
Abstract
Tyrosine kinase inhibitors (TKIs) are the mainstay of treatment for chronic myeloid leukemia (CML). Patients enrolled in clinical trials investigating the safety and efficacy of TKIs in CML are generally younger, have fewer comorbidities, and are monitored differently than patients treated in the real world. This narrative literature review summarizes efficacy outcomes (complete cytogenetic response, major molecular response, and disease progression) and safety outcomes (duration of TKI therapy, TKI discontinuation rates, dosage changes, and frequently reported adverse events) from landmark clinical trials as well as real-world studies. Patients with CML treated with TKIs in a real-world setting may achieve different rates of specific response milestones than those treated on clinical trials. While real-world studies reported similar overall incidences of adverse events as clinical trials, real-world patients with CML were more likely to discontinue TKIs due to adverse events.
Introduction
Chronic myeloid leukemia (CML) is a pluripotent hematopoietic stem cell disorder which accounts for approximately 15% of all cases of leukemia in adults and is characterized by the reciprocal translocation of chromosomes 9 and 22, also known as the Philadelphia chromosome. Translocation produces the BCR-ABL1 fusion gene that encodes a constitutively active tyrosine kinase, leading to uncontrolled cell proliferation and resistance to apoptotic signaling. 1 Since the initial development of a BCR-ABL tyrosine kinase inhibitor (TKI), TKIs have remained the mainstay of treatment for CML.
National Comprehensive Cancer Network (NCCN) and European LeukemiaNet (ELN) guidelines currently recommend four TKIs for first-line treatment of CML: imatinib, nilotinib, dasatinib, and bosutinib.2,3 Treatment choice is based on CML phase at initiation as well as patient-specific characteristics, such as medication adverse event profiles, comorbidities, concomitant medications, and financial considerations. Prognostic risk stratification through Sokal, Hasford, or EUTOS risk scores is also considered. Response to TKIs is monitored using several different criteria: hematologic, cytogenetic, and molecular response. Achievement of complete cytogenetic response (CCyR) within 12 months on first-line TKI therapy is an established predictor of long-term survival. 2 While many landmark clinical trials used conventional bone marrow cytogenetics as the method of monitoring response, quantitative RT-PCR (qPCR) performed on peripheral blood has become the most commonly utilized method of evaluating response to TKIs in CML. Major molecular response (MMR), or a 3-log reduction in detectable BCR-ABL mRNA assessed by qPCR, is associated with a decreased risk of disease progression and a higher likelihood of achieving deep molecular response allowing for consideration of discontinuation of TKI therapy and pursuit of treatment-free remission. 2
First-line BCR-ABL TKIs have proven to be highly effective therapies, all associated with 5-year overall survival (OS) rates greater than 90%.4–6 However, much of the data currently available are derived from clinical trials, where patient populations and safety and efficacy monitoring are tightly controlled. These studies are not completely representative of the real-world CML population, enrolling patients with a median age of 10 years younger than patients treated in the real world and often excluding patients with significant comorbidities and higher ECOG scores. 7 As many as 60% of real-world patients with CML are estimated to be excluded from enrollment in landmark clinical trials, suggesting that a large percentage of real-world patients are not represented in these studies. 8 Additionally, pursuant to the 21st Century Cures Act, the United States Food and Drug Administration (FDA) has developed a program framework to incorporate real-world evidence in regulatory decision making. 9 As real-world data becomes more prevalent, the need to bridge the gap between clinical trial data and real-world data in CML becomes increasingly valuable.
This narrative review provides a comprehensive summary of efficacy and safety outcomes associated with TKIs for treatment of CML for patients treated on landmark clinical trials as well as those treated in real-world settings.
Materials and methods
Study design
This review included published full-text data of observational as well as landmark randomized phase II and III studies of patients receiving both first and subsequent-line TKI therapy for CML. Efficacy outcomes evaluated in this study included CCyR, MMR, and rate of disease progression. Safety outcomes evaluated included the average duration of TKI therapy, rate of TKI discontinuation, TKI dose adjustments, and reported adverse events.
Search methods
A search of PubMed and Embase was performed with the following Boolean queries:
Tyrosine kinase inhibitor AND real world AND chronic myeloid leukemia (Imatinib OR nilotinib OR dasatinib OR bosutinib OR ponatinib) AND real world AND chronic myeloid leukemia
The titles and abstracts of each study were manually screened. Inclusion criteria were as follows: retrospective study design, real-world patient population, assessment of efficacy or safety of any TKI FDA approved for treatment of CML, published at the time of data collection (August 31st, 2021). All other clinical trials or studies reporting any exclusion criteria were not included. Landmark phase II and III studies for each TKI were also assessed in this review. Reference lists were also investigated for additional studies.
Statistical methods
Included studies were categorized into two groups based on their focus on TKI efficacy or safety. Descriptive statistics were used to characterize the patient population, efficacy outcomes, and safety outcomes of each study.
Results
Efficacy
A total of five studies met inclusion criteria and evaluated the efficacy of TKIs in real-world patients, two of which evaluated first-line TKI therapies and three of which evaluated second- or subsequent-line TKIs.10–14 Seven landmark phase II or III clinical trials (three of first-line therapy and four of second-line therapy) were analyzed for efficacy outcomes.4–6,15–18 Demographic and baseline characteristics from each study of first-line TKI treatment of CML are summarized in Table 1. Complete efficacy data for each study of first-line TKI therapy are reported in Table 2.
Baseline data from first-line TKI studies.
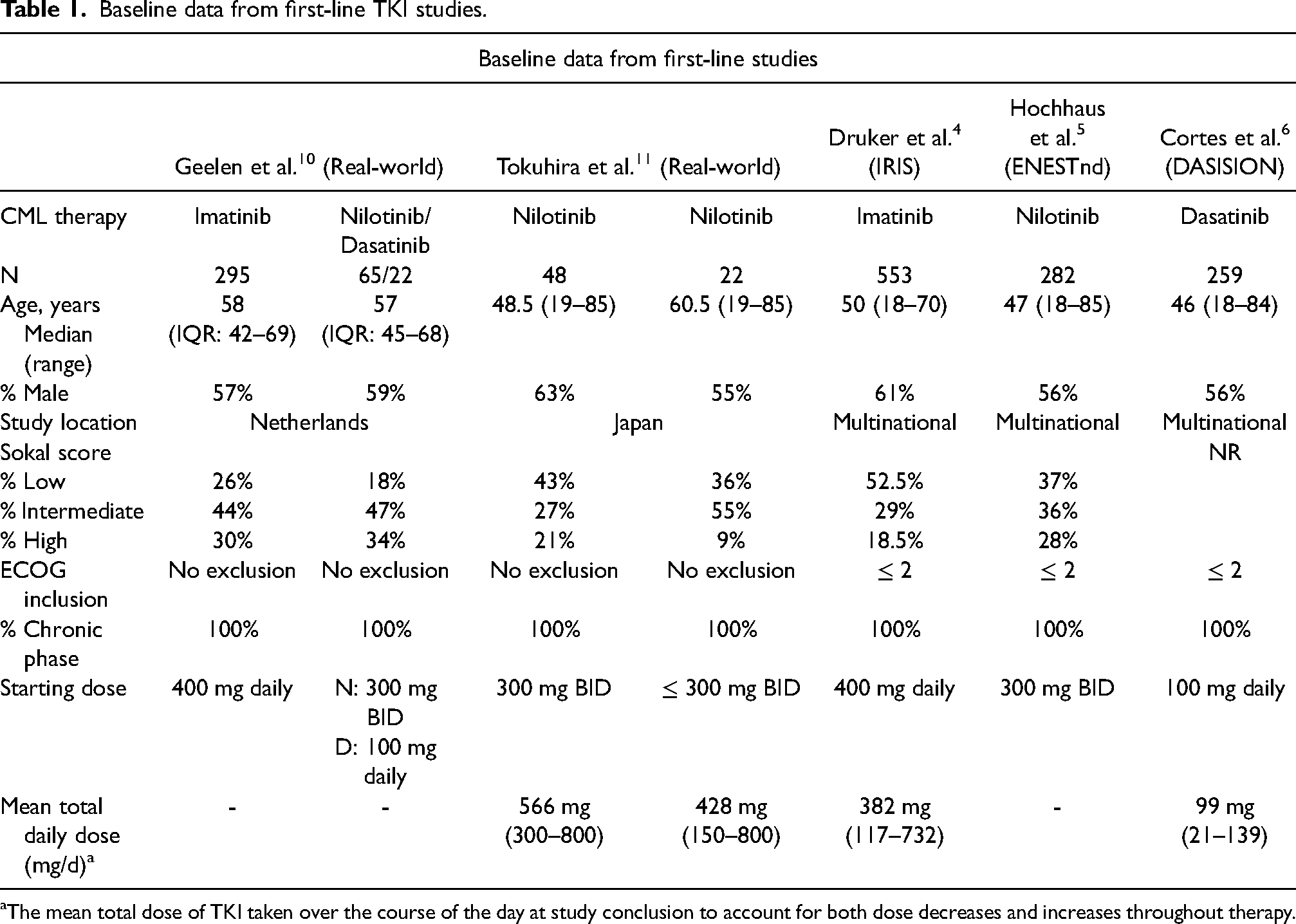
The mean total dose of TKI taken over the course of the day at study conclusion to account for both dose decreases and increases throughout therapy.
Efficacy outcomes of first-line TKI studies.
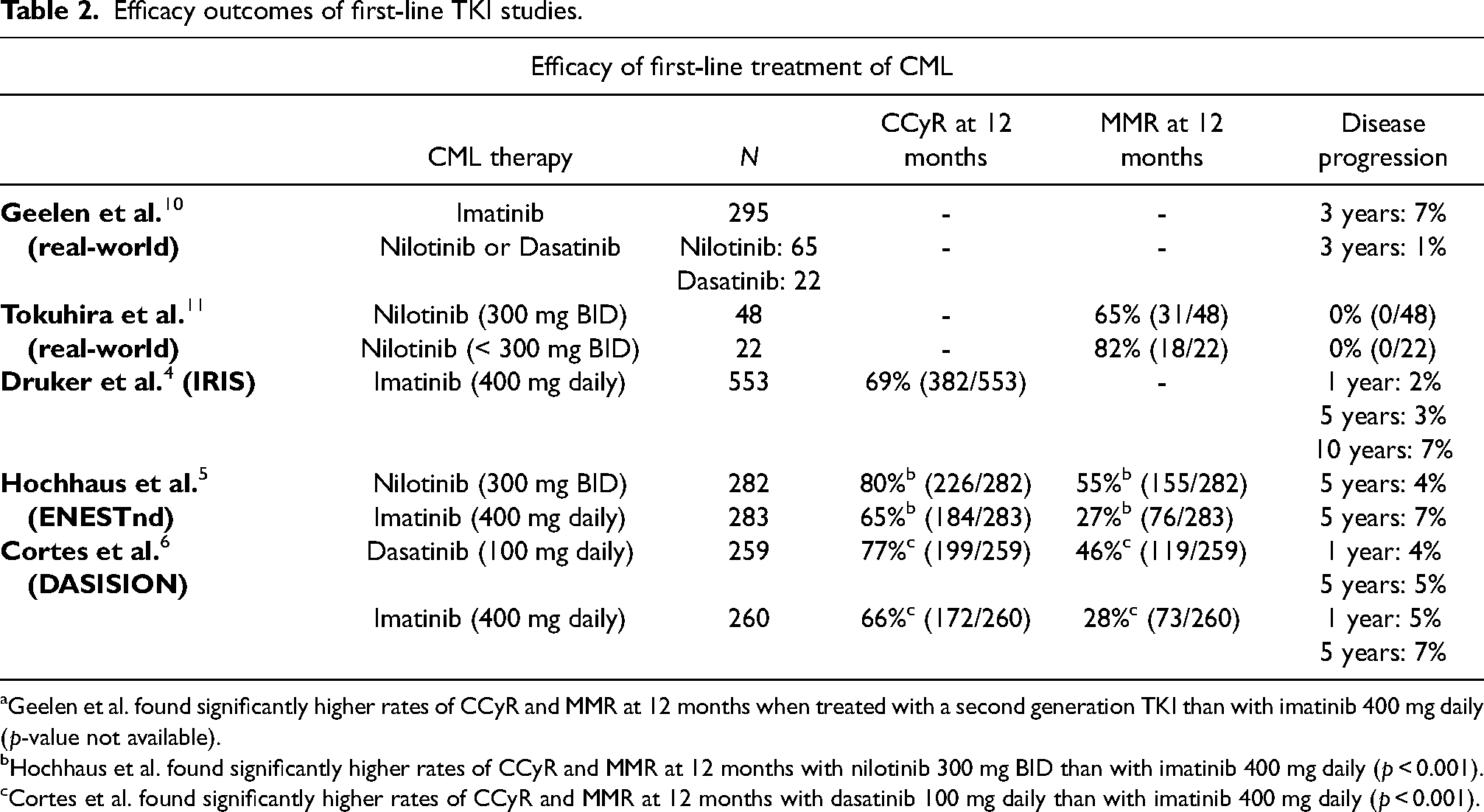
Geelen et al. found significantly higher rates of CCyR and MMR at 12 months when treated with a second generation TKI than with imatinib 400 mg daily (p-value not available).
Hochhaus et al. found significantly higher rates of CCyR and MMR at 12 months with nilotinib 300 mg BID than with imatinib 400 mg daily (p < 0.001).
Cortes et al. found significantly higher rates of CCyR and MMR at 12 months with dasatinib 100 mg daily than with imatinib 400 mg daily (p < 0.001).
Imatinib was consistently the most prescribed first-line TKI in real-world studies (75–90% of patients).7,10,19 In one real-world study investigating patients treated with first-line imatinib, 7% of patients experienced disease progression to accelerated or blast phase CML at 3 years. 10 CCyR and MMR rates associated with first-line imatinib were not reported in this real-world study. In the landmark phase III clinical trial (IRIS), 69% of patients achieved CCyR at 12 months and 3% of patients experienced disease progression after 5 years and 7% after 10 years of follow-up. 4 MMR was not reported in the IRIS study. However, long-term follow up of the phase III ENESTnd study comparing frontline imatinib to nilotinib reported that 27% of patients receiving imatinib achieved MMR at 12 months. 5
Nilotinib was the second most commonly reported TKI used in the frontline setting in included real-world studies.10,11 In patients treated first-line with nilotinib in the real world, 70% achieved MMR at 12 months compared to 55% of patients treated on the ENESTnd clinical trial with long-term follow-up.5,11 Patients in this real-world study who were older than 65 years underwent a pre-emptive dose reduction to prevent adverse events. Limited data was available regarding 12-month CCyR rates for first-line nilotinib in the real world and thus could not be compared to available clinical trial data. There is currently insufficient real-world efficacy data for first-line dasatinib and bosutinib.
There are several studies investigating the efficacy of second- and subsequent-line TKI therapy in real-world patients with CML. Demographic data from each of these studies are summarized in Table 3. Complete efficacy data for each study of second- or subsequent-line TKI therapy are reported in Table 4.
Baseline characteristics of second- or subsequent-line TKI studies.
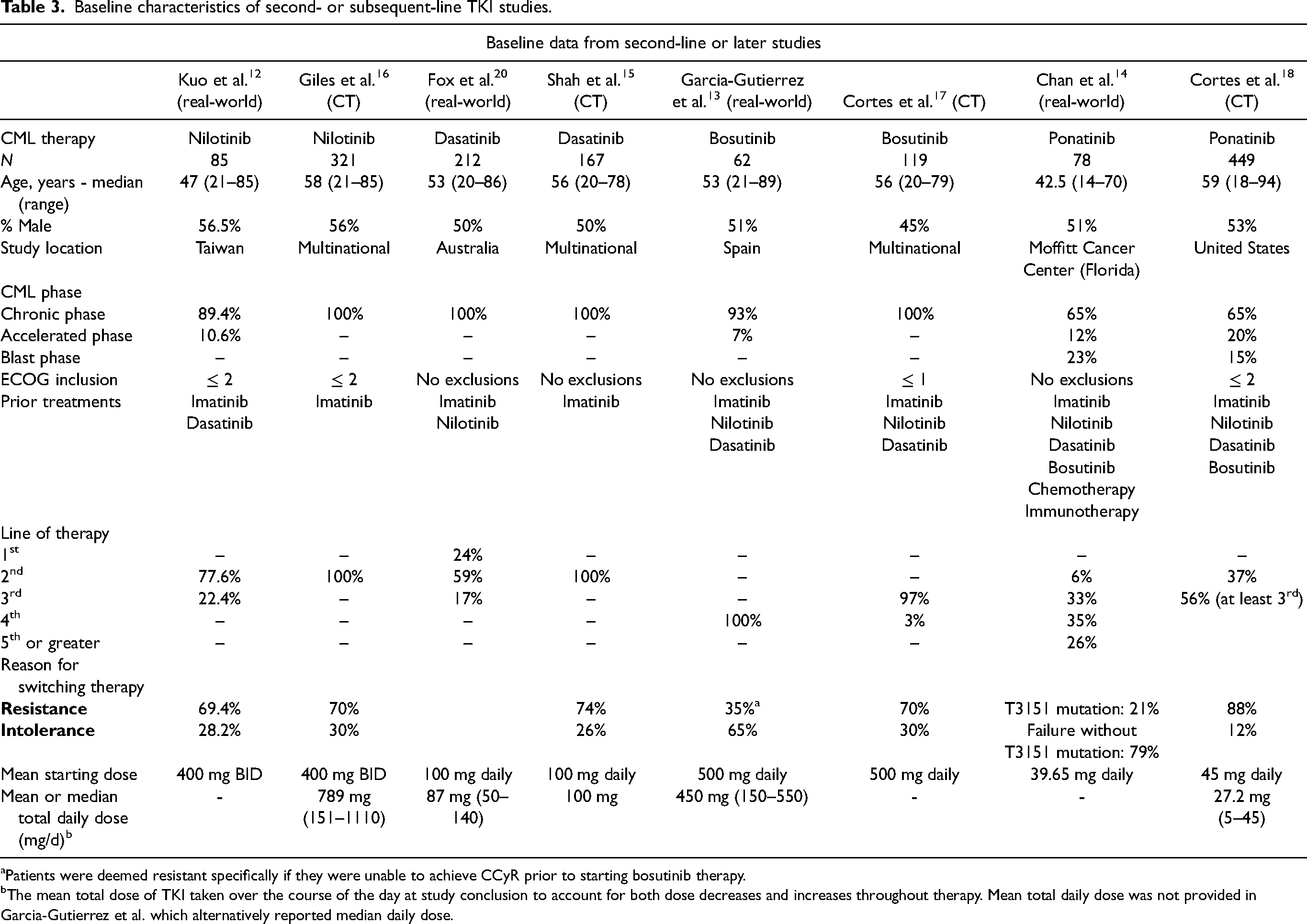
Patients were deemed resistant specifically if they were unable to achieve CCyR prior to starting bosutinib therapy.
The mean total dose of TKI taken over the course of the day at study conclusion to account for both dose decreases and increases throughout therapy. Mean total daily dose was not provided in Garcia-Gutierrez et al. which alternatively reported median daily dose.
Efficacy outcomes of second- and subsequent-line TKI studies.
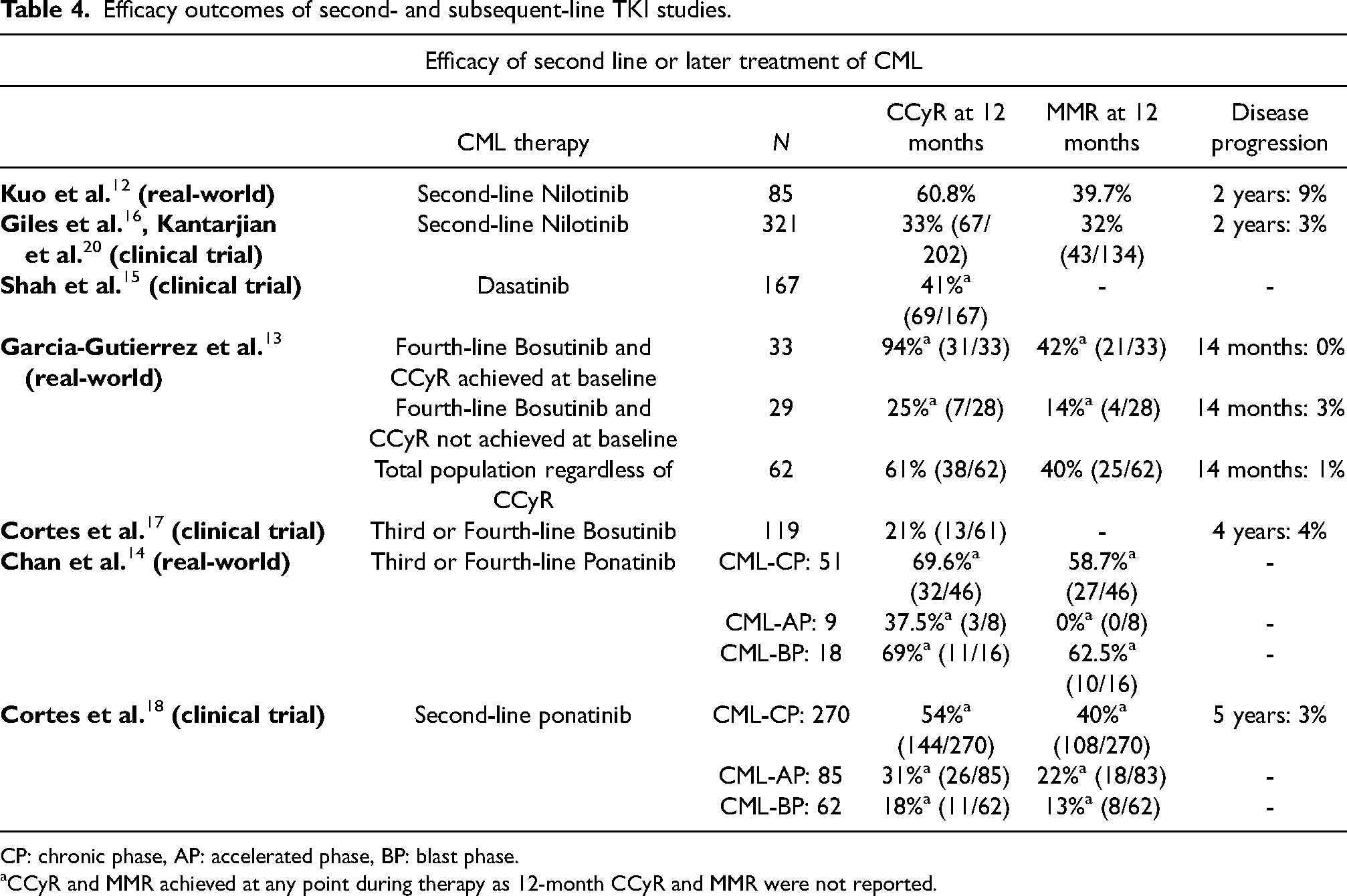
CP: chronic phase, AP: accelerated phase, BP: blast phase.
CCyR and MMR achieved at any point during therapy as 12-month CCyR and MMR were not reported.
Nilotinib is commonly used as second-line therapy after patients develop resistance or intolerances to first-line treatment. In one real-world study investigating Taiwanese patients treated with second-line nilotinib, 60.8% of patients achieved CCyR at 12 months and 39.7% of patients achieved MMR at 12 months. 12 While this study was labeled as a non-interventional, prospective study, participants were still chosen intentionally based on inclusion criteria, so it may not be fully representative of a real-world population. Alternatively, in a phase II clinical trial setting, 33% of patients treated with nilotinib following imatinib resistance or intolerance achieved CCyR at 12 months and 32% of patients achieved MMR at 12 months.16,20
While bosutinib is an approved first-line therapy for CML, the only available real-world study examines the medication as a fourth-line agent after resistance or intolerance to imatinib, nilotinib, and dasatinib therapy. For patients who had already achieved CCyR prior to starting bosutinib, 94% maintained CCyR for the duration of therapy and 42% achieved MMR at any point during therapy over a median follow-up time of 14.3 months. For patients who had not achieved CCyR on prior therapy, 25% were able to achieve CCyR and 14% were able to achieve MMR at any point during treatment. Rates of 12-month CCyR and MMR were not reported in this study. 13 There are no currently published clinical trials evaluating bosutinib in solely the fourth-line setting, however in a phase I/II study evaluating bosutinib in the third- or fourth-line setting, 21% of patients achieved CCyR at 12 months. Rates of MMR were not reported in this clinical trial. 17
Ponatinib is only FDA approved for chronic-phase (CP) CML with resistance or intolerance to at least two prior TKIs or for T315I mutation-positive CML. The only available real-world study examines ponatinib as a third- or fourth-line agent. Of patients with CP-CML, 69.6% achieved CCyR and 58.7% achieved MMR at any point while on ponatinib. Rates of CCyR or MMR at 12 months were not reported in this study. 14 There are no currently published clinical trials evaluating ponatinib in the third- or fourth-line setting. However, the phase II PACE trial evaluated ponatinib for patients with resistance or intolerance to a second-generation TKI. Of the patients with CP-CML, 54% achieved CCyR and 40% achieved MMR at any point while on ponatinib. Rates of CCyR or MMR at 12 months were not reported in this study. 18
Safety
A total of seven studies met inclusion criteria and evaluated the safety of TKIs in real-world patients.7,10,11,13,19,21,22 Five landmark phase II or III clinical trials were analyzed for safety outcomes.4–6,15,17
Changes and discontinuations of TKI therapy were the most commonly reported measures of safety and tolerability in real-world studies. TKI discontinuation rates and change of TKI reported in real-world studies and clinical trials are shown in Table 5. Based on limited available data and lack of clear reasons for discontinuation in many studies, a combined endpoint of discontinuation of therapy or change in TKI was assessed. Discontinuation rates and dose adjustments reported in real-world and clinical trials were further compared in Figure 1. There are currently no available real-world discontinuation data for ponatinib.
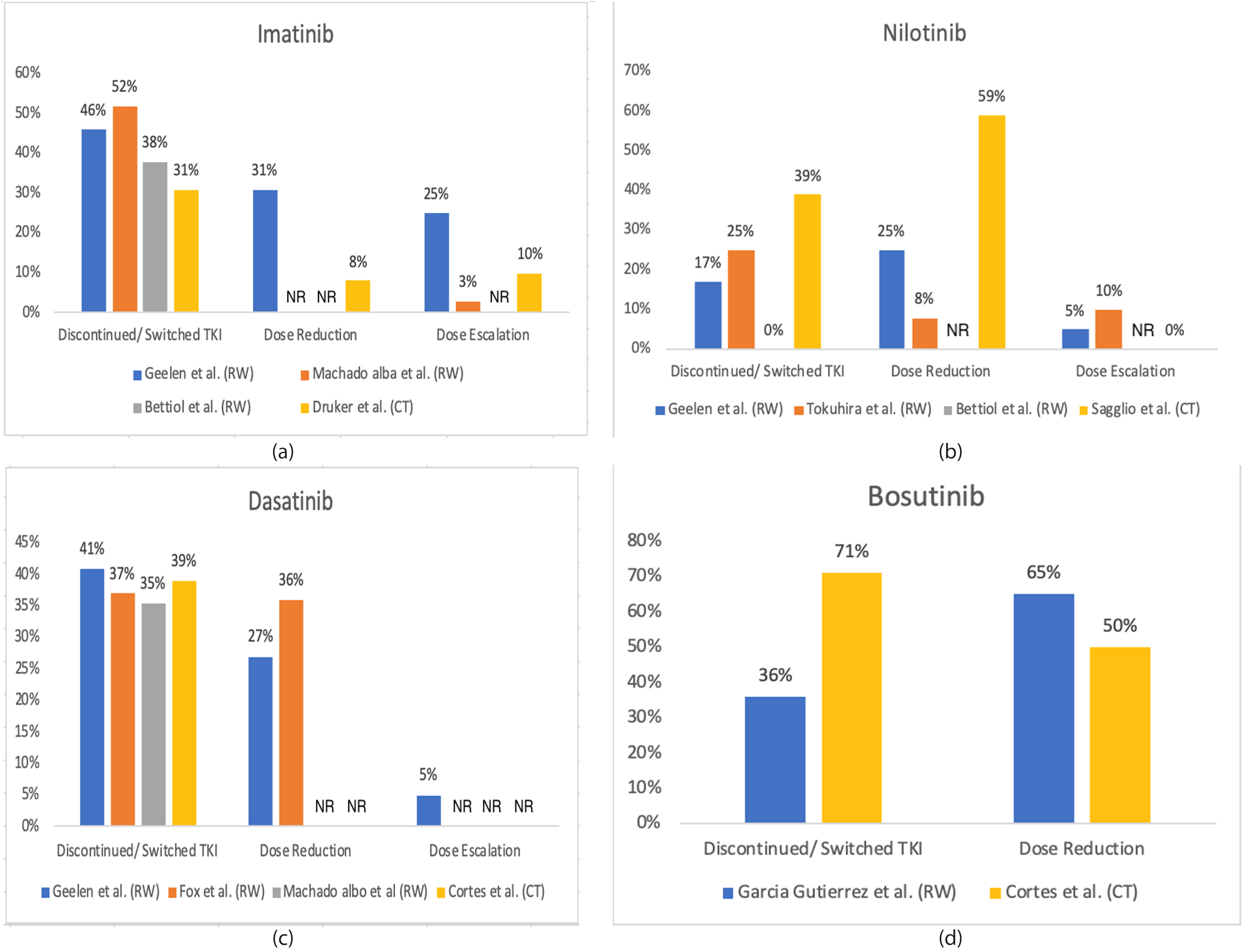
Real-world (RW) versus clinical trial (CT) data: TKI discontinuation, dose reduction, or dose escalation for first-line TKIs. (a) imatinib, (b) nilotinib, (c) dasatinib, and (d) bosutinib. “NR”: data not reported.
Safety outcomes of TKI studies.
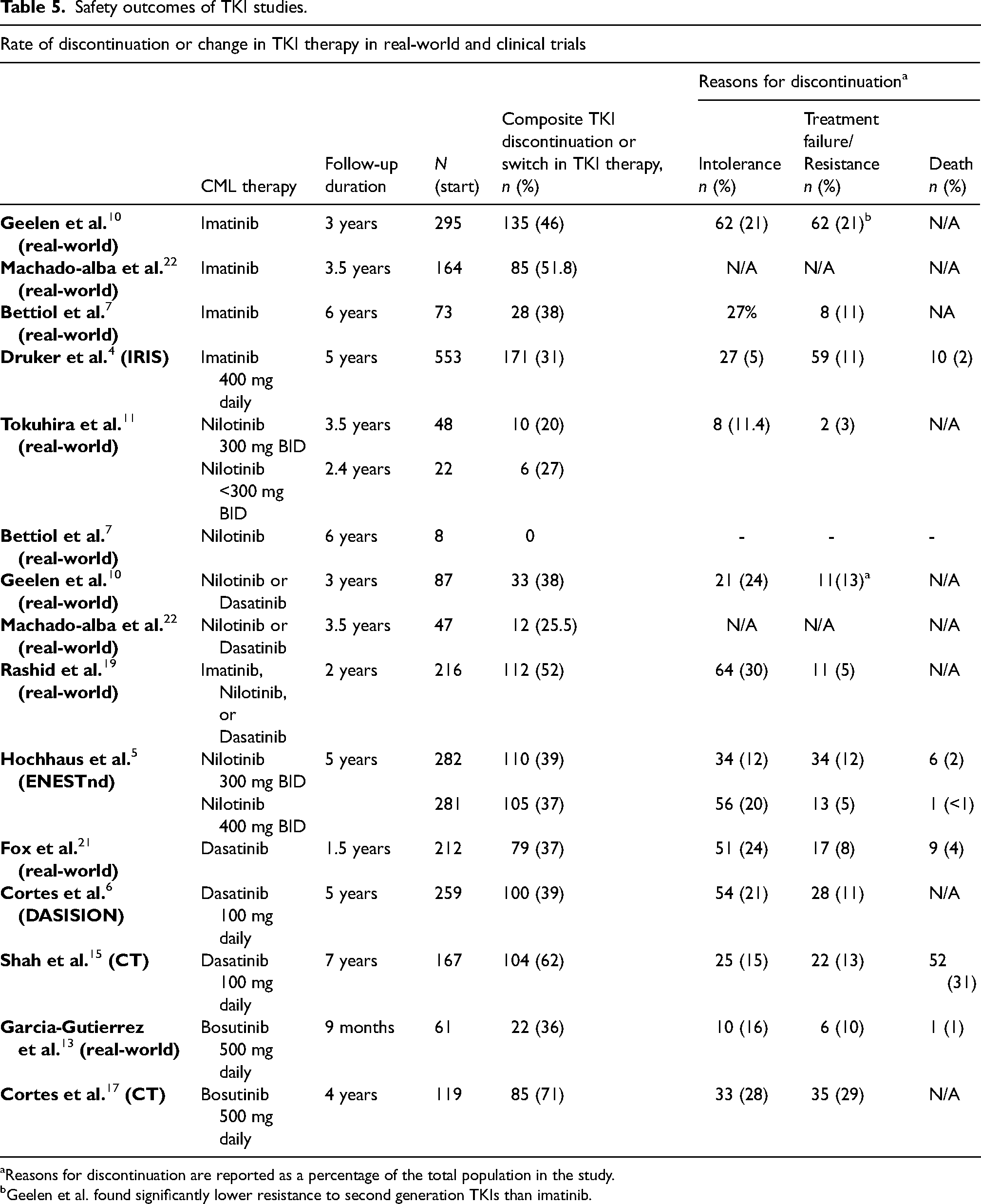
Reasons for discontinuation are reported as a percentage of the total population in the study.
Geelen et al. found significantly lower resistance to second generation TKIs than imatinib.
While imatinib is the most prescribed first-line TKI, it is also associated with a relatively high rate of discontinuation and transition to second-line therapy. In two real-world studies investigating first-line imatinib, 46% of patients required a switch in TKI therapy for any reason within the first 3 years, and 51.8% within the first 3.5 years.10,22 In another real-world population-based study of first-line TKI therapy, significantly more patients receiving imatinib discontinued treatment due to resistance or treatment failure than those receiving a second generation TKI (21% vs 13%, p=0.046). 10 For comparison, in the phase III trial IRIS, 31% of patients required a switch in TKI therapy for any reason within the first 5 years. 4 While the rate of discontinuation of imatinib due to resistance or treatment failure was higher in the real world than that reported in the IRIS study, rate of discontinuation of second generation TKIs in the real world were consistent with clinical trial data from ENESTnd and DASISION.
In real-world population-based studies of second generation TKIs used for first-line therapy, between 48% and 80% of patients were reported to remain on initial therapy, with median follow-up times ranging from 1.5 years to 3.5 years.10-11,19,21,22 Nilotinib, dasatinib, and bosutinib were associated with real-world discontinuation rates of 20%, 37%, and 36%, respectively, at their recommended starting doses.11,13,21 Across all studies, the most common reason for a switch in TKI therapy was intolerance followed by treatment failure. Clinical trial data reported 5-year discontinuation rates for any reason of 39%, 39%, and 71% for these second generation TKIs respectively, with median follow-up times ranging from 4 to 5 years.5-6,17 Real-world studies reported higher rates of TKI dose adjustments than clinical trial data for imatinib, dasatinib, and bosutinib as demonstrated in Figure 1.
Reported adverse events in real-world studies as well as clinical trials are listed in Table 6. Many real-world adverse events were consistent with clinical trial data for all five TKIs, with a few exceptions. In real-world studies of imatinib and nilotinib, fewer gastrointestinal adverse events such as diarrhea, abdominal pain, nausea, and vomiting were reported than in clinical trials. Regarding hematologic toxicities, neutropenia was rarely reported in real-world studies.
Safety outcomes and reported all grade adverse events of TKI studies.
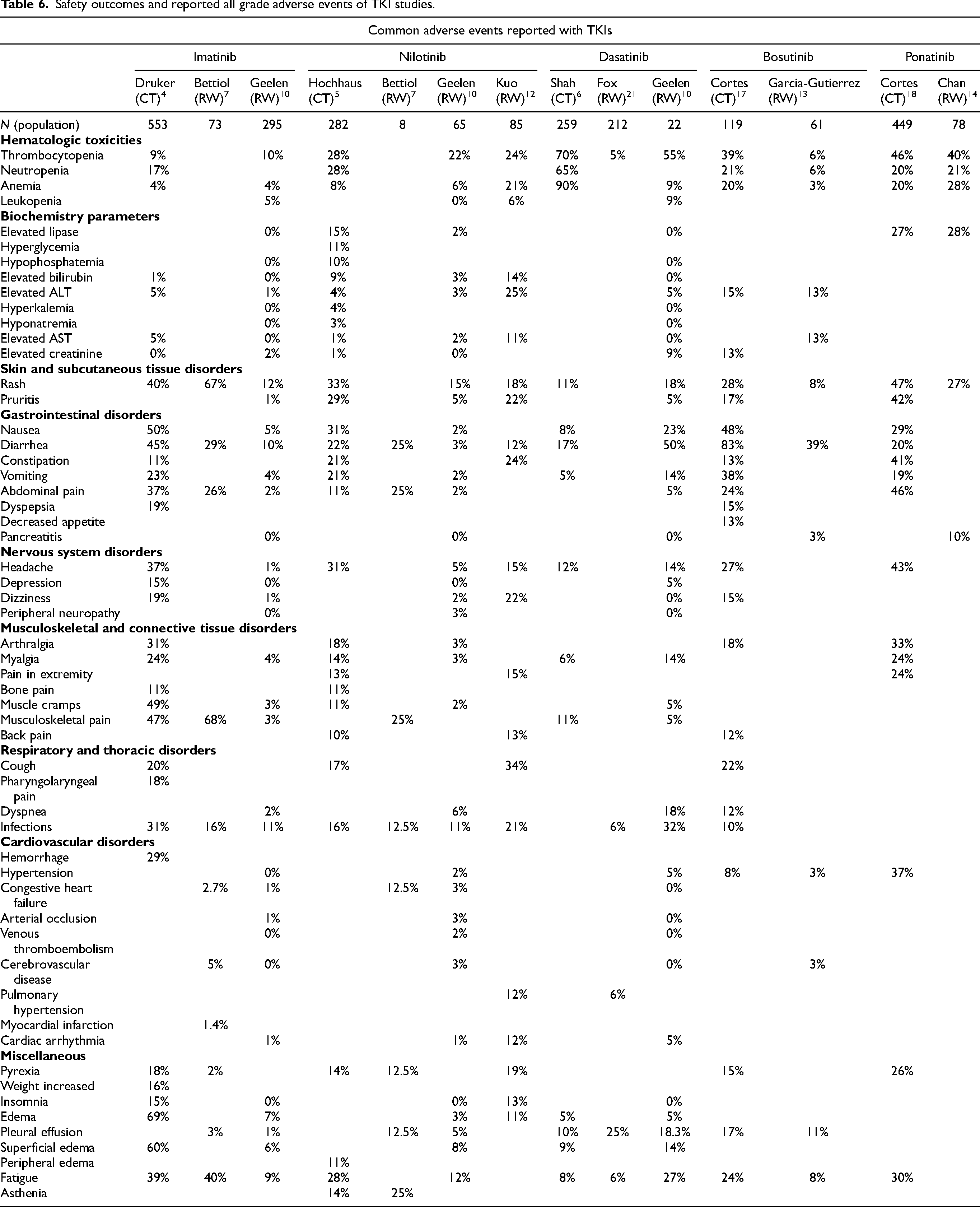
There were several notable medication-specific differences in reported adverse events. Imatinib was more commonly associated with osteoarticular pain in the real world (67% of patients) compared to 47% reported incidence in clinical trials. However, patients receiving imatinib in the real world reported less edema, fatigue, weight changes, and hemorrhage than patients enrolled in clinical trials.4,7,10 In real-world studies, between 31% and 70% of patients experienced an adverse event while receiving nilotinib. However, adverse events improved when dose adjustments were made, with only 27% of patients experiencing recurrence of the adverse event after dose adjustment. 11 Notable reported adverse events by real-world patients receiving nilotinib include pleural effusion (5–12.5%) and heart failure (3–12.5%) which were reported more commonly in real-world studies than in clinical trials (1.8% and 0%, respectively).5,7,10, 12
Similar to imatinib and nilotinib, differences in AEs between clinical trials and real-world studies were observed with dasatinib. Approximately 55% of real-world patients reported experiencing an adverse event while receiving dasatinib. Pleural effusion occurred in 13.8–25% of patients in real-world studies, compared to 12% in clinical trials. Pleural effusions were the predominant cause of dasatinib therapy cessation and were more commonly associated with older age and higher dasatinib doses.10,21 Pulmonary hypertension is another significant adverse event reported; however, this was found to be reversible with discontinuation of treatment. 21 Interestingly, for bosutinib, adverse events were reported at a lower rate in the real-world setting, leading to a much lower discontinuation rate than in clinical trials.13,17 However, comparison of adverse events associated with bosutinib is somewhat limited due to available real-world data.
Discussion
There have been several published reviews summarizing clinical trial safety and efficacy data for TKIs in the treatment of CML. However, patients included in clinical trials are closely monitored and may not fully represent patients who are treated in the real-world setting. To the authors’ knowledge, this is the first comprehensive narrative literature review evaluating reported safety and efficacy outcomes of TKI therapy in both real-world studies and landmark clinical trials.
Differences between real-world and clinical trial patient populations are evident in demographic data and baseline characteristics. The median age of patients in most real-world studies was approximately 10 years older than patients included in landmark clinical trials. However, in some efficacy studies, especially those performed in Asian countries, the median age of patients in real-world studies was 10–15 years younger than patients included in landmark clinical trials.12,14 Of note, the median age of patients in all real-world studies and clinical trials included in this review was younger than the median age at diagnosis for CML in the US (64 years). 1 Additionally, the majority of real-world studies did not contain ECOG exclusion criteria, while clinical trials generally excluded patients with an ECOG score ≥3, representing a trial population with superior functional status.
Efficacy outcomes including rates of CCyR and MMR varied between real-world studies and clinical trials. Formal statistical analyses could not be performed due to the limited number of available real-world studies evaluating each TKI. However, numerical differences in the rates of 12-month CCyR and MMR between real-world and clinical trial patients warrant future investigation.
Clinical trials have shown that TKI therapy is generally well tolerated by patient populations who are most often younger, healthier, and with few comorbidities; however, there are many medication-specific adverse events associated with TKIs used in the treatment of CML. Previously reported comparative safety data revealed a relatively high 1-year risk of safety events associated with TKIs: imatinib, 37%; dasatinib, 44%; and nilotinib, 40%. Higher safety risks were observed among patients receiving dasatinib (RR 1.17; 95% CI 1.06 to 1.30) and nilotinib (RR 1.07; 95% CI 0.93 to 1.23) compared with those receiving imatinib. 23 Many adverse events reported in clinical trials were also reported in the real-word setting; however, reported incidences were variable. Notably, for dasatinib, pleural effusions were reported at a higher rate in the real-world setting than in clinical trials. However, rash and diarrhea were less frequently reported across all agents, potentially demonstrating improved supportive care management of these specific adverse events in the real-world or post-marketing settings. Despite similar overall incidences of TKI-related adverse events between real-world patients with CML and clinical trial patients, TKI discontinuation rates due to adverse events were higher in real-world studies. These findings suggest either a lower threshold to discontinue or a higher severity of adverse events exist for TKI discontinuation due to intolerance in the real-world setting. Additionally, higher discontinuation rates in the real-world setting highlight an opportunity for more prompt recognition and optimized management of TKI-related adverse events.
For all TKIs, dose reductions were shown to decrease the occurrence of adverse events. 10 Real-world patients receiving nilotinib were still able to achieve major response milestones while receiving a reduced dose, with 82% of patients achieving MMR at 12 months while on reduced doses of nilotinib compared to 65% of patients on the recommended starting dose (p = 0.17). The median age of patients receiving a reduced dose of nilotinib was 12 years older than those receiving the recommended starting dose, suggesting that older patients may benefit from either empiric or reactive dose reductions. 11 The correlation of reduced doses of TKI and decreased incidence of adverse events amongst real-world studies provides encouraging data that TKI dose adjustments due to adverse events may improve tolerability and maintain TKI dose intensity without compromising efficacy.
Safety is an important consideration of CML therapy. Medication-specific toxicity profiles as well as a patient's age, comorbidities, and concomitant medications play a large role in determining the appropriate first-line TKI for each patient. 3 As the duration of TKI therapy may be indefinite for many patients with CML, minimizing adverse events and maintaining quality of life is essential. Published reviews comparing TKIs based on patient-reported health-related quality of life (HRQoL) outcomes revealed that initiation of TKI therapy improved HRQoL, but there was no observed difference in HRQoL improvements between any of the first-line TKIs.24,25 A change to second-line TKI therapy was associated with an improvement in patient HRQoL, especially in those who discontinued first-line TKI therapy due to adverse events. However, TKI treatment discontinuation altogether was not associated with any HRQoL improvements. 25 These data further emphasize the need for diligent monitoring for TKI-related adverse events, appropriate supportive care management, and individualized therapy plans for patients with CML treated with TKIs.
This narrative review has several limitations. Adherence is a critical determinant of efficacy outcomes in CML but could not be analyzed between real-world studies and landmark clinical trials. Adherence is known to be lower in real-world patient populations, but proactive monitoring and management of TKI-related adverse events may mitigate toxicity-related non-adherence. 26 The financial burden of TKIs has also been associated as a barrier to timely initiation and ongoing maintenance of therapy in CML. All studies analyzed in this review were inclusive of patients who had already overcome cost barriers to initiate therapy. Most real-world studies were performed in countries other than the US, where affordability of TKIs may differ due to government-subsidized programs. In the US, the high cost of targeted anti-cancer agents remains a major barrier to cancer care, potentially leading to suboptimal outcomes in the real-world setting.27–29 Another limitation of this review is the inclusion of only clinical studies. Claims-based and other registry studies may yield additional valuable data regarding TKI safety and effectiveness in real-world patients. Notably, the novel kinase inhibitor asciminib was FDA approved in 2021 for treatment of adult patients with CML after prior treatment with two or more TKIs and for adult patients with chronic phase CML and T315I mutation. While real-world studies investigating the efficacy and safety of asciminib are emerging, no published studies met inclusion criteria for this review based on time of publication. Lastly, follow-up intervals at which efficacy outcomes were measured varied between many real-world studies and clinical trials, limiting the ability to truly compare the incidence of disease progression associated with each TKI.
Conclusions
This comprehensive narrative literature review summarizes and describes the reported safety and efficacy of TKI therapy in real-world patients with CML as well as those treated on clinical trials. These findings suggest that patients in real-world settings achieve different rates of specific response milestones including CCyR and MMR than patients treated on clinical trials, although the impact on survival outcomes was not compared. Similar overall incidences of adverse events were reported in real-world studies as in clinical trials. However, real-world patients with CML were more likely to discontinue TKIs due to adverse events than patients enrolled in landmark clinical trials, highlighting an opportunity for more prompt recognition and optimized management of TKI-related adverse events in the real-world setting.
Footnotes
Author contributions
JC and SP contributed to research design, data analysis, and writing of the manuscript. BM contributed to research design, data analysis, and manuscript editing.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: James B. Collins, PharmD: now an employee of GSK. Benyam Muluneh, PharmD, BCOP, CPP: consultant (Servier Pharmaceuticals), spouse is an employee and stockholder of Novartis Pharmaceuticals. Sarah Profitt, PharmD, BCPS, BCOP: consultant (Genentech, Inc.), consultant (Rigel Pharmaceuticals, Inc.).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.