
Abstract
Objectives:
Analysis of tumor immune infiltration has been suggested to outperform tumor, node, metastasis staging in predicting clinical course of colorectal cancer (CRC). Infiltration by cells expressing OX40, a member of the tumor necrosis factor receptor family, or CD16, expressed by natural killer cells, monocytes, and dendritic cells, has been associated with favorable prognosis in patients with CRC. We hypothesized that assessment of CRC infiltration by both OX40+ and CD16+ cells might result in enhanced prognostic significance.
Methods:
Colorectal cancer infiltration by OX40 and CD16 expressing cells was investigated in 441 primary CRCs using tissue microarrays and specific antibodies, by immunohistochemistry. Patients’ survival was evaluated by Kaplan-Meier and log-rank tests. Multivariate Cox regression analysis, hazard ratios, and 95% confidence intervals were also used to evaluate prognostic significance of OX40+ and CD16+ cell infiltration.
Results:
Colorectal cancer infiltration by OX40+ and CD16+ cells was subclassified into 4 groups with high or low infiltration levels in all possible combinations. High levels of infiltration by both OX40+ and CD16+ cells were associated with lower pT stage, absence of peritumoral lymphocytic (PTL) inflammation, and a positive prognostic impact. Patients bearing tumors with high infiltration by CD16+ and OX40+ cells were also characterized by significantly longer overall survival, as compared with the other groups. These results were confirmed by analyzing an independent validation cohort.
Conclusions:
Combined infiltration by OX40+ and CD16+ immune cells is an independent favorable prognostic marker in CRC. The prognostic value of CD16+ immune cell infiltration is significantly improved by the combined analysis with OX40+ cell infiltration.
Introduction
Colorectal cancer (CRC) is the second most common cause of cancer-related deaths in industrialized countries. 1 Colorectal cancer screening tests, including fecal occult blood test, fecal immunochemical test, flexible sigmoidoscopy, and colonoscopy are recommended by the age of 50. 2 Following CRC diagnosis, treatment decisions are largely based on tumor, node, metastasis (TNM) staging, as described by the Union for International Cancer Control/American Joint Committee on Cancer. Since advanced TNM stage does not appear to necessarily correlate with increased risk of recurrence or death, this practice is currently debated. 3
Analysis of tumor microenvironment (TME) is emerging as a novel and/or complementary staging approach. 4 -7 Although the role of CRC infiltration by cells of the innate immunity system is still unclear, 8 several reports have convincingly shown that infiltration by cells of the adaptive immune system has a critical prognostic significance. 9 -11 A number of studies indicate that high densities of CD8+ cells in CRC are associated with improved overall survival. 9 -12 Furthermore, infiltration by FOXP3+ regulatory T cells and myeloid cells has also been shown to correlate with improved prognosis in human CRC 13 -15 at difference with frequently reported experimental models. 16
Activated CD4+ and CD8+ T cells express OX40, a member of the tumor necrosis factor-receptor superfamily, 17 -19 whereas CD16 is expressed by an array of cells including monocytes, natural killer (NK) cells, and dendritic cells (DCs). 20 -22 Previous work indicates that tumor infiltration by OX40+ or CD16+ cells represents an independent favorable prognostic factor in patients with CRC. 13,23,24 We could also previously demonstrate that OX40+ cell infiltration enhances the prognostic significance of CD8+ cell infiltration in CRC. 23 The aim of this study was to evaluate whether the analysis of this activation marker also enhances the prognostic significance of tumor infiltration by cells expressing CD16, a marker of innate immune response.
Materials and Methods
Tissue Microarray Construction
A total of 441 unselected, nonconsecutive, primary CRC samples were included in the tissue microarray (TMA) and formalin-fixed, paraffin-embedded tissue blocks were generated. Approval by the Regional Ethics Committee (EKBB, Basel Stadt and Basel Land) for the use of this clinically annotated TMA was obtained in advance; 0.6 mm wide tissue cylinders were punched from morphologically representative areas of each donor block and included into one recipient paraffin block (30 × 25 mm), using a semiautomated tissue arrayer, as previously described. 25 Each TMA spot consisted of at least 50% tumor cells.
Clinicopathological Features
Clinicopathological data for the 441 patients with CRC included in the TMA have previously been published. 26 Briefly, data were collected retrospectively in a nonstratified and nonmatched manner. Annotation included patient age, tumor diameter, location, pT/pN stage, grade, histologic subtype, vascular invasion, border configuration, presence of peritumoral lymphocytic inflammation at the invasive tumor front, and disease-specific survival. Tumor border configuration and peritumoral lymphocytic inflammation were evaluated using the original hematoxylin and eosin slides of the resection specimens corresponding to each TMA punch. 27
Immunohistochemistry
Standard indirect immunoperoxidase procedures were used for immunohistochemistry (IHC; ABC-Elite, Vector Laboratories, Burlingame, California). Slides were dewaxed and rehydrated in distilled water. Endogenous peroxidase activity was blocked using 0.5% H2O2. Sections were incubated with 10% normal goat serum (DakoCytomation, Carpinteria, California) for 20 minutes and incubated with primary antibody at room temperature (RT). Primary antibodies used were specific for CD16 and OX40 (polyclonal anti-CD134/OX40, ab119904, Abcam, Cambridge, United Kingdom; biotinylated anti-CD16 were purchased from DAKO (Glostrup, Denmark) and Novocastra (Newcastle, United Kingdom). Fluorescein isothiocyanate-conjugated anti-CD16, phycoerythrin-conjugated anti-CD16, Cy5-conjugated anti-CD16, and isotype-matched monoclonal antibody were purchased from BD Bioscience (San Jose, California), as previously published by our group. 22,23 Subsequently, sections were incubated with peroxidase-labelled secondary antibody (DakoCytomation) for 30 minutes at RT. For antigen visualization, sections were immersed in 3-amino-9-ethylcarbazole plus substrate-chromogen (DakoCytomation) for 30 minutes and counterstained with Gill’s hematoxylin.
Evaluation of IHC
CD16 and OX40 data were available from previous publications. 22,23
Description of cutoff value calculation for OX 40
Cutoff values used to classify CRC with low- or high-immune cell infiltration were obtained by receiver operating characteristic (ROC) curves (survival ROC package), evaluating sensitivity and false positive rate for the discrimination of survivors and nonsurvivors with respect to the Kaplan-Meier method, on the training subset and validated on the validation subset. The threshold value for OX40+ infiltration, calculated in the training test, was 40 cells/TMA-punch. This value was reconfirmed in the validation set. 23,28,29
Description of cutoff value calculation for CD 16
Cutoff scores for protein marker positivity were determined on the test group using ROC curve analysis with the end point survival/death and the 0,1 criterion to select the most discriminating cutoff score from the ROC curve. Cut-off scores were further validated by assessing the interobserver variability of positivity by a second and a third observer. For the basel CD16 study, the level of innate inflammatory cell infiltration was scored as 1 and 2, when the CD16+ infiltrate consisted of 10 cells and >10 cells per punch, respectively. For the Athens CD16 study, similar to the Basel study, the cutoff was also set at 10 immunoreactive cells. 29,30
Tumor infiltrating cells were counted for each punch (approximately 1 high power [20×] field). All immunohistochemical reading was performed by a trained research fellow, and data were independently validated by an additional investigator, as previously described. 23 Samples of CD16 and OX40 staining is shown in Figure 1.

Samples of CD16 and OX40 staining (40×). Negative control (A); single positive biopsy for CD16 (B); single positive biopsy for OX40 (C); CD16 (D), and OX40 (E) staining of the same double positive biopsy.
Statistical Analysis
All statistical analyses were made using STATA software version 13 (StataCorp, College Station, Texas). Associations with survival were explored using the Cox proportional hazard regression model. Cutoff values used to classify CRC with low- or high-immune cell infiltration were available from previous publications. 23,28,29 Threshold value for OX40+ infiltration, calculated in the training test, was 40 cells/TMA-punch. This value was reconfirmed in the validation set. Further specific scores were set at 10 cells/TMA-punch for CD16 and 17 cells/TMA-punch for FOXP3, as previously calculated in larger collectives by our team. 30 Chi-square, Fisher exact, and Kruskal-Wallis tests were used to determine the association of OX40+ and CD16+ cell infiltration and clinical pathological features. For survival analysis, the study population was randomly assigned to test and validation groups. Univariate survival analysis was performed by Kaplan-Meier and log-rank tests. Further analysis included 4 combinations of OX40+ and CD16+ cell density: OX40−/CD16−, OX40+/CD16−, OX40−/CD16+, and OX40+/CD16+.
The assumption of proportional hazards was verified for all markers by analyzing correlation of Schoenfeld residuals and ranks of individual failure times. Any missing clinicopathological information was assumed to be missing at random. Subsequently, OX40+ and CD16+ cell density data were entered into multivariate Cox regression analysis, and hazard ratios (HRs) and 95% confidence intervals (CIs) were used to determine prognostic effects on survival time; P values <.05 were considered statistically significant.
Results
Patient and Characteristics
A total of 441 CRC tissues were analyzed. Median age was 70.6 years (range 40-96). Of 441 patients, 235 were female and 206 were male. Most samples were from left-sided tumors (n = 290). Median tumor size was 50 mm (range 5-170). Histopathologic assessment revealed that 19 CRCs were T1, 60 T2, 286 T3, and 63 T4. Regarding N stage, 229 CRCs were N0, 113 N1, and 83 N2. Most CRCs were classified as grade 2 tumors (388), while 13 were grade 1 and 26 grade 3. In all, 302 CRCs showed infiltrative tumor border configuration, and vascular invasion was undetectable in 303 cases. Among all samples, 379 were mismatch repair (MMR) proficient, and 62 were MMR-deficient cancers. Median overall survival was 62.1 months (range 1-152), and the median 5-year survival was 0.47 (range 0.43-0.52; Table 1).
Characteristics of CRC Patient Cohort.a,b

Abbreviations: CI, confidence interval; CRC, colorectal cancer; UICC, Union for International Cancer Control.
a n = 441.
b Percentages may not add to 100% due to missing values of same variables. Age and tumor size were evaluated using the Kruskal-Wallis test. Gender, anatomical site, T stage, N stage, grade, vascular invasion, and tumor border configuration were analyzed using the χ2 test. Survival analysis was performed using the Kaplan-Meier method.
Association of Clinicopathological Features With Infiltration by OX40+ and CD16+ cells
In order to understand whether infiltration by cells expressing OX40 or CD16 correlates with specific histologic parameters, we performed a statistical comparison of different clinicopathological features, as assessed histologically by an experienced pathologist (LT). Therefore, we subclassified OX40+ and CD16+ cell infiltration in the following groups: (1) OX40high and CD16high, (2) OX40high and CD16low, (3) OX40low and CD16high, and (4) OX40low and CD16low. Statistical analyses revealed that CRCs with high levels of infiltration by both OX40+ and CD16+ cells were associated with lower T stage, as compared with the CRCs with OX40low CD16low infiltration status (P = .003, Table 2). Furthermore, OX40high and CD16high infiltration status was associated with N0 status (P = .016, Table 2). Finally, high infiltration by OX40+ and CD16+ cells was associated with presence of PTL inflammation (P = .015, Table 2).
Association of OX40+ and CD16+ Low- and High-Immune Cell Density With Clinicopathological Features in CRC.a

Abbreviations: CI, confidence interval; CRC, colorectal cancer; SD, standard deviation.
a Percentages may not add to 100% due to missing values of same variables. Variables are indicated as absolute numbers, %, median, or range; age and tumor size were evaluated using the Kruskal-Wallis test. Gender, anatomical site, T stage, N stage, grade, vascular invasion, and tumor border configuration were analyzed using the χ2 test. Survival analysis was performed using the Kaplan-Meier method.
P values <.05 were considered statistically significant.
In contrast, no association was found between tumor infiltration by cells expressing OX40 or CD16 and age, tumor diameter, gender, tumor location, histologic subtype, tumor grade, vascular invasion, tumor border, and microsatellite stability (P > .005, Table 2).
Subgroup analysis (OX40low/high; CD16low/high) of single OX40 or CD16 expression is shown in Supplementary Tables 1S to 4S. Interestingly, the most significant 5-year survival rate difference for double positive biopsies was seen in the CD16high (Supplementary Table 2S) and OX40 high (Supplementary Table 4S) subgroup.
Prognostic Significance of Tumor Infiltration by OX40+ or CD16+ Cells
Univariate Hazard Cox regression survival analysis was performed considering combined infiltration by OX40+ and CD16+ cells (Table 3). As expected, we observed that poor survival was significantly associated with age (HR = 1.02; 95% CI = 1.01-1.04; P = <.001), gender (HR = 1.68; 95% CI = 1.31-2.16; P = <.001), pT stage (HR = 2.57; 95% CI = 1.72-3.84; P = <.001), pN stage (HR = 2.88; 95% CI = 2.22-3.73; P = <.001), vascular invasion (HR = 2.12; 95% CI = 1.63-2.75; P = <.001), and invasive margin (HR = 1.63; 95% CI = 1.22-2.19; P = <.001). In contrast, most importantly, CRC infiltration by OX40+ and CD16+ cells was significantly associated with favorable prognosis (HR = 0.52; 95% CI = 0.36-0.77; P = <.001). Multivariate analysis confirmed that the combination of high-density OX40+ and CD16+ cell infiltration (HR = 0.58; 95% CI = 0.39-0.87; P = .01) represents a positive prognostic factor for survival in CRC. Expectably, age (HR = 1.03; 95% CI = 1.02-1.05; P = <.001), gender (HR = 1.73; 95% CI = 1.32-2.26; P = <.001), pT (HR = 1.75; 95% CI = 1.12-2.71; P = .01), pN (HR = 2.25; 95% CI = 1.70-2.98; P = <.001), and vascular invasion (HR = 1.65; 95% CI = 1.25-2.17; P = <.001) were found to independently correlate with poor prognosis in multivariate analysis, as well (Table 3).
Uni- and Multivariate Hazard Cox Regression Survival Analysis Considering the Combination of Both Markers.a,b

Abbreviations: CI, confidence interval; CRC, colorectal cancer; HR, hazard ratio; MMR, mismatch repair.
a n = 441 and n = 409.
b Multivariate analyses showing hazard ratios and P value for all CRCs (n = 409 less than 441 due to missing values) conferred by CD16+ and OX40+ cell density, age, sex, tumor size, lymph node involvement, tumor grade, vascular invasion, tumor border configuration, and microsatellite stability.
P values <.05 were considered statistically significant.
Supplementary Tables 5S to 8S show the prognostic effects of single OX40 expression based on low- or high-CD 16 expression and vice versa.
Synergistic Prognostic Significance of OX40+ and CD16+ Cell Infiltration in the CRC Microenvironment
To increase the robustness of our results, we evaluated overall survival by combining OX40 and CD16 markers in a testing (n = 217) and a validation group (n = 220). Cutoff score of OX40+ and CD16+ tumor infiltrating CRC cells for the assessment of their prognostic significance was established by regression tree analysis at 40 and 10 cells/punch, respectively. Kaplan-Meier plots indicate that in both testing and validation groups, high CD16+ and OX40+ cell infiltration in CRC is associated with improved overall survival, as compared to tumors lacking infiltration by one or both cell subsets (Figure 2A and B).
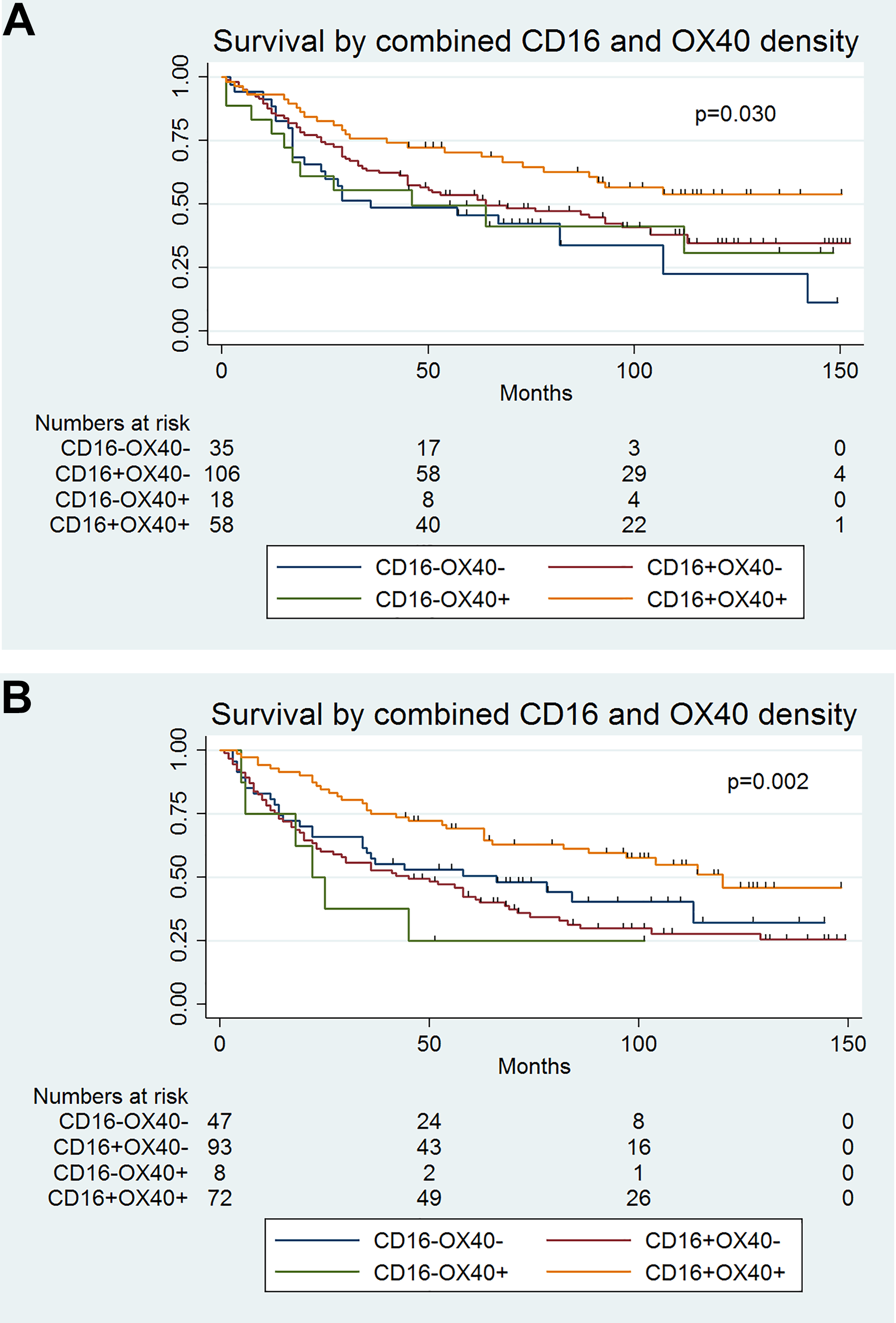
A and B, Overall survival according to OX40+ and CD16+ cell density in a test (n = 217) and validation group (n = 220). Effects of tumor infiltration by OX40+ and CD16+ cells on overall survival in patients with CRC. Kaplan-Meier overall survival curves were designed according to tumor infiltration by OX40+ and CD16+ cells in patients bearing CRC as indicated. Cutoff values established by regression tree analysis were 40 cells/punch for OX40 and 12 cells/punch for CD16 cell infiltration. 23,28,29 . Cumulative effects of tumor infiltration by OX40+ and CD16+ cells were explored. Blue line indicates tumors with low OX40+ and low CD16+ cell infiltration. Green line refers to tumors with low CD16+ and high OX40+ cell infiltration. Purple line refers to tumors with high CD16+ cell infiltration and low OX40+ cell infiltration. The orange line refers to CRC with high CD16+ cell infiltration and high OX40+ cell infiltration. CRC indicates colorectal cancer.
Discussion
Seminal research by the Galon group indicates that analysis of immune cell infiltration in CRC has a superior prognostic value, as compared to TNM classification system. 11
CD16 is a receptor for immunoglobulin G Fc fragment mostly expressed by myeloid cells and NK cells. 20 -22 Tumor infiltration by CD16+ cells is detectable in different malignancies, 31 but their actual immunobiological significance remains largely unclear. The origin of CD16+ cell infiltrate is not fully understood. Previous investigations show that these cells are large (40-50 μm) similarly to tumor-associated macrophages and phenotypically resemble immature DC (CD16+, CD11b+, CD11c+, CD33+, CD14−). 13 However, M1 polarized monocytes/macrophages, characterized by high CD16 expression, 32 might also provide significant antitumor functions. 33
OX40 plays a pivotal role in differentiation and survival of CD4+ cells. Expression of OX40 increases the formation and survival of antigen-specific T cells and OX40-mediated costimulation lead to increases of memory T cells. 34 The OX40 expression has mainly been observed in CD4+ T cells and, predominantly, on a large number of activated CD4+ T cells, including Th1 and Th17 cells as well as Foxp3+ CD4+ regulatory T cells. 17,18,35 Infiltration by OX40+ immune cells has been suggested to mirror antitumor immune response in cancer tissue. 36,37 Lack or loss of this response may, therefore, lead to disease progression, and antitumor relevance of OX40 expression has been described in animal models of colon and breast cancer, sarcoma, and melanoma. 18,24,38
In previous research, the individual prognostic value of CRC infiltration by OX40+ and CD16+ cells, predicting prolonged survival, has already been demonstrated. 13,24 Our results clearly confirm these data. 22,23 Most importantly, for the first time, based on the analysis of a large number of patients (n = 441), our study demonstrates that the combination of OX40+ and CD16+ cell infiltration is an independent, positive prognostic marker for patients with CRC. In contrast, low densities of tumor-infiltrating immune cells expressing these markers might reflect lack of tumor immunity or loss of responsiveness, possibly due to progressing tumor cell dedifferentiation. 39
Our study presents several limitations. First, we could not investigate effects of tumor infiltration by OX40+ and CD16+ cells on disease-free survival. Furthermore, the TMA used in this study included single samples from each individual tumor, thereby potentially underestimating TME heterogeneity. However, the high number of case studies might help to overcome this limitation.
Our study cannot provide information concerning the colocalization of OX40- and CD16-expressing lymphocytes within the tumor. Our study classifies TME into CD16 and/or OX40 low and high biopsies but does not give any information about the position of the 2 biomarkers as shown in Figure 1. However, the fact that biopsies with a double positive microenvironment have a significantly better 5-year survival adds still important information for daily clinical decision-making.
The retrospective nature of this study also represents a limitation but has the potential to support the generation of future prospective studies. The long time frame of patient recruitment (1985-1998) can also be discussed as a further limitation. In view of treatment evolution, for example, neoadjuvant chemotherapy, it is questionable how far this patient cohort reflects actual clinical framework. On the other hand, tissues generated from these CRC specimens may more accurately characterize immunobiology of untreated cancers.
All in all, our results indicate that OX40+ immune cell infiltration significantly improves the prognostic value of CD16+ immune cell infiltration in CRC. The combination of CD16+ and OX40+ cell infiltration emerges as an independent favorable prognostic predictor, thereby extending the fast-growing area of knowledge regarding the prognostic value of the expression of immunomodulatory molecules by immune cells in CRC-TME.
Supplemental Material
Supplemental Material, Supplemental_tables - Tumor Infiltration by OX40+ Cells Enhances the Prognostic Significance of CD16+ Cell Infiltration in Colorectal Cancer
Supplemental Material, Supplemental_tables for Tumor Infiltration by OX40+ Cells Enhances the Prognostic Significance of CD16+ Cell Infiltration in Colorectal Cancer by Fabian Haak, Isabelle Obrecht, Nadia Tosti, Benjamin Weixler, Robert Mechera, Silvio Däster, Marco von Strauss, Tarik Delko, Giulio C. Spagnoli, Luigi Terracciano, Giuseppe Sconocchia, Markus von Flüe, Marko Kraljević and Raoul A. Droeser in Cancer Control
Footnotes
Authors’ Note
Fabian Haak, Isabelle Obrecht, Marko Kraljević, and Raoul A. Droeser equally contributed to this work. Patients are retrospectively selected from the databank system at Pathology (PathowinPlus) from which adequate FFPE- and/or frozen specimens were collected within the Biobank at the institute (Biobank Pathology-USB = BPUSB—see regulation of February 2014). The status of general consent to the further use of patient data and samples for research purposes is actualized in PathowinPlus every day. In case patient’s Veto for research the data and samples are excluded from the study list. The clinical anamnesis and follow-up data will be extracted from the clinical records of the patients (from PathowinPlus and/or Ismed).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sources of financial support: Giuseppe Sconocchia was supported by the Italian Association for Cancer Research (AIRC), IG17120.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.