
Abstract
There are several important roles that staging systems and prognostic models play in the modern medical care of patients with cancer. First, accurate staging systems can assist clinicians by identifying optimal treatment selection based on the scope of disease at the time of diagnosis. Second, both physicians and patients may infer prognostic information from staging and models that may help decision makers identify appropriate therapies for individual patients. Third, in research, there is benefit to classifying patients with disease into subgroups ensuring greater parity between experimental and control arms. Staging systems in most solid organ malignancies rely heavily on an accurate pathologic assessment of the tumor (size, site, number of tumors, locoregional spread, and distant spread). Another consideration in primary liver cancer, such as hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma (ICC), is the fact that the underlying liver function can significantly impact patient survival. In HCC, there are at least a dozen options that have been proposed for staging the disease. Herein, we review the most widely used systems and discuss their strengths and weaknesses. Prognostic models and nomograms are also discussed for a variety of subpopulations with HCC. Interestingly, until 2010, the staging system proposed by the American Joint Committee on Cancer for ICC was identical to HCC. The modern staging system, unique to ICC, is reviewed, and future modifications are identified with the primary supporting literature discussed.
Introduction
Both hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma (ICC) arise from within the substance of the hepatic parenchyma and are known collectively as primary liver cancer. There is tremendous geographic variability in the etiology and incidence of primary liver cancer worldwide. While the population-based incidence in Western countries is around 7 to 10 cases per 100 000, the incidence in the East is far greater. 1,2 Additionally, the incidence of liver malignancy is increasing worldwide as the prevalence of cirrhosis and steatosis, the primary risk factors for cancer, increases. 3 Mortality from liver cancer is also on the rise. For example, death from liver cancer in the United States has doubled over the past 3 decades. 2 There is, however, significant regional variation in the ratio of pathologic diagnosis of HCC and ICC. Although HCC is currently more common in the United States, the diagnosis of ICC seems to be increasing at a faster rate. 4
Staging systems and the generation of prognostic models in any cancer are undertaken with the goal to facilitate treatment decisions and provide guidance on expected long-term outcomes. An additional benefit to a universally accepted staging system is the capacity to better match patients and interpret outcomes in clinical investigations and research. Creating these staging/scoring systems for patients with primary liver cancer is uniquely challenging for several important reasons. Specifically, in contrast to other solid organ tumors, the underlying function of the liver plays a large role in the selection of the therapeutic approach and in overall prognosis. Second, there are significant regional variations in practice for patients who present with similar disease burden based on locoregional experience and (in some cases) access to differing therapeutic modalities. Finally, it is worth noting that while the biology of ICC and HCC differs, ICC staging had historically been modeled on HCC staging systems due to the relative rarity of the diagnosis.
Hepatocellular Carcinoma
Models to Identify Patients at Risk of HCC
The identification of risk factors and particularly their regional variation has led to dramatically different approaches to the screening, diagnosis, and classification of patients with HCC. Identified risk factors for the development of HCC include hepatitis C virus, hepatitis B virus (HBV), metabolic disorders (predominantly nonalcoholic fatty liver disease), alcohol-related cirrhosis, tobacco abuse, and genetic disorders (α-1 antitrypsin and hemochromatosis). The predominant risk factor in a population varies based on geography, culture, and race. 5,6 In the United States, for example, it is now estimated that metabolic disorders contribute more to the burden of HCC than any other risk factor. 5 In contrast, alcoholic liver disease predominates in the United Kingdom and viral hepatitis is the most common etiology of HCC arising in the East. 7,8
With the rising incidence of HCC and significant mortality associated with advanced disease, the use of screening programs is advocated in select high-risk populations. In some geographic locales, this translates into screening the entire population. In Western nations, however, the identification of patients at high risk can be used to justify the additional financial and societal costs of screening. There are several models that can be utilized to assess HCC risk, each with relative advantages and disadvantages, and the optimal model may vary based on region or patient-associated factors. In a population of chronic hepatitis B carriers in China, for example, Wong and colleagues identified advanced age, low albumin, high bilirubin, high HBV DNA titers, and presence of cirrhosis as contributing factors for the development of HCC. 9 This same model was validated in a Western population and had fair accuracy, particularly as a negative predictive tool among patients stratified into the low-risk cohort. 10
Clinical Staging: Patient Presentation
Survival after diagnosis with HCC is due principally to 3 related factors: cancer biology, delivery of an optimal cancer-directed therapy, and a patient’s underlying health and liver function. These 3 factors are not independent, and each has the capacity to impact the other 2 factors. As mentioned earlier, the capacity of the underlying liver parenchyma to impact the overall prognosis is common and relatively unique in primary liver cancer. The impact of underlying liver function on overall prognosis has been the focus of several prognostic models. The classic example is the Child-Pugh classification that was originally developed to model survival in patients requiring emergent surgical intervention for bleeding esophageal varices. 11,12 In this model, physical exam findings of encephalopathy and ascites are combined with laboratory examination of bilirubin, albumin, and prothrombin time to categorize patients into 1 of 3 classes (Table 1). In an initial report 12 of 38 patients in King’s College Hospital in London, mortality after esophageal transection for bleeding varices ranged from 29% in grade A patients to 88% in grade C patients. Over a half century later, categorization of underlying liver function by the Child-Pugh classification has been generalized and validated for use in a wide range of clinical scenarios. The Child-Pugh classification is still included in many of the most widely endorsed clinical decision-making models for HCC, with grade A patients thought to be favorable for operative approaches when possible. The major criticism of Child-Pugh’s grading scale is the relative subjective nature of 2 of the underlying data points in the model (encephalopathy and ascites burden).
Child-Pugh Grading Criteria.a
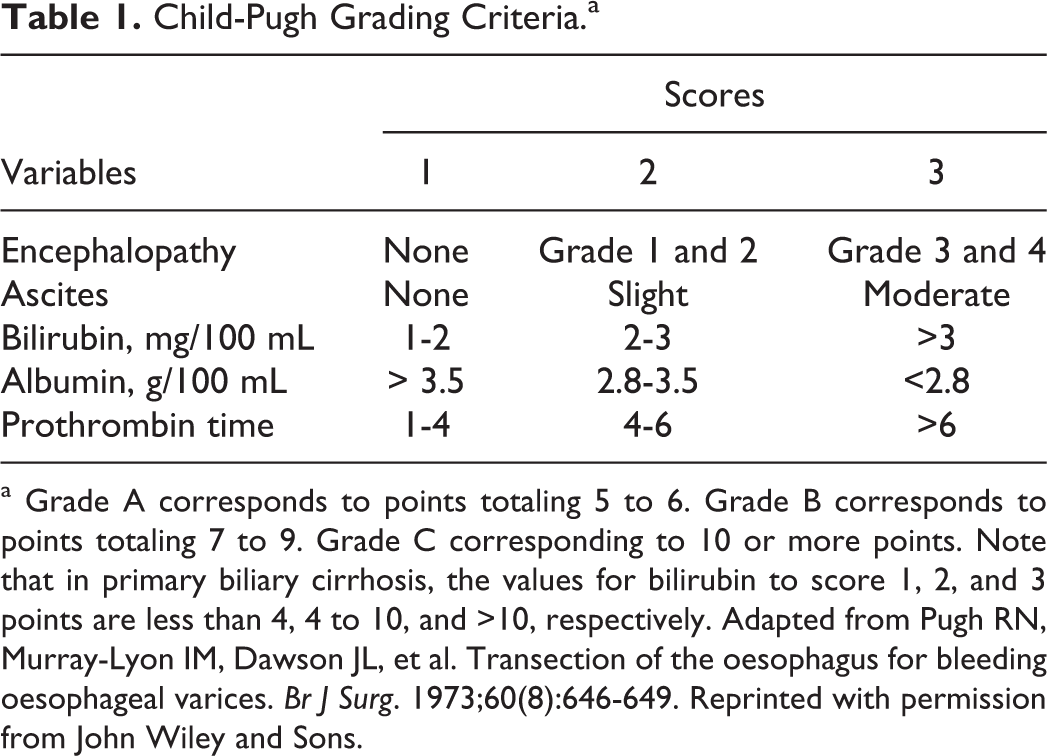
a Grade A corresponds to points totaling 5 to 6. Grade B corresponds to points totaling 7 to 9. Grade C corresponding to 10 or more points. Note that in primary biliary cirrhosis, the values for bilirubin to score 1, 2, and 3 points are less than 4, 4 to 10, and >10, respectively. Adapted from Pugh RN, Murray-Lyon IM, Dawson JL, et al. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg. 1973;60(8):646-649. Reprinted with permission from John Wiley and Sons.
Two other models to assess underlying liver function are commonly utilized by clinicians: the Model for End-Stage Liver Disease (MELD) score and the Albumin–Bilirubin (ALBI) grade. The MELD score was originally developed to estimate periprocedural mortality following transjugular intrahepatic portosystemic shunt placement. 13 The MELD is a composite score generated from 3 laboratory values: international normalized ratio, serum total bilirubin, and serum creatinine. The MELD scoring has been validated and generalized for use in patients with cirrhosis undergoing a wide array of procedures, including liver transplantation and hepatectomy. 14 -16 As a general rule, patients with a MELD score of 10 or less are considered to have an acceptable risk of elective operative interventions. Patients with an MELD between 10 and 15 are considered to be at moderate risk, and decisions on interventions need to be made after careful risk–benefit analysis; in contrast, individuals with an MELD exceeding 15 are largely considered to have a prohibitive risk of elective operative interventions. An important limitation to the generalized use of the MELD score is that it is not predictive of perioperative outcomes in patients without cirrhosis. 17
Recently, some authors have advocated for the use of the ALBI grade as a means to assess liver function. 18,19 The ALBI grade is based on assessment of serum albumin and bilirubin; the ALBI was developed using a retrospective analysis of patients with HCC and included patients with and without cirrhosis. 18,19 External validation was carried out using a broad spectrum of patients, including individuals with limited disease undergoing resection to patients with advanced disease receiving sorafenib. Importantly, compared to the Child-Pugh and MELD classifications, the ALBI model can be used in patients with or without cirrhosis. Additionally, analysis in a multinational cohort suggested a greater prognostic discriminatory capacity within a cohort of patients generally regarded as having a uniformly favorable prognosis (Child-Pugh A). 18
Clinical Staging: Patient Management
Beyond the impact of underlying liver function on survival, other HCC staging and prognostication schemes have focused on the assessment of the underlying disease biology and selection of optimal treatment strategies. Disease biology has classically been assessed using tumor number, size, and total tumor volume. There are several well-known clinical decision models that have attempted to combine the underlying liver function along with markers of disease biology to provide clinical guidance with regard to treatment selection. The most commonly endorsed modern models include the Barcelona Clinic Liver Cancer (BCLC) model and the Cancer of the Liver Italian Program (CLIP) score. 20,21 It is important to highlight that these systems have relative strengths and weaknesses that have led to the development of over a dozen other systems or system refinements. One weakness shared by many of the systems is the relative lack of discrimination in early-stage HCC. This is principally due to a bias toward advanced patient disease in the cohorts used to construct these staging systems.
Originally introduced in 1999, the BCLC model includes an assessment of liver function (Child-Pugh class), an assessment of tumor biology (number of nodules, tumor size, vascular invasion, presence or absence of metastasis), and the evaluation of each patient’s performance status. The inclusion of performance status relies on an assignment of Eastern Cooperative Oncology Group performance status prior to staging and is somewhat unique compared to other staging models. The BCLC classification subcategorizes patients into 5 stages (0, A, B, C, and D), with performance status, underlying liver function, and tumor characteristics used to direct therapeutic recommendations (Figure 1). The BCLC is endorsed by the European Association for the Study of the Liver and the European Organization for Research and Treatment of Cancer. 21,22 While comprehensive in scope, the use of the BCLC for therapeutic selection in early- or intermediate-stage HCC has been challenged by others due to the BCLC’s limited capacity to stratify this group of patients. 23 For example, the use of surgical resection is restricted in the BCLC to patients only categorized as stage 0 (excellent performance and liver function status and single tumor <2 cm in size or carcinoma in situ). A strict interpretation of the BCLC would offer only liver transplantation or ablative therapies for locally confined disease >2 cm. In practice, the use of resection is routinely expanded beyond BCLC stage 0 patients.

Schematic for hepatocellular carcinoma (HCC) from the Barcelona Clinic Liver Cancer (BCLC) staging system. The BCLC system divides patients into 5 distinct cohorts based on liver function (Child Pugh), patient comorbidities (performance status), and tumor burden. Unique to the BCLC, recommendations for therapy are provided according to stage. CP indicates Child Pugh grade; PS, performance status, LT, liver transplantation, TACE, transarterial chemoembolization. Adapted from Llovet JM, Burroughs A, Bruix J. Hepatocellular carcinoma. The Lancet. 2003;362(9399):1907-1917 with permission from Elsevier.
In patients with advanced disease, the BCLC similarly provides treatment selection guidance based on disease biology, patient performance status, and liver function. In patients with multinodular disease and good performance status (intermediate stage, stage B), transarterial chemoembolization strategies are recommended. In contrast, among patients with advanced stage disease who have portal invasion or locoregional or distant metastatic spread, the use of systemic agents (such as sorafenib or clinical trial agents) is recommended (stage C). It must again be noted, however, that there is significant heterogeneity in patients classified in stage B and C. As such, some authors have questioned the BCLC recommendations for these patients and have noted that some patients may be candidates for therapies not routinely recommended by the model, such as resection. 23 Finally, the BCLC recommends best supportive care alone for patients with terminal disease (stage D) due to either performance status or liver function (including all Child-Pugh C).
The CLIP scoring system was introduced in 1998 and includes an assessment of liver function (Child-Pugh) and tumor biology (tumor size relative to liver, vascular invasion, and metastasis; Table 2). 20 There are several differences when comparing the BCLC and CLIP staging systems. First, while the BCLC includes an estimate of patient performance status, the CLIP score does not. Second, the CLIP includes serum α-fetoprotein concentration (with a cutoff of 400 ng/mL) as a surrogate marker of tumor biology, while the BCLC does not. The staging categories in CLIP vary from 0 to 6, with median survival ranging from weeks (score 5/6) to several years (score 0/1). Perhaps the most important difference between the BCLC and the CLIP system is a lack of treatment recommendations in the CLIP score. Similar to BCLC, the CLIP score has been criticized for its relative inability to accurately discriminate the prognostic differences in patients with early-stage HCC (ie, operative with small tumors). The CLIP system is, however, generally favored in nonsurgical patients with advanced HCC. 23
CLIP Scoring System.

Abbreviations: AFP, α-fetoprotein; BCLC, Barcelona Clinic Liver Cancer; CLIP, Cancer of the Liver Italian Program.
a Total score is computed by the sum of points from each variable, ranging from 0 to 6. Unlike the BCLC, no formal treatment assignments are made based on score. Adapted from A new prognostic system for hepatocellular carcinoma: a retrospective study of 435 patients: the Cancer of the Liver Italian Program (CLIP) investigators. Hepatology. 1998;28(3):751-755. Reprinted with permission from John Wiley and Sons.
Pathological Staging Systems
Surgical extirpation or transplantation remains the gold standard of a curative paradigm for patients with HCC. In surgical patients, a staging system based on pathology assessment of the tumor is recommended for use. There are 2 main systems that include a histopathologic assessment of disease: the American Joint Committee on Cancer (AJCC)/International Union Against Cancer (UICC) staging system (now in its seventh edition) and the Japan Integrated Staging (JIS) score. 24 -26 In general, the general recommendation is to use the AJCC/UICC staging system for all patients undergoing resection or transplantation. 23
The AJCC/UICC provides prognostic information based only on the pathologic characteristics of resected specimens. The AJCC/UICC is structured using the TNM scheme, as well as additional designations for histologic grade and fibrosis (Figure 2). 26 Identification of T-stage relies on assessment of tumor size, number of tumors, and involvement of major portovenous structures or adjacent organs. Regional lymph node involvement, although frequently not assessed at the time of surgery, is a binary variable classified as either lack of (N0) or presence of (N1) regional nodal metastasis. In keeping with other tumor systems, metastasis is also a binary variable with either absence (M0) or presence (M1) of distant disease. Anatomic stage and prognostic groups are determined as shown in Figure 2. Histologic grade (G) should be assessed by an experienced pathologist and categorized into 4 classes: well differentiated, moderately differentiated, poorly differentiated, or undifferentiated. Fibrosis score (F) also requires inspection by an experienced pathologist and uses a scale from 0 to 6. In general, no to moderate fibrosis (scale 0-4) is assigned an F0 score, whereas severe fibrosis or cirrhosis is assigned a score of F1.
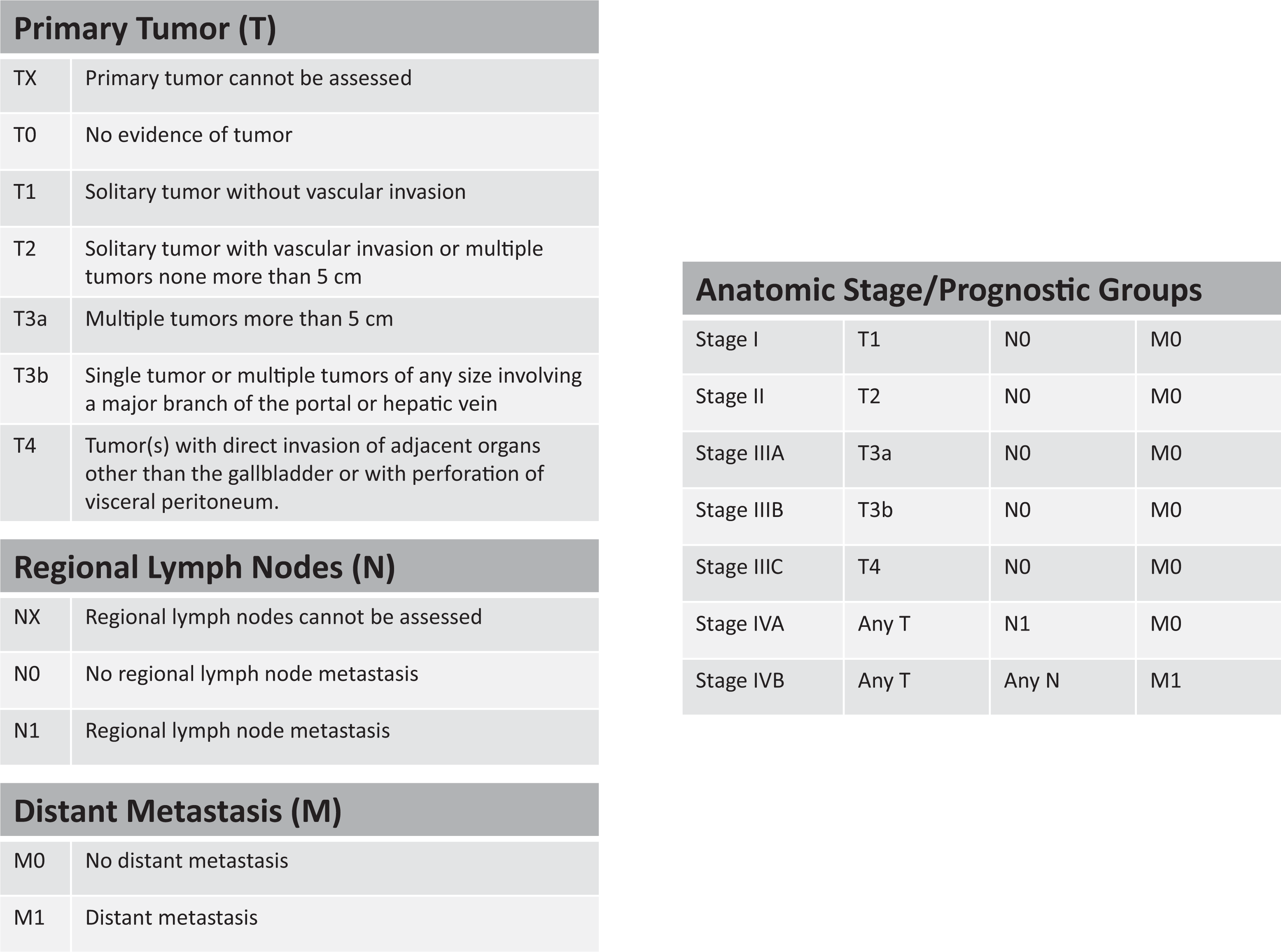
The American Joint Committee on Cancer (AJCC)/International Union Against Cancer (UICC) TNM pathologic staging system for hepatocellular carcinoma (HCC). The recommended staging system for all patients with HCC according to expert consensus, the AJCC/UICC system based on tumor biology (as suggested by tumor characteristics) and stage omits patient comorbidities and liver function from consideration. Additionally, although treatment recommendations can be derived from a variety of sources (such as expert consensus documents, the National Comprehensive Cancer Network guidelines, or loco-regional tumor boards), the AJCC/UICC system does not directly recommend therapies. Finally, a complete pathologic evaluation to include grading of the tumor and fibrosis score are required to complete the AJCC/UICC staging (see text). Adapted with permission from Springer from Edge S, Byrd D, Compton C, et al. AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer; 2010; permission conveyed through Copyright Clearance Center, Inc.
Despite the absence of clinical factors and treatment recommendations in the AJCC/UICC staging system, certain organizations such as the National Comprehensive Cancer Network (NCCN) in the United States use the system upon which to base clinical guidelines. A treatment algorithm has been outlined that includes early surgical assessment based on the technical ability to resect the tumor and the adequacy of liver function (Child-Pugh). Actual treatment decisions are deferred to the discretion of local multidisciplinary teams, but in general, surgical extirpation by either hepatectomy or transplantation is advocated by the NCCN when feasible. While no formal assessment of performance status is included, the NCCN guidelines do caution that patients must be “medically fit for a major operation” when surgery is being considered.
The JIS score is another pathology-based staging system that has gained some acceptance. 24 Similar to the AJCC/UICC system, the JIS score largely focuses on patients diagnosed with HCC that have been treated with resection or transplantation. 24 Based on the Liver Cancer Study Group of Japan, the JIS combines Child-Pugh grade and basic TNM staging to assign patients a total score (Table 3). In turn, some authors have suggested that the JIS scoring system is the best balance between discriminatory capacity and simplicity and therefore lends itself to be used in the clinical setting. 24 When compared directly to CLIP, the stratification of patients (particularly individuals with early HCC) appears superior using the JIS. 24
Japan Integrated Staging (JIS) Scoring System.b

a Adapted with permission from Springer from Kudo M, Chung H, Osaki Y. Prognostic staging system for hepatocellular carcinoma (CLIP score): its value and limitations, and a proposal for a new staging system, the Japan Integrated Staging Score (JIS score). J Gastroenterol. 2003;38(3):207-215; permission conveyed through Copyright Clearance Center, Inc.
b TNM staging in the Japan Integrated Staging (JIS) is initially described as according to the Liver Cancer Study Group of Japan.
Given the plethora of staging systems being utilized, as well as the increased difficulty in efficiently using the staging systems as more variables are included, some groups have advocated for a consensus global scoring system. 25 For example, Farinati et al 27 has recently proposed an international staging system derived from the Italian Liver Cancer (ITA.LI.CA) data set. Based on factors including the size of the largest liver nodule, the number of nodules, and presence or absence of vascular invasion or metastasis, the ITA.LI.CA system outperformed several modern staging systems (Figure 3).
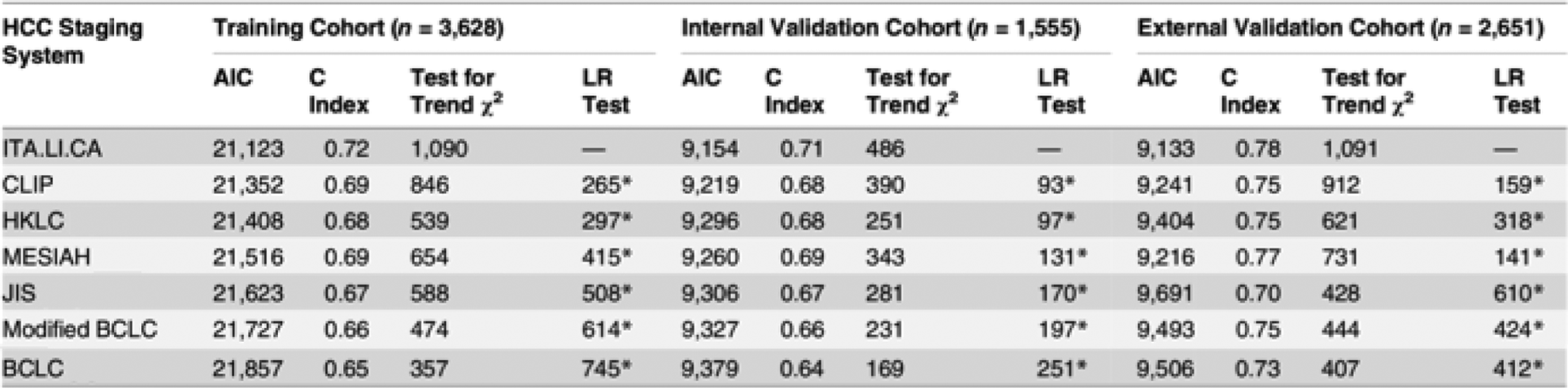
Comparison of major hepatocellular carcinoma (HCC) staging systems, including the recently proposed Italian Liver Cancer (ITA.LI.CA). The suboptimal prospective clinical performance of many HCC staging systems has led to continued efforts at refinement. The ITA.LI.CA staging system is one of the latest to be proposed. 27 In data presented from the latest analysis, the ITA.LI.CA system is compared against several other contemporary systems including the Cancer of the Liver Italian Program (CLIP), 20 the Hong Kong Liver Cancer (HKLC) system, 28 the Model to Estimate Survival in Ambulatory HCC Patients (MESIAH), 29 the Japan Integrated Staging (JIS) system, 24 the modified Barcelona Clinic Liver Cancer (BCLC) system, 30 and the original BCLC. 21 In this comparison, a lower AIC value represents a higher discriminatory ability of the staging system. In contrast, the higher the C index and the test for trend chi-square, the better the discrimination of the system. Finally, the ITA.LI.CA score is used as a baseline and compared against the other systems using the likelihood ratio test. Adapted from Farinati F, Vitale A, Spolverato G, et al. Development and validation of a new prognostic system for patients with hepatocellular carcinoma. PLoS Med. 2016;13(4): e1002006. https://creativecommons.org/licenses/by/4.0/legalcode.
Prognostic nomograms in HCC
Nomogram prediction models have been proposed as a better means to predict long-term survival for individual patients with various malignancies. Nomograms take into account specific disease subsets and may provide more accurate prognostic information for individual patients. For HCC, multiple prognostic nomograms have been proposed that include a wide array of factors (Table 4). Given that most HCC staging systems have focused on patients with advanced disease, nomograms may be particularly helpful among those patients who are relatively healthy with early disease. Accordingly, several proposed nomograms have been developed with a particular goal of stratifying outcomes in the particular patient cohort of early-stage patients. 30 -33,35 To this point, while pretreatment performance status and liver function play a major role in many staging systems, these factors seemingly have a smaller role in many nomograms. Rather, indicators of disease biology such as α-fetoprotein levels are commonly incorporated into many nomograms as a surrogate marker of disease biology. Additionally, pathological variables such as tumor size, number, and presence of vascular invasion (including major and sometimes minor invasion) are commonly included as discriminating factors in many HCC nomograms. 30 -36
Prognostic Nomograms in Hepatocellular Carcinoma.a
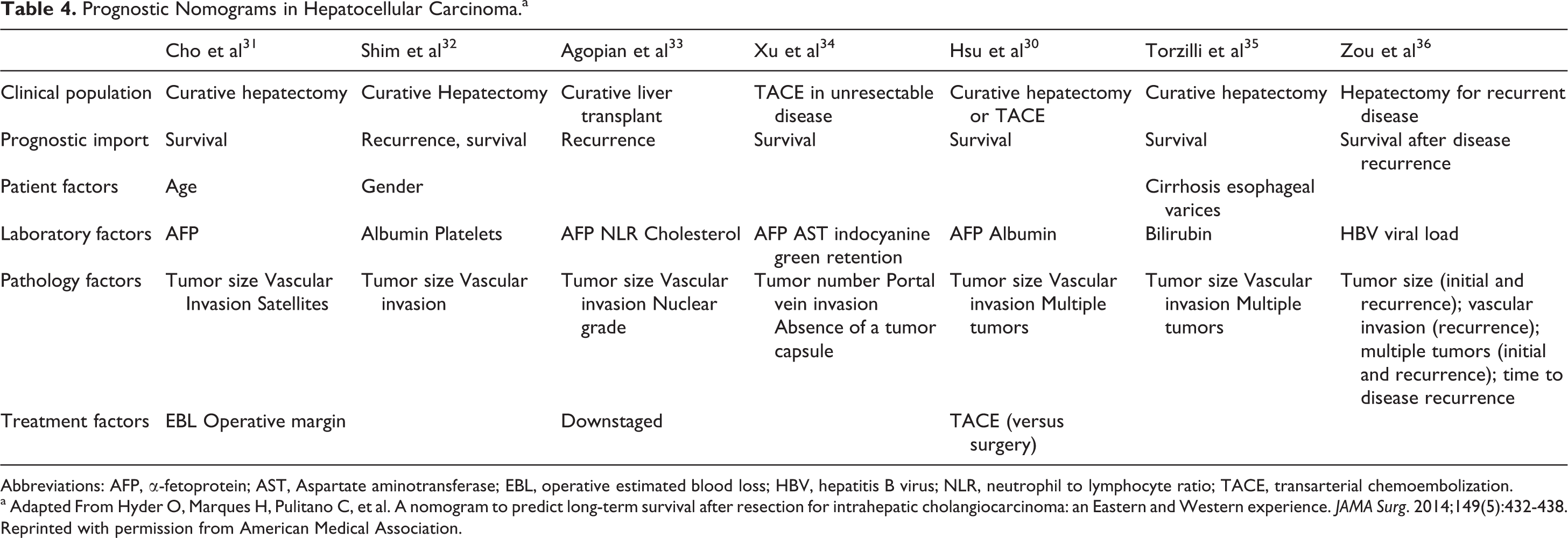
Abbreviations: AFP, α-fetoprotein; AST, Aspartate aminotransferase; EBL, operative estimated blood loss; HBV, hepatitis B virus; NLR, neutrophil to lymphocyte ratio; TACE, transarterial chemoembolization.
a Adapted From Hyder O, Marques H, Pulitano C, et al. A nomogram to predict long-term survival after resection for intrahepatic cholangiocarcinoma: an Eastern and Western experience. JAMA Surg. 2014;149(5):432-438. Reprinted with permission from American Medical Association.
The staging and prognostic models developed to date are designed to understand the biology of HCC and help direct therapies. The delivery of recommended therapies is, however, not uniform. Just as there are differences in the incidence of disease based on geography and patient-level factors, there are also variations in the treatment and survival of patients based on factors other than pathological tumor factors. 6,37 For example, Asian patients in the United States appear most likely to receive treatment for a diagnosis of HCC. 6 Further, despite being older and having larger tumors on presentation, Asian patients have been reported to have the lowest risk of death from HCC. Further research is necessary to better characterize the sociodemographic and biologic factors underlying these racial disparities in care.
Intrahepatic Cholangiocarcinoma
Modeling to Identify Patients at Risk of ICC
When considering ICC, it is important to distinguish ICC from other cholangiocarcinomas such as hilar and distal cholangiocarcinoma. In addition, given the relative rarity of ICC, the number of staging systems that have been proposed for ICC are fewer than that for HCC. While HCC is common enough to warrant development of screening models for patients at risk, there have been no such widespread efforts in ICC. Screening for ICC is generally done on a case-by-case basis, with indications typically including primary sclerosing cholangitis, known history of liver fluke infection, high-risk hepatitis C or B infection, and other conditions associated with chronic inflammation of the biliary tract epithelial lining (including congenital disease, obesity, and carcinogen exposure). 38 -40
Pathological Staging Systems
Historically, the AJCC/UICC staging system used for ICC was identical to the system used for HCC largely due to the rarity of the disease and lack of data. The use of the HCC AJCC/UICC staging system ignored, however, possible unique aspects of tumor biology of ICC. As such, 2 staging systems had been proposed in Japan. 41,42 Yamasaki 41 proposed a staging system based on the Liver Cancer Study Group of Japan that included number of tumors (solitary vs multiple), size of tumor (<2 cm vs ≥2 cm) and vascular invasion (presence vs absence of portal or hepatic vein). In a separate report, Okabayashi et al 42 proposed a different staging scheme that involved only tumor number (solitary vs multiple) and vascular invasion (present or absent). Given the lack of a proposed staging system in the West, Nathan et al 43 analyzed the Surveillance, Epidemiology, and End Results database aimed at developing a staging system for ICC. Assessing nearly 600 patients with ICC, the data demonstrated that the historical AJCC/UICC T-staging system, as well as both Japanese staging systems, failed to discriminate accurately patients with ICC into prognostic groups. The authors proposed a modified, simplified staging system for ICC that largely focused on tumor number and the presence or absence of vascular invasion, while excluding tumor size. Subsequently, Farges et al 44 validated this proposed staging system and noted its superiority over the sixth edition AJCC/UICC staging system, as well as 2 other pathological staging systems reported from Japan.
As such, in 2010, the seventh edition of AJCC/UICC staging manual adopted most of the recommendations from the staging system proposed by Nathan et al 43 and published the first unique staging system for ICC. 26 T-classification depends on vascular invasion, number of tumors, and direct extension to extrahepatic structures. Regional nodal involvement and metastatic disease are both classified as binary factors. Unlike surgical recommendations for HCC, which typically do not support lymph node sampling, general recommendations for ICC patients include a lymphadenectomy, given the important prognostic information provided. 45,46 Anatomic stage and prognostic groupings are shown in Figure 3. Finally, histologic grade is used to further stratify patients.
Several studies have validated the predictive accuracy of the seventh edition AJCC/UICC staging manual, particularly when compared to the sixth edition. 44,47 Using the seventh edition as a baseline, multi-institutional studies have subsequently refined the staging system and have proposed several changes. The eighth edition, published in late 2016, took some of these refinements into account and aimed to move away from a population-based to a more “personalized” approach to cancer care relying on recommendations from prognostic and risk assessment models. Several changes have been made to ICC staging in the eighth edition (Figure 4). Specifically, in the eighth edition staging, the T1 category was revised to account for the prognostic impact of tumor size (T1a ≤5 cm vs T1b > 5 cm). In determining a size cutoff, 2 studies were considered. Sakamoto and colleagues had suggested a tumor cutoff size of 2 cm when analyzing a Japanese patient cohort, 48 and data from a Western report suggested, however, that tumor size >5 cm was most appropriate and generalizable for this staging update. 49 The T2 category is modified to reflect the equivalent prognostic value of vascular invasion and tumor multifocality. In addition, the seventh edition T4 category describing the tumor growth pattern was eliminated from staging but is still recommended for data collection.

The American Joint Committee on Cancer (AJCC)/International Union Against Cancer (UICC) TNM Pathologic Staging System for ICC. The recommended staging system for all patients with ICC according to expert consensus, the eighth edition AJCC/UICC system is based on tumor biology (as suggested by tumor characteristics on pathologic examination). A complete pathologic evaluation of the tumor, including assessment of tumor grade, is required to complete formal AJCC/UICC staging (see text). Adapted with permission from Springer from Amin MB, Edge S, Greene F, et al. AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer; 2016. Permission conveyed through Copyright Clearance Center, Inc.
Prognostic Nomograms in ICC
The prognostic capacity of the AJCC/UICC ICC staging system, similar to the HCC staging system, is limited to some extent by individualized patient variability. Therefore, it is more applicable to broad populations rather than individual patients. Several nomograms have been developed for ICC that may help predict outcomes for specific individuals. The 2 most popular nomograms in ICC involve stratifying prognosis for patients following curative intent hepatic resection. For example, Wang et al 50 developed a nomogram to predict prognosis following partial hepatectomy using data from a single institution in China. Factors included in the nomogram were serum carcinoembryonic antigen, carbohydrate antigen 19-9, tumor diameter, tumor number, vascular invasion, lymph node metastasis, direct invasion, and local extrahepatic metastasis. The authors reported their nomogram outperformed the seventh edition AJCC/UICC on internal validation. With publication of the eighth edition, nomograms such as these may require reexamination.
More recently, an international multi-institutional collaboration resulted in the development of a refined nomogram for patients undergoing resection for ICC (Figure 5). 49 Similar to the Wang nomogram, tumor size, number of tumors, nodal status, and presence of vascular invasion were associated with long-term prognosis and therefore were included in the nomogram. Additional factors included the age at diagnosis and the presence of cirrhosis at the time of resection. Notably, preoperative laboratory values (such as CEA or CA 19-9) were not included. External validation of both nomograms has subsequently confirmed their increased discriminatory ability over the AJCC/UICC staging system for patients with ICC undergoing partial hepatectomy. 51
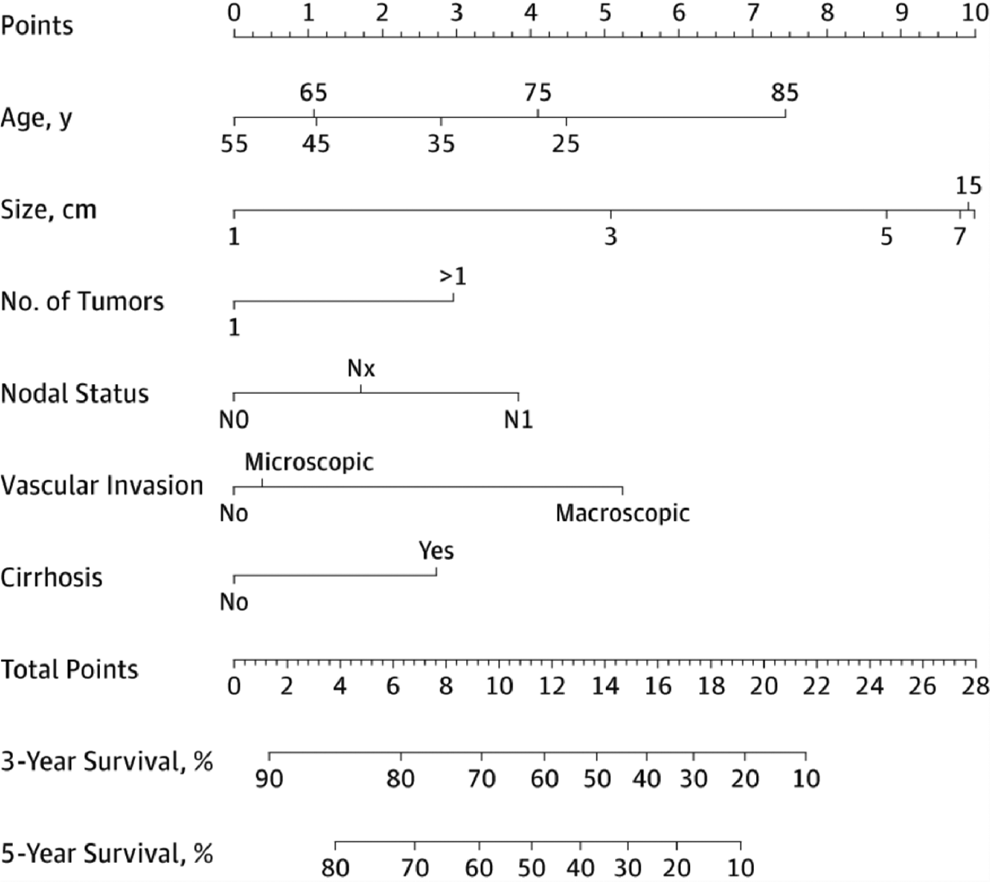
A prognostic nomogram for predicting postsurgical survival of patients with resectable intrahepatic cholangiocarcinoma. The nomogram published by Hyder and colleagues represents one of the most comprehensive efforts to date to clarify survival in the postoperative period for patients with intrahepatic cholangiocarcinoma (ICC).
Conclusion
Given the rarity and biologic heterogeneity of primary liver cancer, the development and acceptance of universal, accurate staging systems has been difficult for these diseases. In HCC, a myriad of proposed systems has led to persistent regional variability in the clinical use of different staging paradigms. In contrast, ICC had no unique staging system until 2010 with the publication of the seventh edition of the AJCC/UICC Cancer Staging Manual. The care and staging of patients now is guided by the eighth edition of the AJCC Cancer Staging Manual. Overall, current expert consensus recommends adherence to the AJCC/UICC system for all patients able to be pathologically staged in both HCC and ICC. The use of AJCC/UICC staging to infer prognostic outcome can, however, at times be overly generalized and fail to account for variations in oncologic therapies and prognosis of individual patients. In these scenarios, clinical use of externally validated nomograms should be encouraged to help facilitate an understanding of individualized patient prognosis. The eighth edition of the AJCC has recognized this need and now documents emerging prognostic factors for clinical care (including recommended risk assessment models when appropriate) and provides recommendations for future clinical trial stratification.
Footnotes
Authors’ Note
No significant relationships exist between the authors and the companies/organizations whose products or services may be referenced in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.