain whether the various multilevel factors would predict the eventual uptake of CRC screening. We also examined lifetime history of CRC screening, which did not necessarily imply that participants were up to date with respective CRC screening modalities. Furthermore, we did not assess the role of healthcare providers in CRC screening discussions with patients and the potential impact of these discussions on participant self-efficacy. Nonetheless, this study lends support to the need for social policies and public health interventions that effectively address structural, cultural, community, and individual-level barriers to quality and timely healthcare services for cancer prevention in Vietnamese American communities. 47 -50 Future studies should focus on empowering and educating study participants in effort to raise awareness of and increase self-efficacy in CRC screening. Future public health campaigns would benefit from providing access to screening resources in a community-setting in effort to mitigate the inherent barrier of health insurance coverage with hopes of reaching the harder to reach populations.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This described study was approved by the Institutional Review Board (IRB) of Temple University (IRB protocol #23693).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was supported by grant R01MD010627 (PI: Grace X. Ma, PhD) from the National Institute on Minority Health and Health Disparities (NIMHD) of National Institute of Health (NIH) and in part by TUFCCC/HC Regional Comprehensive Cancer Health Disparity Partnership, Award Number U54 CA221704(5) from the National Cancer Institute of National Institutes of Health (NCI/NIH). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIMHD or NCI/NIH.
Statement of Human and Animal Rights
All study procedures involving participants were consistent with the requirements of the Institutional Review Board (IRB) of Temple University and approved by the Institutional Review Board (IRB) of Temple University (IRB protocol # 23693).
Statement of Informed Consent
All participants read and signed the informed consent forms to participate in the study.