
Abstract
The overall survival of patients with Chronic Myeloid Leukemia (CML) treated by using tyrosine kinase inhibitors (TKIs) is very close to that of the healthy population. However, little is known about the effect of specific measures such as intermittent fasting, especially during Ramadan period. A 3-year retrospective study was conducted to evaluate the effect of fasting on patients with CML receiving TKIs by evaluating certain clinical, hematological, and molecular parameters. A total of 49 patients were eligible, with a median age of 46 years (range: 22-86), of these 36 (73.5%) were males and 13 (26.5%) were females. Twenty-seven (55%) patients are Middle Eastern, while 16 (32.7%) from the Indian subcontinent, and 6 (12.3%) Africans. Imatinib was the most common TKI; used in 25 patients (51%). The mean White blood cells (WBCs), neutrophils, and BCR-ABL were found to be reduced after fasting compared to before and during with statistical difference. The use of TKIs while fasting did not result in significant changes in hematological nor BCR-ABL levels in our study. Patients who wish to practice intermittent fasting may be reassured in this regard, yet physicians can adopt the safe trial approach, where they allow the patients to fast, but with instructions such as when to break fasting.
Introduction
Chronic Myeloid Leukemia (CML) is a clonal bone marrow myeloid disorder that represents a prototype model for targeted therapy and cancer. Identification of a BCR-ABL1 gene fusion is diagnostic of CML and levels of BCR-ABL1 transcripts detectable following treatment with tyrosine kinase inhibitors (TKIs) can be measured using standardized protocols that allow patients to be managed consistent with expert guidelines. 1 Best practice recommendations from the National Comprehensive Cancer Network (NCCN) and the European LeukemiaNet (ELN) networks define optimal responses at key milestones in treatment allowing for early signs of poor adherence or resistance to treatment to be detected early and allow for effective clinical intervention. 2
Dynamic changes in cellular metabolism are known to accompany oncogene activation to support the growth of a rapidly proliferating clone. Cancer cells are believed to be vulnerable to nutrient deprivation and clinical trials investigating the effects of intermittent fasting are ongoing. 3
Restricting calorie intake could offer potential benefits for clinical use of TKIs, however, compliance remains a significant challenge. In Islam, Ramadan fasting represents one of the 5 pillars of creed and is considered as a mandatory religious duty so a robust social structure exists to support adherence to an intermittent fasting regimen. 4 However, Different types of intermittent fasting are recognized, including 5:2 diet; fasting for 2 days per week, Eat-Stop-Eat diet; a 24-hour fast, once or twice a week, Alternate-Day Fasting; fast every other day, The Warrior Diet; Fast during the day, eat a huge meal at night, Spontaneous Meal Skipping; Skip meals when convenient, and the 16/8 Method; fast for 16 hours per day. 5 And fasting during Ramadan displays some overlap with 16/8 method (fasting for 16 hours each day) as in both instances there are recurring periods of fasting and feeding. Intermittent fasting regimens offer the potential to influence metabolic regulation via effects on (a) circadian biology, (b) the gut microbiome, and (c) modifiable lifestyle behaviors. This type of nonpharmacological intervention is cost-effective and associated with a low risk of adverse events and multiple public health benefits. 5,6
No guidelines or standardized protocols exist that can help physicians advise CML patients who wish to practice intermittant fasting. Furthermore, researchers in Malaysia found that Muslim patients with CML disclosed that they had frequently skipped or changed doses of nilotinib to fulfill their religious obligations during Ramadan. 7
The main purpose of this study was to evaluate the effect of fasting on CML patients receiving TKIs by evaluating their clinical course, hematological parameters, and BCR-ABL1 levels.
Materials and Methods
A retrospective study was conducted by reviewing medical records for adult Muslim patients with CML in a tertiary cancer center in Qatar.
Inclusion criteria include: Confirmed diagnoses of CML in chronic phase. Patients with confirmed fasting of Ramadan month, during all or part of the years 2016, 2017, and 2018. Patients were asked to confirm their fasting practice by a telephone call made by the study team. Patients should have regular follow up, at least for one year, with all hematological and molecular data available. Hematologic, cytogenetic, and molecular responses were monitored according to European LeukemiaNet recommendations of 2013 for the management of CML.
Exclusion criteria include patients who did not fulfill the above criteria.
49 patients fulfilled the above-mentioned criteria, and therefore we evaluated: Complete Blood Count before, during, and after fasting.
BCR-ABL1 transcript levels before, during, and after fasting using real-time quantitative Polymerase chain reaction (RT-qPCR) analysis. The reported results were based on triplicate measurements calculated as the ratio of total BCR-ABL1 transcripts to total ABL1 transcripts, reported as a percentage ratio on the International Scale (IS).
8
Any loss of hematological response or clinical evidence of disease progression (e.g., increase in spleen size during fasting).
Statistical Analysis
Anonymous data were collected and entered into a standard electronic database excel sheet designed in view of study design and objectives. Descriptive statistics were used to summarize demographic, clinical, hematological parameters, and other characteristics of the participants. The normally distributed data and results were reported with mean and standard deviation (SD); the remaining results were reported with median and interquartile range (IQR). Categorical data were summarized using frequencies and percentages. Preliminary analyses were conducted to examine the distribution of the data variables using the Kolmogorov–Smirnov test.
We used the repeated-measures analysis of variance (ANOVA) to compare various hematological parameters measured before, during, and after intermittent fasting periods. And when the repeated-measures ANOVA was significant (P < 0.05), we performed post hoc tests with the Wilcoxon matched-pairs signed-rank test. One-way ANOVA/Kruskal Wallis test was applied to compare various hematological parameters measured among different TKIs, ethnicity and age groups. Associations between 2 or more qualitative variables were assessed using the Chi-square (χ2) test, Fisher Exact or Yates corrected Chi-square tests as appropriate. Quantitative data and outcome measures between the 2 and more than 2 independent groups were analyzed using unpaired ‘t’ test (Mann Whitney U test for non-normal data). Pictorial presentations of the key results were made using appropriate statistical graphs. All P values presented were 2-tailed, and P values <0.05 was considered as statistically significant. All Statistical analyses were done using statistical packages SPSS 22.0 (SPSS Inc. Chicago, IL) and Epi-info (Centers for Disease Control and Prevention, Atlanta, GA) software.
Results
Patients’ Characteristics
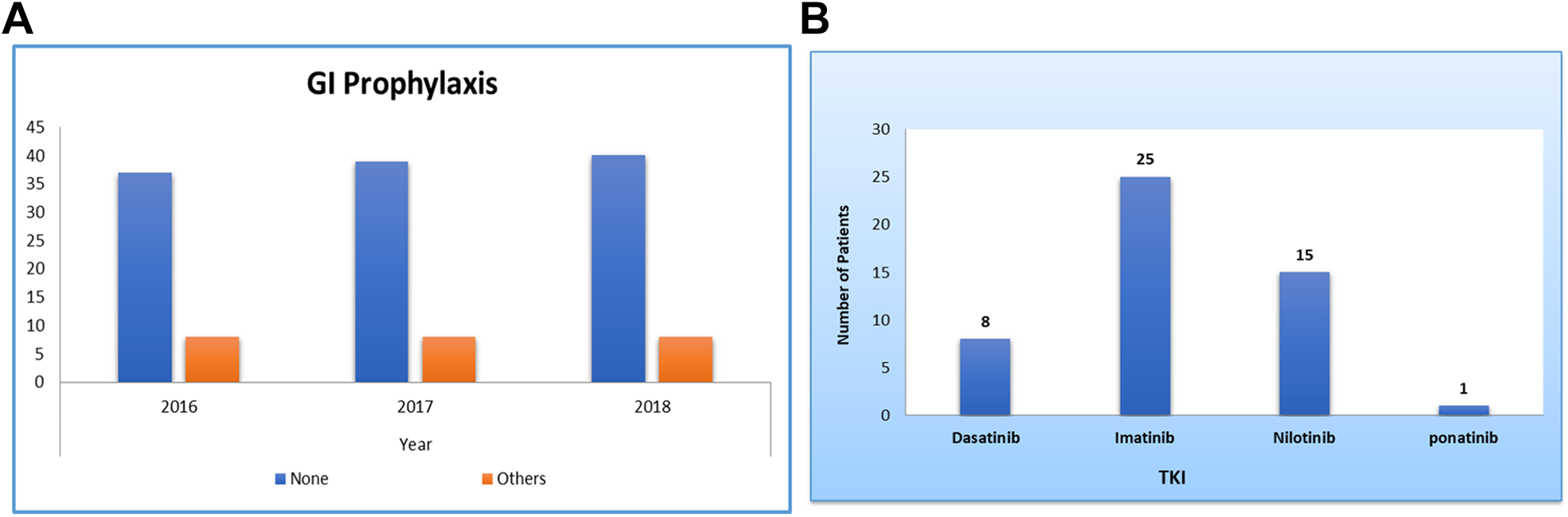
During the study period of 2016, 2017 and 2018, a total of 49 patients fulfilled the criteria of the study, with mean age 46.8 ± 14.51 years (median 46 years; IQR 36 to 58 years), of these 36 (73.5%) were males and 13 (26.5%) were females, with a ratio of 2.8:1. In this cohort of patients studied, 27 (55.1%) patients are Middle Eastern, while 16 (32.7%) patients came from the Indian subcontinent and 6 (12.2%) patients were black Arab ethnicity. The main demographic, clinical and other characteristics of the study population are summarized in (Table 1). Multiple TKIs were used, imatinib was the most common TKI; used in 25 patients (51%), nilotinib in 15 patients (30.6%), dasatinib in 8 patients (16.3%) and ponatinib used only in 1 patient (Figure 1A). GI prophylaxis was reported in <16% of the cases (Figure 1B).
Demographics.

Patients’ characteristics.
Comparison of Various Hematological Parameters Across 3 Periods
Repeated measure analysis of variance (ANOVA) statistical analysis showed that the parameters WBC (median 7, IQR 5.6, 8.7), neutrophils (median 3.8, IQR 2.8, 4.8), Basophils (median 0, IQR 0, 0.05) and BCR-ABL (median 0.03, IQR 0.006, 0.30) were found to be reduced after fasting compared to before WBC (median 7.8, IQR 5.9, 9.3), neutrophils (median 4.1, IQR 3.1, 5.8), Basophils (median 0.02, IQR 0, 0.1) and BCR-ABL (median 0.05, IQR 0.003, 2.9) and during fasting WBC (median 7.1, IQR 5.6, 8.3), neutrophils (median 3.8, IQR 2.5, 4.7), Basophils (median 0.03, IQR 0, 0.1) and BCR-ABL (median 0.04, IQR 0.004, 0.63), however their differences were statistically insignificant (P > 0.05). Moreover, mean platelet and hemoglobin levels and median basophils and eosinophils values did not differ significantly and appeared to have a similar trend in their values measured before, during and after intermittent fasting periods respectively. As illustrated; patients had MMR Before Ramadan, and maintained MMR During and after Ramadan based on the median BCR/ABL1 values; (median 0.05, IQR 0.003, 2.9), (median 0.04, IQR 0.004, 0.63), (median 0.03, IQR 0.006, 0.30), before, during, and after Ramadan, respectively (Tables 2 and 3).
Gender and Hematologic Parameters.

Abbreviations: SD, Standard deviation; IQR, Inter-quartile range.
*P-value computed using non-parametric Mann Whitney U test.
Multivariate Analysis for Hematologic Parameters.
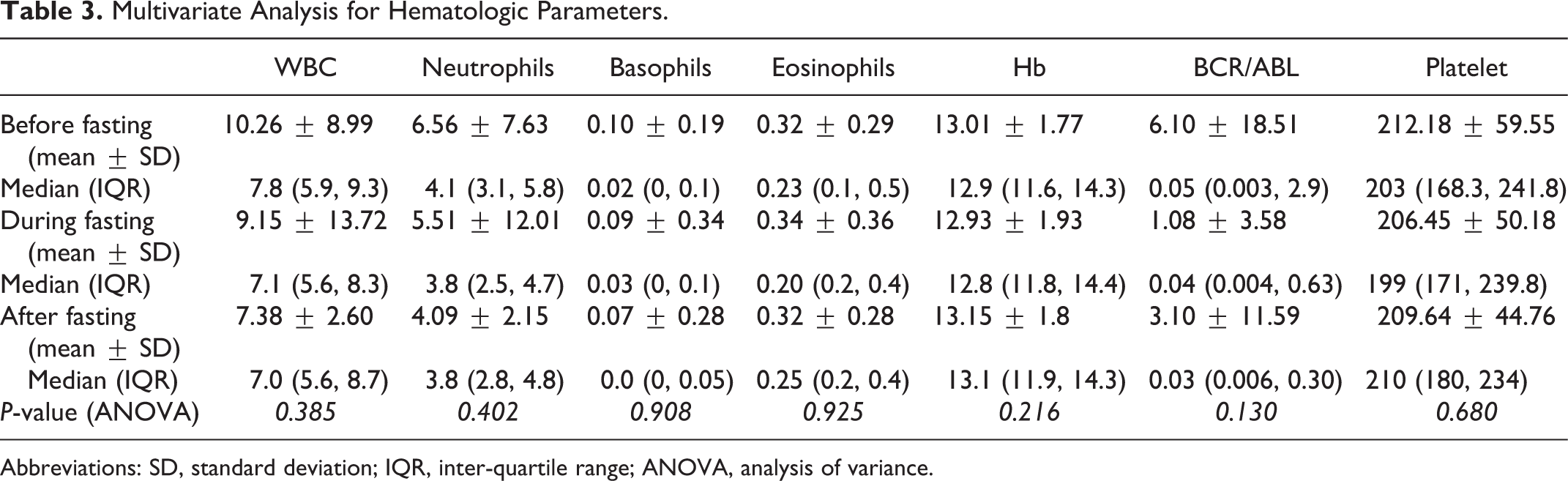
Abbreviations: SD, standard deviation; IQR, inter-quartile range; ANOVA, analysis of variance.
Association Between Various Hematological Parameters With Gender, Age, and Ethnicity
Unpaired t and Mann Whitney U statistical tests revealed that the mean (or median for skewed data distribution) values of most of the hematological parameters among males were observed to be significantly higher compared to females in each before, during and after fasting periods. Age was found to be negatively correlated (low to moderate correlation) with all hematological parameters and BCR-ABL1 levels in each period before, during and after fasting (Pearson correlation (r) ranges from −0.10 to −0.46; P = 0.001 to 0.643). Most of the hematological parameters had lower values in a higher age group (age >60 years) compared to age groups (age ≤40 years and age >40 to 60 years) (Figure 2, Box Plot).
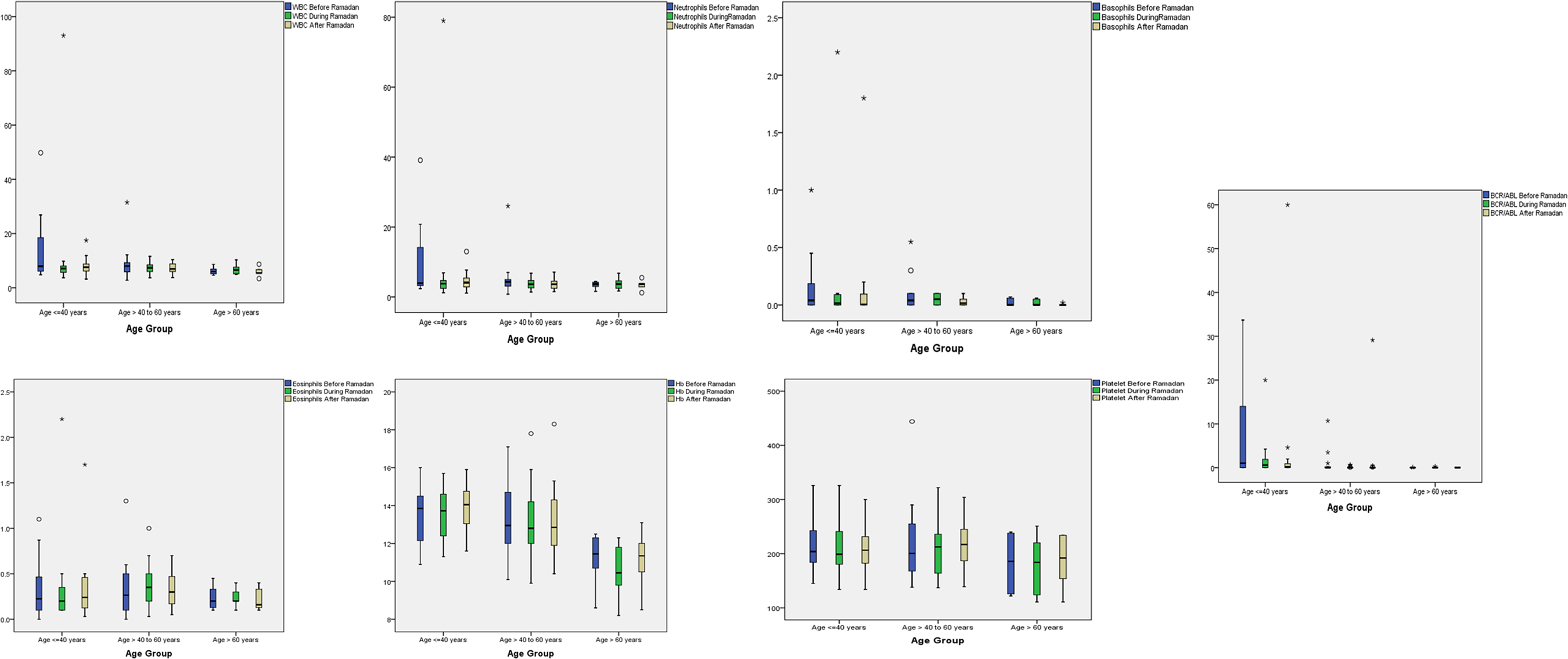
Relationship between various hematological parameters and age across 3 periods.
Hemoglobin (Hgb) levels at both before and after fasting were observed to be significantly higher in patients from the Middle Eastern and Indian subcontinent compared to patients from black Arab ethnicities (Kruskal Wallis test P < 0.05). Whereas, Eosinophils measured before fasting was found to be significantly lower in patients from Middle Eastern compared to the Indian subcontinent and black Arab ethnicities (Kruskal Wallis test P = 0.009). Moreover, other hematological parameters measured did not differ significantly across different ethnicities (P > 0.05) (Figure 3, Box Plot).
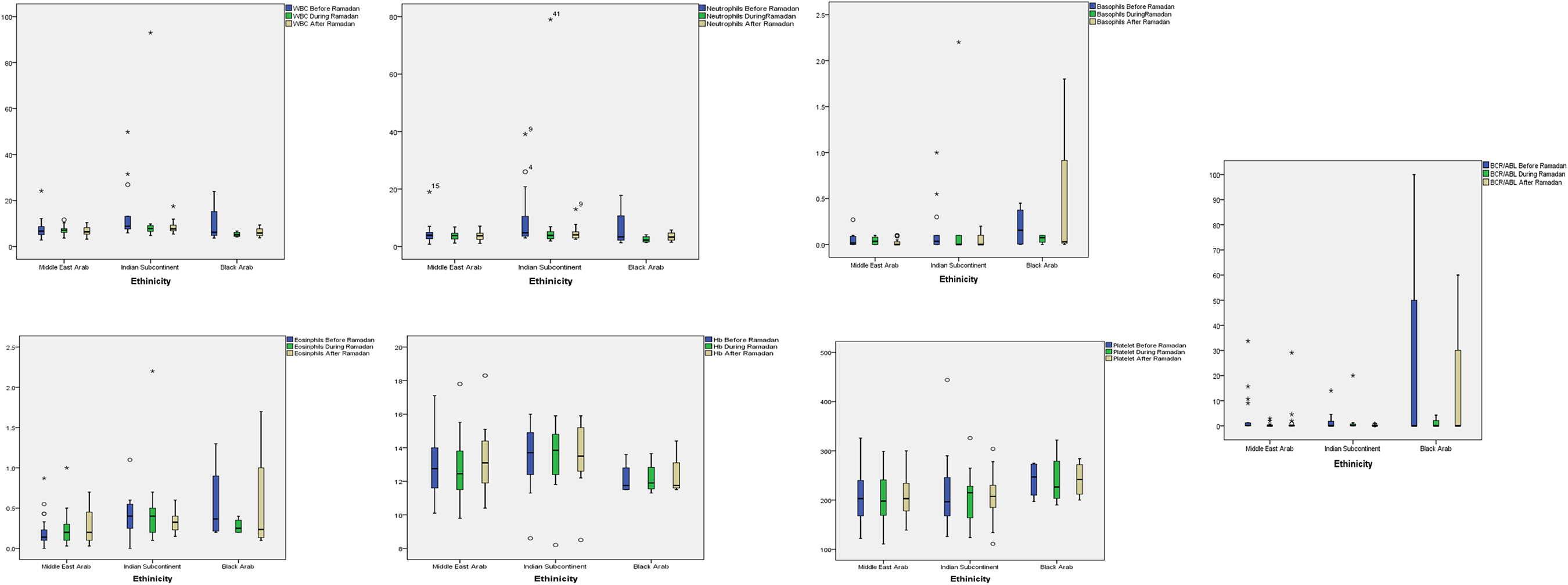
Relationship between various hematological parameters and ethnicity across 3 periods.
Relationship Between Various Hematological Parameters and TKI Across 3 Periods
The mean and SD along with median and IQR for various CBC parameters studied across different types of TKIs and compared within each period (before, during, and after fasting) are presented in Table 3. In all 3 periods (before, during and after fasting), median values of parameters WBC, neutrophils, basophils, eosinophils and BCR-ABL1 were observed to be higher in patients treated with nilotinib compared to imatinib and dasatinib treatment groups. Whereas, parameters like Hgb and platelet count values found to have similar trends and values across 3 treatment groups. However, their differences were statistically insignificant (P > 0.05) (Table 4, Figure 4, Box plot).
Hematologic Parameters and TKIs.

Abbreviations: SD, standard deviation; IQR, inter-quartile range.
* P-value computed using non-parametric Kruskal-Wallis test.
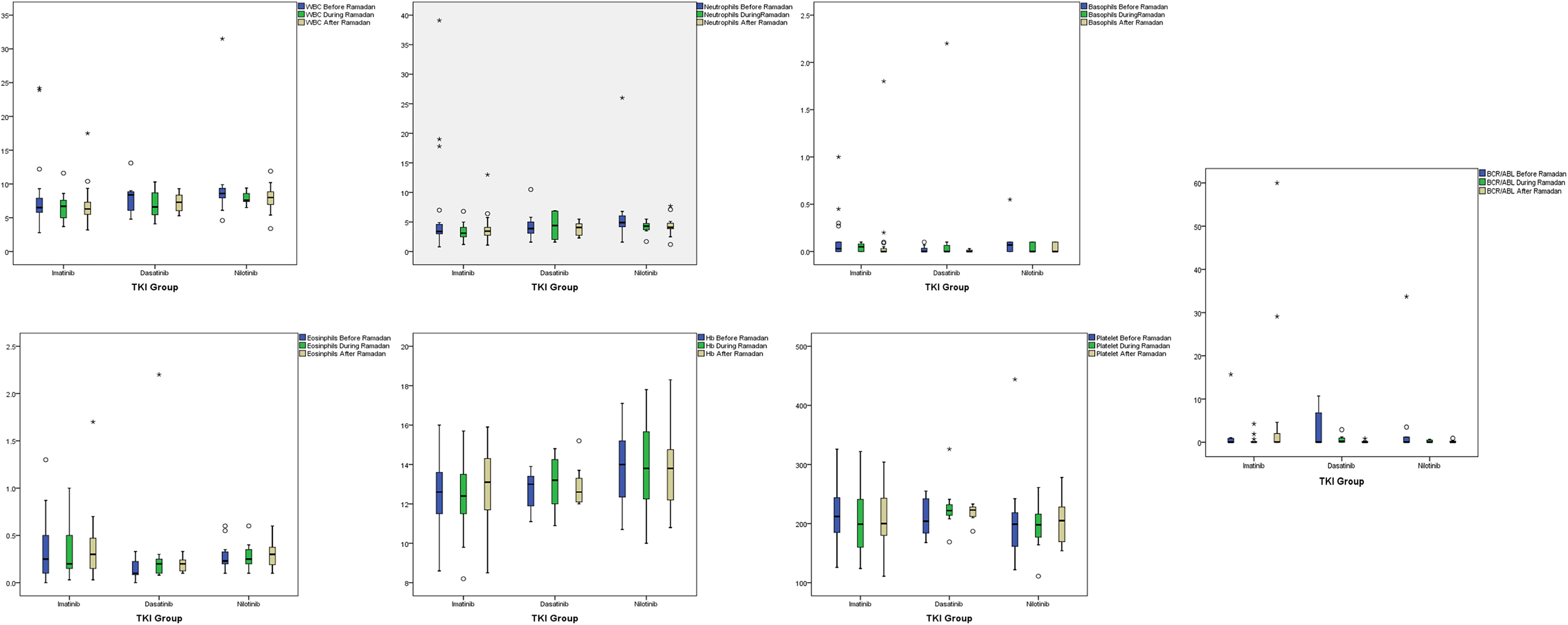
Relationship between various hematological parameters and TKI across 3 periods.
Additional Exploratory Statistical Analysis
TKI and gender
imatinib was used more among females (n = 8, 61.5%), compared to males (n = 17, 48.6%), whereas dastinib (22% vs 7%), and nilotinib (31.4% vs 30.8%) were observed to be used more in males compared to females, however, this difference was noted to be statistically insignificant (P = 0.557).
TKI, age group, and ethnicity
The percentage of patients who treated with imatinib (54% vs 47.1%) or nilotinib (36.5% vs 23.5%) were higher in both age groups
TKI and GI prophylaxis and types of food
There was no statistically significant association observed between various TKIs types and food i.e. large and light meals (P > 0.05). Though statistically insignificant (P > 0.05), GI prophylaxis was noted to be more in imatinib (n = 5, 22.7%) and nilotinib (n = 3, 20%) compared to dasatinib (0%) group respectively. Furthermore, none of the patients reported any TKI related gastrointestinal toxicity during fasting.
Discussion
Different types of fasting have been reported to impact the antitumor effect of chemotherapy. Prolonged fasting (PF, water only for more than 2 days) or of fasting-mimicking diets (FMDs) was shown to enhance the activity of chemotherapy and radiotherapy in preclinical cancer models. 9 -12 However, whether these results can be applied in cancer patients is still to be determined. Despite the importance and relevance of this topic and given the burden of cancer, very few scholars have investigated the impact of fasting on cancer patients, with most of these trials being qualitative.
A small trial conducted in breast cancer patients found that women who fasted 24 hours before and after TAC (docetaxel, doxorubicin, and cyclophosphamide) chemotherapy cycles experienced less hematological toxicity than women assigned to a regular diet. 13 Moreover, in a small case series, patients who underwent chemotherapy with fasting reported a reduction in chemotherapy fatigue and weakness while fasting. 10 Dorff et al investigated 20 cancer patients who are receiving platinum-based chemotherapy regimens with 3 different fasting periods (24, 48 and 72 hours) in a dose-escalation and feasibility study. Fasting was found to be safe and feasible for cancer patients with some preliminary evidence of reduced DNA-damage evident in host leukocytes after chemotherapy exposure for subjects who fasted for 72 hours. These studies were limited by the small sample size. 14
Up to date, limited data is published exploring the effect of intermittent fasting on cancer patients. In King Fahad Medical City, a small trial was conducted to evaluate the safety and feasibility of combining chemotherapy and intermittent fasting during Ramadan. Eleven patients were followed, side effects and blood counts were compared with values measured in response to a similar dose of chemotherapy, given 2 weeks after the end of Ramadan. The authors concluded that combining fasting and chemotherapy during the month of Ramadan was well tolerated and safe and patients reported fewer side effects. 15
Several factors can make CML as one of the most challenging conditions to manage during intermittent fasting. First, TKIs that are used in CML have distinctive pharmacokinetic properties in which some of these agents might interact with food and ultimately affect drug absorption. For instant imatinib and bosutinib should be taken with food to reduce gastrointestinal irritation. In pharmacokinetic studies, imatinib administration with food resulted in an absolute bioavailability of 98%; achieves maximum plasma concentration approximately 2-4 hours in normal conditions; while ingestion a high-fat meal can prolong the uptake and therefore the time to reach a maximum plasma concentration (t max). 16 The administration of dasatinib and ponatinib is not affected by food, while nilotinib needs to be taken without food. 17,18 Furthermore, optimum administration of TKIs and dosing schedule during the holy month is not well defined until now, particularly in the case of nilotinib, patients are counseled not to eat 2 hours before and one hour after taking the medication. Especially in Ramadan, the twice-daily dosing of nilotinib in the absence of food can be challenging for CML patients. 7,19 -21 In addition, drug interactions can be problematic for many patients especially those who experience dyspeptic symptoms, which requires empirical therapy with proton pump inhibitors (PPIs).
Drug compliance is also considered an essential factor. As noticed by some scholars, drug compliance during intermittent fasting tends to fall and patients are less likely to adhere to their treatment schedules. 20 -22 A Malaysian study assessing tyrosine TKIs use in CML patients 7 reported that Muslim patients receiving TKI therapy frequently skipped or changed doses of nilotinib, which needed to be taken twice daily, in order to fulfill their religious obligations during Ramadan. The potential effect of this poor compliance on treatment success is concerning. In this study, patients also reported going against the advice of doctors when advised not to fast. 20 -22
Our study is the first qualitative study that reports the effect of intermittent fasting on CML patients who are receiving TKIs. In our study, the use of TKIs during fasting did not result in significant changes in hematological indices nor in BCR-ABL levels. It has been reported in the literature that the effect of TKIs is enhanced by fasting due to the inhibition of the mitogen-activated protein kinase signaling pathway. 11 For instance, fasting was shown to potentiate the effect of sorafenib in decreasing hepatocellular carcinoma cell proliferation and glucose uptake, while normalizing the expression levels of genes commonly altered by sorafenib itself in hepatic cancer. 23
Our results confirm the feasibility of fasting accompanying TKIs as patients’ responses were not affected during intermittent fasting, Moreover, there was no statistically significant association observed between various TKIs types and food i.e. large and light meals. Though, statistically insignificant, a few patients reported using PPIs during fasting, with most patients receiving imatinib.
There is a distinct paucity of scientific and clinical data investigating the effect of fasting in hematological malignancies. 20,21,24 From the limited data available, Muslim patients with hematological malignancies are less likely to fast than those with solid tumors; nevertheless, the data also clearly demonstrates that a proportion of patients who are on active treatment will attempt to practice intermittent fast. The management of CML patients who are willing to fast is complex and should involve a multidisciplinary team, who should be aware of the importance of cultural and spiritual beliefs of Muslim patients and their abilities to fast.
Limitations of the Study
This is a pilot phase, so our team is planning to do a multi-center study with an appropriate sample size.
Only one type of intermittent fasting studied (16/8), other types of intermittent fasting need to be explored, which is planned to be an extension phase of this study.
Assessment of side effects during fasting shall be considered to investigate the impact of fasting on treatment tolerance and quality of life.
Conclusion
TKIs use during intermittent fasting is poorly studied. This study demonstrates that the use of TKIs during fasting did not result in significant changes in hematological indices or BCR-ABL1 levels. Patients who wish to practice intermittent may be reassured in this regard. Yet, physicians can adopt the safe trial approach, where they allow the patients to fast, but with instructions regarding when and how to break fasting.
Footnotes
Authors' Note
All data generated or analyzed during this study are included in this published article. The article describes an original article. This project has been approved by the IRB in Hamad Medical Corporation (MRC-01-18-411) and has been performed in accordance with the ethical standards noted in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. No consent was required to participate. TKIs use during fasting is poorly studied. The finding of this study highlighted that the use of TKIs during fasting did not result in significant changes in hematological indices nor in BCR-ABL levels. Therefore, patients with CML who wish to practice intermittent fasting should receive clear instructions regarding when and how to break fasting.
Acknowledgment
Authors would like to acknowledge European LeukemiaNet, as this project is the pilot phase of ELN project (Effect of fasting on response to TKI in patients with CML).
Author Contributions
MAY, RSG, MBA, MAA, HMS, AJN, NK, SJA: Data Collection, Literature Search, Manuscript Preparation. PC: Data Analysis, Manuscript Preparation. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This study has been funded by Hamad Medical Corporation.