
Abstract
Social media, in the form of digital videos targeted to people with limited health literacy, as well as disadvantaged or marginalized groups, may help reduce cancer health disparities and improve health outcomes in these populations. In this article, we document the process of adapting the content from the Cancer 101 curriculum to create animated scripts about the cancer care continuum that is clear, straightforward, and in plain language. The development of the Cancer 101 digital videos required a multidisciplinary collaboration from—public health, medicine, technology, and expertise in correctional health, smoking cessation, web development, video producers, and individuals directly impacted by cancer disparities. The Cancer 101 videos were showcased at a community health fair where the videos were viewed by attendants waiting to be seen by a medical provider. While waiting for their cancer screening, 13 individuals were selected and invited to watch all 11 videos totaling less than 60-minutes of viewing time. They included 3 Latina women, 2 Latino men, and 8 Haitian women. All participants were between the ages of 40-65 years old. Overall, participants agreed that they would recommend the videos to friends/family (M = 4.77, SD = 0.44) and that they plan to watch other video modules to learn more information about cancer (M = 4.72, SD = 0.47). Additionally, participants enjoyed the graphics and audio of the videos presented (M = 4.85, SD = 0.38). Furthermore, participants noted that Cancer 101 digital videos described cancer in plain language, leading to a better understanding of the disease. Future research is needed to implement Cancer 101 digital videos in healthcare clinics to increase cancer information and improve cancer screening rates in marginalized communities.
Introduction
With the growing use of cyberspace 1 and the myriad of information that can be sought out, more and more people are using the Internet as a mechanism to understand further their health 2 and the health of others. 3 The PwC Health Research Institute showed a third of consumers are using social media platforms to obtain health-related information. 4 These users are more likely to engage in Facebook, Twitter, and YouTube to seek information about a disease, diagnosis, or treatment rather than engaging with health care providers. 4 The Internet can play a significant role in the way people locate health information, particularly across the cancer care continuum. 5,6 For example, one study found up to 73% of a nationally representative sample was using the Internet to gather information for a family member who had a cancer diagnosis and that 56% of the sample were cancer survivors using the Internet to locate information and resources regarding their diagnosis. 7
Another way that users are engaging other people and information on social media is by using hashtags. A hashtag is used to highlight an issue that is trending to create more visibility and engagement among the hashtag searchers. 8 Social media sites, such as Twitter, have utilized hashtags where users can filter selected topics, including types of cancers, treatment options, etc. 9 Based on these filtered topics, one study found that breast cancer patients, who were engaged in a hashtag conversation on Twitter, were 32% more likely to bring information garnered from these conversations into their treatment plan discussions. 10 This is not surprising since a substantial majority of U.S. adults report that they heavily use social media for health information. 11
Therefore, social media platforms are powerful tools that provide ad-hoc virtual spaces, enabling people to facilitate discussion, ask questions, and exchange stories that can take place anytime and anywhere with a broad audience of online users. 12 Access to content is not restricted to social media. This ease of access and use has contributed to platforms such as YouTube, which has become the most popular online video platform among U.S. adults (with over 6 billion users), 11 allowing individuals to become consumers of information and be content creators at no cost. 13 As such, the use and implementation of online digital videos in targeted communities via online platforms may be complementary to receiving information from a clinician or print materials. Thus, this shift to online platforms as a source of information emphasizes the increasing demand for creating scientifically proven and health literate communication materials from reputable sources.
A systematic review of online digital videos in cancer from 2013 to 2018 demonstrated a potential increase in behavioral change and an increase in knowledge among its users. 14 These studies indicate a need for cancer education materials for underserved populations (e.g., homeless people, people with criminal justice histories, people with mental disorders, immigrant populations), particularly those with low or limited health literacy. 14 -16 Because individuals with low health literacy have been shown to have poor health outcomes 17 using health literacy as a framework for developing digital cancer videos may improve access to health screening, health care services and reduce health disparities. 15 Health literacy is understood as having the capacity to comprehend and process necessary health information to make informed decisions about a health diagnosis or a health problem. 17,18 A nationally represented sample examining health literacy levels reported that Black and Latino adults have a higher proportion of falling the below basic literacy category when compared to White, Asian/Pacific Islander, and multiracial adults. 19 Jacobs et al 3 reported that characteristics such as being an older adult, having poor Internet skills, and being poor were associated with a lower likelihood of using social media platforms compared to their counterparts.
Thompson and colleagues reported that less than 6% of the cancer education interventions that used social media platforms included marginalize d populations. 20 Given that racial and ethnic demographics of the U.S. are rapidly changing and because of widening health disparities, 21,22 there is a need to develop digital videos that focused on people living in the margins. 15,20,23 Therefore, a team of content experts in cancer who are members of the Cancer Health Justice Lab, an interdisciplinary public health lab that addresses inequity in cancer prevention among medically underserved populations, collaborated to develop digital videos for cancer health. The interdisciplinary team included primary care physicians, public health educators, a cancer epidemiologist, a tobacco treatment specialist, and two individuals with criminal justice histories and contractors from HypnoViD, a digital production agency who provided technical support. The team’s goal was to adapt the existing content from the Cancer 101 materials 24 -27 and create digital modules about the cancer care continuum that was clear, straightforward, accurate, and written in plain language.
Methods
The tenants of health literacy to promote behavioral change 28 were used to develop the web-based short digital Cancer 101 videos to reduce cancer health disparities and increase cancer knowledge and awareness. The Cancer 101 modules were curated from the Cancer 101 curriculum developed by the Indian Health Board’s Northwest Tribal Comprehensive Cancer Project 24 for American Indians and Alaskan Natives. Cancer 101 includes 10 learning modules on the following topics: (1) cancer in the target population; (2) what is cancer?; (3) cancer risk factors; (4) the role of genes in cancer; (5) cancer screening and early detection; (6) cancer diagnosis and staging; (7) the basics of cancer treatment; (8) biospecimens and biobanking; (9) chronic conditions and cancer; and (10) support for patients and caregivers. Previous studies have demonstrated an increase in cancer knowledge after completing the Cancer 101 training session among people who were incarcerated, 26 the Puerto Rican community, 27 and the Alaskan and American Indian community. 24-25
The Cancer 101 education materials were selected as an appropriate source of materials for developing the storyboard to expand the reach and use in other vulnerable populations, including people with criminal justice histories and the medically underserved. The adapted Cancer 101 digital videos are presented in 11 modules, with a forward from the first author. The forward is a short introduction (2 minutes and 16 seconds) that explains the Cancer 101 digital videos’ etiology. New content added to the modules focused on human papillomavirus (HPV), including HPV 16 and 18, which increases cervical, penile, oral, and anal cancer risk, and a presentation on the HPV vaccine. 29 In this paper, we describe the creation of Cancer 101 digital videos (developed in 2018) that were adapted and tailored in previous studies. 26
Cancer 101 Digital Components
Based on the team’s input and using the content generated from the Cancer 101 curriculum and the lesson plans, we partnered with HypnoViD to develop and customize whiteboard animated videos. Table 1 outlines the names and scenes of the modules and the illustrations used to describe the content of each module. Video scripts were created for the 11 modules, and each video script focused on the target audience in mind. The scenarios from each of the Cancer 101 modules described the cancer care continuum [focusing on the following areas: etiology, prevention, detection, diagnosis, treatment, and survivorship]. The scripts ranged from 125-150 words of dialogue per minute, which is recommended for individuals with low or limited health literacy. The videos averaged 2 to 6 minutes in length and could be watched in its entirety in less than 60 minutes when watched concurrently. Each script underwent three rounds of revisions. Each script was reviewed for accuracy by members of the team, read aloud for clarity, and reviewed by outside viewers. Furthermore, the same voice actors were used to narrate each video, and background music was added to help with attention and motivation. The content was designed to create a story using the Cancer 101 materials. 30
Cancer 101 Digital Videos—Module Names, Scenes and Graphics.

To improve access to cancer-related information and resources, video content and scripts were written at a fifth or sixth grade (the reading level recommended for low or limited health literacy). 31,32 Additionally, the characters of the scripts were designed to represent members of the target audience to create a sense of trust and relatability with the community. Figure 1 describes one example of how the script and visuals of Module 5—Cancer Screening and Early Detection were developed.
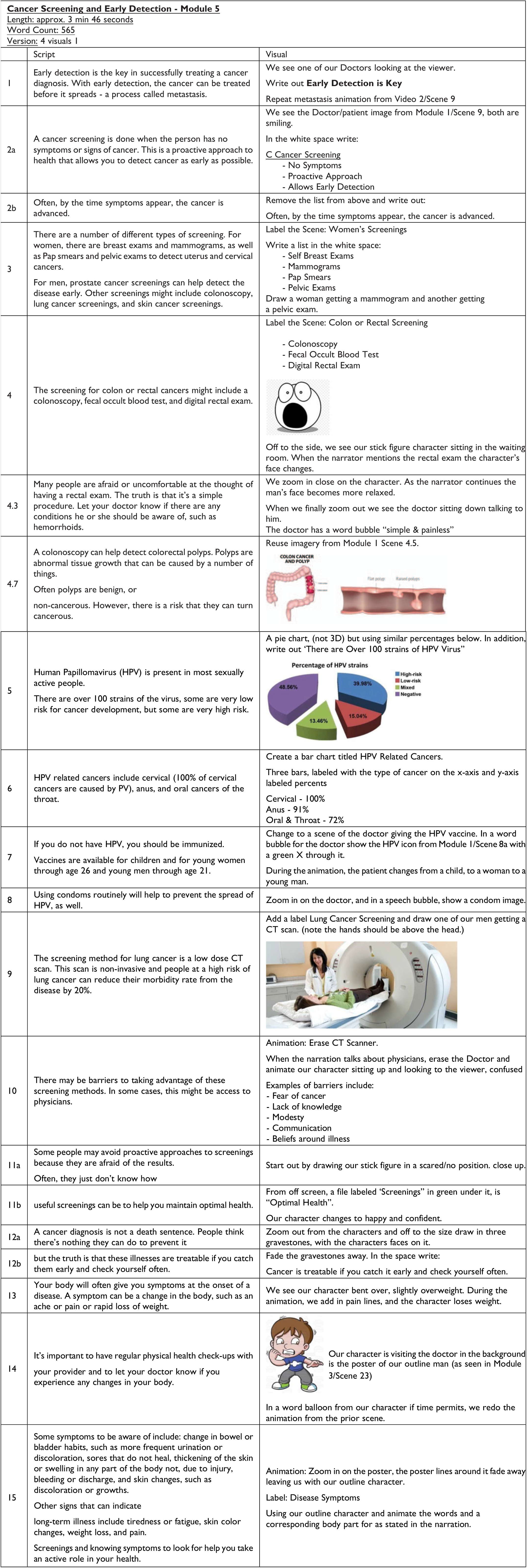
Example of script and visual development.
Once a script was approved, the script, with accompanying written visuals for each scene, was sent to an artist to create the storyboard. Using the script and written visuals as background, the HypnoViD artist then designed and created original hand-drawn artwork and illustrations for each scene. The storyboard creation required a 3-step process, a rough draft including a sequence of drawings that matched the script/voice order. The interdisciplinary team reviewed the resulting product. This allowed the interdisciplinary team to ‘see’ what images were being paired with each section of the approved script. The team provided feedback on the images, and the second version of the storyboard was created. Once approved, production proceeded with animation. The animator selected appropriate music and sound effects to highlight further and enhance the information to keep the viewer engaged. The final video with an accompanying closed captioning file was sent to the team for review.
After the team approved the final videos, captions or subtitles were added to make the digital Cancer 101 videos accessible for people with hearing loss. 33 A study conducted by Verizon and Publics Media in 2019 reported that over 92% of videos were viewed with the sound off on their mobile device, and 83% of viewers watch videos with the sound off, making video captions critical. 34 The benefits of including captioning go beyond Americans with Disabilities Act compliance 35 and accessibility. Adding captions increases flexibility that videos may be watched on multiple platforms.
In the Fall of 2019, the Cancer Health Justice Lab showcased the Cancer 101 videos at a community health fair event called, “Screen, Test, & Treat” sponsored by the Rutgers New Jersey Medical School in collaboration with the Rutgers Cancer Institute at University Hospital. 36 The whole-day event took place at the Rutgers Cancer Institute of New Jersey at University Hospital in Newark, NJ. The event provided free cervical, breast, colorectal cancer screening, and hepatitis C testing, for underinsured or uninsured Essex county residents. The event was open to anyone living in the Greater Newark area. Individuals were sent to a waiting room where they completed paperwork and remained in the area until their name was called into the examining room.
Cancer 101 digital videos were continuously projected onto a television screen in the waiting room for individuals awaiting their health screening. Thirteen participants were invited to participate to provide feedback on the videos. Members of the interdisciplinary team briefly explained the purpose of the videos. Next, viewers were asked to watch all of the videos and share their expectations and reactions with a facilitator after viewing them. After viewing the videos, participants completed a 5-minute brief satisfaction questionnaire. Participants were asked to rate each of the statements (i.e., 1. Basic understanding of cancer. 2. Would recommend videos to friends and family? 3. Materials taught in an easy way to understand. 4. Better understanding of cancer in progressing in body. 4. Enjoyed graphics and audio. 5. Would want to watch other video modules to learn more?) using a 5-point Likert scale with 1 indicating “strongly disagree,” and 5 indicating “strongly agree.” The satisfaction questionnaires were collected before participants left the waiting room for their screening.
Prototype Feedback
Thirteen residents from Essex County were asked to rate their overall experience viewing Cancer 101 videos. They included 3 Latina women, 2 Latino men, and 8 Haitian women. All participants were between the ages of 40-65 years old. The participants were recruited at the waiting room where they were completing paperwork and awaiting to receive cancer screening exams provided by medical professionals. The Cancer Health Justice Lab team members introduced the participants to the Cancer 101 videos. Overall, participants agreed that they would recommend the videos to friends/family (M = 4.77, SD = 0.44) and that they want to watch other video modules to learn more information (M = 4.72, SD = 0.47). In addition, participants enjoyed the graphics and audio of the videos presented (M = 4.85, SD = 0.38). Table 2 describes the participant’s responses to the brief satisfaction questionnaire.
Perceived Attitudes After Watching the Cancer 101 Videos (N = 13).a
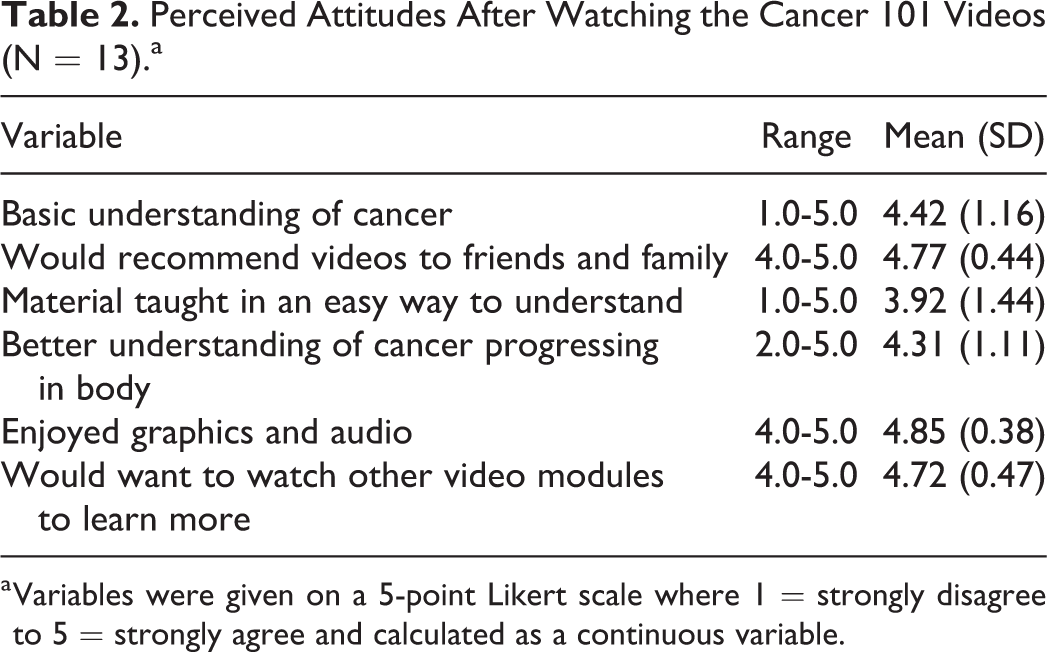
a Variables were given on a 5-point Likert scale where 1 = strongly disagree to 5 = strongly agree and calculated as a continuous variable.
Participants rated their “basic understanding of cancer” as high (M = 4.42, SD = 1.16) but rated the item, “material taught in an easy way to understand” as moderate (M = 3.92, SD = 1.44). Viewers noted that they would have preferred the videos to be available in multiple languages, such as Spanish and Creole.
Discussion
To the best of our knowledge, this is the first interdisciplinary team to adapt the Cancer 101 that was initially developed for American Indians and Alaskan Natives, 24 later tested for effectiveness in diverse populations 24 -27 and applied to a digital platform. The development of the Cancer 101 videos required collaboration from multiple sectors—public health, medicine, technology, and expertise in correctional health, smoking cessation, cancer, web development, video producers, and individuals directly impacted by cancer disparities. Complex medical issues, such as cancer, require interdisciplinary teams where members of various professions and lived experiences come together with a common goal and mission to improve health. 37
The interdisciplinary team was involved in creating the script, multiple revisions, content design such as graphics and images, and sound engineering of videos. Furthermore, the team evaluated the Cancer 101 curriculum and carefully reviewed all of the medical terms used throughout the modules. The team determined which of those would need to be simplified and easily understood by people with limited health literacy by using plain language, jargon-free communication, and succinct messaging. 38 Additionally, to keep viewers engaged with the videos and improve their satisfaction, cartoons were used to present complex information. 37 -39 Most respondents favored the images and graphics. Overall participation in viewing the videos was high, demonstrating a positive reaction to the videos. Participants noted that the Cancer 101 digital videos described cancer in basic language, leading to a better understanding of the disease. In addition, respondents enjoyed watching them and noted they would watch them again to learn more about different cancer topics.
Health literacy was used to guide the development of digital video modules. 28 The video modules emphasize increasing favorability of cancer screening by describing how early detection can lead to optimal health and timely treatment. Moreover, it was imperative to normalize cancer screening ideas by reducing user worries, such as rectal exams and finding out their results from screening. By highlighting these scenarios throughout the various modules, the goal was to increase behavioral change with increasing cancer screening and cancer prevention behaviors.
Future Research for Cancer 101 Digital Videos
The prototype feedback, coupled with previous findings from in-person delivery of Cancer 101, 26 highlight the full potential of implementing digital interventions in health fairs and health clinics. 40 Cancer 101 digital videos with closed captioning designed with marginalized populations in mind may be viewed in waiting rooms for behavioral, clinical, and medical care services, including mental health clinics, homeless shelters, federally qualified health centers, criminal court, and correctional settings, among many others to increase access to health-related information and promote individuals understanding of cancer.
Future research of Cancer 101 digital videos should include more rigorous questionnaires to examine attitudes, evidence of new knowledge using pre and post-test surveys to assess education on cancer screening modalities, and the likelihood of screening after viewing the videos. Furthermore, the studies should explore the usability of the videos and effectively engage viewers who have limited health literacy to seek cancer screening. This would include reaching marginalized populations that are sometimes overlooked in cancer research. 41,42
Limitations and Strengths
There were several limitations in the development of Cancer 101 digital videos. The limitations of this study included enrollment of a small number of viewers who provided feedback of the Cancer 101 digital videos prototype at a single event. In addition to the small sample size, viewers reported wanting the videos to be translated into multiple languages, which may have potentially limited reaching non-Native English speakers at the event. As a result, the team is currently working with HypnoViD to translate the script and captions into other languages, such as Spanish.
While there are notable barriers to developing a successful digital platform for addressing cancer disparities, 41 including limited health literacy 17 and the digital divide, 43,44 the Cancer 101 digital videos were created with these users in mind who may not have access to a laptop computer to view them. That said, the digital videos were formatted so that each of the modules could be easily streamed on any device, including a cellphone. Another strength is that the closed captioning in the videos, allows viewers to read and/or listen to them with greater flexibility.
Conclusion
Applying an interdisciplinary perspective that fosters collaboration is essential to developing a successful digital platform for addressing cancer disparities. It has been shown that digital videos can impact a broad audience related to increasing cancer education knowledge and, in turn, promote prevention activities. 15 In this study, we demonstrate how to develop online digital videos specifically for vulnerable and marginalized populations and the importance of an interdisciplinary team to create 11 modules that focused on various cancer care continuum components using plain language messaging and graphics.
Footnotes
Authors’ Note
Our study did not require ethical board approval because this project was focus on quality improvement and did not contain personal identifiers.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Rutgers Cancer Institute of New Jersey 2017 New Investigator Award (P30CA072720) and the National Institutes of Health/National Cancer Institute (K22CA197066).