
Abstract
The role of external beam radiation therapy for primary liver malignancies has historically been limited due to the risk of radiation-induced liver disease. However, with the advent of stereotactic body radiotherapy (SBRT), we are able to dose escalate while safely sparing critical nearby structures. This review explores the evidence surrounding the use of SBRT for the treatment of primary liver malignancies. A review of the literature was performed. This article discusses the challenges, efficacy, and safety of SBRT for primary liver malignancies in order to conceptualize its role within a multidisciplinary framework. Prospective phase I and II trials show local control rates at 1 to 2 years ranging from 65% to 100%. Overall survival at 1 to 2 years ranged from 48% to 77%. Grade >3 toxicity ranged from 0% to 36%. Total radiotherapy doses ranged from 24 to 60 Gy delivered in 1 to 6 fractions. The SBRT offers a noninvasive therapy for patients with limited treatment options and should be considered in a multidisciplinary setting for the management of unresectable, locally advanced primary liver malignancies. Prospective randomized trials are warranted to determine the efficacy and safety of SBRT compared to and in combination with other treatment modalities.
Keywords
Introduction
Primary liver cancer is the second leading cause of cancer-related mortality globally. 1 The 2 most common subtypes of primary liver malignancy include hepatocellular carcinoma (HCC) arising from hepatocytes and intrahepatic cholangiocarcinoma (IHC) arising from epithelial cells of the intrahepatic bile ducts. The HCC accounts for the majority of primary liver malignancies, and risk factors for HCC (hepatitis and cirrhosis) largely dictate the incidence of primary liver cancer worldwide. The prevalence is highest in males and in Eastern and Southern Asia. The incidence appears to be declining in these high-risk regions due to the decrease in hepatitis B seroprevalence; however, incidence is rising in lower-risk areas including North America, Europe, and India likely due to the increased rates of hepatitis C, obesity, and diabetes. 2
Treatment recommendations for primary liver malignancies are complex and require a multidisciplinary approach, with underlying liver dysfunction playing a key role in guiding management decisions. The preferred treatment modality is surgery with either resection or orthotopic liver transplantation (OLT). In patients with decompensated liver function, OLT offers the best chance of survival with 5-year survival rates of 70% in patients with tumors <5 cm or up to 3 tumors <3 cm without vascular or extrahepatic spread. 3 Surgical resection is largely reserved for patients with normal bilirubin, no portal hypertension, and a solitary lesion <5 cm in diameter. 3 However, only 20% of patients with HCC and 30% of patients with IHC are suitable for primary surgical management at the time of diagnosis. 4 Radiofrequency ablation (RFA) is another curative option, which has been shown to be highly effective for tumors <5 cm in diameter and exhibits comparable results to primary resection. 5,6
The majority of patients with primary liver malignancies, however, are not candidates for curative therapies. For inoperable lesions, where size or location limits the efficacy of RFA, treatment becomes palliative in intent. Options include transarterial therapy, systemic therapy, and external beam radiation therapy (EBRT). Historically, the use of EBRT was limited with regard to primary liver malignancies due to the inability to treat to therapeutic doses while safely sparing critical normal tissues including the uninvolved liver, the duodenum, and the stomach. With advances in patient setup, dosimetry, and treatment planning, we can now safely deliver large doses of radiation while adequately sparing these surrounding normal tissues, thereby increasing the therapeutic ratio. Stereotactic body radiation therapy (SBRT) in particular has allowed for improved local control (LC) when compared to historical controls. Although there is no randomized evidence to evaluate the efficacy of SBRT for primary liver malignancies, multiple prospective and retrospective studies have demonstrated excellent LC rates with minimal toxicity. This review will focus on the evidence surrounding the use of SBRT for the treatment of primary liver malignancies.
The EBRT
The EBRT historically was delivered with 2-dimensional X-ray techniques, with much of the liver being irradiated. This resulted in high rates of radiation-induced liver disease (RILD). There are 2 types of RILD, classical and nonclassical. Classical RILD is seen in patients without underlying liver disorder and is characterized by fatigue, abdominal pain, hepatomegaly, increased abdominal girth, anicteric ascites, and elevation of alkaline phosphatase. 7 Nonclassic RILD, on the other hand, occurs in patients with underlying liver dysfunction and it manifests with jaundice and elevated liver transaminases. 7 The RILD is irreversible and has a high mortality rate. The risk of RILD depends on baseline liver function, volume of liver being irradiated, and radiation dose delivered. This is of particular importance as the patients referred for radiation therapy typically have significantly compromised liver function. The Child-Pugh (CP) grading score is often used to assess baseline liver function prior to treatment. 8 Technological developments have allowed us to significantly reduce the volume of liver being irradiated. The development of 3-dimensional (3-D), cross-sectional-based radiation planning has allowed us to better target liver lesions and spare the remaining, uninvolved liver. Specifically, the development of SBRT has changed the landscape of EBRT to the liver, allowing us to safely deliver high therapeutic doses.
The SBRT
The SBRT is a highly specialized form of EBRT typically utilized for small tumors requiring precise targeting. Stereotactic refers to localization based on a fixed, 3-D reference system. This precise localization allows us to deliver high radiation doses to the target, typically in 1 to 5 fractions, while sparing nearby critical organs. The use of multiple noncoplanar beams that intersect at the region of interest maximizes dose to the target, while minimizing the overlap of exit dose. This technique was first utilized in brain tumors as highly reproducible immobilization of the head is possible and there is no internal motion to account for. The term stereotactic radiosurgery refers to stereotactic radiotherapy delivered within the central nervous system (CNS). As internal localization and motion monitoring techniques have improved, we have been able to safely utilize stereotactic radiation therapy for lesions outside the CNS, referred to as stereotactic body radiotherapy (SBRT).
Stereotactic body radiotherapy to the liver presents unique challenges due to the radiosensitivity of the liver and respiratory motion. The use of magnetic resonance imaging and multiphasic computed tomography (CT; acquisition of images in the arterial and venous phases) has significantly improved the visualization of tumors within the liver. New treatment planning platforms allow fusion of these diagnostic images to the CT simulation scan, allowing for more precise delineation of the gross tumor volume. There are a number of ways to account for respiratory motion including respiratory gating (only treating in certain phases of the respiratory cycle), abdominal compression or breath hold maneuvers to limit breathing motion, 4-dimensional (4-D) simulation (free breathing CT scan taken at the time of simulation so that the internal target volume can account for the location of the tumor throughout the respiratory cycle), or implantation of radiofrequency beacons or fiducials within the tumor that can be tracked during radiation. Daily image guidance is also necessary to improve precision targeting. Onboard imaging with cone beam CT and megavoltage CT has greatly advanced our ability to visualize soft tissue at the time of treatment. With these advances a smaller margin can be utilized for setup uncertainty, thereby sparing normal tissue.
Indications for SBRT
Treatment decision for liver cancer should be made within a multidisciplinary setting. In patients who are not candidates for surgical resection, OLT, or RFA, liver-directed therapies should be considered. These include transarterial therapies, such as transarterial chemoembolization (TACE) and transarterial radioembolization, as well as SBRT. These can be used alone, in combination, or as a bridge to transplantation. Typically, SBRT is reserved for patients with tumors <5 cm, <3 lesions, and tumors located away from bowel. 9 The SBRT becomes a particularly intriguing treatment modality with lesions that are located near the central venous portal vessels or near the biliary system, as these locations often exclude surgery or percutaneous ablative techniques, while SBRT can be delivered without impediment.
Literature Review
The SBRT for liver tumors was first reported in 1995 in a pilot study exploring the use of a stereotactic body frame for extracranial targets. 10 This study included 9 patients with primary liver malignancies, 8 with HCC and 1 with IHC, treated with 16 to 66 Gy in 1 to 3 fractions. Objective response rates were good, with 50% of tumors shrinking or disappearing and 80% of tumors without progression with follow-up from 1.5 to 38 months. A more contemporary phase I/II trial in 2006 evaluated the feasibility, toxicity, and tumor response of SBRT in 8 patients with HCC and 17 with liver metastases.11 Patients with CP A and B were included. Patients with HCC and no cirrhosis or patients with HCC <4 cm and cirrhosis were most commonly treated with 37.5 Gy in 3 fractions, while patients with HCC >4 cm and cirrhosis were treated with either 25 Gy in 5 fractions or 30 Gy in 3 fractions. LC and overall survival (OS) were 75% at 1 year, and grade ≥3 toxicity was 12.5%. One patient with HCC went into liver failure and subsequently died, and authors concluded that although SBRT appears to be feasible with acceptable toxicity and good LC, caution should be taken in patients with CP B. A phase I trial by Tse et al 4 evaluated SBRT for unresectable HCC (31 patients) and IHC (10 patients). All patients were CP A and were treated with 6 fractions delivered every other day over 2 weeks. Dose was determined by the volume of liver being irradiated and a normal tissue complication probability model. Total dose ranged from 24 to 54 Gy. No RILD or grade 4 or 5 complications were seen within 3 months of SBRT, but 7 patients had a decline in liver function from CP A to CP B within 3 months of treatment. Median survival was 11.7 months for patients with HCC and 15.0 months for patients with IHC. Indiana University performed a phase I dose escalation trial for unresectable HCC in 17 patients. 12 Patients with CP A and B and up to 3 lesions with the sum of the diameter of all lesions ≤6 cm were eligible. Total dose delivered ranged from 36 to 48 Gy in 3 to 5 fractions. Local control was 100% at 1 year. A subsequent phase II trial with 26 patients demonstrated a complete or partial response per Response Evaluation Criteria in solid Tumors (RECIST) criteria in 73% of patients. 13 Kang et al 14 performed a phase II trial evaluating the safety and efficacy of SBRT in patients with inoperable HCC as a local salvage therapy after incomplete TACE. Forty-seven patients were evaluable: 41 had CP A cirrhosis, 6 had CP B cirrhosis, and 5 had tumor vascular thrombosis (TVT). Doses ranged from 42 to 60 Gy in 3 fractions. Local control at 2 years was 94.6% and the OS was 68.7%. Treatment was well tolerated, with 11% of patients experiencing a grade ≥3 gastrointestinal toxicity.
The largest prospective study was a combined phase I/ phase II trial performed at Princess Margaret Hospital by Bujold et al. 15 They included 102 patients with inoperable HCC and CP A, with at least 700 mL of uninvolved liver. Dose range was 24 to 54 Gy delivered in 6 fractions every other day over 2 weeks. Primary end points were toxicity and LC at 1 year defined by no progression of irradiated lesions by RECIST. Disease was advanced in this cohort, with 52% of patients having received prior therapy, 55% of patients with TVT, and 12% with extrahepatic disease. Local control at 1 year was impressive at 87%, but grade ≥3 toxicity was seen in 36% of patients, and in 7 patients, death was possibly secondary to treatment.
This study has the largest series of patients with TVT treated with SBRT. The TVT involving the portal or hepatic veins presents a unique clinical situation. These patients are ineligible for most standard therapies and have a poor prognosis with a median survival of 2 to 4 months. 16 Transarterial chemoembolization alone can have some efficacy in this situation but is often limited due to the risk of liver failure. Radiation therapy for TVT in an attempt to recanalize the vessels alone or in combination with TACE has been explored. As discussed above, Bujold et al 15 included 56 patients with TVT. They were treated with a median dose of 36 Gy in 6 fractions with a 1-year OS of 44% and median survival of 10.6 months. On multivariate analysis, TVT was found to be the strongest adverse prognostic factor for survival, highlighting the need for novel treatment modalities to address this situation. Choi et al 17 retrospectively evaluated SBRT alone for small, unresectable HCC and SBRT with TACE for advanced HCC with portal vein thrombosis. Nine patients with advanced HCC and portal vein thrombosis were included in the study. The SBRT dose was 30 to 39 Gy delivered in 3 consecutive fractions, and the interval between SBRT and TACE was at least 4 weeks. Median follow-up was 10.5 months. The overall response rate was 44.4% (4 of 9) and the median survival was 8 months. There were no grade 4 or 5 toxicities. The authors concluded that SBRT followed by TACE is a feasible treatment strategy with acceptable toxicity in selected patients. Finally, Mahadevan et al 18 retrospectively evaluated the efficacy of SBRT specifically for cholangiocarcinomas. They included 31 intrahepatic lesions and 11 hilar lesions. The median prescription dose was 30 Gy in 3 fractions to the median 75% isodose line, and the average maximum dose was 40 Gy. However, a wide range of total dose and fractionation schemes were utilized, with total dose ranging from 10 to 45 Gy delivered in 1 to 5 fractions and maximum total dose ranging from 13.51 to 64.29 Gy. Local control at 4 years was 79%, and median OS was 17 months. The treatment was well tolerated with 4 grade 3 adverse events (12%) including duodenal ulceration, cholangitis, and liver abscess. Grade 4 or 5 adverse events were not observed. Of note, respiratory motion tracking was used, which could account for the low rates of severe toxicity. Phase I and II trials evaluating the safety and efficacy of SBRT for primary liver malignancies are summarized in Table 1. 4,11 -15,19,20 There have been no randomized, prospective trials comparing SBRT to other treatment modalities.
Prospective Trials for SBRT for Primary Liver Malignancies.
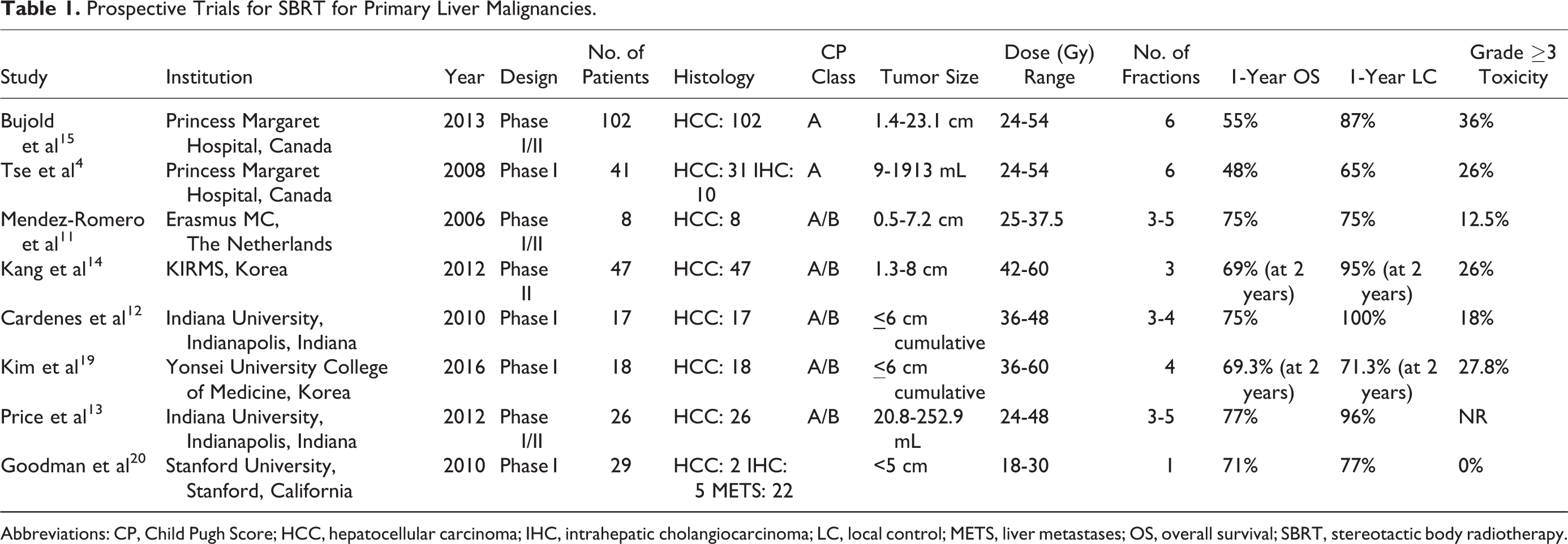
Abbreviations: CP, Child Pugh Score; HCC, hepatocellular carcinoma; IHC, intrahepatic cholangiocarcinoma; LC, local control; METS, liver metastases; OS, overall survival; SBRT, stereotactic body radiotherapy.
As mentioned previously, OLT offers the best chance of survival for patients with decompensated liver function. Unfortunately, limitations in resources and availability of donated organs result in many patients experiencing progression of disease while on the transplant list. Local therapies are often used to treat progressive disease while waiting for organ availability. Both RFA and TACE have historically been the preferred “bridging” modalities, but radiation therapy is emerging as a treatment option. Andolino et al 21 evaluated SBRT in 60 patients with locally advanced HCC, 23 of whom ultimately underwent OLT. Median time to OLT was 7 months. Facciuto et al 22 evaluated 27 patients with locally advanced HCC awaiting OLT. Seventeen patients successfully underwent OLT, 30% had a complete radiographic response, 7% had a partial radiographic response, 56% had stable disease, and 7% had progression of disease. Of the 22 pathologically evaluated lesions, 14% had a complete pathologic response, 23% had a partial response, and 63% had no response. Long-term outcomes of SBRT followed by OLT were published by O’Connor et al 23 in 10 patients with HCC. The median follow-up was 62 months from the time of SBRT. Median SBRT dose was 51 Gy in 3 fractions. Median time from SBRT to OLT was 113 days. All 10 patients successfully underwent OLT with a mean time on the liver transplant wait-list of 163 days. The OS and disease-free survival at 5 years was 100%. A complete pathologic response was achieved in 27% of tumors. The SBRT appears to be a safe and effective bridging modality for patients awaiting OLT.
The body of literature supporting the use of SBRT for primary liver malignancies is growing; however, the optimal radiation dose and fractionation schema is still unknown. The trials to date have used a variety of different doses and fractionations ranging from 15 to 75 Gy in 1 to 15 fractions. A number of studies have demonstrated a dose–response relationship. A retrospective study by Jang et al 24 showed improved outcome with doses >54 Gy. Eighty-two patients with inoperable HCC and tumor diameter <7 cm were treated with 4-fraction SBRT with doses ranging from 33 to 60 Gy prescribed to an isodose line (70%-80% of the maximum dose) that covered at least 97% of the planning target volume. The 2-year LC was 100% and the 2-year OS was 71% in patients treated with >54 Gy, while the 2-year LC and OS was 78% and 64%, respectively, for patients treated with doses from 45 to 54 Gy, and the 2-year LC and OS was 64% and 30%, respectively, for patients treated with doses <45 Gy (P = .009 for LC; P < .001 for OS). Multivariate analysis demonstrated that dose was a significant prognostic for OS. This study showed a dose–response relationship for HCC treated with SBRT with improved LC and OS with doses >54 Gy. Scorsetti et al 25 demonstrated a similar dose–response relationship with improved clinical outcomes with biological effective doses (BEDs) >100 Gy. Forty-three patients with 63 HCC lesions were irradiated. Patients were treated with either 48 to 75 Gy in 3 fractions or 36 to 60 Gy in 6 fractions depending on tumor size and liver function. A BED >100 Gy was significant for LC on univariate analysis (P < .001). Of note, both these studies are retrospective and require further validation. Furthermore, other studies have shown good clinical outcomes with lower doses, particularly with smaller tumors. Sanuki et al 26 reported on 185 patients with tumors ranging from 0.8 to 5 cm in diameter treated with SBRT to doses of 30 to 40 Gy in 5 fractions. Local control was 91% at 3 years and OS was 70% at 3 years. Although lower doses may be effective for small HCC, it is generally understood that a dose–response relationship exists. The HCC is a relatively radiosensitive histology and even higher doses may be needed for IHC and liver metastases. Of course, our ability to dose escalate is limited by normal tissue constraints particularly in patients with compromised baseline liver function. Radiation dose should be prescribed based on the volume of liver being irradiated and the estimated risk of RILD/liver toxicity. Extra caution should be taken in patients with underlying liver dysfunction. Organ at risk constraints are detailed in Table 2.
Dose Constraints for SBRT.a
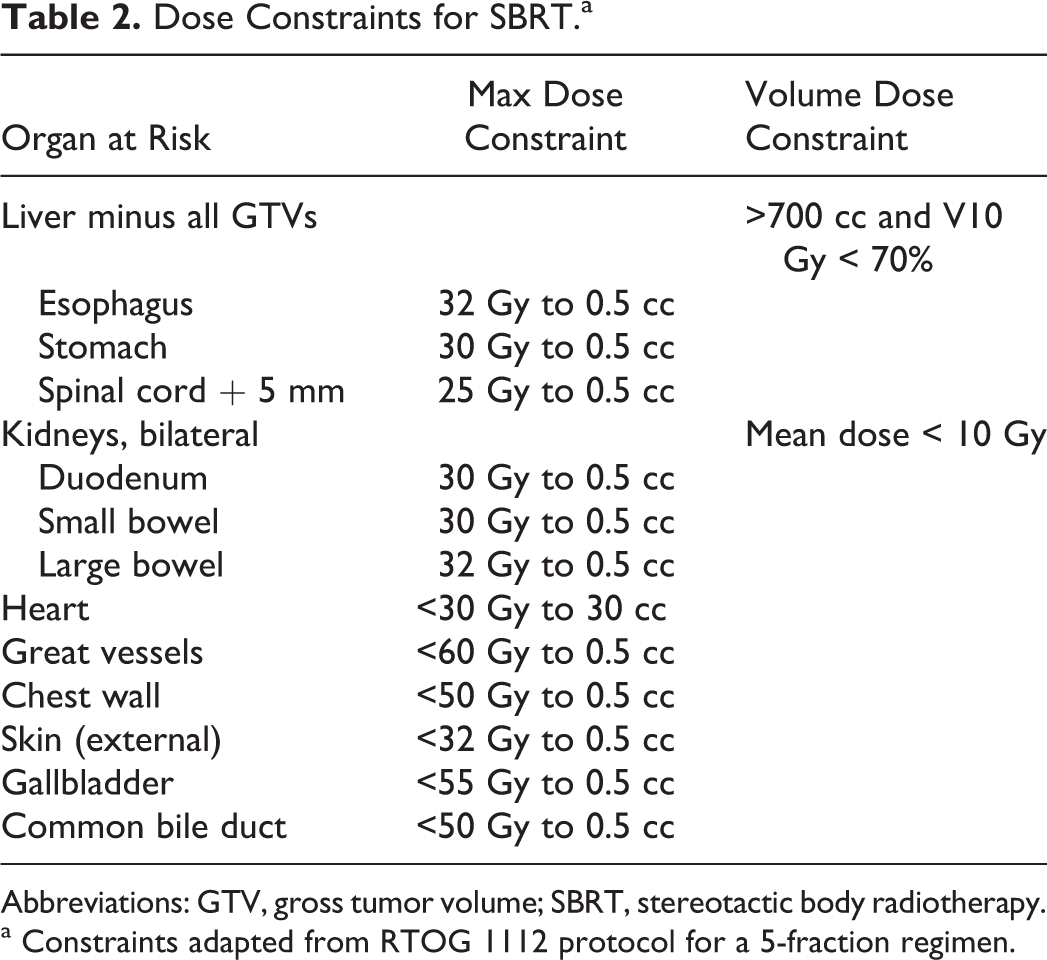
Abbreviations: GTV, gross tumor volume; SBRT, stereotactic body radiotherapy.
a Constraints adapted from RTOG 1112 protocol for a 5-fraction regimen.
Future Directions
The current body of literature surrounding SBRT for primary liver malignancies highlights good LC with acceptable toxicities. What is lacking is prospective, randomized data elucidating the role of SBRT within the multidisciplinary framework for this disease. The RTOG 1112 clinical trial (NCT01730937) is currently enrolling patients to explore this question. It is a phase III, randomized trial comparing sorafenib alone versus SBRT followed by sorafenib in patients with HCC who are unsuitable for resection, OLT, or RFA, as well as unsuitable or refractory to TACE. Sorafenib, an oral multikinase inhibitor, has previously shown improved efficacy in patients with CP A cirrhosis, with improved median survival of 10.7 months versus 7.9 months (P < .001) in a randomized controlled trial when compared to placebo. 27 The RTOG 1112 will help determine whether adding SBRT to sorafenib will further improve outcomes in this population of patients with limited treatment options.
Conclusion
The SBRT is a safe and effective treatment modality for primary liver malignancies. Multiple phase I and II prospective trials, as well as retrospective data, have shown good LC with acceptable toxicities. It can be used alone or in combination with other modalities. It can be used for patients with TVT and as a bridge to OLT. A dose–response relationship exists for HCC, and even higher doses are likely indicated for IHC and liver metastases. However, prescribed dose should be based on the volume of liver being irradiated and the risk for RILD/hepatotoxicity. The SBRT offers a noninvasive treatment for patients with limited treatment options and should be considered in a multidisciplinary setting for the management of unresectable, locally advanced primary liver malignancies. Prospective randomized trials are warranted to determine the efficacy and safety of SBRT compared to and in combination with other treatment modalities.
Footnotes
Author’s Note
No significant relationships exist between the authors and the companies/organizations whose products or services may be referenced in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.