
Abstract
Hepatitis B reactivation (HBVr) in cancer patients is a well-established complication due to chemotherapy-induced immunosuppression. Studies have reported HBVr associated with immunosuppressive medications, such as rituximab, methotrexate, and high dose steroids. There are different risks for different types of chemotherapy with rituximab carrying one of the highest risks for hepatitis B reactivation. Tyrosine kinase inhibitors (TKIs) are the standard of care in patients with chronic myeloid leukemia (CML). The risk of HBVr in chronic myeloid leukemia has been reported in many studies, but to this date, there are no clear guidelines or recommendations regarding screening and monitoring of HBV in CML patients receiving TKIs. We conducted this review to identify the risk of HBVr in patients with CML who are treated with tyrosine kinase inhibitors. We recommend testing for HBV status in patients who are to be treated with TKIs and to consider giving prophylaxis in those who are positive for HBsAg at baseline. More studies are needed to assess the risk of reactivation in patients with Hepatitis B core antibody positive receiving TKIs. Currently, monitoring such patients for reactivation may be the best strategy.
Introduction
Chronic Hepatitis B infection affects a large number of the world’s population. 1 The World Health Organization (WHO) in 2015 estimated that 257 million people might be chronically infected by hepatitis B, translating roughly up to 3.5% of the world’s population. 2 Hepatitis B virus (HBV) can lead to liver cirrhosis and hepatocellular carcinoma. According to the WHO, in 2015 approximately 887 thousand deaths occurred due to hepatitis B related complications. 2
The natural course of HBV follows various phases including immune tolerance, immune control, and/or immune clearance. However, immunosuppression from medications given to patients with prior HBV infection may cause reactivation of the virus. The consequences can be minor, including mild acute liver injury or asymptomatic rise in liver enzymes; or major, such as a flare of hepatic inflammation leading to fulminant liver failure and death. 3,4
Several studies have shown that cytotoxic chemotherapy and immunosuppressive medications can lead to reactivation of chronic HBV infection and such patients are at high risk of complications. 5 -7 The risk of HBV reactivation is reported to be greater than 10 percent in a systematic review of patients who received cytotoxic chemotherapy for solid organ tumors. 8 Rituximab has particularly garnered attention due to its high risk of hepatitis B reactivation in patients who are baseline only hepatitis B core antibody (HBcAb) positive. 9 -11 Other immunosuppressive agents including corticosteroids and anti-TNF agents used for autoimmune and rheumatologic conditions also increase the risk of HBVr in those patients with chronic HBV infection. 12 -16
Tyrosine kinase inhibitors (TKIs) are used in the treatment of various cancers, including chronic myeloid leukemia (CML). Imatinib was the first TKI to be introduced and was approved by the FDA in 2001 for the treatment of CML. Later, as patients developed resistance to imatinib, other agents were approved. Currently there are 5 TKIs approved by the FDA for the treatment of CML, including imatinib, dasatinib, nilotinib, bosutinib, ponatinib. 17 The WHO has placed imatinib, dasatinib and nilotinib on the WHO “Essential Medication List 2019.” 18
TKIs act by competitive ATP inhibition at the catalytic binding site of tyrosine kinases, with different forms of TKIs targeting a different spectrum of tyrosine kinases (e.g. EGFR, VEGFR, PDGFR, FLT3, etc.), resulting in modulation of growth factor signaling. 19,20 Despite potential associated side effects, TKIs are generally well tolerated and currently used widely in hematology and oncology, sometimes combined with chemo- or radiation therapy. 19,20 Examples of TKI use in cancer treatment include: 1) Imatinib in chronic myeloid leukemia (CML) and acute lymphoblastic leukemia (ALL) with the Philadelphia chromosome (Ph) or translocation t(9;22), as well as gastrointestinal stromal tumors (GIST); 2) Erlotinib in non-small cell lung cancers (NSCLC); 3) Sorafenib in renal, colon, pancreatic, lung, ovarian tumors and advanced hepatocellular carcinoma. 20
There have been multiple reports of HBVr in patients receiving TKIs. 21 -32 Due to their common use in hematology and oncology practice, there is increased interest in estimating the risk of chronic HBV reactivation associated with the tyrosine kinase inhibitors. There are several associated unanswered questions, including whether there is a need for screening all patients who will receive TKIs, how long patients with CML should be on HBV prophylaxis for and which are the best antiviral agents to use for prophylaxis of HBV patients on TKIs. To answer these questions, we conducted this review to summarize the reported cases and available studies regarding HBVr in CML patients receiving TKIs.
Methods
English language studies from the year 2000 to date related to hepatitis B reactivation in patients with chronic myeloid leukemia treated with tyrosine kinase inhibitors were searched on Medline and Google Scholar. We used different search terms including “Chronic Myeloid Leukemia,” “Chronic Myelogenous Leukemia,” “Tyrosine Kinase Inhibitors,” “Dasatinib,” “Imatinib,” “Nilotinib,” “Hepatitis B,” “Hepatitis B Reactivation” with Boolean functions to search for the relevant articles.
Our inclusion criteria were: patients who were aged 18 years or above; a confirmed diagnosis of chronic myeloid leukemia; treatment of any duration by one or more of the approved tyrosine kinase inhibitors (including imatinib, dasatinib, nilotinib, and others). Patients with any hepatitis serology marker at baseline at the time of CML diagnosis were included. We included all studies for review, including case reports, case series, and conference abstracts. Patients with chronic hepatitis B with or without hepatitis B virus e antigen (HBeAg) positivity before the start of TKI were excluded from the review. After the initial review, we found 11 publications, including case reports and conference abstracts, which were then reviewed in depth.
Results
We identified 11 studies that have reported a total of 28 cases of hepatitis B reactivation (HBVr) associated with TKI treatment. 24/28 had hepatitis B surface antigen (HBsAg) positive at baseline (before starting TKI), and 1/28 had HBsAg negative at baseline. The remaining 3/28 had reactivation with no clear baseline HBsAg results, but reactivation was determined based on increase in ALT from baseline. These results are illustrated in Table 1.
Summary of 11 Studies Investigating Hepatitis B Reactivation in Patients Receiving Tyrosine Kinase Inhibitors.
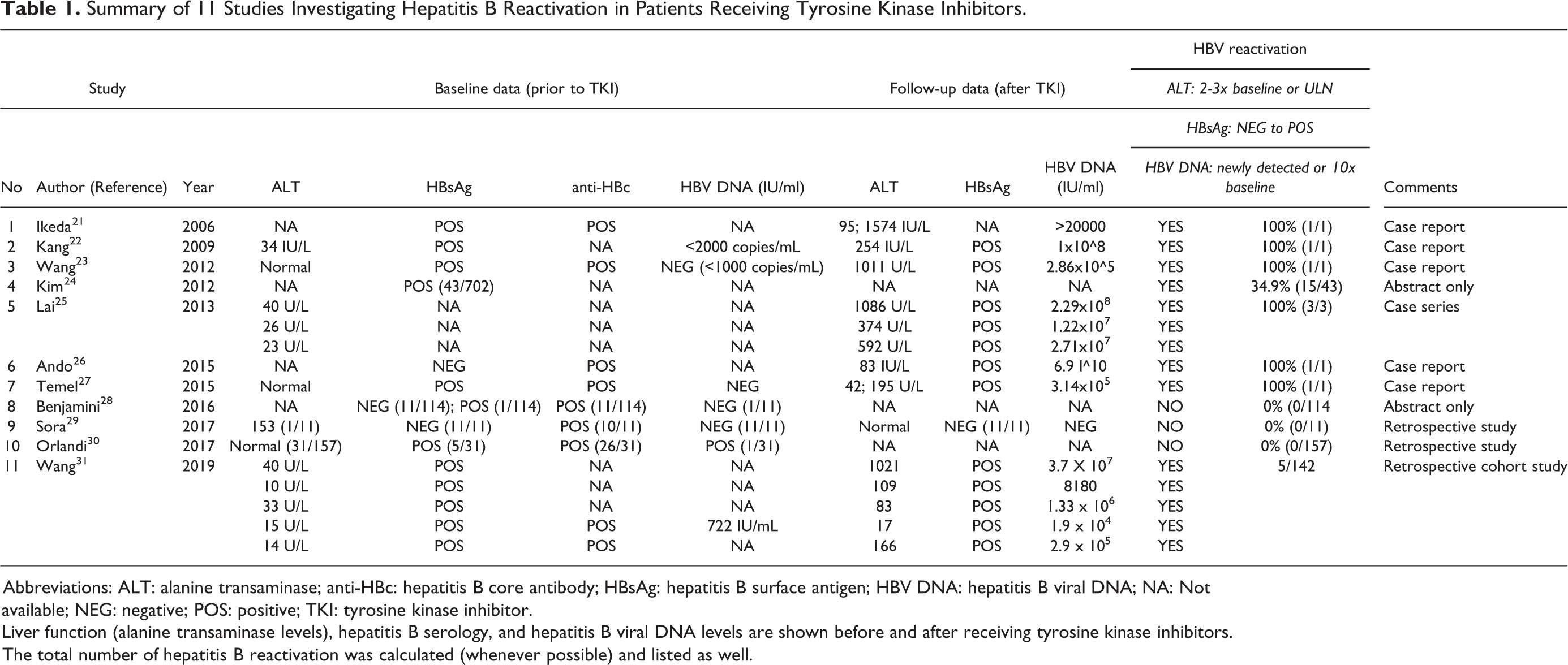
Abbreviations: ALT: alanine transaminase; anti-HBc: hepatitis B core antibody; HBsAg: hepatitis B surface antigen; HBV DNA: hepatitis B viral DNA; NA: Not available; NEG: negative; POS: positive; TKI: tyrosine kinase inhibitor.
Liver function (alanine transaminase levels), hepatitis B serology, and hepatitis B viral DNA levels are shown before and after receiving tyrosine kinase inhibitors. The total number of hepatitis B reactivation was calculated (whenever possible) and listed as well.
There are a number of limitations with regard to the studies that were reviewed. Five of the studies were case reports involving one patient each. 21 -23,26,27 One case series by Lai et al. (2013) involved 3 patients. 25 Although these case reports and series aided in the recognition of the problem and potential outcomes, they lack any statistical power due to their sample size. Three American Society of Hematology (ASH) abstracts were reviewed in this article. 24,28 These studies had larger sample sizes, but only reported limited data that were required to ascertain HBVr in the patients. Some lacked baseline parameters, while others lacked follow up values. In these 3 studies, we were unable to confirm HBVr in accordance with the definition described earlier. Three studies were retrospective in design, 29 -31 and determined the proportion of HBVr in a sample of CML patients on TKI treatment. These managed to investigate HBVr over a longer duration, as the investigators went retrospectively in time. Nevertheless, the number of HBVr cases collected was limited to 5 patients in all 3 studies combined. A further limitation of the retrospective studies is the potential lack of full data, as shown in the study by Orlandi et al., 2017 where follow up values after the commencement of TKIs were not available. This also prevented us from confirming HBVr based on the definition stated previously. 30 None of the studies were randomized, and none had a control or comparison group except study by Wang et al. (2019). 31 This poses a significant limitation to the level of evidence provided. The limited number of studies on HBVr in CML patients receiving TKIs may be due to the low incidence of such events or under-reporting.
In addition, there seems to be an over-representation of studies based in East Asia (China, Taiwan, Japan, Korea). This may be due to the higher incidence of HBV in that population, but it raises the concern of the applicability of the results to patients in the rest of the world. We also excluded non-English language reports from our search criteria and may have missed articles with extra data that were reported, for example, in Chinese.
Discussion
The reported incidence of Hepatitis B reactivation in patients who were HbsAg positive was 10.8 per 100 person-years in the retrospective cohort study where all but one patient did not receive primary prophylaxis. 31
The definition of Hepatitis B reactivation is variable in the literature. 4 Hepatitis B reactivation (HBVr) is usually defined by changes in alanine transaminase (ALT) levels, HBV serological markers, or HBV DNA. Hepatitis B reactivation can be considered in the following 3 situations; a 2- to 3-fold increase of ALT above baseline; hepatitis B surface antigen (HBsAg) seroconversion or detection of HBV DNA in the blood in the absence of HbsAg; newly detected HBV DNA or a ≥10-fold rise in HBV DNA level (compared with the baseline level before immunosuppression). 29,30,33 -36 It is noted that HBV reactivation doesn’t only occur in HBsAg-positive cases but can also occur in HBsAg-negative cases with positive anti-hepatitis B core antibody (HBcAb) and/or anti-hepatitis B surface antibody (HBsAb) positive. 25,35 -38 Patients with occult HBV infection (OBI) who have detectable HBV DNA but HBsAg is negative can also have reactivation of hepatitis B. HBVr in patients with OBI is defined as either seroconversion of HBsAg or an increase of at least 10-fold above the lower limit of detectable HBsAg and HBV DNA if they were previously undetectable. For patients with OBI who had detectable HBV DNA, a 1 log increase above the baseline would also regard as HBVr. 39
According to the American Gastroenterology Guidelines, the risk of HBVr in patients with hematological malignancy receiving chemotherapy is reported to be high (>10%) in patients receiving rituximab, with a recommendation to start prophylaxis treatment for such patients even if they have only HBcAb positive (HbsAg negative). The risk in patients receiving TNF, a moderate to high dose of steroids for 4 weeks, and patients receiving TKIs (e.g. imatinib, nilotinib, and dasatinib) is reported to be moderate (1-10%), with a recommendation for prophylaxis against HBV, but the strength of this recommendation is weak. 29,33
The pathogenesis of HBVr secondary to TKIs is unclear. Probable mechanisms of chemotherapy-induced HBVr are thought to involve 2 stages, the immunosuppression stage and the immune-restoration stage. 25 In the immunosuppression stage, there is a noticeable rise in serum levels of HBV DNA and hepatitis B e-antigen (HBeAg), probably due to suppression of the immune mechanism that helps to control HBV replication. In the immune-restoration stage, after the withdrawal of the immunosuppressive agents, rapid destruction of infected hepatocytes occurs. 25
Studies have shown that imatinib can inhibit T-cell activation and proliferation. 25,40,41 Imatinib can also affect other immune cells in that it prevents the differentiation of progenitor stem cells to antigen presenting cells and inhibits macrophage function. 12,41,42 Nilotinib can inhibit the Src family kinase Lck and T-cell function, and can suppress CD8+ T lymphocytes proliferation and function. 25,43,44
Imatinib and other tyrosine kinase inhibitors are also associated with hepatotoxicity as a side effect. 17 Physicians may face diagnostic challenges in a patient who is a chronic HBV carrier and is receiving TKIs. Differentiating HBVr from hepatotoxicity may not be easy. There has been a reported case in which a patient with CML who was a carrier of hepatitis B developed severe hepatotoxicity and liver failure, resulted in a fatal outcome. 45 A liver biopsy of the patient showed negative immunostaining for hepatitis B markers leading to the conclusion that it was not HBVr but rather drug toxicity that caused the mortality. Other authors have also reported biopsy proven significant hepatotoxicity due to imatinib. 46 -49 The exact mechanism of hepatotoxicity is unknown. Mitochondrial dysfunction and inhibition of glycolysis are possible mechanisms. 50
Based on the data we have gathered, it is advisable to screen all patients who are planned for TKI treatment. Suitable screening tests include ALT, complete hepatitis B serology panel (including HBsAg, anti-HBs antibody, anti-HBc antibody, HBeAg, anti-HBe antibody), and HBV DNA. It is important to identify patients with possible previous HBV infection, as evidenced by hepatitis B serological markers, i.e. positive HBcAb, with negative HBsAg, with or without detectable HBsAb. Patients with only total HBcAb positive most likely have resolved HBV infection. However, other possibilities include false positive results, resolving acute infection or low level chronic infection. 51 These patients are also at risk of reactivation. In our opinion it is unacceptable to start treatment with TKIs in CML patients without assessment of HBsAg. Nevertheless, running all tests may not be feasible due to the costs and availability of testing equipment. Therefore, if unavailable, testing patients using only ALT and HBsAg, or even ALT alone would suffice initially. 52
For HBsAg positive patients, prophylaxis against HBVr should be started as HBVr may happen any time after the commencement of TKIs. The duration of prophylaxis was mentioned only in the study by Wang et al. and was variable from 1 to 60 months. It is worth noting that the time to reactivation has a large range in the available studies, from 1 month to 69 months after starting TKI. However, the median time to reactivation is 9-10 months after TKI commencement. 5 -8,11 -13,15
Based on currently available evidence, we recommend HBV prophylaxis for patients with positive HBsAg receiving TKIs and that prophylaxis be given from the start of TKI treatment and continued for at least 2 years after the commencement of TKIs, if feasible (as the median time to reactivation is 9-10 months). The duration of prophylaxis is not well established, and our recommendation is based on the limited data available. If this is not feasible, it is advisable to monitor markers of reactivation, as mentioned above (i.e. ALT, HBsAg, HBV DNA, whichever is available). For those with possible resolved HBV infection (i.e. positive HBcAb and negative HBsAg), we recommend monitoring for signs of HBVr during the treatment duration without prophylaxis. A reasonable schedule would be to start monitoring at time zero, then at 1, 3, 6, and 12 months in the first year of treatment.
In addition to the limitations with regards to the studies, as mentioned in the “Results” section, a few other limitations in this review can be attributed to the lack of available data. Firstly, it is unclear how long monitoring and prophylaxis should be given. This issue is clinically important as CML patients receive lifelong treatment with TKIs. There are no available studies investigating the most cost-effective strategy of HBV prophylaxis. Secondly, there is no clear answer in the literature as to which antiviral should be used, and there are no studies specifically comparing the efficacy of different antiviral agents for HBVr prophylaxis in CML patients receiving TKIs. In guidelines for HBV prophylaxis for hematologic malignancies, entecavir and tenofovir are the recommended agents with entecavir having the highest quality of evidence for its use. 53
Conclusion
There is a considerable risk of hepatitis B reactivation in HBsAg positive patients with chronic myeloid leukemia treated with tyrosine kinase inhibitors. We suggest that all patients with CML should have baseline values of ALT, complete hepatitis B serology panel as well as HBV DNA if serology is positive before starting TKI treatment, and should be followed up with repeat values of these 3 parameters as required. However, if cost and availability limit the use of these tests, we strongly suggest following up with ALT and HBsAg levels before and after treatment with TKIs. In patients with a risk of HBVr (i.e. positive HBsAg on screening, as well as those with persistent HBcAb), prophylaxis with agents with high resistance barriers such as entecavir or tenofovir can reduce the incidence of reactivation.
Details remain unclear for the most effective antiviral agent, the duration and frequency of monitoring, as well as the duration of prophylaxis. In addition, the cost-effectiveness of differing approaches remains unknown as the prophylactic treatments are expensive and not universally available. Further studies are required to provide appropriate evidence to support such recommendations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.