
Abstract
The extent to which prostate cancer (PCa) pathology interacts with health insurance to predict PCa outcomes remains unclear. This study will assess the overall association of health insurance on PCa disease control and analyze its interrelationship PCa pathology. A total of 674 PCa patients, treated with prostatectomy from 1987 to 2015, were included in the study. Freedom from biochemical failure (FFbF) was used as a measure of PCa disease control. Methods of categorical and survival analysis were used to analyze the relationships between health insurance, PCa pathology, and FFbF. A total of 63.3% patients were privately insured, 27.1% were publicly insured, and 9.5% were uninsured. In a multivariable model, privately (hazard ratio [HR] = 0.64, 95% confidence interval [CI]: 0.42-0.97, P = .03) and publicly (HR = 0.65, 95% CI: 0.41-1.04, P = .07) insured patients showed improvement in FFbF compared to uninsured patients. The association of health insurance was significantly stronger for the patients with pathologically low grade PCa (pathologic Gleason Score 3+3 & preoperative prostate-specific antigen ≤10 ng/mL), likelihood ratio P = .009. Privately (HR = 0.22, 95% CI: 0.10-0.46) or publicly (HR = 0.26, 95% CI: 0.11-0.60) insured patients with low grade PCa demonstrated favorable association with FFbF. Patients with private and public insurance were more likely to experience favorable treatment. The association of health insurance on PCa disease control is significantly stronger among patients with pathologically low grade PCa. This study identifies health insurance status as pretreatment surrogate for PCa disease control.
Keywords
Introduction
Health insurance is closely interrelated with the socioeconomic status (SES) of patients and has a profound effect on overall patient health. 1 In the United States, 91.2% of the population had health insurance coverage in 2016 (private or public insurance). 2 The proportion of uninsured individuals in the United States has been on the decline since the enactment of the Affordable Care Act in March 2010. 2,3 However, with the plausible revision of existing health-care and tax policies, the number of uninsured individuals in the coming years may increase. 4 In light of the current uncertainty of the future of accessible health care in the United States, understanding the role of health insurance status and its implications on disease control in prostate cancer (PCa) remains exigent.
Heterogeneous effects of health insurance on clinical outcomes has been widely reported in various types of cancers, 5 including PCa. Prostate cancer is one of the most prevalent noncutaneous cancer among men and is the second leading cause of cancer-related death. 6 In PCa, studies have indicated positive treatment outcomes associated with private health insurance compared to those with public health insurance or those that were uninsured. 7 -9 In a study of 4000 patients undergoing radical prostatectomy, the authors reported a significant association between private insurance and favorable clinical characteristics resulting in improved PCa outcomes. 10 A recent study by Ellis and team reported an increased likelihood of cancer screening among privately insured patients, 5 leading to early detection of cancer in this cohort. Probable reasons for the differences in clinical outcomes in PCa are multifactorial, ranging from barriers to access of regular medical evaluation, lack of cancer screening, lifestyle-related factors, and delays in the initiation of definitive treatment. 5,11 -14
In this study, we investigated the association of health insurance status on PCa disease control defined as freedom from biochemical failure (FFbF). Most studies in the current literature evaluated the role of type of insurance on PCa outcomes without significant emphasis to account for PCa pathology. Given that outcomes in PCa are highly dependent on the aggressiveness of the disease, 15 -18 PCa progression may be driven concurrently by nonmodifiable characteristics such as advanced pathologic Gleason score (GS) or presence of adverse pathologic features at diagnosis 19,20 alongside SES indicators such as health insurance status. Therefore, the nature of the association between health insurance and PCa outcomes with careful statistical consideration of joint relationships with PCa aggressiveness warrants investigation. In this study, we leveraged the availability of FFbF—identified through rigorous review of well-annotated medical charts available through one of the Moffitt Cancer Center (MCC) data sources—and used it as a primary end point, compared to traditionally used outcomes such as overall survival. This study examined the critical association of type of health insurance on PCa disease control and the extent to which this relation is influenced by PCa pathology.
Materials and Methods
Data Source
This retrospective cohort study included 674 newly diagnosed patients with nonmetastatic PCa who had a prostatectomy as first course of treatment between 1987 and 2015 and have complete clinicopathologic and follow-up information, identified through the Health Research and Informatics platform at MCC. This study was reviewed and approved by the Advarra prior to initiation (Approval #00000971). A waiver of consent was provided at the time of review, and no additional consent was obtained for the conduct of this retrospective study.
Baseline Covariate Variables
Table 1 provides detailed information on all the covariates used in the study. Patient information on primary payer at the time of initial diagnosis and treatment was recorded using the “Primary Payer at Diagnosis” and “Primary Payer at Presentation” variable from our institutional cancer registry. With the utilization of detailed payer information from 2 unique data elements, we potentially limited any migration between insurance categories from the time of diagnosis to the time when patients presented for treatment. Upon initial review, 5 major categories of types of insurance were identified: private insurance (n = 427), Medicare only (n = 66), Medicare with supplemental private coverage (n = 106), Medicaid (n = 11), and uninsured (n = 64). All patients with Medicare alone and Medicare with other supplemental coverage were combined and classified as public insurance. Although the eligibility criteria for Medicaid are different from Medicare, both Medicaid (jointly funded by state and federal government) and Medicare (funded by federal government) remain major government-run insurance programs in the United States. 21 As such, they were grouped as public health insurance for the analysis.
Clinicopathologic and Demographic Characteristics by Health Insurance Status.

Abbreviations: AAM, African American; AJCC, American joint committee on cancer; APF, adverse pathologic features; EAM, European American; ECE, extracapsular extension; LNI, lymph node invasion; pGS, pathologic Gleason score; PSA, prostate specific antigen; SM, surgical margins; SVI, seminal vesical involvement; TTrP, time to receive prostatectomy.
aIndicates Fisher exact P value.
bAPF is calculated by using pathologic indicators of prostatectomy (extracapsular extension, surgical margins, seminal vesicle involvement, and lymph node invasion).
Time to receive prostatectomy (TTrP), race, age at diagnosis, date of diagnosis, date of prostatectomy, pathologic T stage (pT), GS, extracapsular extension, lymph node invasion, seminal vesicle invasion, surgical margins, preoperative prostate-specific antigen (iPSA), and postsurgery follow-up PSA were recorded using electronic patient records. We used Epstein criteria of “Gleason Grading” to determine PCa grade. Patients with Epstein group grade 1 (GS 3+3) were considered as low-grade Pca. 15 Additionally, to limit the possibility of advanced disease, we further excluded patients with iPSA > 10 ng/mL, thus making this group a truly low-grade cohort. 22 Therefore, Epstein group grade 1 (GS 3+3) with iPSA ≤ 10 ng/mL were classified as low grade, while patients with Epstein group grade 1 (GS 3+3) and PSA > 10 ng/mL or Epstein group grades 2 to 5 (GS ≥ 3+4) with any iPSA value were categorized as moderate- to high-grade Pca. 15,19 Based on the criteria, 250 patients were identified as low grade while the remaining 424 patients were classified as moderate to high grade. Pathologic GS instead of biopsy-based GS was used to define PCa grade to avoid the issue of GS upgrading following prostatectomy. 23 In addition, we also included information on patient’s marital status, obesity, and history of tobacco exposure in the analysis.
Outcome
Prostrate cancer disease control, defined as early treatment failure after prostatectomy, was used as the primary outcome. Freedom from biochemical failure was used as a measure of PCa disease control and was calculated as the difference between the date of prostatectomy (index date) and the date of PSA failure (biochemical failure). PSA failure was determined by clinician-documented single PSA ≥ 0.2 ng/mL or 2 consecutive PSA values of 0.2 ng/mL. 20 If follow-up data were not available, for patients who did not experience biochemical failure, their last date of contact was used as a censor date.
Statistical Analysis
Different subgroups of health insurance categories were analyzed using χ2, Fisher exact test, and analysis of variance. Kaplan-Meier (KM) analysis was used to calculate rates of FFbF within the strata of various health insurance categories. Univariable and multivariable Cox proportional hazard (CPH) models were used to estimate the relative rates of biochemical failure using clinicopathological and demographic variables. Patients with aggressive disease, defined as high PCa grade or presence of multiple adverse pathologic features, are at increased risk of treatment failure 19,20 ; therefore, multivariable Cox models adjusted for PCa grade and adverse pathologic features categories along with other demographic variables, hereinafter referred as “Multivariable Model.” Furthermore, interaction of PCa grade and health insurance status was also analyzed in a separate interaction model, hereinafter referred as “Interaction Model.” A likelihood ratio test P value was used to determine interaction model significance. Given the very small number of patients with Medicaid (n = 11), these patients were grouped as public insurance along with Medicare. To ensure that the combination of Medicare and Medicaid did not impact our model estimates, we also conducted sensitivity analysis with and without Medicaid in the public insurance group. Finally, all the variables used in the multivariate cox model were assessed for their time-varying effect to ensure that proportionality assumption holds true. We utilized “assess” and “resample” options provided in Proc Phreg procedure in SAS 24 to calculate cumulative martingale residuals (difference between expected and observed event in the model) by simulating the data over 1000 time. Associated P value of the residuals for each variables was generated. None of the variables used in the model showed a deviation from proportionality assumption with P value >.05.
In addition to pathologic characteristics, multivariable models were also adjusted for the variables that were either known to be associated with PCa outcomes (ie, adverse pathologic features, GS, and race) 19 or if they were associated with the outcome in a univariable model such as TTrP. 25 Both unadjusted HRs (UHR) and adjusted HR (AHR) along with the 95% confidence intervals (CI) were reported. P value ≤.05 was considered statistically significant. 20
Results
A total of 674 histologically confirmed patients with PCa having a median follow-up time of 60 months were analyzed. Among the study cohort, 63.3% (n = 427) were privately insured, 27.1% (n = 183) were publicly insured, and the remaining 9.5% (n = 64) were uninsured. In categorical analysis, comparing different insurance categories and clinicopathologic/demographic characteristics, uninsured patients were more likely to have advanced pathologic stage (pT3; 26.5%) compared to those with private (15%) and public insurance (19.1%; P = .02). Health insurance categories did not differ significantly on other comparable clinicopathologic and baseline characteristics in the analysis (Table 1).
Predictors for FFbF
Over the median follow-up of 60 months, 180 patients failed initial treatment as they had detectable PSA after prostatectomy. In the KM analysis, the 5-year FFbF rate for private, public, and uninsured patients was 79% (95% CI: 74%-83%), 74% (95% CI: 67%-80%), and 62% (95% CI: 49%-73%), respectively, log-rank P = .01 (Figure 1A). In univariable CPH models, delay in TTrP (UHR = 1.08, 95% CI: 1.03-1.13, P < .001), moderate- to high-grade PCa (UHR = 2.13, 95% CI: 1.52-2.97, P < .001), and adverse pathologic features were significantly associated with high risk of biochemical failure (Table 2). None of the other baseline characteristics were associated with PCa disease control. In the univariate model (Table 2), patients with private insurance showed improved FFbF (UHR = 0.54; 95% CI: 0.36-0.82, P = .004) followed by those who had public insurance (UHR = 0.64; 95% CI: 0.40-1.01, P = .05) when compared to uninsured patients. Furthermore, in the multivariable model (Table 2), private insurance remained a strong predictor for the improved FFbF compared to uninsured patients (AHR = 0.64; 95% CI: 0.42-0.97, P = .03). In a similar model, public insurance also showed a protective association with FFbF (AHR = 0.65; 95% CI: 0.41-1.04, P = .07).There was no difference in the risk estimates in sensitivity analysis with or without Medicaid.
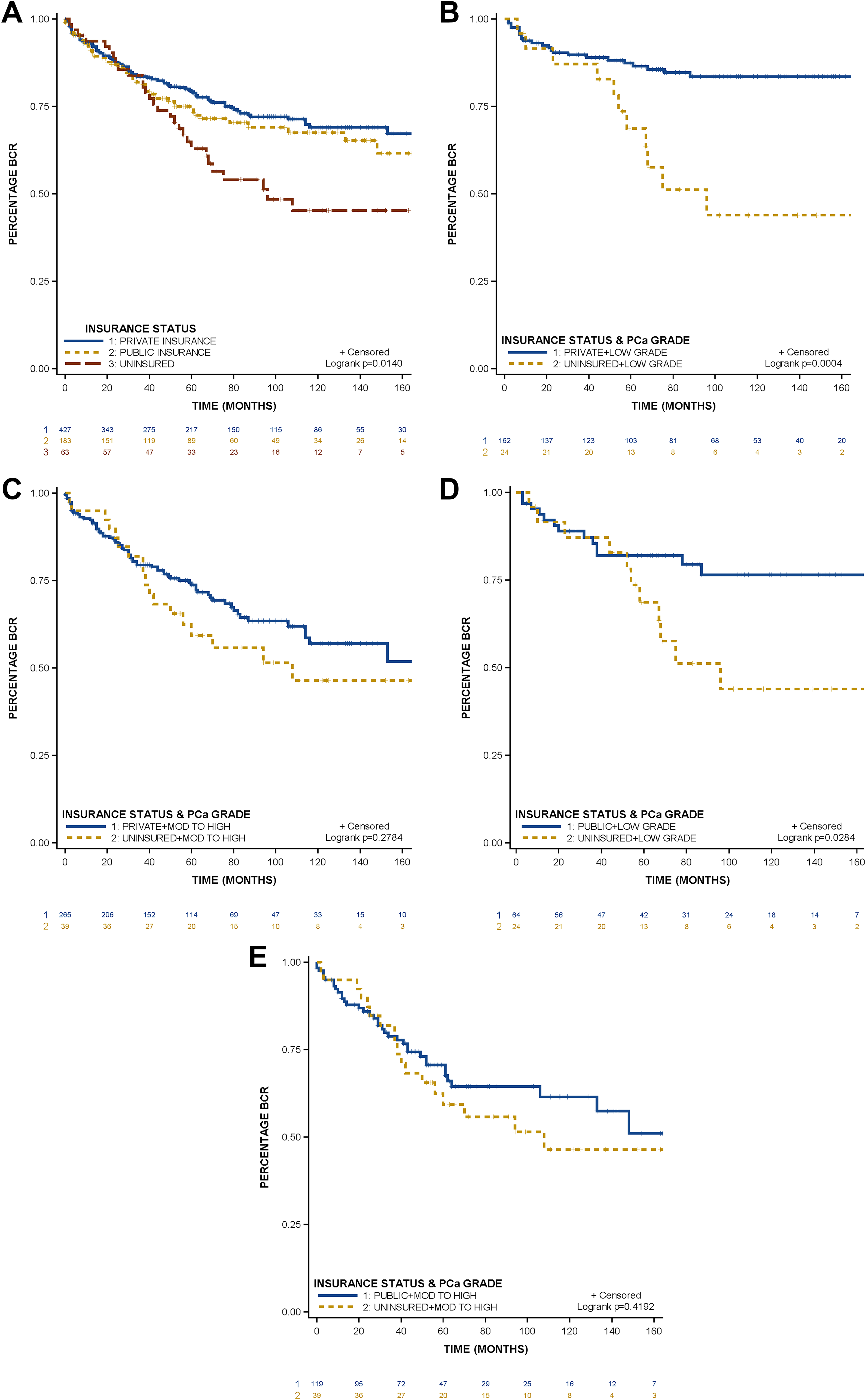
Kaplan-Meier plots. A, Difference in freedom from biochemical failure within the strata of health insurance status. B and 1D, Difference in freedom from biochemical failure for low-grade PCa with private and public health insurance compared to uninsured, respectively. C and E, Difference in freedom from biochemical failure for moderate- to high-grade PCa, with private and public health insurance compared to uninsured, respectively. PCa indicates prostate cancer.
Univariate and Multivariate Model to Predict the Risk of Biochemical Failure for Health Insurance Status Along With Clinicopathologic and Baseline Variables.

Abbreviations: AAM, African American; APF, adverse pathologic features; CAPRAS, Cancer of the Prostate Risk Assessment; CI, confidence interval; HR, hazard ratio; PCa, prostate cancer.
aMultivariate model is adjusted for the variables that were associated with FFBF in univariate model except race. Given the close association of race and PCa outcomes from the literature, race was included in the multivariate model.
bAPF is calculated by using pathologic indicators of prostatectomy (extracapsular extension, surgical margins, seminal vesicle involvement, and lymph node invasion).
cEffects associated with the unknown categories are not shown.
Health insurance status and PCa grade
In PCa grade–stratified KM analysis, patients with pathologically low-grade PCa having private and public insurance showed significant improvement in FFbF, compared to uninsured patients. In contrast, association between health insurance status and FFbF was not significant for moderate- to high-grade PCa. In multivariable interaction model, the interaction between PCa grade and health insurance categories adjusted for concomitant variables was significantly predictive for FFbF (likelihood ratio P = .009). Compared to the uninsured, privately insured patients with low-grade disease had a strong protective association with the risk of biochemical failure (HR = 0.22; 95% CI: 0.11-0.47). Likewise, publicly insured patients (HR = 0.26; 95% CI: 0.11-0.59) also showed a beneficial effect on FFbF. Conversely, among the patients with moderate- to high-grade PCa, insurance categories did not show significant association with FFbF (Table 3).
Multivariable Interaction Model Predicting the Risk of Biochemical Failure.

Abbreviations: CI, confidence interval; HR, hazard ratio; PCa, prostate cancer.
aInteraction model is adjusted for time to receive prostatectomy, adverse pathologic features, and race.
bLikelihood ratio P value.
Discussion
This study emphasizes the importance of having health insurance and the ramifications of being uninsured. The results of this study suggest that health insurance status remains an important predictor for PCa disease control after prostatectomy. Patients with private and public insurance coverage have a significantly lower risk of treatment failure compared to the uninsured. Furthermore, health insurance status was a critical predictor of treatment success in the study population with pathologically low-grade PCa.
In our study, a large proportion of uninsured patients had pathologically advanced-stage (pT3) PCa. These results confirm the findings of Fossati and colleagues who reported an increased likelihood of high-risk disease among uninsured patients with PCa. 9 Our analysis demonstrated notable protective effects associated with private and public health insurance over uninsured. Five-year FFbF rate after prostatectomy was significantly higher for the patients with private and public insurance compared to uninsured. Additionally, in a PCa grade-adjusted model (Table 2) along with other clinicopathologic and demographic indicators, patients with private and public insurance showed treatment benefits compared to the uninsured. Our results were similar to the study by Gallina et al, which demonstrated lower rates of biochemical recurrence among privately insured patients. 10 Similarly, Trinh and colleagues also reported improved outcomes after prostatectomy among privately insured patients. 8 Furthermore, the observed benefit in PCa disease control among the public health insurance group further underscores an important hypothesis that having some form of insurance coverage is better than being uninsured. In a population-based study by Ellis and colleagues, authors showed improved survival for patients with PCa having public insurance over those without any coverage, which substantiates the observed benefits of public insurance over uninsured in our study. 5
Health insurance status and PCa aggressiveness
Given the close association of PCa aggressiveness and outcomes in PCa, we analyzed the potential interaction of PCa grade with health insurance status. In the PCa grade-stratified KM analysis, we observed significant improvement in FFbF for private and public insurance in patients with low-grade PCa. Additionally, we performed a multivariate interaction model to assess the association of health insurance with FFbF within the strata of Gleason Grade (Table 3). Significance of the cross product term of health insurance and Gleason grade was established using likelihood ratio P value. In the interaction model, patients with pathologically confirmed low-grade PCa with private and public insurance had significantly lower risk of treatment failure compared to uninsured patients. This finding highlights the joint association of private insurance and low-grade PCa in achieving favorable treatment outcomes. In a population-based study, Rosenberg and colleagues reported a significantly high risk of cancer mortality among patients with nonprivate insurance and early-stage cancer. 26 Although the outcome investigated by Rosenberg et al differs from the outcome we evaluated, the results from their study correlate with our finding that insurance coverage in early PCa diagnosis may offer outcome benefits compared to uninsured patients. Our observed findings suggest that, in absence of health insurance, patients are at more disadvantage even with low-grade PCa and therefore emphasizes the role of SES indicators as modifiable risk factors for poor oncologic outcomes in early phase of PCa.
Improved outcomes among privately insured individuals over uninsured are primarily considered in relation to increased access to preventive care services such as cancer screening, early diagnosis, and routine medical care. 11 In addition to access to care, the literature has also shown that certain lifestyle factors may influence PCa outcomes. 13 In a study by Bittoni et al, authors reported that patients with private insurance are more likely to make healthy lifestyle decisions including increased physical activity, healthy diet, and lower propensity for tobacco use. 13 Recently, studies have also linked lifestyle and behavioral factors with poor oncologic outcomes including Pca. 5,13,14,27 Although not significant, in our study, a large proportion of uninsured men had history of tobacco exposure (Table 1). These findings may explain the observed potential benefits among patients with early-stage or less advance PCa in our study.
The major strength of this study is the inclusion of data with long-term follow-up along with extensive clinicopathologic and socioeconomic information. Also, our study had a significant proportion of African American patients (30% of the study population), who are traditionally underrepresented, making our results more generalizable to ethnic minorities. In addition, most contemporary studies have used survival (overall or PCa specific mortality) as an end point to study the effect of health insurance status on PCa disease control. 5,7,28 However, survival alone may not adequately capture the possible heterogeneity in PCa burden endured by patients. Instead, imminent economic and psychological burdens resulting from early treatment failure may serve as a strong surrogate for quality of life. Treatment failure in PCa prompts more outpatient visits for further evaluation and medical procedures and additional salvage treatments, 29,30 leading to increased burden on patients. 31 Our results are directly linked with quality-of-life issues that patients are likely to encounter. Although there are studies that have explored the association between insurance and outcomes, there are no studies that have evaluated this association in context of PCa tumor grade. Our results provide a unique perspective of health insurance as we were able demonstrate that PCa pathology can significantly impact the association between insurance and outcome.
Our results can be vital for the clinicians as they can consider insurance status as a viable prognostic indicator for low-grade prostate tumors. Although end points in cancer are driven by a complex set of clinical and pathological factors, the role of health insurance coverage in achieving desirable treatment outcomes should not be overlooked. Our results necessitate the need to ensure broader and more affordable health insurance coverage to all patients, especially at-risk populations (underinsured and those with low SES), to mitigate the disparities in access to care.
There are a few limitations associated with this study. First, health insurance status was the sole indicator used as a measure of the SES of the patients in the multivariable model. Absence of patient-level income information limited our ability to adequately account for patient’s financial status before they received surgery. Second, our study included data spanning more than 25 years, and therefore, any clinical changes in PCa pathology including revision of GS definitions over the years have the potential to introduce misclassification bias in the determination of PCa grade. Furthermore, when stratified by tumor grade, the number of cases in the uninsured categories were smaller which may reduce the precision of our risk estimates, subjecting our results to chance findings. Given the source of our study population, single-center study concerns associated with external validity of our results remain viable. These limitations warrant further replication of our findings in other cohorts with possible inclusion of more detailed baseline demographics.
Health insurance status is an independent pretreatment surrogate for PCa disease control. Patients with private and public insurance are more likely to experience favorable treatment outcomes compared to uninsured patients. Improved outcomes associated with private and public health insurance are stronger for patients with pathologically low-grade PCa. These results can render useful information to clinicians to target patients who are likely to experience inferior treatment outcomes due to a lack of health insurance.
Footnotes
Acknowledgments
Authors thank Nawreen Jahan, Mikhaela Dieudonne, and Adrian Gonzalez-Lozano for assisting in the completion and review of medical records for patients included in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the American Cancer Society MRSG-17-108-01-TBG (to K. Yamoah), the V Foundation (K. Yamoah, J. Park).