
Abstract
In sub-Saharan Africa, cervical cancer is an intersecting epidemic with HIV and it is the second most common cause of cancer-related deaths in women. Therefore, this study was aimed to estimate the current status of the prevalence and associated factors of precancerous cervical lesions among HIV-positive women in sub-Saharan Africa. A systematic literature search was conducted from legitimate electronic databases, including MEDLINE (Ovid), PubMed, EMBASE (Ovid), Emcare (Ovid), CINAHL (EBSCOhost), Web of Science, Scopus, and PopLine and other gray literature including Google, Google Scholar, World Cat, ResearchGate, and Mednar. Data were extracted with a structured format prepared in Microsoft Excel. Each study was evaluated using the Joanna Briggs Institute critical appraisal tool for cross-sectional and cohort studies checklists. Accordingly, medium and high-quality studies were included in the review. Data synthesis and statistical analysis was conducted using OpenMeta and comprehensive meta-analysis version 2 software. The study protocol is registered on PROSPERO with ID: CRD42018114266. The pooled prevalence of precancerous cervical lesion among HIV-positive women in sub-Saharan Africa was 25.6% (95% confidence interval [CI]: 19.4%-31.8%). Having more than 2 lifetime sexual partners (odds ratio [OR]: 4.77; 95% CI: 1.35-16.93), having had a history of sexually transmitted infections (STIs; OR: 1.92; 95% CI: 1.03-3.57), having more than 2 births (OR: 1.84; 95% CI: 1.33-2.53), and CD4 count <200 cells/mm3 (OR: 1.765; 95% CI: 1.23-2.535) were significantly associated with precancerous cervical lesions. The prevalence of precancerous cervical lesion among HIV-positive women was high. One in 4 HIV-infected women suffers from precancerous cervical lesion. Lower CD4 cell count, STIs, multiple sexual partnering, and histories of multiple births and abortions were the foremost contributing factors for this burden. Precancerous cervical lesion could be reduced significantly if preventive and promotive measures are done on the associated factors.
Keywords
Background
Cervical cancer is the second most common cancer in women and the leading cause of gynecologic-related morbidity and mortality in developing countries. It is the cancer that arises from the cervix, which is caused by the abnormal growth of cells that have the ability to invade another part of the body. 1,2 Human papillomavirus (HPV) infection is a known cause of cervical, anal, vulvar, vaginal, and penile cancers as well as head and neck cancers. 3,4
Precancerous cervical lesions and cervical cancer are considered to be more aggravated and progress rapidly in immunocompromised patients. In sub-Saharan Africa, cervical cancer is an intersecting epidemic with HIV and is the second most common cause of cancer-related deaths in women. 5 The high prevalence of precancerous cervical lesion among both male and female partners infected with HIV contributes to transmission of both HIV and HPV. 6 Other risk factors include giving birth to many children, smoking, using oral contraceptives for a long time, low immune system, and first sexual intercourse initiation at an early age. 3
Human papillomavirus frequently causes precancerous cervical lesions and cancer in women; it can be screened for and treated easily if diagnosed early and before turning into an invasive cancer. 7 Screening for cervical cancer is a way to detect abnormal cervical cells, including precancerous cervical lesions, as well as early cervical cancers. However, most women in resource-poor countries do not have access to a screening program. Screening and diagnosis is a major challenge in developing countries. The actual coverage of cancer screening in developing countries is 19% compared to 63% in developed countries. Indeed, a screening rate of 1% or less was observed in countries such as Bangladesh, Ethiopia, and Myanmar. 3,8 Visual inspection with acetic acid or with Lugol iodine followed by biopsy and colposcopy examination of cancer cases was applied to improve the detection of precancerous cervical lesions. This technique has been applied in most developing countries, including Ethiopia. Such technique employs a rational approach to the screening and subsequent management of precancerous cervical lesion in HIV-infected women. 9
Methods
Study Protocol
The protocol for this systematic review and meta-analysis has been registered in the International Prospective Register of Systematic Reviews (PROSPERO) with ID: CRD42018114266, and the published methodology is available at http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42018114266.
The methodology of this systematic review and meta-analysis was developed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement 2009 Checklist 10 (see Additional File 1 in supplemental material).
Sources of Studies and Searching Strategies
The authors conducted systematic literature searches from the legitimate major electronic databases, including MEDLINE (Ovid), PubMed, EMBASE (Ovid), Emcare (Ovid), CINAHL (EBSCOhost), Web of Science, Scopus, and PopLine, and other literature sources, including Google, Google Scholar, World Cat, ResearchGate, and Mednar. In addition, the hand (manual) search of various repositories was accomplished in order to retrieve unpublished studies and gray literatures. We used MeSH terms, key terms, and search strings by extracting from the review questions for all the searches.
Advanced search strategies were applied in major databases to retrieve relevant findings closely related to the prevalence of and associated factors with precancerous cervical lesions among HIV-positive women. The search was conducted with the aid of carefully selected keywords and indexing terms. The search strategy included “precancerous [MeSH] AND “cervical lesion” OR Cervical Intraepithelial Neoplasia [MeSH], “HIV-positive” OR HIV Seropositivity [MeSH] AND women [MeSH], AND Africa south of Sahara [MeSH]. Boolean operators (AND, OR), truncation, and the MeSH terms were used appropriately for the systematic identification of records for the research question. Both authors constructed the search strings (F.W. and T.W.). In addition, the investigators consulted an information specialist on the appropriateness of search strings and applied them according to the specific requirement of the databases. Details regarding the searching strategies are included in an additional file (see Additional File 2). The overall search result was compiled using EndNote X8 citation manager software. 11
Eligibility Criteria
The investigators included observational studies (cross-sectional and cohort) that have been conducted at a facility setting in different parts of Sub-Saharan Africa on the prevalence of and factors associated with precancerous cervical lesions among HIV-positive women. In addition, studies that were published and were accessible until November 10, 2018, and written in English were eligible for this systematic review and meta-analysis. Articles with irretrievable full texts (after requesting full texts from the corresponding authors via e-mail and/or ResearchGate), records with unrelated outcome measures, and articles with missing or insufficient outcomes were excluded. Reviews, commentaries, editorial, case series/report, and patient stories were also excluded from the systematic review.
Selection Process of Studies
All search results (records) were exported to the EndNote X8 citation manager and duplicated studies were removed. Later, articles were screened through a careful reading of the title and abstract. The 2 authors screened and evaluated the studies independently. The titles and abstracts of studies that clearly mentioned the outcomes of the review were considered for further evaluation to be included in the systematic review and meta-analysis. Then the full-texts of the retained studies were further evaluated based on quality of their objective, methods, participants/population, and key findings. The authors (F.W. and T.W.) independently evaluated the quality of the studies included against the Joanna Briggs Institute (JBI) critical appraisal tool for cross-sectional and cohort studies checklists. In case of disagreement between quality assessment results of the 2 authors, the differences were resolved by consensus for the inclusion. The overall study selection process is presented using the PRISMA statement flow diagram 12 (Figure 1).

Schematic presentation of the flow of studies selection process.
Data Extraction and Recording
Findings from the selected studies were extracted and stored using data extraction template prepared on Microsoft Word 2016 and then to Excel (Table 1), followed by extraction of important data based on study characteristics (country, first author, year of publication, study design, patient characteristics, and outcome of interest) by the 2 authors independently. For the prevalence of a precancerous cervical lesion, we used unconverted proportional data to calculate the proportion/prevalence of precancerous cervical lesion among HIV-positive women in percentage using OpenMeta software. Most of the associated factors of the precancerous cervical lesion summary measures were done by the pooled odds ratio (OR) using CMA software.
Summary of Researches Including on the Review.

Abbreviations: ART, antiretroviral therapy; AOR, adjusted odds ratio; CI, confidence interval; FGD, flue-gas desulfurization; HAART, highly active antiretroviral therapy; HPV, human papillomavirus; NA, not applicable; OCP, oral contraceptive use; OR, odds ratio; PCCL, precancerous cervical lesion; RR, relative risk; STD, sexually transmitted disease; VIA, visual inspection with acetic acid.
Critical Appraisal of Studies
The methodological reputability and quality of the findings of the included studies were critically evaluated using the quality assessment tool for observational studies (cross-sectional and cohort studies) developed by the JBI. 27 The 2 authors (F.W. and T.W.) independently evaluated the quality of the studies. The mean score of the 2 authors was taken for a final decision. The differences in the inclusion of the studies were resolved by consensus. The cross-sectional studies checklist was graded out of 8 points, and the cohort studies checklist was graded out of 11 points. The included studies were evaluated against each indicator of the tool and categorized as high, moderate, and low quality. High-quality scores were above 80%, moderate quality between 60% and 80%, and low-quality scores below 60%. Studies with a score greater than or equal to 60% were included. This critical appraisal was conducted to assess the internal validity (systematic error) and external validity (generalizability) of studies and to reduce the risk of biases.
Risk of Bias (Quality) Assessment
The methodological reputability and quality of the findings of the included studies was critically evaluated using the quality assessment tool for observational studies (cross-sectional and cohort studies) developed by the JBI. 27 To ensure quality, the investigators conducted search for studies using a comprehensive strategy (electronic databases and manual search), which included published and/or unpublished, and facility and/or community-based studies. To minimize bias, the 2 authors independently screened the studies using clear objective eligibility criteria. Publication bias was explored using visual inspection of the funnel plot. Additionally, Egger regression test 28 was carried out to check the statistical symmetry of the funnel plot.
Strategy for Data Synthesis
The findings of the included studies were first presented using a narrative synthesis. Study descriptions and summary (author year, country, aim, design and population, sample size, and key findings) were compiled using Microsoft Word. The raw numerical data (precancerous cervical lesion prevalence [n] and total sample size [N]) from each study were extracted and recorded on a Microsoft word, then exported to an Excel Spreadsheet. The authors conducted data synthesis and statistical analysis. Meta-analysis was conducted usingOpenMeta and CMA version 2 softwares to compute the pooled prevalence and factors associated with the precancerous cervical lesion. A meta-analysis of observational studies was conducted, based on recommendations made by Higgins and Thompson (an I 2 of 75/100%, suggesting considerable heterogeneity). In the meantime, heterogeneity between the included studies was examined using the I 2 statistic. 13 Therefore, the presence of heterogeneity between studies was assumed if the I 2 statistic was greater than 75%. A random-effects model was used to determine the pooled prevalence and associated factors with precancerous cervical lesions.
Results
Study Descriptions
A total of 331 articles were identified through the major medical and health electronic databases and other relevant sources. From all the studies identified, 120 articles were removed due to duplication and 211 studies were reserved for further screening. Of these, 179 were excluded after screening by titles and abstracts. Of the 32 remaining articles, 18 studies were excluded due to inconsistency with inclusion criteria set for the review. Ultimately, 14 studies fulfilled the eligibility criteria were included in the systematic review and meta-analysis. General characteristics and descriptions of the studies selected for the meta-analysis are outlined in Table 1.
Prevalence of Precancerous Cervical Lesion Among HIV-Positive Women in Sub-Saharan Africa
Among HIV-positive women, precancerous cervical lesions and cervical tissue neoplasm in the cervical area were prevalent conditions in Sub-Saharan Africa. The included studies in this systematic review and meta-analysis showed that the prevalence of precancerous cervical lesions ranged from 2.9% to 76%. 14 –26,29,30 Furthermore, the pooled prevalence of precancerous cervical lesion among the HIV-positive women in Sub-Saharan Africa was 25.6% (95% confidence interval [CI], 19.4%-31.8%) (Figure 2). Risk of bias/publication bias was analyzed for the included studies. Accordingly, the funnel plot and Egger regression test result showed that the intercept (B 0) was −0.09819 (95% CI, −11.16468 to 10.96831), with t = 0.01933, df = 12. The 1-tailed P value (recommended) obtained was 0.49245, while the 2-tailed P value was 0.98.

The pooled prevalence of precancerous cervical lesion among HIV-positive women in sub-Saharan Africa, 2018 (n = 14).
Factors Associated With Precancerous Cervical Lesion
According to 5 of the studies that were included, having had multiple sexual partners during one’s lifetime was the most important predisposing factor for developing precancerous cervical lesions, tissue change, and cell growth in the cervix of HIV-positive women. The HIV-positive women who had more than 2 lifetime sexual partner were prone to the precancerous cervical lesion and tissue change in the cervical area. 14,16,18,19,30 Similarly, those HIV-positive women who were divorced and widowed and who were commercial sex workers were also at risk of developing precancerous cervical lesion and cervical tissue neoplasm. 19,26,30 The HIV-positive women who had more than 2 sexual partners in their lifetime were 4.77 times more likely to be at risk of developing precancerous cervical lesions than those women who had a history of less than 2 sexual partners (OR, 4.77; 95% CI, 1.35-16.93). The heterogeneity test indicated I 2 = 98%; hence, the random-effect model was employed for the analysis. To reduce heterogeneity, the random and fixed-effect model was employed interchangeably for analysis and a sensitivity analysis was done, but no change was seen in the overall OR and heterogeneity (Figure 3).

Association between having more than 2 lifetime sexual partner and precancerous cervical lesion among HIV-positive women in sub-Saharan Africa, 2018 (n = 5).
Six observational studies reported that any condition which was responsible for the formation of ulcer, lesion, inflammation, and any other abnormalities to the cervix, vagina, genitalia, and pelvis as a whole was a very critical predisposing factor for the development of precancerous cervical lesion. Sexually transmitted infection (STIs) play a key role, mainly those causing recurrent ulcerative lesions. 14-16,18,24,25,30 Similarly, in this analysis, HIV-positive women who had a history of STIs were 1.92 times more likely to develop precancerous cervical lesion compared with women without such history (OR, 1.92; 95% CI, 1.034-3.570). Heterogeneity test indicated I 2 = 80.29%; hence, the random-effect model was assumed in the analysis. Sensitivity analysis was conducted but did not bring about any significant change in the overall summary results of OR and reduction of I 2 value (Figure 4).

Association between sexually transmitted infections (STIs) and precancerous cervical lesion among HIV-positive women in sub-Saharan Africa, 2018 (n = 6).
Three studies reported that HIV-positive women with a history of having more than 2 births were at risk of developing precancerous cervical lesion and adaptive tissue changes. 18,26, 30 Similarly, having had recurrent abortions also had a persuasive effect for precancerous cervical lesion development. 26,30 The meta-analysis results of the review showed that there was a significant association between parity and precancerous cervical lesion (OR, 1.84; 95% CI, 1.333-2.53). The HIV-positive women with a history of having more than 2 births were 1.84 times more likely to be at risk of developing precancerous cervical lesion compared with those of who had 2 or fewer births. Heterogeneity test indicated I 2 = 80.98%; hence, the fixed-effect model was employed for analysis. In addition, a sensitivity analysis was done, and no change was illustrious in the overall OR (Figure 5).
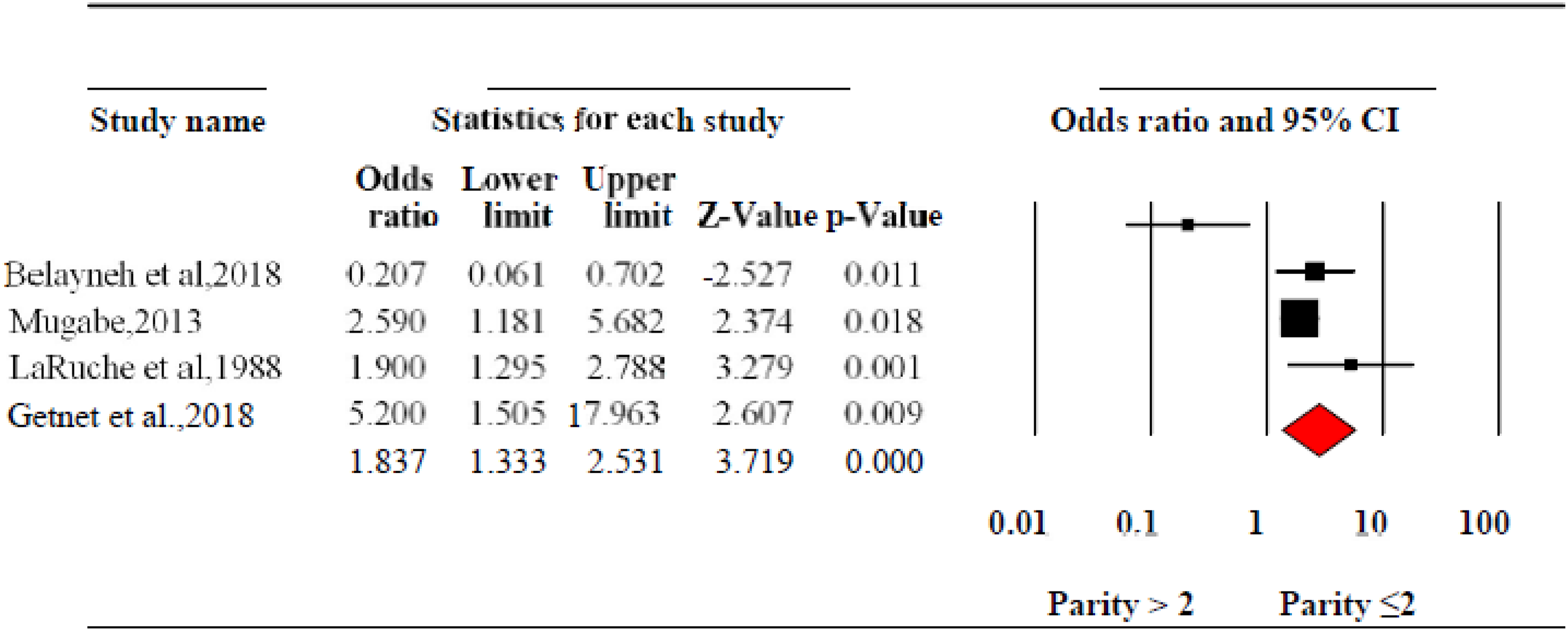
Association between parity with precancerous cervical lesion among HIV-positive women in sub-Saharan Africa, 2018 (n = 4).
CD4 cell count was an additional factor associated with the precancerous cervical lesion. Since the level of the CD4 count is the vital indicator of immune status, having a better immune status helps protect women from precancerous cervical lesions. 17,1 9,23-25 The pooled OR revealed that there was a significant association between CD4 count and precancerous cervical lesion among HIV-positive women (OR, 1.75; 95% CI, 1.22-2.517). The HIV-positive women who had a CD4 count of <200 cells/mm3 were 1.75 times more prone to precancerous cervical lesions than those who had a CD4 count of >200 cells/mm3. The heterogeneity test indicated I 2 = 94.32%; hence, the fixed-effect model was employed for analysis. In addition, a sensitivity analysis was done, and no change was seen in the overall OR and heterogeneity (Figure 6).

Association between CD4 count and precancerous cervical lesion among HIV-positive women in Africa, 2018 (n = 3).
Starting and adhering to antiretroviral therapy (ART) was among the factors that prevents the occurrence of the precancerous cervical lesion and tissue change, since it boosts immunity, improves clinical condition, and reduces viral load. 23,26 In contrast, some studies reported that being on ART was the risk for the development of precancerous lesion. 14,20 However, according to the meta-analysis result of this review, there was no significant difference between whether or not someone was on highly active antiretroviral therapy (OR, 0.544; 95% CI, 0.106-2.79; Figure 7).

Association between being on highly active antiretroviral therapy (HAART) and precancerous cervical lesion among HIV-positive women in sub-Saharan Africa, 2018 (n = 3).
Discussion
This review was aimed to summarize the findings of primary studies that generate abridged evidence on the level of precancerous cervical lesion among HIV-positive women and its associated factors. A total of 14 studies that were conducted in Sub-Saharan Africa region were identified and included. 14 -26,29,30
The investigators used extensive and comprehensive search strategies from multiple databases and included published and unpublished studies and gray literature. Studies were evaluated for the methodological quality of studies using a JBI critical appraisal tool for cross-sectional and cohort studies checklists. Although the literature search assessed all related studies within the desired scope, it is possible that some relevant publications were missed, for example, some studies which were not written in English language; studies could not be accessed in full text were excluded. This was after failing e-mail communication with the author. In addition, it is hard to conclude that the studies were homogenous. The generalizability of the study might not be in full confidence because the selected study was not from all regions of Sub-Saharan Africa. Publication bias was also observed for some studies (Figure 8).

Publication bias of the studies (n = 14).
The prevalence of precancerous cervical lesion and tissue change was very high among HIV-positive women. Hence, almost more than one-fourth (25.6%) of HIV-positive women identified with the precancerous cervical lesions. This finding strongly showed that being HIV-positive means at risk for developing a precancerous cervical lesion. Most of the included studies to this review reported that and our finding confirmed that CD4 count >200 cells/mm3 was important factor in preventing precancerous cervical lesion. This study was consistent with other systematic review and meta-analysis conducted elsewhere. 31,32 In addition, those preventable factors, having multiple sexual partners and multiple abortion and birth, were seeming to be the key predisposing factors for the precancerous cervical lesion. Nonetheless, some studies reported that age, first sex less than 18 years, and longer use of hormonal contraceptive have an impact in the development of precancerous cervical lesion; the meta-analysis finding of this study confirms that it has no any associations. Although the aforementioned factors were a crucial element of the precancerous cervical lesion, its preventive measures were overlooked by the women living with HIV/AIDS and the country’s government of Sub-Saharan Africa.
Conclusion
The prevalence of precancerous cervical lesion among HIV-positive women was high. Having had multiple sexual partners, STIs, CD4 cell count, multiple births, and abortions were among the foremost contributing factors. Despite this reality, peoples are not paying enough attention to the prevention of precancerous cervical lesions. Precancerous cervical lesion could be reduced significantly if preventive and promotive measures are carried out on the possible contributing factors. Hence, it is suggested that key stakeholders should design interventions to avert these factors such as early screening for all HIV-positive women, vaccination for HPV, and work on behavioral change counseling and support.
Future Directions
Cervical cancer is one of the areas that need advanced research, mainly in the developing world. To advance the field, researchers need to focus to carry out feasibility studies for implementation of an intervention to tackle and prevent the factors contributing to its occurrence. Furthermore, the finding gives an insight for policymakers, program planners, researchers, clinician, and other key stakeholders to implement an intervention that prevents cancer among HIV-positive women in Sub-Saharan African countries.
Supplemental Material
Supplemental Material, Additional_file_1_PRISMA_checklist - Precancerous Cervical Lesion Among HIV-Positive Women in Sub-Saharan Africa: A Systematic Review and Meta-Analysis
Supplemental Material, Additional_file_1_PRISMA_checklist for Precancerous Cervical Lesion Among HIV-Positive Women in Sub-Saharan Africa: A Systematic Review and Meta-Analysis by Fitsum Weldegebreal and Teshager Worku in Cancer Control
Footnotes
Author’s Note
Both authors conceived and designed the study, collected scientific literature, critically appraised individual articles for inclusion, analyzed and interpreted the findings, drafted the manuscript, and prepared the final version for publication. Both authors read and approved the final version.
Acknowledgments
The authors thank Medical Laboratory Science and School of Nursing and Midwifery staffs who technically supported us for the realization of this article. The authors also thank Lauren Ebay for editing the English language.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.