
Abstract
Prostate cancer (PCa) is the most frequent tumor among Latin American (LATAM) men. The incidence of de novo metastatic PCa is higher in LATAM than other parts of the world, and demographic changes in the region have increased disease burden. However, region-specific information regarding prevalence, progression, and treatment effectiveness is not currently available for nonmetastatic, castration-resistant PCa (nmCRPC). Nonmetastatic, castration-resistant PCa is a heterogeneous disease with varying potential to develop metastasis with limited treatments available, until recently. New clinical trials with promising results have allowed second-generation antiandrogen drugs to be used as first-line treatments, rendering guidelines outdated. As a result, this panel of experts reviewed the current status and challenges and developed recommendations for nmCRPC diagnosis and management in LATAM. The Americas Health Foundation (AHF) conducted a literature review and identified LATAM scientists and clinicians who have published in the field of PCa since 2012. The AHF convened a panel of 7 chosen experts urologists and medical oncologists from the region. The AHF developed specific questions relating to nmCRPC, which were answered by the experts prior to the multiday meeting. Each narrative was discussed and edited by the panel, through numerous rounds of discussion until a consensus was reached in a final manuscript. The panel proposes specific and realistic recommendations for improving access to diagnosis and management of PCa in LATAM. No treatment has yet shown improvement in overall survival; however, when including metastasis-free survival as an end point, second-generation antiandrogen drugs have emerged as effective treatment options and are currently included as first-line treatment. Although nmCRPC is a specific disease that represents a small percentage of patients with PCa, effective diagnostic and treatment strategies can contribute toward increasing quality of life and survival rates of patients with PCa in LATAM.
Introduction
Latin America (LATAM) is generally considered a group of 21 countries that covers an area that stretches from the northern border of Mexico to the southern tip of South America, including the Caribbean, whose inhabitants speak a Roman language. 1 The region comprises almost 8.5% of the world’s population. 2,3 During the last few decades, LATAM has experienced an increase in life expectancy and subsequent aging of the population. This shift inevitably results in an increasing incidence of cancer, including prostate cancer (PCa). 4 Despite recent health-care improvements, cancer mortality rates in LATAM are twice that of developed countries. 5
Materials and Methods
To address the above issues, The Americas Health Foundation (AHF) used PubMed and Embase to conduct a literature review and identify LATAM clinicians and scientists with an academic or hospital affiliation who are experts in the field and who have published in the PCa arena since 2012. As a result of this effort, AHF convened a panel of 7 experts from LATAM, representing the specialties of urology and oncology. Great attention was paid to ensure a diverse group representing various aspects related to PCa.
To better focus the discussion, AHF staff independently developed specific questions, addressing the salient issues on the subject, for the panel to address. A written response to each question was initially drafted by a different member of the panel. During the multiday meeting, several rounds of discussion were made to obtain consensus.
Search Strategy and Selection Criteria
Manuscripts referenced in this recommendation paper were identified through searches of PubMed and Embase with the search terms “non-metastatic prostate cancer,” “nmCRPC,” “prostate cancer Latin America,” and “prostate oncology Latin America” from January 2012 until April 2019. Articles were also identified through the bibliographies of the papers identified in the search as well as from sources of the authors’ own files. Particular attention was paid to papers that reviewed or summarized the topic in question or that were related to activities in LATAM. The final reference list was generated based on the relevance to the broad scope of this consensus document.
Epidemiology and Burden of PCa in LATAM
Prostate cancer is a highly prevalent disease among men. Worldwide, GLOBOCAN estimates nearly 1.3 million new cases of PCa and 360 000 PCa-related deaths in 2018. In LATAM, PCa is the third most frequent tumor (after lung and breast), and the most frequent among men, reaching the highest mortality rate among all cancers. It is projected that in 2018, PCa will be responsible for approximately 152 000 new cases and 51 000 deaths in the region. 6 The highest PCa incidence and mortality rates in the world are seen in 2 countries in LATAM: Guadeloupe and Barbados. 2
Despite GLOBOCAN projections, epidemiological information by country in LATAM remains scarce. As of 2011, only 21% of countries in the region had a population-based cancer registry, although some improvements are underway. In Brazil, according to the local National Cancer Institute (INCA), about 68 000 new patients PCa were expected to be diagnosed in 2018 7 , corresponding to an incidence rate of 66.1 new cases per 100 000 men, making it the most frequent tumor excluding nonmelanoma skin cancers. 1 In Argentina, PCa is also the most frequent cancer in men, with an incidence of 44 cases per 100 000 men in 2017. 8 In Colombia, PCa is the third most lethal cancer in men, after stomach and lung cancer, though no precise information about incidence has been reported. 9 In Peru, the mortality rate of PCa is 15.6 per 100 000 men, with higher rates occurring along the coast in contrast with the highlands and the jungle. 10,11 Mexico presents one of the lowest PCa incidences in LATAM, with 27.3 cases per 100 000 men and a mortality rate of 11.3 deaths per 100 000 men in the last 3 decades. 12 The incidence and mortality rates of PCa are still on the rise in most countries in LATAM such as Brazil, Ecuador, Colombia, and Costa Rica. 4 This is a result of changing risk factors, increased longevity in the population, and limited access to effective local or systemic treatment. 13
Although most individuals living in LATAM have basic health coverage, large disparities remain among different countries and health systems, resulting in variable and inequitable outcomes. Only a few countries in LATAM have universal health care. 5 In addition, there is a large discrepancy between public and private health-care systems. In some countries within the region, direct negotiations with payers have benefited from recommendations made by medical societies. As a result, in Brazil, the population with private health care has observed the same rate of early diagnosis as developed countries. 14
Life expectancy in LATAM is estimated to reach 80.7 years for women and 74.9 years for men between 2025 and 2030, 15 which raises concerns about quality of life and diseases with increased prevalence in the elderly population, including PCa. Health-care policies should be designed to tend to the needs of the aging population. Furthermore, tailored cancer programs establishing policies for prevention, early diagnosis, when indicated, and effective treatment with access to care are crucial to ensuring quality of life.
There is no published data describing the impact of early diagnosis of PCa on mortality, health-care costs, or quality of life in LATAM. The vast majority of countries in the region do not have official PCa screening programs. 16 -23 Although a number of programs have been developed and implemented to detect PCa in the region, the majority of these initiatives are isolated campaigns and programs promoted by specific groups, being not necessarily governmental policies. 24 -39
Given the lack of organized screening, the incidence of de novo metastatic PCa in LATAM is higher than in other parts of the world, evidencing the need for such policies in order to improve the rate of diagnosis and treatment of localized disease. Although some cases of metastatic disease could be prevented by screening policies, the benefits of detecting early disease should be balanced against overdiagnosis and overtreatment.
Nonmetastatic Castration-Resistant PCa
A systematic review demonstrated that around 10% to 20% of patients with PCa will develop castration-resistant prostate cancer (CRPC) within 5 years of follow-up. When high risk factors such as a rapid PSA doubling time (DT; PSA DT <10 months) are present in patients with no evidence of metastasis at diagnosis of CRPC, it is expected that 33% of these patients could develop metastatic disease within the next 2 years 40 and 60% in the next 5 years, impacting directly quality of life. 41 Today these men are considered to have nonmetastatic, castration-resistant PCa (nmCRPC). 40
Nonmetastatic, castration-resistant PCa is defined as a rising PSA that is at least 1 ng/mL, castrate testosterone levels (<50 ng/mL), and no radiographic evidence of metastatic disease by conventional imaging methods (eg, computed tomography [CT] and bone scan). 42 Currently, nmCRPC is estimated to affect around 100 000 men in the United States, with an annual incidence between 50 000 and 60 000, 43 though epidemiology about nmCRPC outside the United States is lacking. The proportion of patients with nmCRPC compared to those diagnosed with distant metastasis is currently unknown, in part because in some cases metastasis may be present but not promptly detected due to the strong dependence on the sensitivity and specificity of the diagnostic tools used. 44 With the introduction of more sensitive imaging modalities, such as prostate-specific membrane antigen (PSMA) and positron emission tomography (PET) scan, the nmCRPC landscape is expected to evolve, allowing metastatic disease to be detected earlier, 45 reducing the number of patients with nmCRPC and increasing the number of patients with “low burden” metastatic disease. This new stage of the disease (metastases only diagnosed by PSMApet) will certainly result in a new stratification of PCa stages with corresponding new terminology and treatment approach.
Data on nmCRPC in LATAM from a 2013 study presented at the American Society of Clinical Oncology showed a patient flow model that was developed to estimate the 5-year limited duration prevalence of nmCRPC in 28 countries, including Brazil and Mexico. It was estimated that nmCRPC represents a relatively small proportion (2%-8%) of the PCa population. 46
Diagnosis and Risk Stratification of nmCRPC
The natural history of PCa goes through different stages. When a patient is not cured by treatment of localized disease, the next stage is biochemical recurrence that is evidenced by a rise in PSA without any signs of metastasis detected by conventional imaging methods. For patients with local recurrence, salvage radiotherapy (SRT) is the standard of care and the only option that can kill PCa cells left behind after radical prostatectomy or at least postpone the use of androgen deprivation therapy (ADT) in many cases. Nevertheless, biochemical progression does occur after SRT, which probably results from microscopic local, regional or distant disease.
There is some controversy on how and when to start ADT in patients with biochemical recurrence after treatment of the primary tumor without evidence of metastatic disease. The debate on immediate versus delayed initiation of ADT is inconclusive, despite data suggesting early use is better. In 2017, the majority of the panel in the Advanced Prostate Cancer Consensus Conference pointed that multiple parameters, including projected life expectancy, PSA value and kinetics, and comorbidities have to be taking in account to starting ADT. 47 Men with PSA recurrence are a heterogeneous group with a frequently good prognosis that does not require immediate treatment. 48 Despite these recommendations, some physicians begin ADT at any PSA rise because both patients and physicians are reluctant to leave the PSA recurrence untreated. Since ADT is not curative in this scenario, it is inevitable that all patients at some point will develop nmCRPC. Nonmetastatic, castration-resistant PCa can also be a result of inappropriate treatment of patients with locally advanced disease who do not receive treatment of the primary tumor but instead are treated only with ADT. Physicians should be aware that this approach is not considered the standard of care. 49,50
In practice, when not indicated, early initiation of ADT could expose patients to possible and unnecessary side effects without altering the risk of death from PCa. 51 -54 Moreover, unlike metastatic CRPC (mCRPC) where the main goal is improving overall survival (OS), treatments for nmCRPC have the additional aims of seeking to delay both the initiation of subsequent treatments and the appearance of metastasis, thereby preserving quality of life. Stratifying PCa recurrence by PSA kinetics remains the most important predictor of these end points, 48,55 as PSA DT is a strong predictor for developing metastasis. 56,57
There are no specific guidelines on follow-up imaging for patients with nmCRPC. As such, clinical practice will vary based on the availability of imaging technology. In the absence of high-quality evidence, the RADAR III Group’s 2018 recommendations suggest that follow-up imaging should be conducted every 6 to 12 months, or more frequently, based on a PSA DT of less than 6 months and/or symptoms in patients undergoing therapy for nmCRPC. 47,58 Additionally, when conventional imaging methods fail to detect metastasis, new imaging methods can be used and therapy should not be ceased for PSA rise alone. 59
Newer techniques such as 11C-choline PET/CT, 68Ga-labeled PSMA, and whole-body magnetic resonance imaging (MRI) can detect metastatic lesions earlier than conventional imaging methods. As a result, increased use of PET/CT and PSMA would likely result in stage migration as smaller metastasis are able to be diagnosed earlier. Two meta-analyses demonstrated increased sensitivity and specificity for PSMA in finding metastatic lesions in patients being staged before treatment of the primary tumor and after biochemical recurrence. 60,61 However, data on the sensitivity and specificity of PSMA in nmCRPC are insufficient, and the biological significance of shifting from nmCRPC to mCRPC with minimal disease burden remains unclear. Thus, the risks of overtreatment should be taken into consideration when using these newer techniques. Currently, there is no strong evidence to indicate that treating oligometastatic disease, outside of the pelvis, focally has a positive impact on survival or of the type of patient that will benefit the most from this therapeutic approach.
Treatment Practice for nmCRPC
Recently, 3 studies with second-generation antiandrogen drugs (apalutamide, enzalutamide, and darolutamide) were published. These results dramatically changed the landscape for patients with nmCRPC. In 2018, apalutamide and enzalutamide received Food and Drug Administration (FDA) approval based on the results of the 2 prospective randomized trials, SPARTAN 62 and PROSPER. 63 In 2019, the results of the ARAMIS trial with darolutamide were also published 64 (Table 1).
Inclusion Criteria, Randomization, and End Points (SPARTAN, PROSPER, AND ARAMIS).
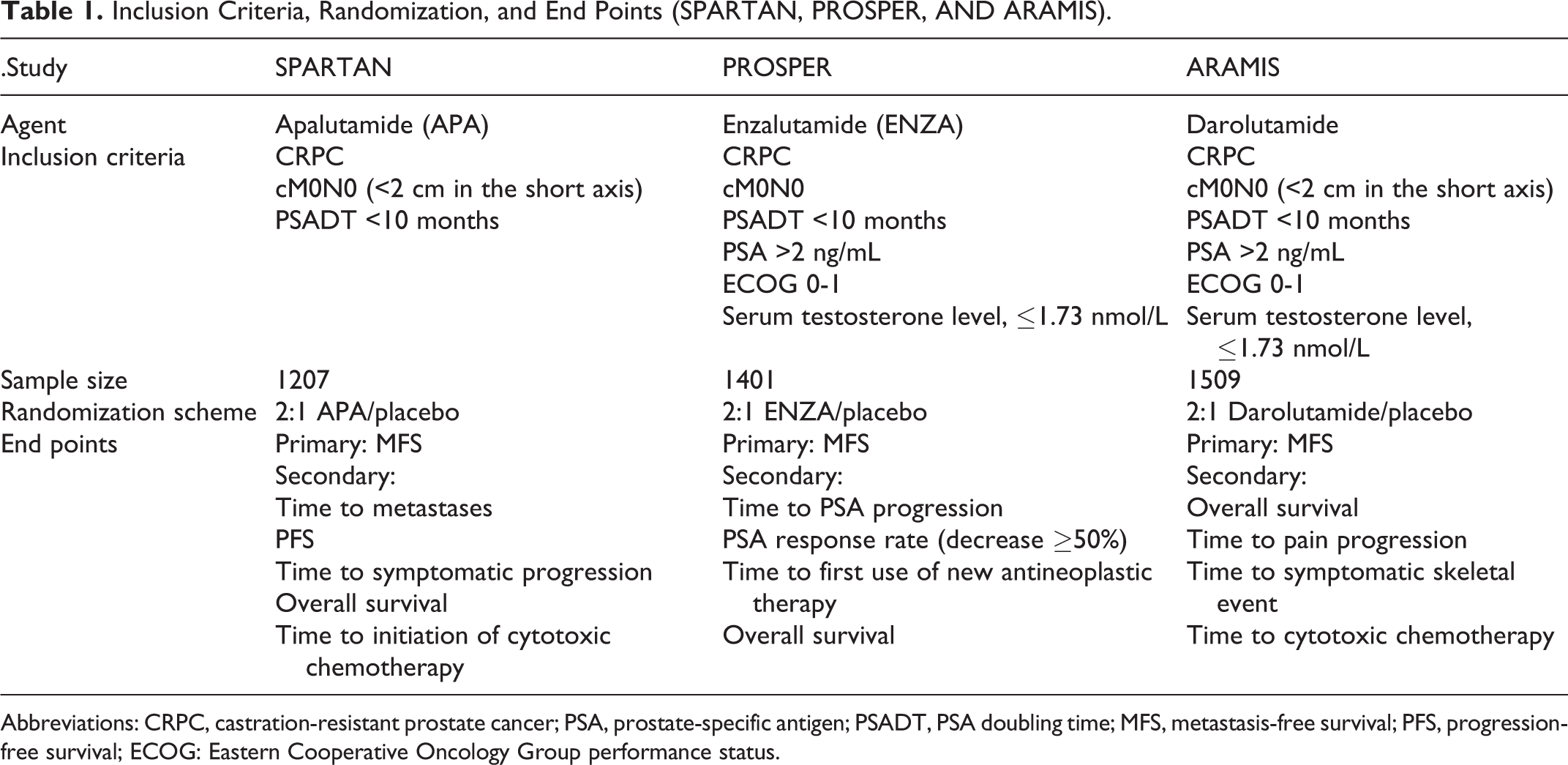
Abbreviations: CRPC, castration-resistant prostate cancer; PSA, prostate-specific antigen; PSADT, PSA doubling time; MFS, metastasis-free survival; PFS, progression-free survival; ECOG: Eastern Cooperative Oncology Group performance status.
For approval of new drugs, traditionally, OS was the unique primary end point considered by the FDA. The hypothesis that metastasis-free survival (MFS) could be a surrogate for OS in PCa was tested by Intermediate Clinical Endpoints in Cancer of the Prostate (ICECaP) working group in patients with hormone-sensitive localized PCa. The ICECaP group collected data from 19 randomized trials and confirmed MFS as a valid intermediate clinical end point for OS (R 2 = 0.92, 95% confidence interval: 0.81-0.95). 65 Since then MFS has been extrapolated as a surrogate on different clinical scenarios especially in trials of early and adjuvant therapies; later MFS was also validated as surrogate for patients with nmCRPC. 66,67 However, in clinical practice, quality of life and treatment toxicity are a critical part of the decision-making process, especially in patients with long life expectancy.
The FDA approval of apalutamide was based on the improvement in MFS when compared to the placebo (median: 40.5 vs 16.2 months; hazard ratio [HR] = 0.28; P < .0001). The use of enzalutamide (PROSPER trial) was also approved using MFS as an end point, which more than doubled MFS compared to the placebo (median: 36.6 vs 14.7 months, HR = 0.29; P < .0001). Darolutamide, approved in 2019, also demonstrated a significant increase in MFS when compared to placebo (median: 40.4 vs 18.4 months; HR = 0.41; P < .0001; Table 2).
Results (SPARTAN, PROSPER, and ARAMIS).

Abbreviations: FU, follow-up; HR, hazard ratio; MFS, metastasis-free survival; PFS, progression-free survival; PSA, prostate-specific antigen.
General clinical practice guidelines for the treatment of patients with nmCRPC have been developed. The National Comprehensive Cancer Network (NCCN), the American Urological Association, and The European Association of Urology updated their guidelines. They recommend apalutamide and enzalutamide to be included as part of the first-line treatment for nmCRPC when PSA DT is equal to or less than 10 months. In cases where the PSA DT is greater than 10 months or the patient has a short life expectancy and/or poor performance status due to comorbidities, the guidelines indicate that observation is an option. While the NCCN has developed PCa guidelines specific for LATAM, the last update was in 2017, prior to the approval of the latest treatments. If category 1 drugs are unavailable or contraindicated, the NCCN Prostate Cancer Guidelines recommend that other treatment options be provided, such as secondary hormonal therapies (eg, nonsteroidal antiandrogens like nilutamide, flutamide, and bicalutamide or corticosteroids), despite the lack of information about quality of life and MFS-associated and clinical benefits of these drugs. The European Society of Medical Oncology and the American Society of Medical Oncology have not updated their recommendations yet.
Prostate Cancer: Challenges in LATAM
Applying international practice guidelines to LATAM is difficult given the financial barriers and the lack of country-specific information about populations with nmCRPC. Moreover, cultural, social, and health system differences among LATAM countries pose additional challenges for developing nmCRPC management policies for the region. Important challenges for the management and control of PCa in LATAM include: an aging population, which will invariably increase the number of individuals at risk for PCa and CRPC; a lack of comprehensive PCa registries in the majority of LATAM countries; a lack of timely diagnosis of the different stages of CRPC in targeted populations; inadequate and unequal access to the technologies necessary for the diagnosis and eventual treatment of PCa, including CT and bone scans, PSMA-PET, MRI, and radiation therapy; a lack of clinical practice guidelines for PCa management, including the proper use of new drugs and technologies that can impact quality of life and survival; the high cost of incorporating new drugs, even those that have been shown to have a direct impact on patient outcomes; a low level of awareness among PCa-related specialists of the latest information regarding the diagnosis, treatment, and management of CRPC.
Recommendations for Increasing Awareness, Early Diagnosis, and Treatment of PCa in LATAM
Given the differences between LATAM and other parts of the world, existing international PCa guidelines cannot always be extrapolated to the region’s unique economic, cultural, and regulatory landscape. Instead, LATAM countries must collaborate to determine the most effective strategies for counteracting this health issue and ensuring that the burden of PCa, including nmCRPC, is effectively managed. In this context, the following actions should be considered: Governments should implement comprehensive and reliable national cancer registries, with the goal of sharing information across the region and facilitating the development of integrated national and region-wide policies for PCa and nmCRPC; Stakeholders should establish national and region-wide cancer networks to optimize resources for the diagnosis, management, and treatment of patients with PCa; Prostate cancer–related specialists should identify the population of patients with nmCRPC at risk of developing metastasis. Health authorities, in conjunction with medical societies, should design programs specifically targeted for this population in order to ensure quality of life; Governments should promote access to newly approved PCa drugs, such as second line AR blockers, for patients with nmCRPC, and particularly for those with PSA DT of less than 10 months; Regulatory agencies should collaborate to review data on cost-effectiveness analyses regarding the treatment and management of nmCRPC; Professional associations should establish continuing medical education programs to ensure that CRPC populations are adequately identified, diagnosed, and managed. This also requires the development and implementation of education and awareness programs for primary care physicians on the importance of identifying patients at risk of PCa and directing them to specialists; Health authorities should help reduce time-to-diagnosis by increasing the availability and accessibility of high-quality conventional imaging methods for patients with nmCRPC; This panel is withholding any recommendation regarding the use of PSMA-PET scans until prospective data on utility and health outcomes in patients become available.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The organization and implementation of the consensus conference was carried out by the Americas Health Foundation (AHF), a 501(c)(3) nonprofit organization dedicated to improving healthcare throughout the Latin American Region and was supported by unrestricted grants from Astellas and Johnson & Johnson.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This manuscript was supported by a grant from the Americas Health Foundation (AHF), a 501(c)(3) nonprofit organization dedicated to improving healthcare throughout the Latin American Region. The AHF was responsible for the development, organization, and implementation of the consensus conference, along with independently selecting the experts to serve on the panel. The AHF had no role deciding the content of the manuscript and the recommendations are those solely of the panel members.