
Abstract
Aims:
Postoperative Atrial fibrillation (POAF) after esophagectomy may prolong stay in intensive care and increase risk of perioperative complications. A minimally invasive approach is becoming the preferred option for esophagectomy, yet its implications for POAF risk remains unclear. The association between POAF and minimally invasive esophagectomy (MIE) was examined in this study.
Methods:
We used a dataset of 575 patients who underwent esophagectomy. Multivariate logistic regression analysis was performed to examine the association between MIE and POAF. A cox proportional hazards model was applied to assess the long-term mortality (MIE vs open esophagectomy, OE).
Results:
Of the 575 patients with esophageal cancer, 62 developed POAF. MIE was negatively associated with the occurrence of POAF (Odds ratio: 0.163, 95%CI: 0.033-0.801). No significant difference was observed in long-term mortality (Odds ratio: 2.144, 95%CI: 0.963-4.775).
Conclusions:
MIE may reduced the incidence of POAF without compromising the survival of patients with esophageal cancer. Moreover, the specific mechanism of MIE providing this possible advantage needs to be determined by larger prospective cohort studies with specific biomarker information from laboratory tests.
Keywords
Introduction
Previous studies have shown that patients who undergo esophagectomy have a higher risk of post-esophagectomy atrial fibrillation (POAF) compared with patients who undergo other surgical procedures. 1,2 POAF generally develops within 3 days after an esophagectomy. A meta-analysis found that patients with POAF had higher perioperative mortality, longer hospital stays, and a greater incidence of complications. 3 Risk factors, demographic data 4 and medical history 5 were all shown to play a role in the development of POAF.
Thoracoscopic/laparotomy-assisted esophagectomy (MIE) has become the preferred approach in order to speed recovery and enhance the patient’s quality of life. 6 -8 However, little attention has been paid to the effects of MIE on POAF. In the present study, a dataset of patients who underwent esophagectomy was analyzed to evaluate the impact of MIE on POAF. A further comparison of long-term mortality was compared between MIE and hybrid cases (OE).
Materials and Methods
Study Population
A dataset of patients with esophageal cancer from an online database (https://figshare.com/articles/Association_between_Postoperatively_Developed_Atrial_Fibrillation_and_Long-Term_Mortality_after_Esophagectomy_in_Esophageal_Cancer_Patients_An_Observational_Study/3306883) was analyzed. A total of 575 patients with esophageal cancer were enrolled in the study from January 2005 to April 2012. POAF was defined as the incidence of newly developed POAF that required treatment. MIE was defined as thoracoscopic/laparotomy-assisted esophagectomy (hybrid cases were included as OE). The database of figshare.com grants a secondary analysis on its’ dataset. In addition, the license of CCBY 4.0 of the original paper indicates that copying and redistributing the material in any medium or format is unrestricted. Since the analysis was based on a dataset of a published study that contained no personal identification, no ethical approval was required.
Preprocessing of Variables
The primary outcome was set as POAF, and the secondary outcome was long-term mortality. Long-term mortality was defined as the mortality rate within 5 years after the surgery. Previous studies suggested that demographic factors, 9 complications, 10 and medications 11 were associated with the incidence of POAF. Therefore, the following factors were included as independent variables for outcomes of POAF: 1. Demographics (including age, sex, and body mass index (BMI)); 2. Preoperative assessment of cardiac function (including heart rate (HR), and left ventricular ejection fraction (LVEF)); 3. Comorbidities and medications (including diabetes mellitus (DM), hypertension (HTN), chemo-radiation therapy (CRT), β-blockers, and diuretics); 4. Cancer and procedures (including anesthesia time, crystalloids, colloids, pathologic stage of cancer, and surgical procedures); 5. Complications (including pneumonia, anastomotic leaks, sepsis, and AKIN classification). Postoperative pneumonia was defined as pneumonia occurring within 7 days post-surgery, as indicated by an increase in opacity in chest radiography in addition to at least 2 of the following findings: an increase in temperature above 38°C, an increase in white blood cell count above 10,000/ µL or a decrease to less than 3000/µl, and the presence of purulent sputum. 9 Sepsis was defined as an increase in the sequential organ failure assessment (SOFA) score ≥ 2 points caused by a dysregulated host response to infection. 10 Independent variables for the outcome of long-term mortality included age, sex, Body Mess Index (BMI), HR, LVEF, DM, HTN, CRT, β-blockers, diuretics, pathologic stage of cancer, surgical procedures, pneumonia, anastomotic leak, sepsis, and AKIN classification. The continuous variable BMI was translated into a categorical variable (i.e., low weight for BMI <18.5, normal weight for BMI ≥ 18.5 and <25, overweight and obese for BMI ≥ 25). The continuous variables age, HR, LVEF, anesthesia time, crystalloids, and colloids were categorized into quartiles.
Statistical Analysis
Descriptive statistics were used to summarize the baseline characteristics of all variables. Categorical variables were presented as frequency of occurrence, while continuous variables were presented as means ± standard deviation. A student’s t-test was used to compare continuous variables, and a chi-square test was applied to categorical variables. Multivariate logistic regression was used to simulate the models for the primary outcome. The secondary outcome of long-term mortality was assessed using the Cox Proportional Hazards model. Sensitivity analysis was conducted by building models with and without variable of complications. All analyses were conducted using Stata (version 15; StataCorp, USA). A value of p < 0.05 was considered significant.
Results
Esophagectomy was performed on 575 patients, of which 62 (10.8%) developed new-onset POAF (Table 1). Sinus rhythm was restored by electrical cardioversion or amiodarone administration.
Univariate Analysis Between OE and MIE.

Abbreviations: OE = Open Esophagectomy; MIE = Minimally Invasive Esophagectomy; BMI = Body Mass Index; DM = Diabetes Mellitus; HTN = Hypertension; HR = Heart Rate; LVEF = Left Ventricular Ejection Fraction; CCRT = Chemo-Radiation Therapy; AKIN = Acute Kidney Injury Network.
Variables were demonstrated in frequency (percentage).
Demographics
Compared with patients who underwent OE, those who underwent MIE were relatively older (age > 68 years: 33.3% in MIE versus 22.0% in OE, p = 0.072). In patients who underwent OE, 93.7% were male (n = 477). The percentage of males was similar to patients who underwent MIE (n = 63, 95.5%, p = 0.786). No statistical difference was found in BMI between the 2 groups (χ2 = 3.476, p = 0.173).
Perioperative Medications
The use of perioperative β-blockers and diuretics was not significantly different between patients who underwent OE or MIE (5.9% versus 9.1%, p = 0.313 for β-blockers, and 8.1% versus 9.1%, p = 0.773 for diuretics). CRT was performed in 44.6% of patients (n = 227) who underwent OE and 10.6% of patients (n = 7) who underwent MIE (p < 0.001).
Characteristics of Cancer and Procedures
In the OE group, 82.7% of patients had early esophageal cancer (20.6% in T0 and 62.1% in Stage 0, I, and II), and 95.5% of patients who underwent MIE were in various stages (9.1% in T0 and 86.4% in Stage 0, I, and II) (p < 0.001). The majority of surgical procedures performed on patients differed between the 2 groups (79.2% of patients in the OE group had the Ivor Lewis procedure, whereas 92.4% of patients in the MIE group had the Mckeown procedure). Increased volumes of crystalloids were used in patients who underwent OE (>1400 mL: 49.9% in OE versus 30.3% in MIE, p = 0.015).
Complications and Follow Up
The morbidity of patients with anastomotic leak who underwent MIE was higher than that of patients in the OE group (12.1%, n = 8 in the MIE group versus 4.9%, n = 25 in the OE group, p = 0.018). Similar morbidity between the 2 groups was observed for the incidence of pneumonia, sepsis, and AKIN classification. On average, long-term mortality was over 20% (24.0% in the OE group versus 21.2% in the MIE group, p = 0.620).
Multivariate Analysis
For the primary outcome, logistic regression was performed. MIE was negatively associated with the incidence of POAF (OR = 0.163, 95% CI 0.033-0.801, p = 0.026) (Table 2). In the Cox model, no statistically significant associations between long-term mortality and MIE were found (HR = 2.144, 95% CI 0.963-4.775, p = 0.062) (Table 3). Sensitivity analysis indicated same results (effect of MIE on POAF: OR=0.162, 95% CI 0.033-0.793, p = 0.025; effect of MIE on long-term mortality: HR = 1.940, 95% CI 0.963-4.775, p = 0.102) (Supplemental Table 1&2).
Mulvariate Analysis of Risk Factors Associated With Postoperative Atrial Fibrillation.

Abbreviations: POAF = postoperative atrial fibrillation; OR = Odds Ratio; CI = Confidence Interval; BMI = Body Mass Index; DM = Diabetes Mellitus; HTN = Hypertension; HR = Heart Rate; LVEF = Left Ventricular Ejection Fraction; CCRT = Chemo-Radiation Therapy; AKIN = Acute Kidney Injury Network.
1 Referent is Open Esophagectomy; 2 Referent is Age ≤57 (years); 3 Referent is Male; 4 Referent is Low weight (Level 1); 5 Referent is ≤66 (beat per minute); 6 Referent is ≤59%; 7 Referent is T0; 8 Referent is Ivor Lewis; 9 Referent is ≤365 (minutes); 10 Referent is ≤1000(ml); 11 Referent is ≤900 (ml); 12 Referent is No AKI.
Cox Model With Outcome of Long-Term Mortality.
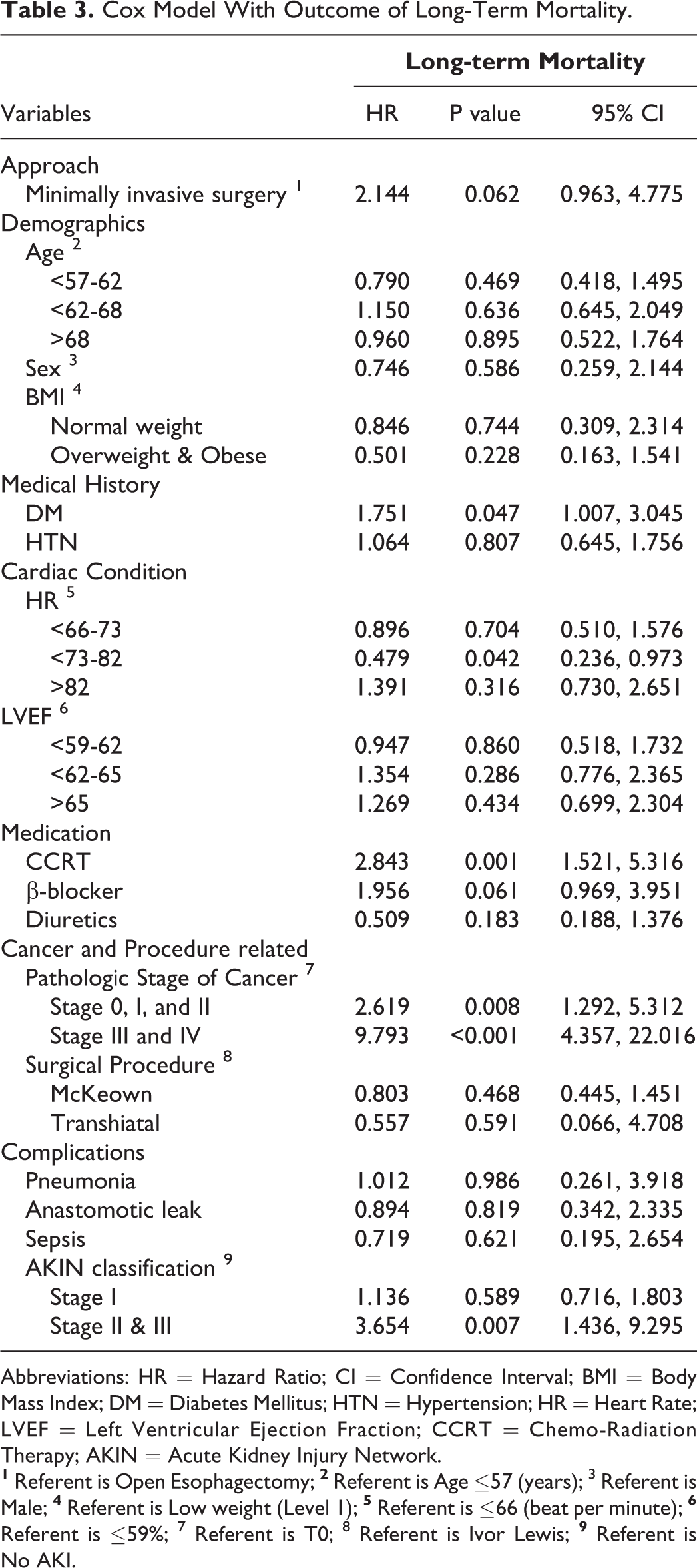
Abbreviations: HR = Hazard Ratio; CI = Confidence Interval; BMI = Body Mass Index; DM = Diabetes Mellitus; HTN = Hypertension; HR = Heart Rate; LVEF = Left Ventricular Ejection Fraction; CCRT = Chemo-Radiation Therapy; AKIN = Acute Kidney Injury Network.
Discussion
Compared with the many studies that examined the atrial fibrillation that developed after cardiac and pulmonary surgery, studies that focused on post-esophagectomy atrial fibrillation were relatively limited. 3,11,12 In these studies, complications of infections (anastomotic leakage and sepsis) were consistently associated with new-onset atrial fibrillation. 3,12 However, a few studies have been conducted to assess the effects of MIE, which plays a major role in reducing infectious complications 13,14 with no significant impact on anastomotic leakage. 15 -17 In the present study, we assessed the link between MIE and the incidence of atrial fibrillation after esophagectomy. The identified negative association pointed to the possible cardiovascular benefit of a minimally invasive approach.
A previous study demonstrated that patients who underwent MIE had a lower inflammatory response as demonstrated by an analysis of cyto- and chemokines. This indicated that minimally invasive techniques attenuate the inflammatory response compared to open surgery. 18 Lower C-reactive protein levels and white cell blood counts were associated with minimally invasive esophagectomy, suggesting an improved state of systemic inflammatory and catabolic responses to surgical trauma. 19 The trauma and associated inflammatory reactions play a major role in the pathogenesis of POAF. 20 -22 By minimizing the operative trauma and inflammatory status, MIE could theoretically reduce POAF. In the present study, the odds of developing atrial fibrillation after MIE were reduced (0.163, 95% CI 0.033-0.801) compared to OE. In contrast to our results, 2 previous studies did not find significant differences in POAF risk between MIE and OE. 23,24 The incidence rate of new-onset atrial fibrillation after esophagectomy varies greatly (12%–37% of patients). 25 Study population and analysis methods could be the potential reasons for the different findings. Day et al. compared the POAF rate in their MIE cohort with a prior reported incidence of POAF in OE cases, 23 where the groups for comparison were not from the same study population. In addition, both studies compared only the crude frequency of POAF in the MIE and OE groups. This is consistent with our findings that the crude frequency of POAF was not associated with the type of surgery. However, after adjusting for confounders, there was a significantly lower odds of POAF risk in the MIE group than in the OE group in our study.
Considering the possible advantage of decreasing POAF through MIE, the future of new robot-assisted minimally invasive esophagectomy is promising. Efforts should be made to carry out further studies examining the development of advanced robot-assisted minimally invasive esophagectomy for the purpose of minimizing trauma and inflammation. Although infection-related complications such as pneumonia and sepsis were included in the multivariate regression model, they were not statistically significant (p = 0.813 for pneumonia and p = 0.162 for sepsis). In addition to the MIE procedure, another potential method to reduce POAF risk is the use of prophylactic antiarrhythmic medication. A previous study showed that prophylactic intravenous amiodarone is associated with a lower incidence of atrial fibrillation following esophagectomy. 26
Similar survival rates between OE and MIE have been reported in patients with esophageal cancer. 27,28 However, most studies have focused on the immediate postoperative outcomes and short-term prognosis. 16,17,29,30 In the present study, a comparison of the prognosis was performed with a 5-year mortality outcome. The Cox proportional hazards model revealed comparable odds of survival in patients who underwent MIE. However, these patterns were not statistically significant (p = 0.062).
This study has several limitations. The limited sample size could have led to insignificant results of tests that might yield significant results with a larger dataset. Another limitation was the lack of particulars in the assessment of patients. For example, without the details of blood pressure and blood glucose association between DM, HTN, and the outcomes may have been compromised. Important information regarding complications was not abstracted from this dataset. More severe complications related to covariates (including pleural effusions, conduit necrosis, etc.) and infective sources of sepsis were unavailable from the original dataset, which may potentially influence POAF rates in the multivariate regression analysis. Sensitivity analysis was conducted by building models with and without variable of complications, resulting in same conclusion that MIE was associated with POAF but not long-term survival. For future studies, information regarding inflammatory factor indices, invasive cardiac hemodynamic monitoring, and most severe complications will be helpful for testing the biomedical mechanism of the association between MIE and POAF.
Conclusion
Given the negative impact of POAF, MIE may be a superior option for reducing POAF without compromising the long-term survival of patients with esophageal cancer. Moreover, the specific mechanism of how MIE could provide this possible advantage requires determination by larger prospective cohort studies with specific biomarker information from patient laboratory tests.
Database of figshare.com grants a secondary analysis on its’ dataset. In addition, the license of CCBY 4.0 of the original paper indicates that copying and redistributing the material in any medium or format is free. Since the analysis was based on a dataset of a published study that contained no personal identification, no ethical approval was required.
Supplemental Material
Supplemental Material, supplemental_tables - Impact of Minimally Invasive Esophagectomy in Post-Operative Atrial Fibrillation and Long-Term Mortality in Patients Among Esophageal Cancer
Supplemental Material, supplemental_tables for Impact of Minimally Invasive Esophagectomy in Post-Operative Atrial Fibrillation and Long-Term Mortality in Patients Among Esophageal Cancer by LaiTe Chen, BinBin Li, ChenYang Jiang and GuoSheng Fu in Cancer Control
Footnotes
Acknowledgments
We would like to thank Ji-Hyun Chin, Young-Jin Moon et al in the Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea to provide the dataset.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.