
Abstract
Hepatocellular carcinoma (HCC) is a major cause of cancer-related death worldwide. In select patients, surgical treatment in the form of either resection or transplantation offers a curative option. The aims of this review are to (1) review the current American Association for the Study of Liver Diseases/European Association for the Study of the Liver guidelines on the surgical management of HCC and (2) review the proposed changes to these guidelines and analyze the strength of evidence underlying these proposals. Three authors identified the most relevant publications in the literature on liver resection and transplantation for HCC and analyzed the strength of evidence according to the Grading of Recommendations Assessment, Development and Evaluation (GRADE) classification. In the United States, the liver allocation system provides priority for liver transplantation to patients with HCC within the Milan criteria. Current evidence suggests that liver transplantation may also be indicated in certain patient groups beyond Milan criteria, such as pediatric patients with large tumor burden or adult patients who are successfully downstaged. Patients with no underlying liver disease may also benefit from liver transplantation if the HCC is unresectable. In patients with no or minimal (compensated) liver disease and solitary HCC ≥2 cm, liver resection is warranted. If liver transplantation is not available or contraindicated, liver resection can be offered to patients with multinodular HCC, provided that the underlying liver disease is not decompensated. Many patients may benefit from surgical strategies adapted to local resources and policies (hepatitis B prevalence, organ availability, etc). Although current low-quality evidence shows better overall survival with aggressive surgical strategies, this approach is limited to select patients. Larger and well-designed prospective studies are needed to better define the benefits and limits of such approach.
Introduction
Primary liver cancer is the fifth most common malignant tumor in men and ninth in women worldwide and is associated with the second highest cancer-related mortality rate among both sexes. 1 The highest incidence has been reported in Southeast Asia and sub-Saharan Africa. During the last 4 decades (1973-2007), its incidence increased among the North American and European populations. 2 In the United States, its incidence approximately doubled from 1976 to 2000. 3 Chronic hepatitis B virus (HBV) infection is a major risk factor in parts of the world with high liver cancer incidence, while chronic hepatitis C virus (HCV) infection is the main risk factor among low-incidence populations. Liver cirrhosis and metabolic syndrome also have been identified as independent risk factors. 4
Hepatocellular carcinoma (HCC) is the most common form of primary liver cancer, followed by intrahepatic cholangiocarcinoma and mixed hepatocholangiocellular carcinoma. The former originates from hepatocytes, while the latter from cholangiocytes (bile duct epithelium). The biological behaviour of these tumors differs, as well as the survival benefit obtained from surgical therapies. This review will concentrate on the surgical treatment of HCC, assessing the most recent data on the role of liver resection (LR) versus liver transplantation (LT).
Our goal is to review the patient and tumor characteristics that affect the decision for choosing the modality of surgical treatment, to present the recent changes in liver allograft allocation for patients with HCC in the United States, and to discuss the controversies on the surgical management of HCC stage by stage. Table 1 is a summary of the literature and evidence-based review based on the GRADE classification.
Summary of Statements.a
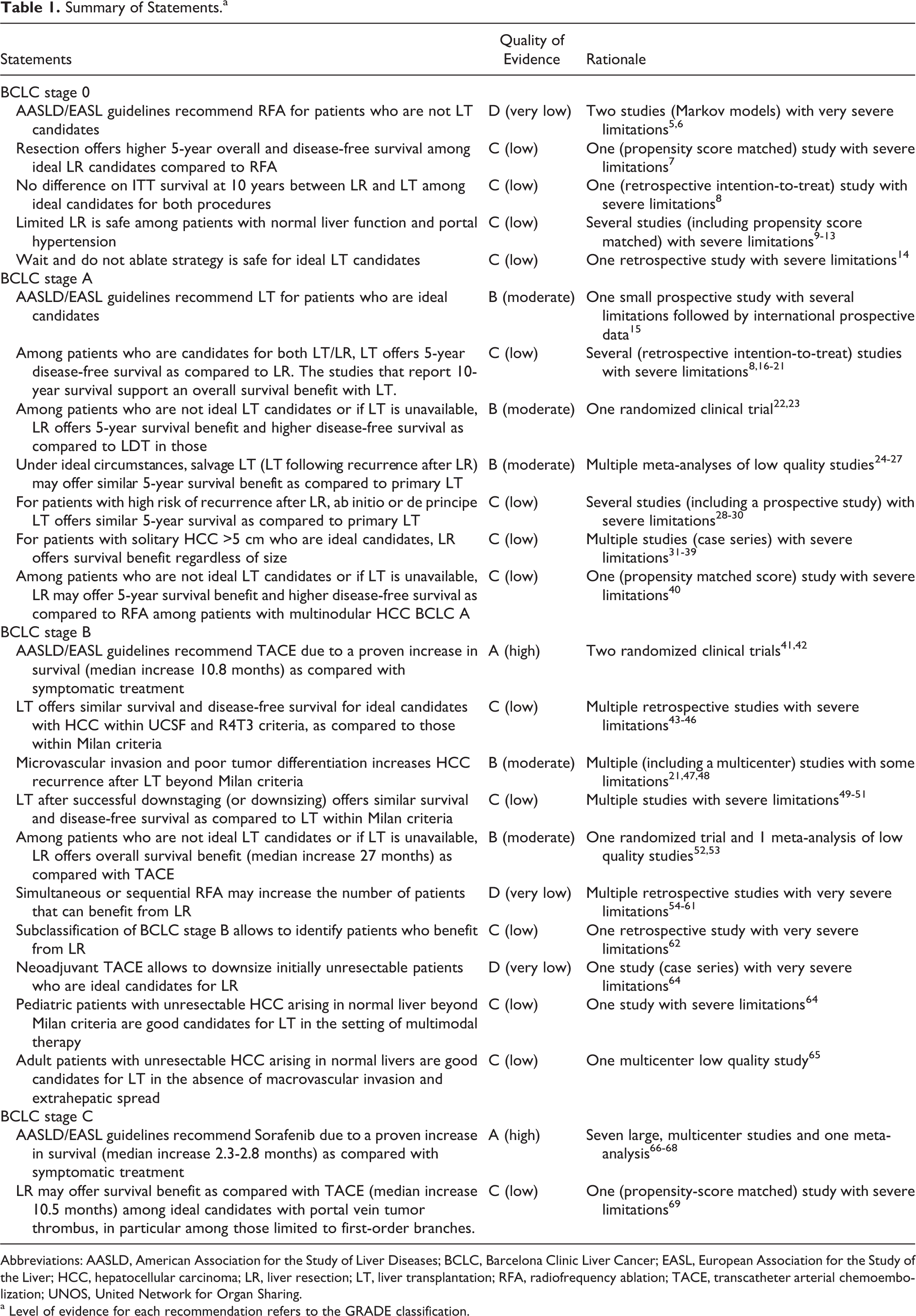
Abbreviations: AASLD, American Association for the Study of Liver Diseases; BCLC, Barcelona Clinic Liver Cancer; EASL, European Association for the Study of the Liver; HCC, hepatocellular carcinoma; LR, liver resection; LT, liver transplantation; RFA, radiofrequency ablation; TACE, transcatheter arterial chemoembolization; UNOS, United Network for Organ Sharing.
a Level of evidence for each recommendation refers to the GRADE classification.
Evaluation of Patients for LR: Special Considerations
Etiology of the Underlying Liver Disease
Countries with high prevalence of chronic HBV infection have more consistently offered LR to patients with low or intermediate stage HCC than those with low prevalence, as overall survival (OS) after LR among patients with HBV-associated HCC is greater than that observed in patients with HCV-associated HCC. 70 This outcome is likely the result of both the degree of liver disease and the biology of the HCC. Patients with HBV frequently have livers without cirrhosis, larger HCC, less satellite nodules, and less macrovascular invasion than patients with HCV. 71 ,72
Serum α-Fetoprotein
In patients with chronic liver disease, serum α-fetoprotein (AFP) alone has limited utility for screening and diagnosis of HCC. It can be falsely elevated in association with other tumors and benign portal vein thrombosis. However, in the setting of confirmed HCC, AFP is a marker of disease biology. Blank et al 72 demonstrated that even within normal range (<6.0 ng/mL), patients with higher AFP have worse prognosis. Among patients within Milan criteria undergoing LT, a serum AFP >1000 ng/mL at the time of LT predicts early HCC recurrence. Among patients exceeding Milan criteria, the AFP levels less than 100 ng/mL predict a significantly lower 5-year risk of recurrence. 73
Other biological markers, such as protein induced by vitamin K absence-II 74 and neutrophil–lymphocyte ratio, 75 have been proposed as predictors of disease progress and/or recurrence, alone or in combination with AFP. As the value of these markers has not been verified in larger cohorts, despite their promising potential, they are not used currently for the selection of candidates with HCC for LR or LT listing.
Liver Function
Preoperative liver function is typically assessed by the Child-Pugh (CP) classification, based on serum albumin, total bilirubin, and prothrombin time as well as the presence and grade of ascites and hepatic encephalopathy. To avoid the use of subjective variables (ascites and encephalopathy), a multinational collaborative group developed the albumin–bilirubin (ALBI) score as an alternative. The ALBI score, similar to CP classification, predicts OS after LR and provides a better predictive value for patients within CP class A. 76 There is no universal cutoff to determine a patient’s candidacy for LR, as this is based on the expected outcomes, local resources, and health system policy. Current American Association for the Study of Liver Diseases/European Association for the Study of the Liver (AASLD/EASL) guidelines recommend LR for HCC only in patients with serum total bilirubin ≤1 mg/dL. A cutoff of ≤2 mg/dL bilirubin are often used in Asian centers. 77 Child-Pugh stage C is universally accepted as a contraindication for any form of LR.
The model for end-stage liver disease (MELD) score also predicts perioperative mortality among patients with cirrhosis undergoing resection for HCC. In 3 different studies, patients with cirrhosis and an MELD score <9 had a low morbidity (8%) and no mortality from postoperative liver failure. In contrast, patients with an MELD score ≥9 had a greater risk of postoperative liver failure and perioperative mortality. 78 -80
Indocyanine green (ICG) clearance was introduced as an adjunctive measure to assist in the decision and extent of LR in patients with cirrhosis. Indocyanine green is an anionic organic dye that is selectively taken up by hepatocytes and rapidly excreted in bile. It is usually measured as percentage serum retention at 15 minutes (R15). An ICG cutoff of <10%, 10% to 20%, 20% to 30%, and >30% at 15 minutes has been reported as safe for extended resection, hemihepatectomy, segmentectomy, and wedge resection, respectively. 77 Recently, a multicenter study developed a grading system using serum albumin and ICG R15 evaluation (ALICE). Similar to the previously described ALBI, ALICE had predictive power similar to CP classification but allowed further stratification of CP class A patients. These results were validated in a retrospective European cohort. 81 The use of ICG clearance over other functional tests is debated and rarely used in the United States.
Portal Hypertension
Bruix et al 82 described the results of 29 CP class A patients with cirrhosis who underwent LR for HCC after hepatic venous pressure gradient (HVPG) measurement. This analysis showed that 73% of patients with clinically significant portal hypertension, defined as HVPG ≥10 mm Hg, had acute decompensation of their chronic liver disease postoperatively which persisted for >3 months in 39%. In contrast, none of the patients with HVPG <10 mm Hg had hepatic decompensation persisting for >3 months. This HVPG cutoff is currently included in the AASLD/EASL guidelines. Cucchetti et al 83 confirmed the risk of decompensation after LR for HCC among patients with HVPG ≥10 mm Hg and demonstrated that (1) HVPG <10 mm Hg cutoff excludes 1 of every 4 patients who would benefit from surgery without morbidity and (2) the risk of postoperative liver failure among patients with HVPG ≥10 mm Hg undergoing wedge LRs is 14% (as compared with 66% with larger resections). 83
Hepatic venous pressure gradient measurements are not performed routinely in many centers, instead surrogates of clinically evident portal hypertension (CEPH), platelet count (<100 000/µL), splenomegaly, and the presence of varices are used, which leads to variability in data reporting. According to a recent meta-analysis, the presence of CEPH has been associated with an increased risk of acute hepatic decompensation (odds ratio [OR]: 3), perioperative mortality (OR: 2), and lower 3- and 5-year OS (OR: 2). 84 The study has been criticized due to advanced liver dysfunction among patients with CEPH included in some of the studies and the statistical methods employed. 85
Large case series from Asian centers suggest that the outcome of patients undergoing minor LR with or without CEPH is similar. Only patients with CEPH undergoing major LR have had a decreased OS (1-year 88% vs 95%, 3-year 59% vs 73%, and 5-year 30% vs 50%). 9 Zhong et al 86 argued that the impact of portal hypertension on the outcome of LR for HCC is lower than the potential benefit of LR on OS as compared to other therapeutic strategies. 86 A recent multinational collaborative study evaluated the application of current guidelines among 20 centers from 3 continents: CEPH (defined by platelet count <100 000/µL and imaging findings; splenomegaly, varices, or ascites) had little impact on the centers’ decision to offer LR to patients with HCC. In addition, CEPH did not have a significant impact on the outcome in CP class A patients who underwent LR. Based on their data, Roayaie et al 87 estimate that expanding resection criteria to include those with CEPH, with platelet count >50 000/µL, and without ascites would increase the pool of LR candidates by approximately 60%. 87 The potential benefit of increasing the number of patients undergoing LR needs to be weighed against the expected morbidity, mortality, and organ availability, should the patient be a candidate for salvage LT (SLT). 88,89
Extent of LR
The question of anatomical versus nonanatomical LR in patients with HCC has been debated over the past decades. The proponents of the former often argue that anatomical LR has the theoretical advantage of removing possible satellite lesions and microscopic dissemination. No randomized trial has addressed this issue to date. Multiple single-center analyses have demonstrated variable results. Unfortunately, many confounding factors that correlate with survival are not addressed in these analyses, limiting the strength of their conclusions. Indeed improved OS among patients who undergo anatomical LR may be a consequence of selection bias, as most patients with lower functional reserve undergo nonanatomical LR. 90 In a meta-analysis including 12 nonrandomized studies with a total of 1829 patients, no significant difference was observed between the 2 strategies on OS or disease-free survival (DFS). 91
Volume of Liver Remnant
Patients with normal liver function and no parenchymal disease can tolerate resection of up to 70% to 80% of the liver, provided that vascular inflow–outflow and biliary drainage are maintained. 92 Cirrhotic livers have a lower regenerative capacity and tolerate any additional injury poorly. Patients with cirrhosis, even with normal liver function tests, tolerate far less parenchymal loss and are unlikely to survive resection of more than 60% of the liver. 93
Limited experience of extended LR in patients with liver fibrosis or cirrhosis has been reported, mainly by Asian centers. Patients who require extended LR often have large tumors replacing most of the affected lobe, thus removal of the involved lobe may not result in substantial loss of functional parenchyma. 94 The indications for such extended LR, especially in patients with no parenchymal disease, have been expanded over the past 3 decades. 95 In patients with small future liver remnants (FLRs), preoperative selective portal vein embolization (PVE) has been used successfully to increase the remnant size. 96 For patients with cirrhosis, PVE has been recommended when the FLR is ≤40%. 97 Alternatively, PVE has been advocated for FLRs ≤40% when the ICG R15 is ≤10%, and for FLRs ≤50% when the ICG R15 is 10% to 20%. 98 Importantly, because regenerative capacity is diminished, 10% to 20% of patients with chronic parenchymal disease undergoing PVE do not experience adequate contralateral hypertrophy. 99
The HCC-targeting radioembolization with yttrium90 (Y90) -loaded microspheres has been used as an alternative to PVE, 100 controlling the disease while providing a lower degree of contralateral hypertrophy. 101 The experience with this approach has been very limited and the parenchymal transection after Y90 therapy is technically more demanding. 102 A novel method to induce FLR hypertrophy in patients with extensive colorectal liver metastases, associated liver partition with portal vein ligation for staged hepatectomy (ALPPS), has recently been attempted in patients with HCC. In a cohort of 35 patients with or without parenchymal disease, ALPPS induced a 47% hypertrophy of the FLR (usually the left lateral sector). The degree of hypertrophy significantly correlated with the degree of fibrosis. In this cohort, however, the perioperative mortality was very high (31%). 103 Thus, this procedure should be limited to young patients without cirrhosis or comorbidities, who are not LT candidates and in whom the risk of the operation is deemed acceptable.
Performance Status
Performance status (PS) accurately predicts long-term OS in patients with HCC. 104 Performance status is rated through a scale developed by the Eastern Cooperative Oncology Group (ECOG), ranging from 0 (fully active) to 4 (completely disabled). 105 According to the Barcelona clinic liver cancer (BCLC) system, patients with PS 0 are ideal candidates for LR. Patients with PS >1 are considered as higher risk for LR. 106 ,107 This component of the BCLC staging system is based on limited data and has been criticized widely. In fact, in a single-center analysis, Hsu et al 107 demonstrated that patients with cirrhosis, HCC, and PS 1 who underwent either surgical therapy or liver-directed therapies (LDTs) had OS similar to that of PS 0 patients and a significantly better OS than those with PS 2.
Evaluation of Patients for LT
Patients with any degree of parenchymal liver disease and portal hypertension can undergo liver transplantation, as liver replacement solves both problems. Patients with HCC considered candidates for LT must otherwise be ideal candidates for transplantation.
Hepatocellular carcinoma management by LT in Western countries implies that a liver allograft is obtained from the limited pool of deceased donors. In order to ethically justify the use of these allografts for patients with any form of malignancy, the expected OS should be similar to that obtained after LT for chronic liver disease without cancer.
Early retrospective studies showed that incidental HCC <5 cm could be “cured” by LT (defined, at that time, as a patient alive and disease free beyond 2 years from the date of transplantation). 108,109 The second significant finding of these early studies was that patients with multifocal disease, lymphatic metastasis, vascular invasion, and/or positive margins (documented pathologically by examination of the resected liver) recurred within the first year after LT. Based on these findings, Mazzaferro et al 15 developed a set of criteria based on the number and size of lesions (single lesion ≤5 cm or ≤3 lesions none exceeding 3 cm) identified on imaging studies before LT. They prospectively followed 48 patients who underwent LT for unresectable HCC, radiologically within these criteria. During pathological examination after LT, it was shown that 73% of the patients had tumors within criteria, while 27% had lesions beyond the criteria. The OS of patients within the criteria on pathological examination was significantly greater (4-year OS 85% vs 50%). These cutoffs on number and size of HCC are now known as the Milan criteria and widely used worldwide as listing criteria for LT from deceased donors.
The current liver allocation system in the United States uses the Model for Endstage Liver Disease (MELD)-Na score calculated from the levels of serum total bilirubin, sodium, creatinine, and international normalized ratio (INR) for prothrombin time. This score predicts the 90-day mortality of patients with cirrhosis in the absence of LT. Under this system, patients on the LT waiting list with the highest MELD-Na scores (highest predicted mortality without transplantation) receive allograft offers first (“sickest first” policy). Many patients with early HCC have compensated liver disease and consequently low MELD-Na scores, which otherwise limit access to LT. To rectify this problem, patients with cirrhosis and HCC within Milan criteria are assigned an exception score, which aims to provide adequate timing of LT before progression beyond criteria for transplantation. When this policy was implemented initially in 2002, candidates with very early HCC (1 lesion <2 cm) and early HCC (1 lesion ≥2 cm but <5 cm, or as many as 3 lesions <3 cm each) were assigned 24 and 29 points, respectively. Patients who were not transplanted within the first 3 months were then granted 3 additional points every 3 months, to account for 10% increased mortality risk during the same interval. Although little data were available prior to the implementation of the policy, tumor doubling time reported by Barbara et al 110 and Cheng et al 111 were used to estimate the risk of falling out of criteria. Within a year, this policy resulted in a 300% increase in the proportion of patients undergoing LT for HCC (from 7% to 22%). 112 The waiting time for transplantation among patients with HCC decreased from 2.3 to 0.7 years and their dropout rate at 5 months decreased from 25.9% to 6.7%. However, this system unfairly favored patients with HCC over patients with chronic liver disease without HCC; inadvertently increasing the risk of delisting of the latter group to 35.8% because of death or degree of illness. Consequently, the policy was revised, and patients with single HCC <2 cm who are candidates for LT are no longer granted exception points. Subsequently, the United Network for Organ Sharing (UNOS) MELD exception policy for HCC has undergone multiple modifications. Currently, to counterbalance opportunities for LT between candidates with HCC and others with chronic liver disease, only patients with HCC within Milan criteria (single nodule ≥2 and ≤5 cm or 2-3 nodules all ≤3 cm) are granted 28 points after a mandatory 6-month delay, with 1 to 2 additional points every 3 months until LT. The MELD exception score has been capped at 34 points. The rationale for the initial mandatory delay was to identify patients with rapidly progressive HCC that would have limited OS benefit from LT due to early disease recurrence.
If untreated, approximately 70% of patients with HCC have further tumor growth within 1 year of initial diagnosis in whom 20% develop vascular invasion and 9% develop metastases. 113 To prevent such progression while awaiting LT, most patients with HCC undergo LDT. 114 In the United States, the use of LDT in patients awaiting LT ranges from 31% to 65% based on UNOS region that affects donor availability and expected waiting times. 115 Response to LDT predicts HCC recurrence and it is currently used as a prognostic marker of disease biology. 116 -118
Controversies on the Surgical Management of HCC
Very Early Stage HCC
Child-Pugh class A, mild parenchymal liver disease without CEPH, and good PS with a single lesion <2 cm
Liver resection results for very early HCC in ideal candidates is excellent, and intention-to-treat (ITT) outcomes comparing LR and LT have shown similar 5- and 10-year OS benefit. 8 Among ideal surgical candidates, the main controversy is whether LR or radiofrequency ablation (RFA) is preferable. No randomized trial compared LR to RFA specifically among patients with HCC <2 cm. Liver resection in such patients is associated with a median OS of 74.5 months (5-year OS of 70%) and <1% 90-day mortality. 119 A recent propensity score match analysis of 237 patients with very early HCC who underwent LR (n = 109) or RFA (n = 128) demonstrated a greater 5-year OS after LR (80% vs 66%; P = .034). Also, 5-year DFS after LR was greater (48% vs 18%; P < .001). 7 Despite these findings, current AASLD/EASL guidelines recommend RFA.
Child-Pugh class A, advanced stage parenchymal liver disease with CEPH, good PS with a single lesion <2 cm
If LT is contraindicated or unavailable, CP class A patients with CEPH and peripherally located HCC could undergo wedge LR safely. However, the potential benefit of LR must be weighed against the risk of complications, with RFA being a safe and effective alternative. Currently, patients with single HCC <2 cm who are otherwise candidates for LT are not granted MELD exception points. Quite commonly LDT are held until HCC growth reaches size eligibility for listing. Mehta et al 14 analyzed 114 candidates for LT with HCC <2 cm and was followed every 3 months. Tumor diameter increased a median of 0.14 cm per month. Progression beyond Milan without LT listing occurred in 4.4% at 6 months and 9.0% at both 12 and 24 months. Predictors of progression beyond LT criteria were AFP ≥500 ng/mL and rapid tumor growth (defined as >1 cm increase in total tumor diameter over 3 months). Overall survival was 94.5% and 75.5% at 1 and 3 years, respectively. This study showed that the strategy of “wait and not ablate” may be beneficial for patients in need of an LT without compromising the oncological control of their HCC.
Early Stage HCC
Child-Pugh class A, with or without CEPH, and good PS with a single lesion >2 cm and <5 cm without vascular invasion
For patients with early stage HCC (single lesion ≥2 cm) within Milan criteria and CEPH, LT is recommended as a first-line treatment, if there is no contraindication. The 5-year OS after LT for HCC improved dramatically over time: 25.3% (1987-1991), 46.6% (1992-1996), and 61.1% (1997-2001; P < .0001). Current 5-year OS is estimated at 62%. The 5-year OS of patients on the waiting list (ie, ITT) is estimated at 51%, due mainly to dropouts on the wait-list. In the United States, 18% of patients with HCC listed for LT are delisted due to disease progression or death. 120 Dropout and LT rates have differed significantly between UNOS regions. 121,122 Size (>3 cm) and number of lesions (≥2 nodules), serum AFP (≥20 ng/mL), and complete response to LDT have been identified as predictors of dropout or death without transplant among patients with HCC listed for LT. One-fifth of the patients with HCC listed for LT have none of these variables and the corresponding dropout rate is 1.3% and 1.6% at 1 year and 2 years, respectively. On the contrary, patients with 1 or more of the aforementioned variables have had a dropout rate of 21.6% and 26.5% at 1 year and 2 years, respectively. 122
The major controversy on patients with no CEPH and a potentially resectable single HCC 2 cm to 5 cm is LR versus LT. In the unusual circumstance where a patient is a candidate for LR but not LT, or LT is not available, LR is the treatment of choice. To date, 4 randomized trials have compared LR to RFA. Huang et al showed an improved OS and recurrence-free survival (RFS) with LR. 123,124 Feng et al 23 showed similar outcomes with both strategies; however, they identified a higher risk of residual tumor with RFA, leading to the need for repeated therapy. Chen et al,124 randomized 90 patients to LR and RFA each, identifying no difference between the 2 strategies; however, an unusually high number of crossover (19 patients switched from RFA to LR) may have overstated the benefit of RFA. A randomized trial including 200 patients showed greater 1-, 3-, and 5-year OS and DFS after LR compared to combined LDT (transcatheter arterial chemoembolization [TACE] + RFA). 22 ,23
To date, there has been no randomized trial comparing LT versus LR (or ablative therapies) in these patients. Numerous retrospective single-center studies have addressed the outcome after LR and LT. Unfortunately, most of these studies lack adequate control of confounding factors and have variable criteria for LT listing and organ availability. In particular, a selection bias toward patients with better liver function and more aggressive HCC in the LR cohort is observed in several studies. Regardless, some reports have provided insight and are noteworthy: Llovet et al 16 showed an ITT OS advantage for LT (69% vs 51% after LR) in patients with a single HCC <5 cm. Five-year ITT OS was similar for LT and LR only in patients with no portal hypertension and serum total bilirubin ≤1 mg/dL (74% vs 69% after LT). Similar results were reported by Bigourdan et al, 17 with a 5-year OS benefit of LT over LR (71% vs 36%; P = .04). However, the treatment groups had significant demographic differences. Moreover, there were no wait-list dropouts in the LT arm. Another study from the University of Toronto group has shown that patients with a low waiting time before LT (<4 months) had greater ITT OS than similar patients undergoing LR (P = .04). 18 Furthermore, a report from Paul Brosse Hospital (which included patients with CP class B and C) found that patients undergoing LT had greater ITT OS (61% vs 50% after LR; P = .05) than those with LR. 19,125 A meta-analysis of 10 heterogeneous studies concluded that LT was associated with greater OS than LR (OR: 0.58; 95% confidence interval [CI]: 0.36-0.94) in CP class A patients with early stage HCC. 20
Despite the intergroup heterogeneity of the patients, recurrence rate has been consistently greater after LR for HCC than after LT. To address this issue, some centers offer LR as the first-line therapy and LT for recurrence, if the recurrent HCC is within the Milan criteria. This strategy is referred to as SLT in the literature. The 2 main limitations of this approach have been (1) the frequency of HCC recurrence beyond Milan criteria (20%-50%) and (2) increased perioperative morbidity and mortality. 21
The outcome after SLT has been compared to primary LT for HCC by several groups. Belghiti et al 126 described similar operative time, blood loss, transfusion rate, ICU and hospital stay, morbidity, and 30-day mortality as well as equal 3- and 5-year OS for both approaches. Adam et al 125 found greater blood loss and 60-day mortality after SLT. Moreover, 5-year DFS and OS were reduced by 30% and 20%, respectively. A meta-analysis of SLT and primary LT showed no difference in 1-, 3-, and 5-year OS. 24 A recent report demonstrated that the ITT 5- and 10-year OS was greater after primary LT (68/58% vs SLT 58/35%; P = .008) which likely related to the fact that SLT was feasible only in one-third of patients who underwent primary LR. 127 The DFS is lower among patients who undergo LR and, currently, most centers in the country opt for primary LT for early HCC.
In lieu of organ scarcity, some centers offer LR as first strategy and, to avoid recurrence beyond Milan criteria, preemptively list patients with high-risk features, like the group of the hospital clinic in Barcelona. 28 The presence of microvascular invasion, poor tumor differentiation, and satellite or additional nodules could potentially decrease OS benefit after LT. To test this concept, 164 patients who underwent LR for HCC since 1995 were followed. All patients were having CP stage A without CEPH, had a single HCC <5 cm (72% <3 cm), and were also ideal candidates for LT. Patients with resected HCC and high-risk features for recurrence were listed for LT before HCC recurrence occurred (ab initio SLT). 128 Of the 37 patients with these tumor characteristics, it recurred in 23 (62%) patients before LT, but in 9 (24%) patients the recurrences were beyond Milan criteria. Ab initio SLT was performed in 17 (46%) patients, of whom 7 (41%) had confirmed recurrence before transplantation. Five-year OS after LT was 82.4% and ITT OS was 60.2%. 29 A similar strategy was explored by others in which patients were listed for LT after LR either before (de principe) or after detection of recurrence. 30 Their results demonstrated that the patients with low-risk HCC features (no microvascular invasion and well-differentiated tumors) have similar OS with the SLT or de principe LT, but patients with high-risk features (microvascular invasion and/or moderately or poorly differentiated tumors) have greater 5-year OS with the de principe LT strategy (86% vs 60%; P = .032).
Although not a routine practice outside the centers cited above, the strategy of SLT and/or ab initio LT has several potential advantages: (1) by decreasing the waiting time on the LT list, the dropout rate may be reduced, (2) the allografts currently used for such patients may be allocated to patients on the list for indications other than HCC, and (3) it allows for identification of tumor biology in patients with early and aggressive recurrence after LR, which, in turn, may be used as a criterion to exclude such patients from LT. If such an approach is to be adapted, the candidates should be informed on the potential benefits and disadvantages of upfront LR, including the risk of developing new HCC in the remaining parenchyma.
Child-Pugh class A, without CEPH and good PS, with a single lesion >5 cm without vascular invasion
According to the BCLC staging system, any solitary HCC lesion exceeding 2 cm without vascular invasion is stage A. Reported outcomes of LR in such patients require scrutiny because many reports of LR for HCC >5 cm come from countries with high incidence of HBV infection. As stated previously, HBV-associated HCC are frequently larger and have less vascular invasion, which more commonly occur in patients with better liver functional reserve.
Multiple single-center studies have demonstrated the feasibility of LR for solitary HCC >10 cm in ideal candidates. 31 -38 Liver resection on patients with solitary HCC >10 cm has been associated with similar OS and DFS than LR on patients with HCC <10 cm (OS: 53% and 58%; DFS: 24% and 26%, respectively). 39 Advanced liver disease (serum total bilirubin >1.8 mg/dL), CEPH (platelet count <150 000 cells/mL), and malignant portal vein thrombosis have been associated with death within the first 3 months. 35
Child-Pugh class A, without CEPH and good PS, with 2-3 lesions <3 cm without vascular invasion
Patients with 2 to 3 HCC nodules, all <3 cm, are considered early HCC, BCLC stage A and are candidates for LT. Current AASLD/EASL guidelines recommend RFA for patients who are not LT candidates. Few reports have addressed LR on multinodular BCLC stage A patients. Jiang et al 40 have reported the outcome of patients with multifocal BCLC A HCC who underwent LR (n = 224) or RFA (n = 160). Propensity score–matched analysis showed greater DFS in the LR group and no difference on 1-, 3-, and 5-year OS. This analysis demonstrated that patients with all nodules within the same hemiliver had the greater DFS. Multivariate analysis showed that having CEPH, 3 nodules, and/or different sectorial localization were poor predictors of survival.
Intermediate Stage HCC (Stages B and C)
According to the BCLC staging system, patients with multinodular HCC >3 cm (or >3 nodules) and good PS are stage B. Most BCLC stage B patients are not candidates for either LT or LR, and the goal is to prolong OS and maintain PS rather than cure. Thus, current AASLD/EASL guidelines have recommended TACE as a standard of care based on 2 randomized trials that showed an approximately 10-month improvement in mean OS compared to symptomatic treatment. 41,42 Only select patients with BCLC B stage will be candidates for surgical management. In the rare setting where a surgical approach is feasible, LT was associated with greater OS and DFS. 129
Liver Transplantation for HCC Beyond Milan Criteria
Reports of LT for patients with a single HCC lesion >5 cm which is HCC beyond Milan criteria (but BCLC stage A) require specific comment. Currently, patients presenting with HCC beyond Milan criteria can still access LT through (1) listing with their biological MELD, (2) living donor LT, (3) domino LT, and (4) “downstaging” or “downsizing” using LDT. The Milan criteria have been considered too restrictive by some, and expanded criteria for patients with larger tumor burden to gain access to LT without increasing the risk of recurrence have been proposed. The University of California in San Francisco (UCSF) group proposed the expanded criteria of solitary HCC ≤6.5 cm or ≤3 nodules ≤4.5 cm (provided that total tumor diameter is ≤8 cm). Liver transplantation for HCC within these criteria were associated with 5-year OS of 75% and these results have been validated by other centers. 43,130
Onaca et al 44 analyzed the International Registry of Hepatic Tumors in Liver Transplantation, which included 1206 patients with HCC. The 5-year OS of patients within Milan criteria in that registry was 61.8%. In the same registry, patients with a solitary HCC ≤6 cm or with 2 to 4 lesions ≤5 cm each had a DFS similar to those within Milan criteria. 44 These listing criteria have been applied in UNOS region 4 and referred to as R4T3 criteria. The same group updated their experience, showing greater 3-year OS and DFS in patients beyond Milan but within R4T3 criteria as opposed to those beyond both criteria. 45
Mazzaferro et al 48 performed a similar retrospective study by including 1556 patients from 36 LT centers of whom 1112 had HCC beyond the Milan criteria. Tumor size, number, and microvascular invasion were evaluated on the explant to develop a predictive tool for disease recurrence. Accordingly, increasing HCC size correlated linearly to recurrence after LT, but the number of HCC did not. Microvascular invasion was associated with doubling of the risk of death. These data led to the development of an online tool that can predict 3- and 5-year OS for a given patient with known microvascular invasion, size, and number of nodules (http://www.hcc-olt-metroticket.org/calculator/). Findings of this study show similar outcomes after LT in patients within Milan criteria and in patients with the “up-to-seven” criteria (diameter of the largest nodule [centimeter, cm] plus number of nodules ≤7) in the absence of microvascular invasion. To aid in the selection of latter criteria, a biopsy of the HCC can be obtained to assess the latter. Patients with poorly differentiated HCC have been excluded from LT. 47,131
The concept of “downstaging” (or perhaps better “downsizing”) refers to the treatment of an ideal LT candidate with HCC beyond Milan criteria by LDT, specifically to meet acceptable listing criteria for LT. 49 A recent systematic review of 12 studies showed heterogeneity in baseline tumor burden, waiting time, downstaging protocols, and measures of treatment response. The UCSF group has used a downstaging strategy in 3 groups of patients: (1) single HCC lesion >5 and ≤8 cm, (BCLC stage A), (2) 2 to 3 HCC lesions, at least one >3 and ≤5 cm with total tumor diameter ≤8 cm, and (3) 4 to 5 HCC lesions, each ≤3 cm with total tumor diameter ≤8 cm (both BCLC B). 50 Successful downstaging was reported in 65.3% of the patients, leading to LT in approximately half of the patients after a mean of 10 months. Five-year ITT OS on patients undergoing downstaging was 56% versus 63% in patients within Milan criteria. Although the dropout rate was greater among downstaged patients, the recurrence rate of HCC was similar. Neither ITT nor DFS differed between the 3 groups. 51
The use of living donor LT for patients with HCC is controversial. Some reports describe a higher risk of HCC recurrence after living donor LT compared to deceased donor LT, 132 -134 while others describe no difference. 135 -139 Significant differences between the 2 procedures may explain these results. First, waiting time is shorter among patients with HCC undergoing living donor LT. Currently, patients with HCC have a mandatory waiting time of 6 months before acquiring MELD exception points, in the United States. As mentioned before, this may help to identify patients with an unfavorable biological profile due to the progression of HCC or the appearance of new lesions. It is possible that offering living donor LT to patients with recently diagnosed HCC may not allow such observation period, leading to LT of unfavorable HCC. Second, LDT while awaiting deceased donor LT may contribute to a better control of the disease and improve survival. Third, the need to preserve the distal hilar structures and the inferior vena cava in living donor LT may increase the possibility of tumor capsule violation or tumor dissemination through the hepatic veins, leading to a suboptimal oncological operation. Fourth, the partial liver allograft in living donor LT undergoes regeneration early after reperfusion in the recipient. Because HCC may have an enhanced growth rate and increased risk of venous invasion in the setting of partial hepatectomy corresponding to the size of the LR, 140,141 theoretically, microscopic extrahepatic seeding of HCC may happen after living donor LT. In a systematic meta-analysis of 16 heterogeneous studies, similar OS were found between living donor and deceased donor LT (hazard ratio [HR]: 0.97; 95% CI: 0.73-1.27; P = .808), and a lower DFS after living donor LT (HR: 1.59; 95% CI: 0.73-1.27; P = .041). 142
Many Asian centers with limited deceased donor allografts offer living donor LT to patients with HCC using center-specific selection criteria. In Korea, under the National Insurance coverage, living donor LT can be offered to any patient with HCC without distant metastasis, even in the presence of macroscopic vascular invasion. 143 Insurance coverage for LT for HCC in Japan is limited to patients who fulfill the Milan criteria, but each center developed expanded selection criteria based on institutional and regional experience, 144 like the University of Tokyo, reporting a 5-year OS of 75% after living donor LT among patients with HCC having up to 5 nodules, none >5 cm (5-5 rule). 46 The experience in these countries demonstrates that living donor LT can be offered to patients with HCC even beyond Milan criteria, by following the same principles used in deceased donor LT: selection, observation (after LDT), and LT.
Liver Resection for Intermediate Stage B HCC
A meta-analysis of 9 studies including 4958 patients with BCLC B HCC reported greater 3- and 5-year OS after LR compared to TACE. All studies included in this meta-analysis were from countries with high HBV prevalence (China, Taiwan, and South Korea), and all but 1 study were nonrandomized and retrospective. 52 In the randomized trial comparing LR and TACE among patients with BCLC stage B HCC, median OS was 41 months after LR, compared to 14 months after TACE. 53 Whether or not improved TACE techniques will affect outcome will require further study. 145 Combination of LR and ablative therapies, either simultaneous or sequential, have had variable success. 54 -61
In an attempt to further stratify the risk in BCLC stage B lesions, Wada et al 62 have proposed 3 subtypes: type 1, up to 3 lesions <5 cm; type 2, up to 3 lesions ≥5 cm or 4 nodules of any size, and type 3, >4 nodules. Patients undergoing LR for type 1 HCC had greater 5-year OS than patients with type 2 HCC who in turn had greater OS than patients with type 3 HCC after LR. Histopathology of resected HCC showed that 60% of patients with type 1 and >90% of patients with type 2 had microscopic, intrahepatic metastases. Among patients with type 3 BCLC B HCC, LR was not curative, unless the incident HCC was controlled with LDT, and no new nodules appear during follow-up. 62 This finding highlighted the need for LDT in these patients as a means of assessing disease biology. Fan et al 63 reported 360 patients with unresectable HCC at diagnosis who underwent TACE for intended downstaging before LR. Only 65 patients became resectable and underwent a salvage operation. The 5-year OS for these patients was 56.0%.
Barcelona Clinic Liver Cancer Stage C
Patients with HCC and vascular invasion, lymph nodes metastases, distant metastases, and/or PS 1 to 2 are designated as BCLC stage C. The indication of surgical therapy for patients with BCLC stage C has been widely evaluated. Reports on the experience of LR and, particularly, LT on such patients have been followed by criticism. 146 A multi-institutional study including North American, European, and Asian centers reported a 5-year OS of 38% and DFS of 18% for select patients who underwent LR for BCLC stage C. Torzilli et al reported 30- and 90-day mortality of 2.5% and 3%, respectively. Reportedly, major morbidity was similar to that observed among patients with BCLC 0 and A. 147 A recent propensity score–matched analysis in Japan showed OS benefit with LR among patients with portal vein tumor thrombus, provided that it is limited to a first-order branch. 69 Current AASLD/EASL recommendations for these patients are limited to medical treatment with sorafenib, which has been shown to provide an OS benefit in patients with HCC who are not candidates for any other therapies. Sorafenib is associated with stabilization of the disease but rarely with objective tumor response. 66 Sorafenib, either as neoadjuvant or as adjuvant therapy after LR or LT, has not proven beneficial in prospective studies. 148,149
Advanced Stage HCC (Stage D)
Patients with HCC and PS 3 to 4 and/or CP class C (not candidates to LT) are classified under BCLC stage D. In this stage, only supportive medical management is indicated. Child-Pugh class C patients who are good candidates for LT could be transplanted using their biological MELD score, without the need for MELD exception points. As liver function may be further deteriorated by LDT, these patients can only be transplanted if they fall within the center’s criteria at diagnosis.
Special Circumstances
Infiltrative HCC
Infiltrative HCC is an uncommon morphologic form of HCC (5% to 13%) that is not specifically incorporated into the BCLC staging classification. Imaging fails to reveal a discrete lesion in 42.7% of patients with infiltrative HCC, whereas portal vein tumor thrombus is found in 68% to 100%, often affecting both extra- and intrahepatic branches. 150 Infiltrative HCC is best differentiated from the surrounding liver parenchyma on diffusion-, T1-, and T2-weighted magnetic resonance images than on dynamic contrast-enhanced images. 151 Because current imaging cannot reliably delineate the exact tumor burden in these cases, frequently biopsy is required (or even random biopsies of the suspicious area) to establish the diagnosis. Stage at diagnosis is frequently advanced and OS is poor, even among patients undergoing screening. Radiologic assessment of the response to LDT in these patients is similarly limited. Infiltrative HCC is seldom an indication for LR. 152 Among patients with HCC beyond Milan criteria who are candidates for LT, infiltrative HCC is a predictor of failure to downstage to Milan criteria (0% vs 90% for noninfiltrative HCC).
Hepatocellular Carcinoma in Normal Livers
Data on surgical management of patients with normal livers and HCC are anecdotal. The exact pathogenesis of HCC in a normal liver remains unclear, although they could develop from a preexisting liver adenoma. 153 The incidence peaks on the fourth decade of life, earlier than HCC in patients with cirrhosis. Screening in the general population is not justified, except for males above 40 years and females above 50 years with known active chronic HBV infection. Liver resection is not always feasible despite normal parenchyma and liver function. Multiple centers have reported their experience with LR on patients with normal livers and HCC, showing greater 5- and 10-year OS and DFS than those observed among patients with cirrhosis. 154 -159 Pediatric patients without cirrhosis undergoing LT for HCC beyond Milan criteria have been shown to have excellent outcomes. 64 However, the outcome in adult patients is heterogeneous. A recent multi-institutional European study showed size is not a predictor of OS after LT in these patients. Five-year OS of 59% can be achieved among patients with no macrovascular invasion, lymph node metastases, or distant metastases. Patients with liver-only HCC recurrence of more than 12 months after initial LR may be candidates for SLT. 65
Summary and Future Directions
As the incidence and detection of HCC increase worldwide, its surgical management continues to evolve. Improved outcomes lead to more liberalized patient selection for both LR and transplantation. Larger well-designed prospective studies with long-term follow-up are needed to test whether these single-center results could be repeated prior to changing current guidelines. Ideally, tumor biology, rather than its surrogates (size, number, or growth rate of the HCC), will be used in the future for these studies.
Footnotes
Authors’ Note
No significant relationships exist between the authors and the companies/organizations whose products or services may be referenced in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.