
Abstract
Despite rapid and successful development in pediatric cancer treatment, many ethical challenges remain. These challenges have been, and continue to be, the subject of much research, but few qualitative studies have explored the views of nurses, especially in the Middle East. This study, therefore, seeks to fill a knowledge gap in this area and to better understand the concerns of nurses—particularly those in Saudi Arabia and the Middle East. Face-to-face, in-depth interviews were conducted with 17 male and female nurses working in pediatric units at 2 hospitals in Saudi Arabia to explore their views on the ethical challenges in caring for children with cancer. All interviews were recorded and transcribed, then line-by-line encoded, merged, and categorized into themes. Our results show that pediatric cancer is perceived as being “different” from other diseases, and from cancer in adults. Nurses are an integral part of the medical care team and are aware of the importance of their role, as well as the special relationships that they develop with the children. Consent is mandatory and necessary and can be signed by any parent. Assent is important when children become able to give it. Pediatric cancer is seen as a different disease by nurses for various reasons. Their roles and relationships with children and families pose many challenges. Though parental consent and child assent are essential, nurses’ collaboration is important for shared decision-making. Our study paves the way for broader studies to understand the concerns of nurses and other health-care providers about treating children with pediatric cancer.
Introduction
In recent decades, 2 very important issues have had a profound effect on nurses and their feelings about children with cancer. Firstly, despite rapid advances in cancer treatment, caring for children with cancer remains extended and exhausting. It has a variety of physical and psychological effects on the patient, their family, the child’s school, and caring staff, including nurses. Secondly, perceptions of the legal, moral, and ethical status of children are changing in terms of dignity and autonomy.
Previous studies have attempted to explore the challenges and emotions faced by pediatric cancer nurses, often called “Angels of Mercy,” as they care for childhood patients with cancer for many months or years. Some, like Wiener et al, 1 Nassin et al, 2 Pye, 3 and Al-Gamal and Long, 4 have used quantitative research methods to target the attitudes of nurses. In 2018, a systematic review of qualitative studies of informed consent in pediatric cancer showed that only 1 of 13 studies interviewed nurses, most targeted parents. 5 The results reflect a lack of nurses both in conducting research and as research participants in qualitative studies of pediatric cancer ethics (Table 1).
Qualitative Literature Targeting Nurses’ Views Regarding Informed Consent in Pediatric Cancer.

Abbreviation: IRB, institutional review board.
In a study of health professionals’ experiences of various ethical challenges, Bartholdson et al 13 asked 87 health professionals open-ended questions. Of these participants, 11 were registered nurses and 9 were nurse aides working in pediatric cancer care. The researchers concluded that caring for children with cancer gives rise to strong feelings and challenges of the conscience. They also raised ethical questions about the effects of differing and conflicting visions between specialists and parents, and the possibility of sharing these visions to combine ethical approaches. 13
Other studies highlighted other issues, such as Eilertsen et al, 19 which involved more than 1 neonatal nurse, using the focus-group research method. This study sought to demonstrate the importance of collaboration and communication between specialists. Kathy Ruccione interviewed the “living legend” Jean Fergusson, reviewing her long experience as a pediatric oncology nurse and the challenges she faced. 20
Despite the fact that many medical centers in Saudi Arabia and the wider Arab region provide treatment for pediatric patients with cancer, there is a paucity of qualitative research on the ethical challenges faced by nurses involved in the care of children with cancer. Therefore, we conducted in-depth interviews with several nurses working in Saudi Arabia to explore their views on childhood cancer care and the ethical issues involved. Data generated from these interviews may form the basis for subsequent research.
Materials and Methods
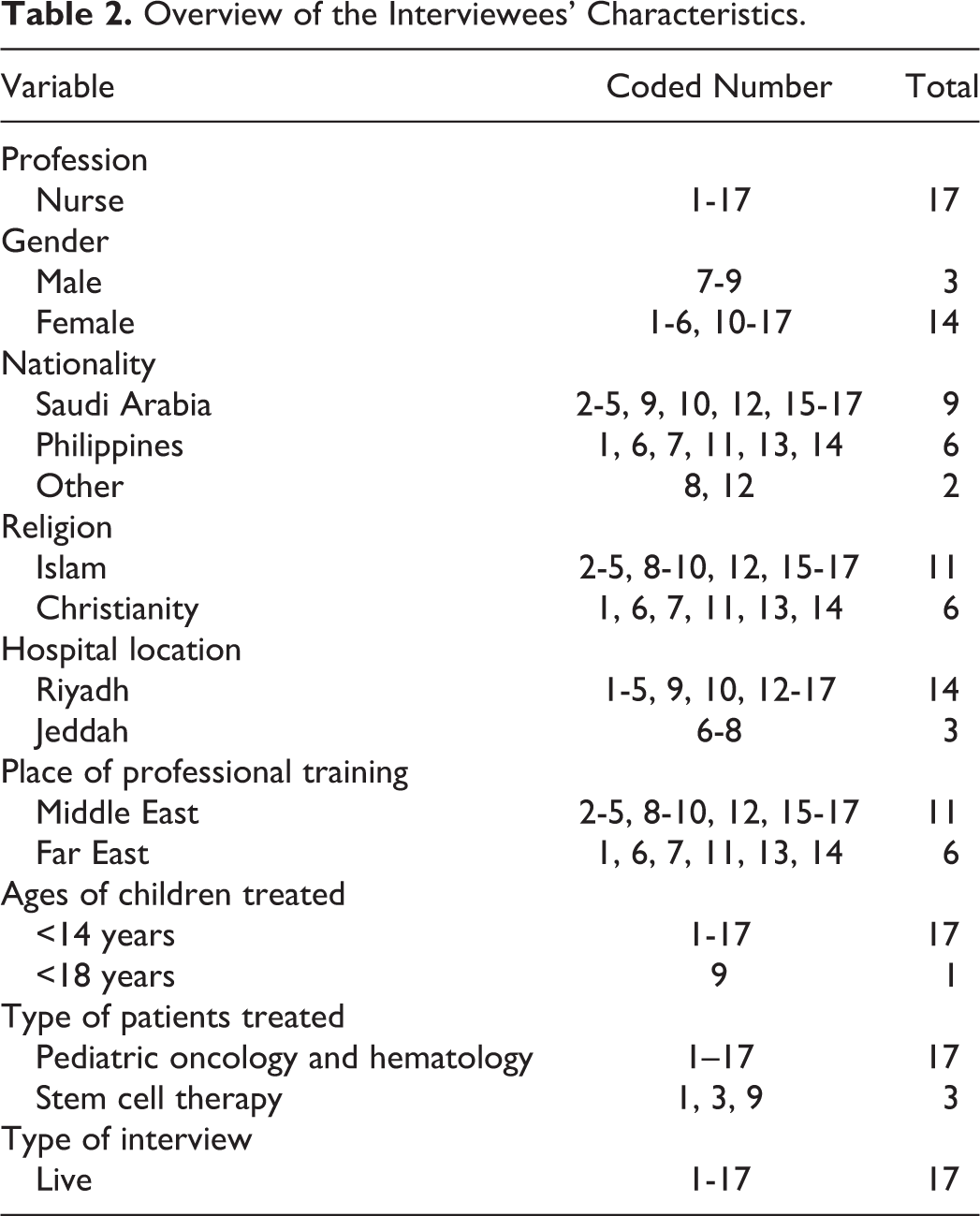
The selection of interviewees was guided by the purpose of the study, so they were nurses with good experience and knowledge of pediatric cancer. Interview participants were selected using the “snowball” technique 21 until we reached a satisfactory point of saturation, when the data related to themes became repetitive and no new relative information could be generated. 22 Participants were 17 nurses (14 females and 3 males) employed at branches of King Abdul Aziz Medical City in Riyadh and Jeddah. These 2 cities were selected because of the presence of specialized units to treat children with cancer. Moreover, included nurses were of Saudi, non-Saudi, and non-Arab nationality/ethnicity, as shown in Table 2.
Overview of the Interviewees’ Characteristics.
A well-trained research coordinator, who was not part of the research team, approached research participants by visiting pediatric departments treating children with cancer, and interview appointments were made after obtaining informed consent. Face-to-face interviews were conducted in English, for between 45 and 60 minutes. Semi-structured, open-ended questions were used to allow participants to express their views freely and to be able to include important findings. 23 Since all the nurses were able to speak fluent English, English was the only language used in all the interviews to avoid any language biases.
Research questions were developed by the authors, building on a previously published paper and a review of related literature, as explained in the introduction. A variety of interview questions were used and included questions about the interviewee’s profiles, experience, and history with dealing with pediatric cancer, and information about the department or center. This was followed by a number of questions about ethical challenges related to pediatric cancer treatment, which included questions about the differences between it, and other diseases and adult cancers, as well as questions about collecting informed consent, type and degree of involvement of children in decision-making, the family role, and how important it is to be aware of and respect the family concerns and values. Additionally, questions were asked about the other duties of nurses who take care of children with cancer.
All interviews were recorded and then transcribed without making any changes or corrections. Then, the interview texts were manually encoded, line-by-line, and participants’ answers to the questions were merged and categorized into themes, based on the interview questions and relevant literature. The themes were modified and, finally, shaped to display all major ideas. Finally, the codes were validated by a second, independent relistening to the recordings.
Ethical approval was obtained from the institutional review board institutional review board at King Abdullah International Medical Research Center (KAIMRC). In quotations from participants’ statements, nurses are referred to as “nurse,” rather than by name, for the sake of confidentiality. Other personal characteristics (see Table 2) are only referred to if necessary for context.
Results
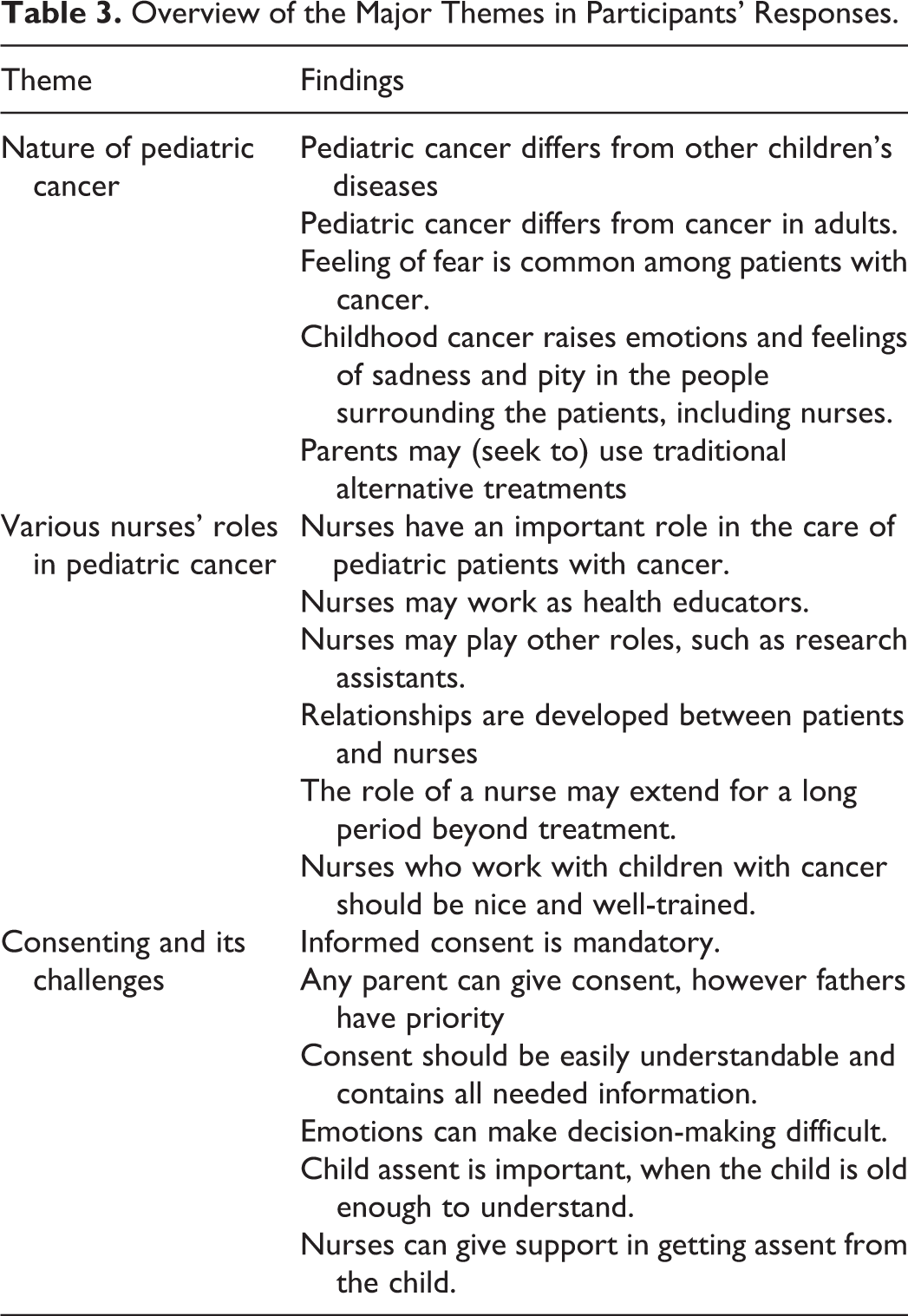
Through previously explained methods, our results could be classified into 3 main themes that reflect the views of interviewed nurses. The first theme was about the nature of pediatric cancer and its differences from other pediatric diseases, and from adult cancers. The second theme concentrated on the role of nurses and the factors affecting these roles and what characteristics these nurses should have. The third theme was about parental consent and child assent, and what are consenting challenges (See Table 3).
Overview of the Major Themes in Participants’ Responses.
First Theme: Nature of Pediatric Cancer
Our results showed that many of the participants agreed that cancer is perceived as being “different” from other diseases, regardless of its type, diagnosis, treatment, or dimensions. One nurse said: “Cancer differs from other diseases, by nature, ways, and duration of treatment,” while another said, “Treatment is a long-term process, affecting everyone, including children themselves.” However, one nurse expressed the view that cancer in children is not different from other serious diseases in children: “In case life-threatening diseases, I do not see any difference with cancer, as both need more careful care.”
When comparing childhood cancer with cancer in adults, most nurses believe that the main difference is the children’s inability to understand the nature of the disease, and their inability to express their feelings and properly make decisions. One nurse said, “Children do not know what cancer is and why they come every day, while adults know that and can be educated.” Another said, “Children are unable to express their complaints.” On the other hand, one nurse expressed the opinion that adults with cancer are more psychologically affected by it and, thus, require more support.
No non-Saudi nurses reported any differences in perceptions of the challenges of pediatric cancer between their home country and Saudi Arabia, apart from financial challenges. One Filipino nurse, who worked in both Saudi Arabia and the Philippines, said: “Compared with the situation in Philippines, I do not see any difference, unless when it comes to survival rate because of financial support which is bigger here.”
Our results confirm the perception that, according to their nurses, patients with cancer experience a mixture of feelings of fear, hope, and frustration, as exemplified by a comment from one nurse, who said: “Feeling of fear is common among cancer patients.” Moreover, childhood cancer also raises emotions and feelings of sadness and pity in the people surrounding the patients, including nurses. One nurse said, “It is full of emotions,” while another described, “It is heartbreaking to see a child with a cancer at a very young age, with a long process of treatment.” Nurses see that childhood cancer affects not just the child, but their whole family. For example, “We see the reaction of family and I think their acceptance of disease is a most important challenge.”
Nurses see how the parents—who are, at first, shocked to learn that their child has cancer, and then by the prospect of a long phase of treatment—start to look for alternative treatments, some of which may pose risks. One nurse said, “Some alternative traditional methods used by patients and their families are acceptable, such as reading verses of holy book, but when it comes to certain practices, such as using cautery, then we should give them clear recommendations not to use them, especially when they contradict treatment protocols.”
Second Theme: Nurses’ Roles in Pediatric Cancer
Nurses are an integral part of the medical care team. Nurses are aware of the importance of the role assigned to them, as exemplified by 1 nurse who said, “Nurses have important role in care of pediatric cancer.”
Nurses start to provide care from the moment of diagnosis, through treatment, and even for many years afterward. One nurse said, “We are following up all kinds of patients, including post-marrow transplantations, chemotherapy, blood transfusion, and others.”
Patients with cancer are among the longest-term patients, and, along with their relatives, nurses are in the closest contact with them. A special relationship develops between the nurse and the child. One Saudi nurse described the feeling when a young man called her by name, and she realized he was a former patient, “I was so happy because I saw the fruit of my work.”
According to our interviewees, the role of the nurses extends beyond the care of patients, to help in educating patients and in medical research. One nurse said, “As a nurse, I play the role of witness in collecting informed consent process.” Because of their proximity to patients, they can also play an educational role. One interviewee said, “All staff working in caring of patients with cancer should have a duty to educate patients on how to deal with their diseases.”
Nurses participating in our study agreed that a nurse should be patient, courteous, well informed, and well-trained in this field. One nurse said, “Nurses who work with children of cancer should be nicer and should have training on how to deal gently with children and their families.”
Third Theme: Decision-Making and Consenting in Pediatric Cancer
Making decisions in the care and treatment of children with cancer is not always easy. Frequently, decisions are made through discussion and collaboration between the treatment team, parents, and the child himself.
In regard to parental consent, the nurses interviewed in our study considered parental consent mandatory and necessary from the moment the child is admitted to the hospital, as well as during the course of diagnosis and treatment. One nurse said, “We need consent in each stage of treatments plan.”
Most nurses agreed that “Both women and men have the right to sign the consent,” but most of these nurses viewed the father as having priority. For example, “Any parent can sign the consent, and the father is the one who sign if he is available.” However, the nurses reported that disagreement between the parents was rare, and social workers were used to resolve any problems. One nurse said, “It happened, but it was rare, a mother came after medication taken after a father consenting asking why you gave it, I refuse that. Such kind of problem should be solved through social workers.”
This consent should easily understandable and contain all the required information for an informed decision. One nurse said, “It is important to the family to know if the treatment is curative or palliative, because this may help them in preparing themselves.”
Nurses reported that parents’ emotional and psychological states sometimes made it difficult to obtain consent from them. One nurse said, “The main problem is that the parents are usually being emotional, under strong feelings and maybe not completely able to make proper decisions.” In light of this, some nurses considered the process of collecting consent sometimes to be insufficient, as exemplified by the comment, “I do not think our practice in getting consent is adequate—we need to help them in taking decision. I always see it as shared decision and a shared responsibility between parents and healthcare providers.”
When it comes to child assent, nurses agreed that children with cancer are often weak and require care, so the child’s own decisions cannot be relied upon. A nurse said, “Children are not who take decisions,” At the same time, while it was noted that it is important for children to participate in decision-making, one nurse said it depends on their age, “From age of 12 years, we have to seek permission from child besides of parental consent.” However, another nurse expressed that the child’s understanding of their illness, the procedure, and the treatment provided was more important than age, “When the child can understand, he should be involved in consenting process.” That said, it was stressed that any information given should be provided in a simplified way, and—if possible—used as an opportunity to teach the child, “The child can understand, and the nurse can educate him about his disease.”
Discussion
Nature of Cancer
Three main ideas have shaped nurses’ views about pediatric cancer: children’s vulnerability, differences from other childhood diseases, as well from adults’ diseases. Children weakness gives rise to many emotions and feelings. It is not surprising that the nurses in our study described moments of sadness when faced with a child with cancer.
Pediatric cancer causes feelings of sorrow and pain not just for the child but also for the whole family. This explains why breaking the news to the child’s family is an important step. 24
It is not surprising, then, that after their child’s diagnosis, parents often reprogram their lives to adjust to the new situation and often begin to look for solutions—both inside or outside hospitals. Nurses may not be happy with pursuit of alternative therapies, 25 so they feel a moral duty, which goes beyond the scope of their job, to warn against practices that may pose a danger or harm. As has been noted by other researchers, 26 reading verses from the Qur’an and the supplication of du’aa (prayers) are widely accepted in Saudi Arabia. It is not surprising to find that some nurses in our study reported that they had encouraged parents to do that, along with following treatment protocols, especially when they see a beneficial psychological effect that helps parents to accept their child’s disease.
Childhood cancer is the same, here or there, as is the human vulnerability of the child and their parents. In cases of childhood illness, differences are eliminated and, nurses have the same attitudes toward children in different countries. This is a reflection of the moral principles of equality and justice that must be exercised by all who care for the sick.
Despite advances in cancer treatment, we found that nurses view cancer as being different from other childhood diseases. That said, stereotypes associated with cancer are difficult to eliminate from people’s minds—even from the minds of nurses, who are arguably more aware of developments in treatment and diagnosis, and with a direct contact with sick children and their families. Perhaps the causes of and the distinction between diseases relate to therapeutic methods other than those used in the treatment of other diseases.
The nurses interviewed in our study also viewed childhood cancer as being different from cancer in adults, reporting the perception that adults are better able to understand their illness and can make independent decisions. Although this difference is not limited to cancer, it is unique here because of the nature of the disease. Furthermore, lack of adequate knowledge about cancer may even be a positive thing—adults with cancer might be more susceptible to its psychological effects, thus requiring greater care and support to overcome the ordeal.
Nurses’ Roles and Duties in Caring for Children With Cancer
The main role of the nurse is to take care of patients, and this is arguably most important in pediatric cancer when around the clock care is needed from the moment of hospital admission to the moment of discharge. Although nurses do not develop treatment plans, they are required to implement them, step by step, monitoring patients, and responding to questions from patients and their parents. Nurses follow-up with children after they take strong medications that may affect the whole body, making them feel exhausted, weak, vulnerable, and helpless. Other authors have also noted this, including Al-Gamal and Long, 4 who investigated the significant impact that pediatric cancer has on quality of life.
The development of special, memorable, and long-lasting relationships between health-care providers, especially nurses, and patients and their families is a result of love, compassion, kindness, and sympathy. Nurses must have the emotional and social skills to be able to deal professionally with patients and their families. This indicates a need for robust training programs 27 to ensure that future nurses possess these qualities, with a moral basis in the rules and laws governing professional ethics, and the customs and ethos of people and their religions and laws. 28
Although nurses are not usually required to educate patients, they sometimes, give advice. Because of the good relationships with patients, and families, such advice is often trusted, and will lead to shared decision-making. 3 As reported by one of the nurses in our study, the fact that nurses are in regular contact with, and are trusted by, patients and their parents means that nurses also play other roles, such as being the doctor’s and researcher’s “right arm.”
Parental Consent
In caring for children with cancer, it is accepted and expected to obtain parental consent, whether in terms of hospital admissions, surgery, analysis, investigations, or remedial actions. Obtaining parental consent for such cases is in line with the ethical principles of general clinical practice, local 29 and international ethical norms, 30 and Islamic fatwas. 31
Since children are unable to make their own decisions, parents must play this important role to protect their child’s interests and avoid harm as far as possible. 32 It is well established that nurses who care for children view the receipt of parental consent as essential.
Furthermore, nurses in our study noted the importance of providing adequate information to parents, enabling them to make a free and fully informed decision about consent. This is considered to be a milestone in ethical clinical practice, including in pediatric oncology. 33 This finding implies that nurses know that obtaining informed consent is a reflection of the principle of respect for autonomy. 34 At the same time, some nurses highlighted some practical challenges in obtaining informed consent, in particular, that the process is suboptimal and done too quickly. This may be due to nurses’ heavy workload and responsibilities. It may also be because parents are perceived to have confidence in their doctor’s decision-making capabilities while, at the same time being under great emotional stress. Perhaps nurses sense that parents are disinterested in reading the consent copy, or that they are too emotionally weak to make decisions with full awareness and will. 35 In turn, this may require the medical team to provide sufficient professional psychological support to help parents make appropriate decisions.
Obtaining consent from the child’s father, as mentioned by the interviewees, reflects a cultural difference, that has been reported in other Middle Eastern 36 and Saudi 37 research. However, an increase in mothers’ input in decisions making is noticed, which indicates a shift that has been observed in recent years, although decision-making is still largely a male domain. Furthermore, the priority given to fathers is supported by the procedural policies of the institution in which the research was carried out, that is, that consent may be obtained from family members in the following order: father, mother, grandfather, elder brother, and so on. The influence of the opinions of scholars of Islamic law and traditions explains why nurses try to obtain consent from children’s fathers. 31
Child Assent
There is broad acceptance that children do not have the capacity or qualifications to make fully informed decisions about their medical care, thus any child’s health decision must be made by the child’s parents and not by the child. 38 The complex nature of cancer treatment, and the toll that it takes not only on the child’s body but on the child’s family, as well, makes this issue even more pertinent since it stands in the way of children’s ability to understand their disease and its treatment. Nevertheless, this does not mean that children should not participate in decision-making, an idea which is supported by other studies. 39
Several factors can make it difficult to accept a child’s assent, such as their inability to fully comprehend or to make decisions, but if this ability is present—regardless that the final decision should remain in the parent’s or guardian’s hands—children must be consulted. Despite differences in capacities between children, the generally accepted minimum age at which a child’s consent can be accepted is 12 years old. Some researchers believe that every child should be evaluated on a case by case basis, 40 and others agree that child consent can be used instead of assent when the child is 12 years old or older. 41
It is important to discuss a child’s treatment with them before obtaining their assent. Such discussions should provide information in a simple and educational way, and nurses can play a key role in this education, for both children and their families. 42
Conclusion
There is little information about nurses’ views of the ethical challenges in pediatric oncology in Saudi Arabia. Pediatric cancer is seen as a different disease by nurses, for various reasons, and it has familial, social, and psychological reflections. Exploring other groups’ views, such as family’s members and physicians, will help in having a complete picture.
Nurses’ roles in providing care for children with cancer poses challenges other than those related to the quality and success of treatment. These challenges must be taken into account more broadly for better clinical and ethical practice.
It is also necessary to provide satisfactory training on how to properly and correctly collect consent, with the options available, taking into account the emotional state of the parents. The present study paves the way for broader research in the Arab region to explore nurses’ views on other relevant issues, such as refusing treatment and research on children.
Supplemental Material
Supplemental Material, Interview_guide_-_Nurses-_Pediatric_cancer_care_(1) - Ethical Challenges of Pediatric Cancer Care: Interviews With Nurses in Saudi Arabia
Supplemental Material, Interview_guide_-_Nurses-_Pediatric_cancer_care_(1) for Ethical Challenges of Pediatric Cancer Care: Interviews With Nurses in Saudi Arabia by Ghiath Alahmad, Halah Al-Kamli and Haneen Alzahrani in Cancer Control
Footnotes
Authors’ Note
This research is ethically approved by the IRB at King Abdullah International Medical Research Center (KAIMRC), under the IRBC/027/17.
Acknowledgments
The authors sincerely wish to thank all of the nurses agreed to be interviewed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Sanad Children’s Cancer Support Association, Saudi Arabia.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.