
Abstract
Objectives
To explore the effect of combined hematological and physical measurement indicators on the prognosis of patients undergoing surgery for gastric or colorectal cancer and to screen for the best prognostic indicators.
Introduction
Gastric and colorectal cancer is a widespread health concern worldwide and one of the major contributors to cancer-related death. The hematological and physical measurement indicators have been shown to associate with the prognosis of patients undergoing surgery for gastric or colorectal cancer, respectively, but it is still unclear whether the combination of the two can reflect the prognosis more effectively.
Methods
Thirteen hematological indicators and 5 physical measurement indicators were selected in this study, and the most promising ones were screened using LASSO regression. Then, the best prognostic indicators were selected by time-ROC curves. Survival curves were constructed using the Kaplan–Meier method, and the effects of hematological and physical measurement indicators on the prognosis of patients undergoing surgery for gastric or colorectal cancers were evaluated by Cox proportional risk regression analysis. In addition, the relationship between hematological and physical measurement indicators on secondary outcomes, including length of stay, hospitalization costs, intensive care unit (ICU) admission, and patients’ subjective global assessment scores (PGSGA), was explored.
Results
After initial screening, among the hematological indicators, the geriatric nutritional risk index (GNRI) showed the highest mean area under the curve (AUC) values. Among body measures, calf circumference (CC) showed the highest mean AUC value. Further analyses showed that the combination of combined nutritional prognostic index (GNRI) and calf circumference (CC) (GNRI-CC) had the best performance in predicting the prognosis of patients undergoing surgery for gastric or colorectal cancers. Low GNRI, low CC, and low GNRI-low CC increased the risk of death by 44%, 48%, and 104%, respectively. Sensitivity analyses showed the same trend. In addition, low GNRI-low CC increased the risk of malnutrition by 17%.
Conclusion
This study emphasizes that a combination of blood measures and body measures is essential to accurately assess the prognosis of patients undergoing surgery for gastric or colorectal cancers. The GNRI-CC is a good prognostic indicator and can also assess the risk of possible malnutrition.
Keywords
Introduction
Gastrointestinal cancer stands as a widespread global health concern and holds its position as a foremost contributor to cancer-related mortalities. 1 Within the context of China, projections suggest that in 2022, the 5 most frequently diagnosed cancer types will encompass lung, colorectal, gastric, liver, and breast cancer. 2 The cornerstone of gastrointestinal cancer treatment is surgery.3,4 However, it is important to emphasize that following resection of gastrointestinal tumors, there are certain anatomical changes within the gastrointestinal tract. 4 This surgical intervention can potentially lead to disruptions in vital physiological processes such as digestion, absorption, and secretion. Particularly in cases of extensive tumor excisions, patients may face more complex situations. This may engender a cascade of complications postoperatively, including infections, emaciation, and muscle wastage. These complications have the potential to significantly compromise patients’ quality of life and postoperative prognosis.5,6
In recent years, a number of hematological indicators have emerged that can reflect immunoinflammatory level, including prognostic nutritional index (PNI), neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio, advanced lung cancer inflammatory index (ALI), platelet-to-lymphocyte ratio (PLR), and systemic immune-inflammatory index (SII).7-10 Systemic inflammation is a general phenomenon and exhibits a profound relationship with the initiation, progression, and metastasis of cancer.11-13 Importantly, empirical evidence supports the direct relationship between a heightened inflammatory state and the prognosis of patients with gastric or colorectal cancer. In addition, physical measurement indicators have emerged as crucial tools for assessing the prognosis of cancer patients.14,15 By monitoring and analyzing these indicators, a more precise understanding of patients’ physical status and nutritional conditions can be gained. Surgery can have a range of adverse effects on the body, including muscle loss, weight reduction, and nutritional deficiencies. 16 Preoperative evaluation of physical measurement indicators contributes to assessing patients’ overall health status and surgical risks, while also providing predictive value for their long-term survival and quality of life.
Previous research has predominantly focused on elucidating the individual impacts of hematological and physical measurement indicators on the prognosis of patients undergoing surgery for gastric and colorectal cancer, respectively. However, there were few studies investigating the combined effects of hematological and physical measurement indicators on prognosis. Consequently, we have chosen patients undergoing surgery for gastric and colorectal cancer as target population to investigate this aspect.
Methods
Study Participants
The INSCOC cohort, a multicenter cross-sectional study, was designed to investigate the general health status and clinical outcomes of cancer patients.
17
This study was a retrospective study and collected data from April 2013 to September 2019. Each patient has a unique ID number and all patient details are de-identified. In its initial phase, the study included 1669 patients undergoing surgery for gastric or colorectal cancers. To ensure the rigor of the research, certain participants were excluded from the study based on the following criteria: (1) those who had undergone neoadjuvant chemotherapy and radiation, (2) those lacking subsequent follow-up data, and (3) those possessing incomplete clinical records (Figure 1). As a result, 1188 participants were ultimately included in the study. Flow chart.
Clinical Characteristics
Body mass index (BMI) was calculated as weight/height2 (kg/m2), and its classification followed Asian standardized cut-off values, specifically categorized into ranges of <18 kg/m2, 18–24 kg/m2, and ≥24 kg/m2. 18 To provide a deeper analysis, a range of composite immunoinflammatory indicators were computed. The specific computational formulas employed for these indicators can be found in Supplementary Table 1.
Outcome Evaluation
All enrolled patients actively participated in either telephone interviews or outpatient follow-up appointments as dictated by the study’s protocol. The primary observed outcomes under scrutiny included instances of mortality, calculated from the initial diagnosis of cancer until the time of death, as well as occurrences of withdrawal from the study or the latest recorded follow-up.
Statistical Analysis
In this study, continuous variables that displayed normal or non-normal distribution were presented as mean (standard deviation [SD]) or median (interquartile range [IQR]), respectively. Categorical variables were presented as absolute numbers (proportions). LASSO regression was used to winnow down the potential hematological and physical measurement indicators. To pinpoint the optimal cut-off value for distinct indicators, the maximally selected log-rank statistic was employed and the corresponding values were displayed in Supplementary Table 2. Subsequently, the time-ROC curve was used for selecting the most robust prognostic indicator from these candidates. The t test was used to compare the mean AUC values of different indicators, thus facilitating identifying the best indicators. The nonlinear relationship between the best indicators and OS was unveiled through restricted cubic spline curves. The survival curve was constructed through the Kaplan–Meier method, followed by validating through the log-rank test. To quantitatively assess the association between the combination of the hematological indicator and the physical measurement indicator and overall survival (OS), hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated. Model a was an unadjusted model; model b was adjusted for age, sex, BMI, and TNM stage; and model c was additionally adjusted for smoking status, alcohol consumption, hypertension, diabetes, enteral nutrition, and parental nutrition. Sensitivity analysis was used to enhance the study’s robustness; participants who died within 3 months were excluded to mitigate the potential impact of reverse causation. Lastly, we expanded the scope of investigation to encompass secondary outcomes, including length of stay, hospitalization costs, ICU admission ratio, and the Patient-Generated Subjective Global Assessment (PGSGA) scores. We scrutinized the relationship between the combination of the hematological indicator and the physical measurement indicator and secondary outcomes through the logistic regression analysis. The reporting of this study conforms to STROBE guidelines. For the statistical analyses, R software version 4.2.0 was leveraged. All P-values below the threshold of .05 from the two-sided test were deemed statistically significant.
Results
Selection of Hematological and Physical Measurement Indicators
We initially incorporated thirteen hematological and 5 physical measurement indicators into our analysis (Supplementary Table 1). The results of the LASSO regression unveiled that 8 hematological indicators (PNI, NLR, SII, ALI, albumin-to-globulin ratio [AGR], geriatric nutritional risk index [GNRI], platelet-to-albumin ratio [PAR], and neutrophil-to-albumin ratio [NAR]) and all the physical measurement indicators (BMI, mid-arm circumference [MAC], triceps skinfold [TSF], hand grip strength [HGS] and calf circumference [CC]) displayed non-zero coefficients (Figure 2). The outcomes of the time-ROC curve suggested that among the hematological indicators, GNRI exhibited the highest average Area Under the Curve (AUC) value (mean AUC: .569) (Supplementary Figure 1). Among the physical measurement indicators, though CC showcased the highest average AUC value (mean AUC: .570), there were no statistically significant differences in mean AUC values when compared to MAC (mean AUC: .559) and TSF (mean AUC: .554) (Supplementary Figure 1). Consequently, we proceeded to examine the combined effects of GNRI with CC, MAC, and TSF by comparing their respective AUC values. Taking GNRI and CC as an illustrative example, we segregated the participants into 4 groups: Group 1 (high GNRI and high CC), Group 2 (high GNRI and low CC), Group 3 (low GNRI and high CC), and Group 4 (low GNRI and low CC). The outcomes revealed that, compared with GNRI-MAC (mean AUC: .596) and GNRI-TSF (mean AUC: .596), GNRI-CC demonstrated the highest average AUC value (mean AUC: .608) (P < .05) (Figure 3). The KM curves for these indicators are shown in Supplementary Figure 2. These findings led us to select GNRI and CC for the subsequent analysis, exploring their combined effects with the prognosis of patients undergoing surgery for gastric or colorectal cancers. Screening of Hematological and Physical measurement Indicators Using LASSO Regression. Notes: (A-B) hematological indicators; (C-D) physical measurement indicators. Comparison the Effectiveness of Combined Indicators in Predicting the Prognosis of Patients Undergoing Surgery for Gastric or Colorectal Cancer Using ROC Curves. Abbreviations: GNRI: geriatric nutritional risk index; CC: calf circumference; MAC: mid-arm circumference; TSF: triceps skinfold.

Baseline Characteristics
Baseline Characteristics.
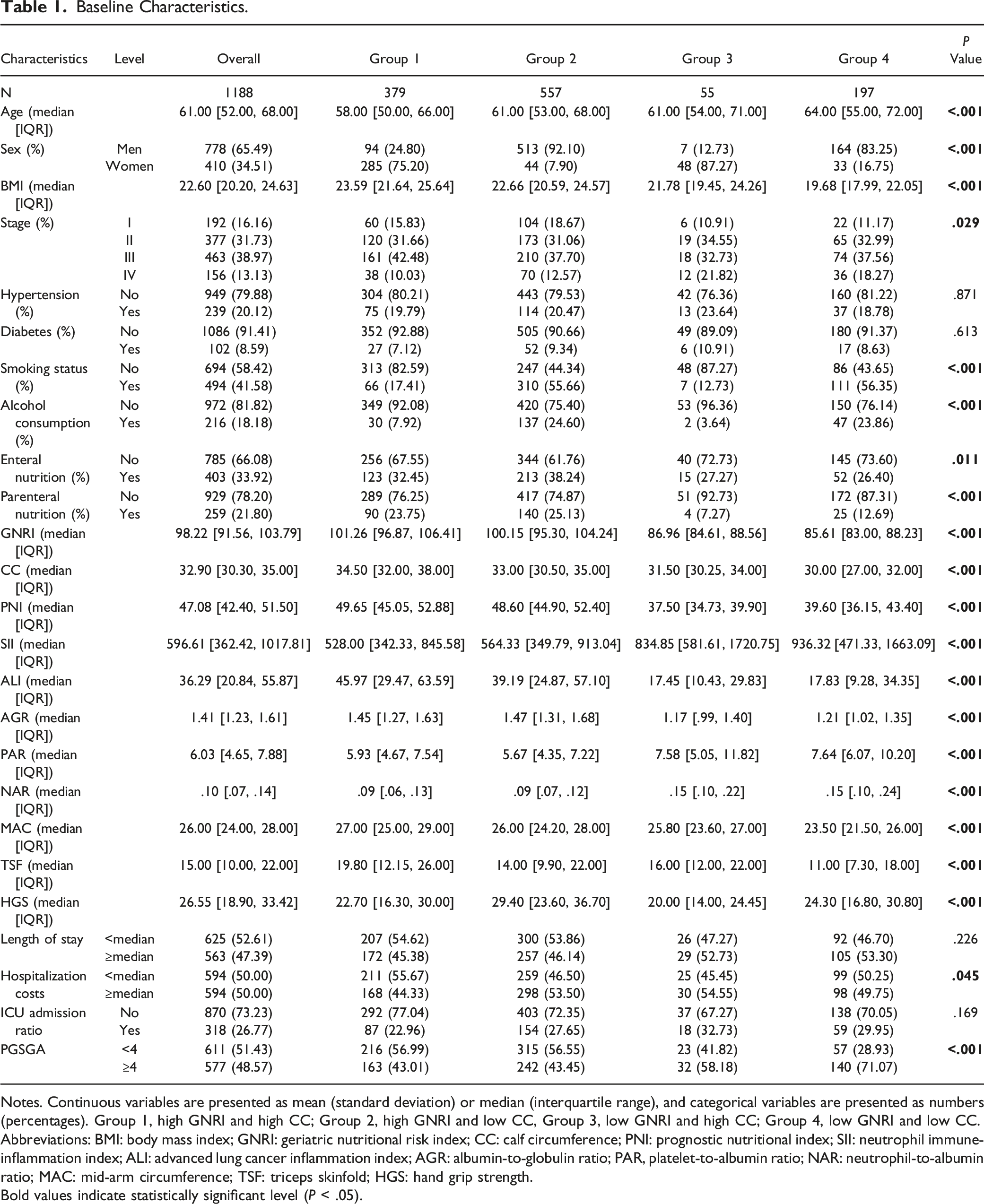
Notes. Continuous variables are presented as mean (standard deviation) or median (interquartile range), and categorical variables are presented as numbers (percentages). Group 1, high GNRI and high CC; Group 2, high GNRI and low CC, Group 3, low GNRI and high CC; Group 4, low GNRI and low CC.
Abbreviations: BMI: body mass index; GNRI: geriatric nutritional risk index; CC: calf circumference; PNI: prognostic nutritional index; SII: neutrophil immune-inflammation index; ALI: advanced lung cancer inflammation index; AGR: albumin-to-globulin ratio; PAR, platelet-to-albumin ratio; NAR: neutrophil-to-albumin ratio; MAC: mid-arm circumference; TSF: triceps skinfold; HGS: hand grip strength.
Bold values indicate statistically significant level (P < .05).
Relationship Between GNRI-CC and OS
The Association Between GNRI Combined With CC and OS.
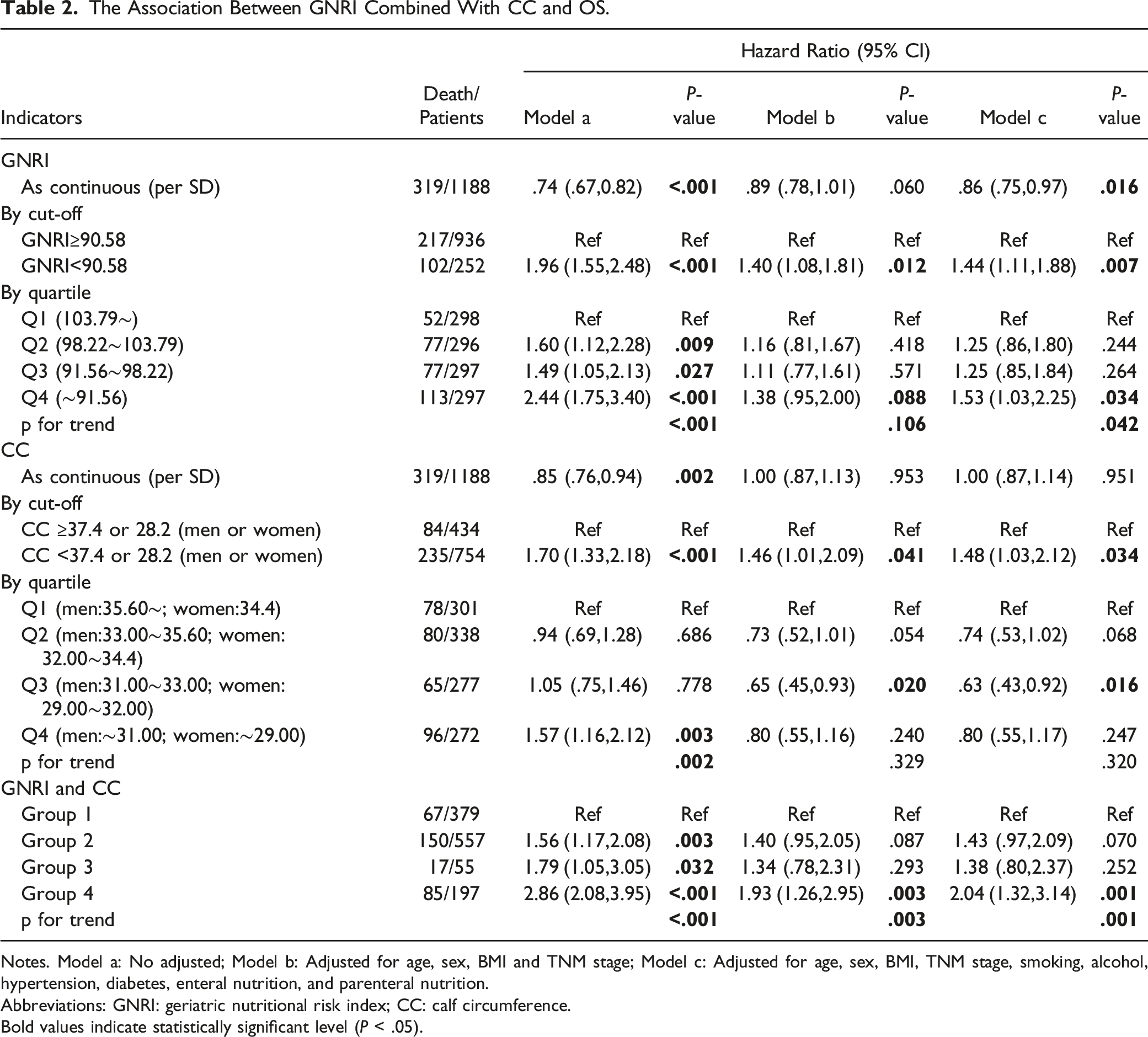
Notes. Model a: No adjusted; Model b: Adjusted for age, sex, BMI and TNM stage; Model c: Adjusted for age, sex, BMI, TNM stage, smoking, alcohol, hypertension, diabetes, enteral nutrition, and parenteral nutrition.
Abbreviations: GNRI: geriatric nutritional risk index; CC: calf circumference.
Bold values indicate statistically significant level (P < .05).
Sensitivity Analysis. (Excluded Participants Died Within 3 Months).

Notes. Model a: No adjusted; Model b: Adjusted for age, sex, BMI, and TNM stage; Model c: Adjusted for age, sex, BMI, TNM stage, smoking, alcohol, hypertension, diabetes, enteral nutrition, and parenteral nutrition.
Abbreviations: GNRI: geriatric nutritional risk index; CC: calf circumference.
Bold values indicate statistically significant level (P < .05).
Relationship Between GNRI-CC and Secondary Outcomes
Finally, this study extended to explore the relationship between GNRI-CC and key healthcare metrics, including length of stay, hospitalization costs, ICU admission ratio, and PGSGA scores. Through the logistic regression, the results are displayed in Supplementary Table 3. Group 4 displayed a positive relationship with elevated PGSGA scores, thereby elevating the risk of malnutrition by 17% (adjusted hazard ratio [aHR], 1.17; 95% CI, 1.06–1.31; P = .003). However, the relationship of GNRI-CC with the other 3 outcomes was not significant. This finding revealed a tangible relationship between GNRI-CC and the propensity for malnutrition.
Discussion
This study offers valuable insights into prognostic factors for patients undergoing surgery for gastric or colorectal cancers. The research revealed that GNRI-CC holds significant predictive value for OS. Specifically, low GNRI and low CC were associated with a significantly elevated risk of death, with the highest risk observed in patients belonging to the low GNRI and low CC group. The results consistently demonstrated the superior predictive performance of the combined GNRI-CC metrics. The study underlines the importance of utilizing a combination of hematological and physical measurement indicators for accurately predicting the prognosis. It highlights that relying solely on single-factor assessment might not suffice for precisely predicting patient survival.
In previous studies, several studies have examined the association between hematological and physical measurement indicators and the long-term prognosis of patients undergoing surgery for gastric or colorectal cancer. Immunoinflammatory indicators such as GNRI, SII, PNI, ALI, and NLR have been demonstrated to hold prognostic significance in this patient population.19-23 For instance, a study involving 225 patients with stage III gastric cancer who underwent R0 resection aimed to identify optimal markers and their respective cut-off points. The findings indicated that CAR and PLR were independent prognostic factors for OS and tumor-specific survival, respectively. 24 Furthermore, a retrospective cohort study encompassing 8257 cancer patients explored the impact of low HGS on cancer-related mortality. The outcomes of this study indicated that reduced HGS is a risk factor for colorectal cancer in both men and women. 25 Another study involving 502,293 participants from the UK Biobank aimed to investigate the association between HGS and the incidence of cardiovascular, respiratory, and cancer, as well as all-cause mortality. The results revealed that diminished HGS was associated with an increased risk of cancer incidence and all-cause mortality. 26 Nevertheless, no prior study has examined the combined influence of hematological and physical measurement indicators on the prognosis of patients undergoing surgery for gastric or colorectal cancer. Our study addresses this gap in the existing literature by exploring this relationship.
The impact of hematological and physical measurement indicators on the prognosis of patients undergoing surgery for gastric or colorectal cancers may involve several intricate biological mechanisms.27-30 First, cytokines and inflammatory mediators released from tumor tissues can prompt an inflammatory response within the body, activating immune cells and triggering excessive cytokine release. This process might establish a favorable microenvironment that facilitates tumor growth, proliferation, and invasion, subsequently influencing patient prognosis. Second, nutritional status holds utmost importance for the recovery and survival of cancer patients. Post-surgery for gastric or colorectal cancers, nutritional intake could become constrained, potentially leading to protein-energy malnutrition in patients. Low CC in the preoperative period reflects an inadequate reserve of the patient’s nutritional status, implying that the body lacks sufficient energy and nutrients to support the postoperative healing and repair process, and therefore may affect the postoperative recovery and long-term prognosis. Moreover, the anatomical and physiological modifications occurring within the gastrointestinal tract due to surgical resection might further impede appetite, nutrient absorption, and metabolic equilibrium, consequently impacting patient prognosis. These effects could be compounded by the combined influences of hematological factors and physical measurements. Inflammatory states might contribute to the deterioration of a patient’s nutritional status, while malnutrition could intensify the inflammatory response, creating a cyclic detrimental loop. Additionally, the tumor itself might influence the patient’s immune and nutritional statuses through diverse pathways, further elevating the complexity. Nevertheless, despite observing associations between hematological and physical measurement indicators with prognosis in this study, further research is imperative to fully elucidate the precise underlying mechanisms. This could enhance the prognosis and quality of life for patients undergoing surgery for gastric or colorectal cancers.
To our knowledge, this is one of the largest studies on the association between the combination of hematological and physical measurement indicators and prognosis in patients undergoing surgery for gastric or colorectal cancers. Another strength of this study is that the best hematological and physical measurement indicators were screened. Although our study presents important findings, some limitations need to be recognized. First, our study design was a cross-sectional study, which limited our ability to establish a direct causal association in patients undergoing surgery for gastric or colorectal cancer. A more comprehensive exploration of causality would require further longitudinal studies or randomized controlled trials. Another limitation lies in the selection of prognostic indicators. Although we focused on several hematological and physical measurement indicators, we did not include C-reactive protein, skeletal muscle mass index, and waist-to-hip ratio due to its limited applicability in some patients. This may lead to the possibility that the optimal indicator is still yet to be identified. Furthermore, although baseline values of GNRI and CC showed prognostic significance, in the absence of repeated measurements during follow-up, we were unable to capture potential dynamic changes and their impact on clinical outcomes. Additionally, we did not carry out sample size calculations, however, considering that a sufficient number of people were included in this study, the results can be considered reliable. Finally, while we have adjusted for a range of variables, unmeasured or unknown factors may influence the observed associations.
Conclusion
In conclusion, this study reveals important factors affecting the prognosis of patients undergoing surgery for gastric or colon cancer. The combination of both hematological and physical measurement indicators, especially GNRI and CC, emerged as a strong predictor of OS. Low GNRI-CC were associated with a higher risk of death.
Supplemental Material
Supplemental Material - Geriatric Nutritional Risk Index Combined with Calf Circumference Can be a Good Predictor of Prognosis in Patients Undergoing Surgery for Gastric or Colorectal Cancer
Supplemental Material for Geriatric Nutritional Risk Index Combined with Calf Circumference Can be a Good Predictor of Prognosis in Patients Undergoing Surgery for Gastric or Colorectal Cancer by Xin Zheng, Jin-Yu Shi, Zi-wen Wang, Guo-Tian Ruan, Yi-Zhong Ge, Shi-Qi Lin, Chen-An Liu, Yue Chen, Hai-Lun Xie, Meng-Meng Song, Tong Liu, Ming Yang, Xiao-Yue Liu, Li Deng, Ming-Hua Cong, and Han-Ping Shi in Cancer Control
Footnotes
Acknowledgments
The authors thank the INSCOC project members for their substantial work on data collection and patient.
Author Contributions
Conceptualization, Xin Zheng, Jin-Yu Shi, Guo-Tian Ruan; methodology, Xin Zheng, Guo-Tian Ruan and Yi-Zhong Ge; software, Xin Zheng and Jin-Yu Shi; validation, Yi-Zhong Ge, Shi-Qi Lin and Chen-An Liu; formal analysis, Xin Zheng and Jin-Yu Shi and Zi-Wen Wang; investigation, Zi-Wen Wang, Hai-Lun Xie and Yue Chen; writing—original draft preparation, Xin Zheng, Jinyu Shi and Zi-Wen Wang; writing—review and editing, Zi-Wen Wang, Meng-Meng Song, Ming Yang and Xiao-Yue Liu; supervision, Li Deng Hanping Shi and Ming-Hua Cong; funding acquisition, Hanping Shi. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Program (2022YFC2009600 to Dr Hanping Shi), National Natural Science Foundation of China (32100939 to Z.W.), China National Postdoctoral Program for Innovative Talents (BX2021198 to Z.W.), China Postdoctoral Science Foundation (2022M712215 to Z.W.) and Beijing Postdoctoral Research Foundation (2022-ZZ-009 to Z.W.).
Ethical Statement
Data Availability Statement
All data needed to evaluate the conclusions in the paper are present in the paper and/or the Supplementary Materials. Data described in the manuscript, code book, and analytic code will be made available upon request pending application and approval.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.