
Abstract
Objective:
Patients with lung cancer are at risk of radiation pneumonia (RP) after receiving radiotherapy. We established a prediction model according to the critical indicators extracted from radiation pneumonia patients.
Materials and Methods:
74 radiation pneumonia patients were involved in the training set. Firstly, the clinical data, hematological and radiation dose parameters of the 74 patients were screened by Logistics regression univariate analysis according to the level of radiation pneumonia. Next, Stepwise regression analysis was utilized to construct the regression model. Then, the influence of continuous variables on RP was tested by smoothing function. Finally, the model was externally verified by 30 patients in validation set and visualized by R code.
Results:
In the training set, there was 40 patients suffered≥ level 2 acute radiation pneumonia. Clinical data (diabetes), blood indexes (lymphocyte percentage, basophil percentage, platelet count) and radiation dose (V15 > 40%, V20 > 30%, V35 >18%, V40 > 15%) were related to radiation pneumonia (P < 0.05). Particularly, stepwise regression analysis indicated that the history of diabetes, the basophils percentage, platelet count and V20 could be the best combination used for predicting radiation pneumonia. The column chart was obtained by fitting the regression model with the combined indicator. The receiver operating characteristic (ROC) curve showed that the AUC in the development term was 0.853, the AUC was 0.656 in the validation term. And calibration curves of both groups showed the high stability in efficiently diagnostic. Furthermore, the DCA curve showed that the model had a satisfactory positive net benefit.
Conclusion:
The combination of the basophils percentage, platelet count and V20 is available to build a predictive model of radiation pneumonia for patients with advanced lung cancer.
Introduction
According to the latest statistics, the morbidity and mortality of lung cancer rank first among malignant tumors, 1 which seriously affects the living standards of residents. With the wide application of radiotherapy, radiotherapy technology has become 1 of the main treatments for patients with stage Ⅲ and Ⅳ lung cancer who are unable to undergo surgery or unwilling to undergo surgery. It is reported that after receiving chest radiotherapy, patients have a probability of radiation pneumonia of 15% ∼ 40%, 2 among which the incidence of severe pneumonia is 10%∼20%, and the mortality rate is high to 50%. Even asymptomatic pneumonia will cause the decline of lung reserve function. 3 Early studies suggested that MLD, lung V20 and lung V30 were the related factors of radiation-induced lung injury. 4,5
3D-CRT or IMRT has successfully reduced the radiation dose to normal lung tissue, but it still cannot completely avoid radiation pneumonia. 6 Therefore, besides dosimetry, there are other factors that affect the occurrence of radiation pneumonia. How to find effective measures to prevent and treat radiation pneumonia on the basis of 3D-CRT or IMRT is 1 of the important parts that must be considered in radiotherapy of lung cancer. Many studies have focused on the correlation between radiation pneumonitis and voxel level, basic diseases, cytokines, tumor factors, lung function and treatment, 7 -13 which provides many valuable indicators for the occurrence of radiation pneumonia.
At present, it is considered that the occurrence of radiation pneumonitis is a complex process of interaction, mutual influence and joint regulation by many factors, such as clinical factors and dosimetry factors, 14 so it is particularly important to find sensitive indicators or models that can predict the occurrence of radiation pneumonia. However, there are few reports about using some simple and easy-to-get information to predict radiation pneumonia. Therefore, by collecting clinical information, hematological indexes and radiation dose parameters that may be related to radiation pneumonia, this study retrospectively analyzed multiple groups of data of 104 patients with stage III and IV radiation pneumonia, trying to find out the factors that affect the occurrence of radiation pneumonia, establish a mathematical prediction model, provide reference indexes for clinic, optimize radiotherapy plan and help prevent radiation pneumonia in clinical radiotherapy.
Materials and Methods
Data Collection
Lung cancer patients who received radiation therapy from January 2016 to June 2020 in the radiotherapy department of Oriental Cancer Hospital affiliated to Anhui University of Science and Technology were retrospective studied as a development term, and lung cancer patients who received radiation therapy from January 2019 to June 2020 in the radiotherapy department of the First People’s Hospital affiliated to Anhui University of Science and Technology were retrospective studied as a validation term. Enrollment criteria: (1) patients was confirmed by pathology as lung cancer in stage III or IV; (2) and received a chest radiation therapy; (3) and diagnosed as ≥ 2 radiation pneumonia in regular or follow-up. Exclusion criteria: (1) patient had lung cancer surgery history; (2) or was non-first-time diagnosis of lung cancer for radiation therapy; (3) or has incomplete parameters of the 3D-CRT or IMRT; (4) or the interval between chemotherapy and radiotherapy is less than 14 days. According to the inclusion and exclusion criteria, a total of 74 patients, 51 male and 23 female with the average age of 68 years old (39-88y), was selected in the development term, including, of which 35 cases of lung adenocarcinoma, 23 cases of lung squamous cell carcinoma, 14 cases of small cell lung cancer and 2 cases of sarcoma-like cancer. A total of 30 patients (20 male and 10 female) with the average age of 64 years old (34-83 y), was selected in the verification term, including 11 cases of lung adenocarcinoma, 7 cases of lung squamous cell carcinoma and 12 cases of small cell lung cancer. Detail information can be seen in Table 1.
Description of the Crowd.

Abbreviation: RP, Radiation pneumonia.
aOther: large cell lung cancer.
Diagnostic Criteria
All patients were followed up for 6 months, CT scan was reexamined 1, 3, and 6 months after radiotherapy to evaluate the effect of tumor control and pulmonary changes. Based on the clinical symptoms and imaging data, radiation pneumonia was diagnosed and graded according to the common adverse reaction event evaluation criteria (CTCAE,5.0). Level 1: Asymptomatic, only clinical or imaging changes, no need for treatment; Level 2: mild symptoms, limited instrumental daily activities, need medication; Level 3: Severe symptoms, limited individual daily activities, need oxygen; Level 4: Life-threatening respiratory symptoms, requiring urgent treatment; Level 5: Causing the death of the patient.
Collection of Relevant Indicators
Clinical general characteristics: age, sex, smoking history, physical status score (PS), chronic obstructive pulmonary disease (COPD), tumor location, tumor pathology type, tumor stage, tumor type, and diabetes history.
Hematological indexes: white blood cell count and its classification count (number and percentage of Neutrophils, lymphocytes, monocytes, eosinophils, and basophilic granulocytes), red blood cell count (red blood cell volume, average red blood cell volume, standard deviation of red blood cell distribution width, variation of red blood cell distribution width), hemoglobin count determination (average hemoglobin content, average hemoglobin concentration), and platelet count (average platelet volume, platelet volume distribution width).
Radiation dosimetry parameters: Observation parameters include percentage of lung volume irradiated by bilateral lung reception greater than 5, 10, 15, 20, 25, 30, 35, 40 Gy doses (V5, V10, V15, V20, V25, V30, V35, and V40), mean lung dose (MLD), Gross Tumor Volume (GTV).
Treatment Regimen
The energy selected was 6MV-X Varian L-2100C linear accelerator. The 3D-CRT or IMRT radiotherapy was adopted, and the isocenter multi-field coplanar irradiation technology was adopted. SAD = 100 cm, the prescription dose was 40-70 Gy, and the single radiotherapy dose was 1.8Gy-2.0 Gy, 1F/D, and 5 f/w. The radiotherapy plan was evaluated and reviewed by 2 tumor radiotherapy physicians with rich clinical experience. The final radiotherapy plan ensured that ≥ 95% of the corresponding target prescription dose covered more than 95% of the target volume. Normal tissue dose limits: normal bilateral lung tissue dose limits V5 ≤ 60%, V20 ≤ 30%, V30 ≤ 20%, cardiac dose limits V30 ≤ 40%, V40 ≤ 30%; Spinal cord dose limit Vmax ≤ 45 Gy.
Statistical Methods
Logistics regression was applied for single factor analysis, wherein the dependent variable (with or without radiation pneumonia) was dichotomous variables: without radiation pneumonia was assigned 0, and with radiation pneumonia was assigned 1; the dichotomous variable in independent variable was assigned 0 and 1, and the continuous variables use their clinical standard units, such as: 109/L (WBC, NEU, LYM, MON, PLT), g/L (HGB, MCHC) or percentage (basophils percentage, eosinophil percentage, lymphocyte percentage). The results of single factor analysis were used in stepwise regression analysis and fitted to calculate variance expansion factor for preventing of collinearity. R language was utilized for visualization of the chart, ROC curve, and calibration curve. Decision curve analysis was employed to evaluate the differentiation, accuracy and practicality of the mode. The ethical statement: Our study was approved by The Biomedical Research Ethics Committee of AUST (Xiaolunzike 20190116).
Results
A total of 104 patients with lung cancer were divided into development term (n = 74) and verification term (n = 30). In the development term, there were 51 male patients and 23 female patients, of which 52 received radiotherapy and 22 received radiotherapy alone. In the verification term, there were 20 male patients and 10 female patients, of which 21 received radiotherapy and 9 received radiotherapy alone. In the development term, 40 patients (54%) developed grade 2 or above radiation pneumonia, including 23 cases of grade 2, 12 cases of grade 3, and 5 cases of grade 4. In the verification term, 11 patients (36.7%) developed grade 2 or above radiation pneumonia in 6 cases of grade 2, 4 cases of grade 3, and 1 case of grade 4. There were 3 cases of grade 4, 3 cases of grade 4 and 2 cases of grade 5. These events are often observed within 1 to 3 months after radiation.
Univariate Analysis of Related Factors in Diagnosis of Radiation Pneumonia
Table 2 showed that univariate analysis results of clinical factors suggest a correlation between the history of diabetes (P = 0.042) and the radiation pneumonia. Table 3 showed that univariate analysis results of hematological indexes suggest that lymphocyte count (LYM: P = 0.044), basophilic percentage (BAS%: P = 0.006) and platelet count (PLT: P = 0.016) are related to radiation pneumonia. Table 4 showed that univariate analysis results of radiation dosimetry indexes suggest that V15 (P = 0.001), V20 (P = 0.004), V35 (P = 0.019) and V40 (P = 0.002) are associated with radiation pneumonia.
Single-Factor Analysis of the Effects of Clinical Factors on Radioactive Pneumonia in the Training Set.

*P-value <0.05.
Single-Factor Analysis of the Effects of Hematological Indicators on Radioactive Pneumonia in the Training Set.

*P < 0.05.
**P < 0.01.
***P < 0.001.
Single-Factor Analysis of the Effects of Radiation Dosing Indicators on Radioactive Pneumonia in the Training Set.a

a The volume of V5-V40 refers to the bilateral lung volume.
*P-value <0.005.
**P-value <0.01.
***P-value <0.001.
Stepwise Regression Analysis of Related Factors in Diagnosis of Radiation Pneumonia
The variables of p < 0.05), and negative relation between radiation pneumonia with the BAS%, PLT and V20 was confirmed by smoothing function test (Figure 1). At the same time, the collinear test showed that the variance expansion factors of BAS%, PLT, diabetes and V20 were 1.1, 1.1, 1.1 and 1.7 (Table S1), all below the standard value of 10, suggesting that there was no colinear relationship among the factors.
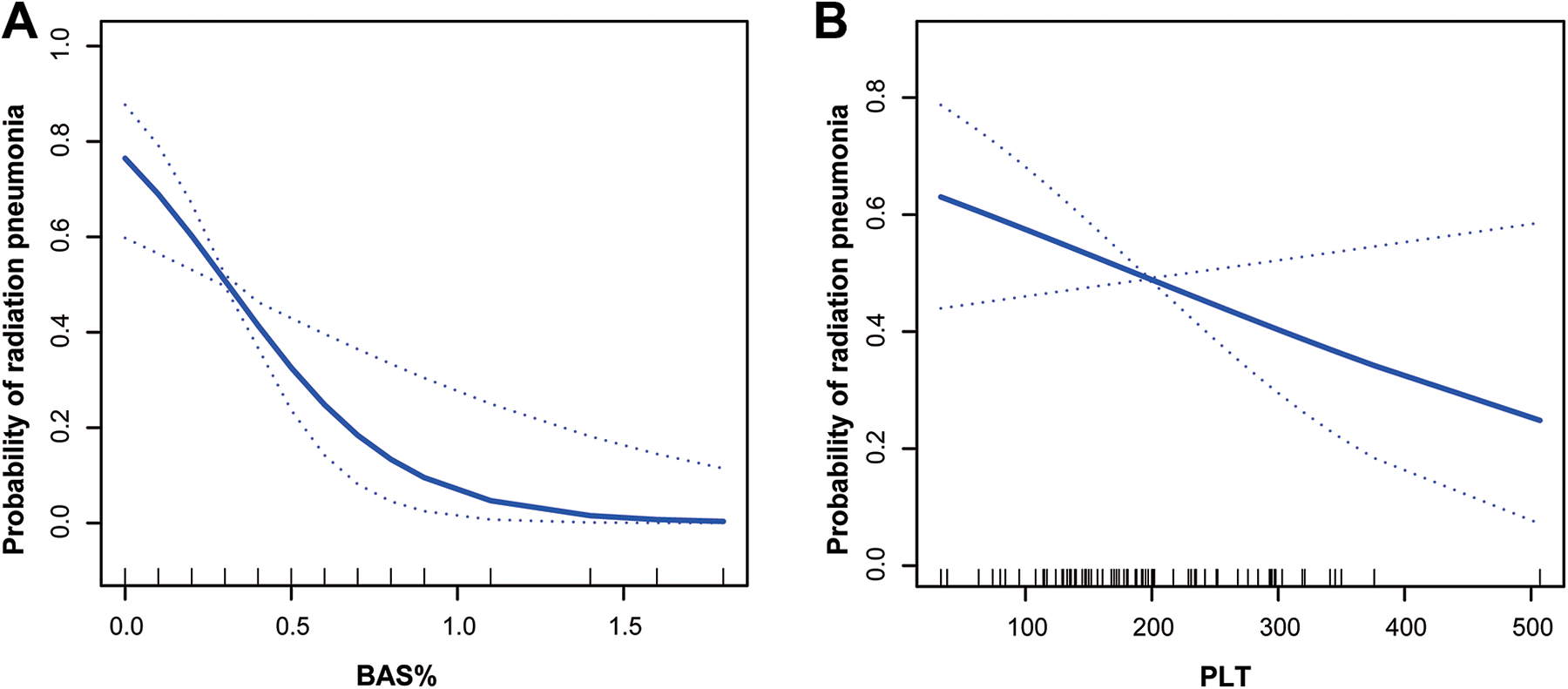
The correlation between continuous variables and radiation pneumonia. A, The relationship between BAS% and radiation pneumonia. B, The relationship between platelet count and radiation pneumonia.
Construction and Validation of Predictive Model
According to the method of stepwise regression analysis, We screened out the prediction model of 4 variable combinations (Table 5), and Table 6 shows that the ROC of prediction model is better than any single variable. Although, the diabetes p > 0.05 in stepwise regression, it was still included in the model because of its great clinical significance, and the ROC value of the four-factor model was higher than that of the three-factor model (Figure S1). The corresponding regression coefficient was calculated and the predictive mathematical model was established. As shown in the Figure 2, the probability of radiation pneumonia was P = 1.87476 − 3.92066*BAS% − 0.00912*PLT + 1.11323*Diabetes + 1.62853*V20, and the predictive mathematical model was visualized in nomogram.
Stepwise Regression Analysis in the Training Set.

AUC of BAS, PLT, Diabetes, V20, and Model.


Prediction nomogram of radiation pneumonia.
In order to evaluate the performance of the model, we carried out a series of analysis and verification. Firstly, the ROC curve (Figure 3A) in the training set showed that the AUC value of the predictive model is 0.853, the sensitivity of the model is 70%, and specificity of the model is 94%. Secondly, the calibration curve (Figure 3B) showed that the diagnostic efficiency of the model is in good agreement with the actual diagnosis. Finally, the decision curve analysis result (Figure 3C) showed that the model has a satisfactory positive net benefit, suggesting that the model has a good reference significance for predicting radiation pneumonia in clinical. In the validation set, the model ROC curve (Figure 3D) showed an AUC value is 0.656, sensitivity is 63% and specificity is 73%, and the calibration curve (Figure 3E) and the decision curve analysis result (Figure 3F) also indicate that the model has certain auxiliary significance.

Verification of prediction model. Training set: (A) Receiver operating characteristic curves; (B) Calibration curve; (C) Decision curve. Validation set: (D) Receiver operating characteristic curves; (E) Calibration curve; (F) Decision curve.
Discussion
Radiation pneumonia, one of the most common dose-limiting toxic reactions of lung cancer after radiotherapy, has no obvious effective treatment, and affects the treatment process and survival time of cancer patients. At present, it is recognized that the most important influencing factor of radiation pneumonia is the radiation dose parameters. 15 However, in the practice of radiotherapy, the occurrence of radiation pneumonia still confuses clinicians even though the dose parameters are strictly limited before radiotherapy. This shows that in addition to dose parameter factors, other multi-factors are involved in radiation pneumonia.
In this study, the diagnostic prediction model of RP was constructed comprehensively using 3 easily obtained parameters. The univariate analysis results showed that the history of diabetes in clinical factors, the LYM, the BAS%, and the PLT in hematological indexes, and the radiation dosage indicators V15, V20, V35 and V40 were all associated with radiation pneumonia. The indicators of practice.
Among the clinical factors, some studies concluded that the patient’s age, 16 sex, 17 physical status, 18 chronic lung disease, 19 tumor location, 16 smoking status 20 and pathological type may be the clinical individual factors affecting radiation pneumonia. However, some studies found that age and sex were not the influencing factors of radiation pneumonia. 21 This study found that there was no significant difference in clinical factors such as age, sex, smoking, pathological types and tumor location. It is generally believed that female patients may be more prone to radiation pneumonia due to small lung volume and high dose per unit lung tissue, 22 but the same conclusion was not got by this study, may due to the insufficient sample size of patients. The elderly may have poor tolerance to radiation due to lung function and other factors, and the incidence of radiation pneumonia is high. 23 Therefore, the data of this group did not show the influence of age on radiation pneumonia. In addition, the tumor stages of patients in this group were mainly stage III and IV, and the patients in stage I and II were not included, so there the correlation between tumor stages and radiation pneumonia were not considered. Some studies suggest that in the case of poor blood glucose control, the probability of radiation pneumonia is high. 24 Glycosylated hemoglobin (GHb) can reflect the blood glucose control of patients for about 2 months, which is more reliable than a single fasting blood glucose, postprandial blood glucose and other blood glucose indicators, so GHb can also be used as an independent factor in the diagnosis of radiation pneumonia in other study. 25 Although this study did not include the blood glucose indicators, the history of diabetes of patients was considered and a high risk of radiation pneumonia was confirmed because of their poor blood glucose control. Similarly, a new study 14 further explored the relationship between monocytes and neutrophils, which suggested that monocyte to lymphocyte ratio (MLR) could predict the occurrence of radiation pneumonitis in patients with thoracic tumor radiation.
In terms of hematological indicators, based on convenient and fast considerations, only 22 routine blood test parameters were considered. Among them, basophilic granulocytes count (BAS) fluctuates greatly in the 95% confidence interval due to its small fluctuations range and the small sample size. Univariate analysis results showed that LYM, BAS% and PLT were negatively correlated with the occurrence of radiation pneumonia. In stepwise regression analysis, the BAS% and PLT were also independent diagnostic factors for radiation pneumonia. Normally, the number of basophilic granulocytes circulating in the outer circulation of blood is small, but they can secrete a variety of B cell regulation molecules, and then express CD40 L, IL-4 and IL-6, to support the proliferation of B cells and the production of IgM and IgG1, 26 which suggests that the basophils play an important role in humoral immunity regulation. In the case of pathogen invasion, platelets can make a rapid immune response to resist the invasion of pathogenic microorganisms. In addition, platelets can also play a role in adaptive immune regulation through T cells, antigen presenting cell, and B cells. Therefore, when the BAS% and PLT are lower than the normal standard, the patient’s immune function is poor, and prone to radiation pneumonia.
Radiation dose parameters always account for a large proportion in the occurrence development of radiation pneumonia. More and more studies have found that the radioactive lung injury is closely related to the low dose volume of the lungs. Meanwhile, some studies have found that radioactive lung damage is related to lung V5-V65. 27 The correlation between MLD, lung V5-V20 and radioactive lung injury has also been confirmed by many researchers. 28,29 The results of this study showed that lung V15, V20, V35 and V40 were associated with RP. This is consistent with previous research. The stepwise regression analysis showed that lung V20 was a valuable index to predict RP. Lung V20 means the percentage of lung volume that received radiation dose over 20 Gy, and was the most common-used radiation dose volume factor, 30,31 which is not only related to the incidence of radiation pneumonia, but also closely related to the severity of radiation pneumonia. 30
In summary, after comprehensive analysis of clinical factors, hematological indicators and radiation dosing indicators, BAS%, PLT and V20 were determined as independent diagnostic factors, and a more visualized and reliable predictive model was obtained by combining multiple indicators, which was simple and easy to obtain and could be used as a reference for clinicians in clinical practice.
Conclusion
In this study, the prediction model is constructed by integrating clinical factors, hematological indicators and radiation dosimetry indicators. The prediction performance is reliable and the detection indicators are simple and easy to obtain, which can reduce the economic burden of patients and is worth popularizing after further verification. However, the correlation of radiation pneumonia is not limited to the above 3 types of parameters. It is expected that in the subsequent study can be added to the radiomics and other indicators, to establish a better and more comprehensive prediction model, which can provide help in clinical practice.
Supplemental Material
Supplemental Material, sj-tif-1-ccx-10.1177_10732748211026671 - Construction and Verification of a Radiation Pneumonia Prediction Model Based on Multiple Parameters
Supplemental Material, sj-tif-1-ccx-10.1177_10732748211026671 for Construction and Verification of a Radiation Pneumonia Prediction Model Based on Multiple Parameters by Liu Yafeng, Wu Jing, Zhou Jiawei, Xing Yingru, Zhang Xin, Li Danting, Xie Jun, Tian Chang, Mu Min, Ding Xuansheng and Hu Dong in Cancer Control
Supplemental Material
Supplemental Material, sj-xlsx-1-ccx-10.1177_10732748211026671 - Construction and Verification of a Radiation Pneumonia Prediction Model Based on Multiple Parameters
Supplemental Material, sj-xlsx-1-ccx-10.1177_10732748211026671 for Construction and Verification of a Radiation Pneumonia Prediction Model Based on Multiple Parameters by Liu Yafeng, Wu Jing, Zhou Jiawei, Xing Yingru, Zhang Xin, Li Danting, Xie Jun, Tian Chang, Mu Min, Ding Xuansheng and Hu Dong in Cancer Control
Footnotes
Authors’ Note
HD, WJ, and DX: conception and design, and study supervision. LY, ZJ, MM, ZX, LD, and TC: development of methodology, analysis and interpretation of data, and writing of the manuscript. HD, XY, and XJ: review of the manuscript. I would like to declare on behalf of my co-authors that the work described was original research that has not been published previously, and not under consideration for publication elsewhere, in whole or in part. All the authors listed have approved the manuscript that is enclosed. All datasets presented in this study are included in the article/supplementary material. Our study was approved by The Biomedical Research Ethics Committee of AUST (Xiaolunzike 20190116). This study was conducted in accordance with the ethical standards of the World Medical Association Declaration of Helsinki. All patients are required to provide written informed consent prior to enrollment in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (No. 81971483), the Top Talents Program of Disciplines (Majors) in Colleges and Universities of Anhui Province (gxbjZD12), the Anhui University collaborative innovation project (gxxt-2020-058) and the Natural Science Foundation of Educational Commission of Anhui Province of China (KJ2018A0097). The funders had no role in the study design, data collection, analysis, and decision to publish or preparation of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.