
Abstract
Objectives
The objective of our study was to investigate and compare the epidemiologic characteristics, prognostic factors, and survival between hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma (ICC) patients.
Methods
Age-adjusted incidence rates were evaluated from 1975 to 2016 using the Surveillance, Epidemiology, and End Results (SEER) database. Overall survival (OS) was investigated using the Kaplan–Meier method and log-rank test. Univariate and multivariate Cox regression analyses were performed to identify the independent prognostic factors for OS.
Results
In the last 10 years, the incidence rate of ICC increased rapidly by 109% (annual percentage change (APC) = 8.24, 95% CI = 6.64 to 9.86; P < .001), compared with a much more modest 12% increase in the incidence of HCC (APC = 1.59, 95% CI = .56 to 2.62; P < .001). This trend persisted throughout the study across different age groups, sexes, and races. Males older than 70 years and of other races (non-African American and non-Caucasian) showed the highest incidence rates of HCC and ICC. Multivariate Cox regression analysis demonstrated that other race, married status, later year of diagnosis, more examined lymph nodes, and surgery were significant protective factors of OS in HCC patients. In contrast, the race and year of diagnosis were not independent prognostic factors, but radiation and chemotherapy were protective factors of OS in ICC patients. The median OS was 18 months and 12 months in HCC and ICC patients, respectively.
Conclusion
In the last 10 years, the incidence of HCC had a slow growth in the United States, whereas ICC showed a remarkable increase. The 5-year OS of the former has improved in recent years while that of the latter showed no significant improvement. Therefore, surgery could contribute to superior survival outcomes as compared to other treatments.
Introduction
Primary liver cancer (PLC), a rising public health concern, is the third most lethal malignancy worldwide, according to the GLOBOCAN 2020 database (https://gco.iarc.fr). Primary liver cancer includes 2 main histologically distinct subtypes, hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma (ICC), accounting for 75–85% and 10–15% of the malignancies confined within the liver, respectively. 1
Recently, several studies have been conducted on the incidence and mortality rate of PLC, which has been rising rapidly worldwide.2,3 In the past few decades, the incidence of PLC has increased remarkably in the United States, and according to this trend, the incidence is anticipated to continue rising in the coming decades.4-6 The increased incidence of HCC is mainly attributed to the associated risks such as hepatitis B virus (HBV), hepatitis C virus (HCV), 7 alcohol abuse, 8 obesity and diabetes. 9 On the other hand, the etiology and pathogenesis of ICC remain unclear, especially in Western countries. 10 Hence, no specific or explicit risk factors have been validated to be associated with an increased incidence of ICC.
Hepatocellular carcinoma and ICC share some common clinical characteristics and are easily prone to misdiagnosis. 11 However, they are histologically and biologically heterogeneous.12,13 Thus, there are significant differences in the clinical diagnosis, treatment, and prognosis between them. Therefore, the complicated clinical features in combination with the high incidence and unfavorable prognosis of these two subtypes underscores the fact that analyzing and comparing the various biographic, demographic, and clinical variables between the two subtypes is of great significance.
Traditional tumor-node-metastasis (TNM) staging system is performed for tumor classification based on the anatomic extent of the cancer lesion. Generally, this staging system possesses crucial guiding value for establishing treatment strategies and assessing the prognosis in the clinic. 14 However, its practical application in PLC patients is not satisfactory owing to the heterogeneity of patient backgrounds. Consequently, it is essential to consider demographics, clinicopathological characteristics, and treatment characteristics to predict the survival. Furthermore, univariate and multivariate Cox proportional hazard regression models could effectively evaluate the potential prognostic factors and assist in the early diagnosis and clinical decision-making accordingly in the population at large.
Therefore, in this retrospective study, we used the Surveillance, Epidemiology, and End Results (SEER) database to investigate the incidence trends of HCC and ICC between 1975 and 2016 in the United States. As it is based on a large population, the SEER database is valuable for exploring rare tumors such as ICC. Additionally, we compared the demographics, clinicopathological characteristics, and treatment characteristics between the two subtypes of PLC to identify the distinguishing variables and reduce the possibility of misdiagnosis. Additionally, we attempted to gain insight into the predictive factors that influence the prognosis of HCC and ICC, and offer accurate clinical decisions in routine practice via univariate and multivariate Cox proportional hazard regression models. Furthermore, we investigated the trends of the 5-year overall survival (OS) of the HCC and ICC patients diagnosed from 2004 to 2012 and evaluated the effect of the three main therapeutic methods of surgery, radiation, and chemotherapy on the 5-year OS.
Materials and Methods
Database and Case Selection
The retrospective data used in this study were obtained from the National Cancer Institute’s SEER program. The database covers 9.1 million cases diagnosed with different types of cancers, representing approximately 28% of the United States population. Our study included the data of patients diagnosed between 1975 and 2016 to assess the trends of PLC incidence by pathological type, including the primary site of PLC (HCC or ICC), age, sex, ethnicity, and stage according to SEER historical staging. We included all patients diagnosed with HCC and ICC using the age-mandated eligibility criteria in the SEER 18 Registries, Nov 2018 Sub (1975–2016 varying). We signed the SEER database-use agreement, and we were provided with a license to access the SEER information (accession username: 14820-Nov2019). As the information in the SEER database is publicly accessible for use in relevant medical research globally, the present study was exempt from the requirement to obtain local institutional review board oversight.
Patients diagnosed with HCC were identified using the primary site code “C22.0” for the liver and International Classification of Diseases for Oncology-3rd edition (ICD-O-3) histology/behavior codes “8170/3,” “8171/3,” “8172/3,” “8173/3,” “8174/3,” and “8175/3” for HCC. Intrahepatic cholangiocarcinoma was identified using the primary site code “C22.1” for the intrahepatic bile duct and ICD-O-3 histology/behavior codes “8032/3,” “8033/3,” “8041/3,” “8050/3,” “8070/3,” “8071/3,” “8140/3,” “8141/3,” “8160/3,” “8260/3,” “8480/3,” “8481/3”, “8490/3,” and “8560/3” for cholangiocarcinoma. 15 The age during diagnosis of patients was ≥18 years. Patients who met any of the following criteria were excluded from the study: (I) unknown survival time or survival time <1 month; (II) unavailability of follow-up information including race, marital status, and TNM stage; (III) multiple primary tumors; and (IV) diagnosis at autopsy or without positive histologic results. In total, 77 674 patients diagnosed between 2004 and 2015 were initially screened from SEER 18 Registries. Unknown survival time or survival time <1 month (n = 11 633), unavailability of follow-up information including race, marital status, and TNM stage (n = 16 982), multiple primary tumors (n = 8854), diagnosed at autopsy or without positive histologic results (n = 16 762) were omitted. Finally, a group of 23 443 patients diagnosed with either HCC or ICC, who met the inclusion criteria and were diagnosed between 2004 and 2015 according to the detailed 6th edition of the American Joint Committee on Cancer (AJCC 6th edition) TNM staging information, were selected to evaluate the prognosis factor of HCC and ICC. Additionally, data of 16 277 patients with HCC or ICC, who met the criteria and were diagnosed between 2004 and 2012 (excluding patients from 2013 to 2015, n = 7166), were collected to assess the 5-year OS trends.
Statistical Analysis
We used SEER*Stat version 8.3.8 to calculate the incidence rates via age-adjusted to the United States standard population of 2000. Incidence rate were further classified based on the primary site, sex, ethnicity, and TNM stage according to different historical staging. Pearson chi-square tests were used to analyze and compare categorical variables between the HCC and ICC patients. The main outcome assessed was OS, which was estimated using the Kaplan–Meier method. The log-rank test was used to compare the OS between the HCC and ICC patients. Variable significantly influencing survival in the univariate analysis were further estimated using a multivariate Cox proportional hazards model. We tested the proportional hazard assumptions for the Cox models before we started the Cox regression analysis. All variables conformed to the hypothesis test.
For all the statistical tests, two-sided P-values <.05 were considered statistically significant. The Pearson chi-square test and Cox proportional hazards model were performed using SPSS Statistics, version 23 (IBM Corp). Nonlinear regression was performed using GraphPad Prism_7.0. The Kaplan–Meier method was performed using the package of survminer and survival in R version 3.6.3 (R Foundation for Statistical Computing).
Results
Incidence Trends
General incidence trend
Forty-two-year incidence trends for HCC and ICC are described in Figure 1. The age-adjusted incidence rates of both HCC and ICC have increased over the last 4 decades. The incidence rate of HCC increased by approximately 3.10-fold from 1.57 per 100 000 in 1975 to 6.43 per 100 000 in 2016 (annual percentage change [APC] = 4.20, 95% confidence interval [CI] = 3.97 to 4.43; P < .001). Likewise, the incidence rate of ICC increased by almost 3.38-fold from .32 per 100 000 in 1975 to 1.40 per 100 000 in 2016 (APC = 3.47, 95% CI = 2.97 to 3.97; P < .001). Whereas, in the last 10 years, the incidence rate of ICC increased rapidly by 109% from .67 per 100 000 in 2007 to 1.40 per 100 000 in 2016 (APC = 8.24, 95% CI = 6.64 to 9.86; P < .001). In contrast, the incidence rate of HCC increased by 12% from 5.72 per 100 000 in 2007 to 6.43 per 100 000 in 2016 (APC = 1.59, 95% CI = .56 to 2.62; P < .001). Age-adjusted incidence of hepatocellular carcinoma and intrahepatic cholangiocarcinoma, 1975–2016.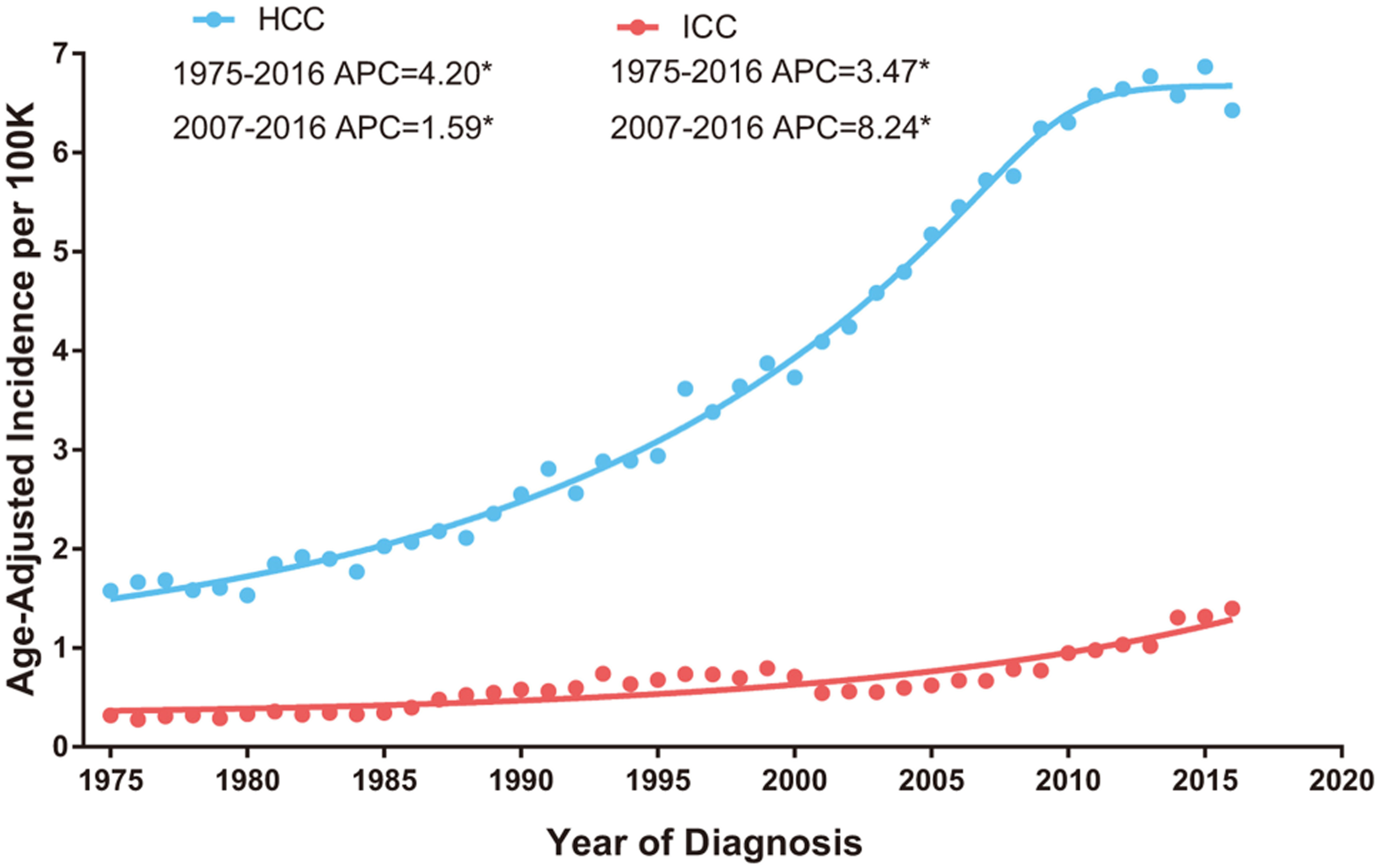
Gender, Race and Age Distribution
In addition to the general incidence trends of HCC and ICC, we further investigated the incidence trends of these two pathological types of PLC according to the demographic characteristics of the patients during the study period. The median age at diagnosis of HCC patients was significantly younger than that of the ICC patients since1981 (Figure 2A). Remarkably, the median age of the HCC patients showed a decreasing trend since the 5-year period from 1991 to 1995 and remained at a lower level than that of the previous periods. In contrast, although the median age of ICC had declined since the 5-year period from 1996 to 2000, the age level was not lower than that of the previous 5-year period from 1991 to 1995 (Figure 2A). In total, 36.81% of the diagnosed HCC patients were younger than 50, as compared to the 25.98% of ICC patients. In contrast, 47.5% of the diagnosed ICC patients were diagnosed older than 70 whereas only 32.3% of HCC patients were above that age (Figure 2B). The incidence of ICC cases showed an increasing tendency for each age group between 1975 and 2016. Furthermore, the increasing trend of ICC was statistically more evident in those younger than 50 (APC = 4.00, 95% CI = 3.23 to 4.78; P < .001) than in those aged 50–69 years (APC = 3.87, 95% CI = 3.33 to 4.42; P < .001) or older than 70 (APC = 3.12, 95% CI = 2.43 to 3.82; P < .001) (Figure 2D). Nevertheless, the incidence of HCC in those younger than 50 increased from 1975 to 2006 (APC = 5.99, 95% CI = 5.33 to 6.65; P < .001) but declined from 2007 to 2016 (APC = −5.33, 95% CI = −7.34 to −3.27; P < .001). Although the incidence trend of HCC continued to show an increase in patients aged 50–69 years and older than 70 from 2007 to 2016, it had slowed down obviously as compared to the previous period (Figure 2C). Age distribution of HCC and ICC. (A): Median age at diagnosis by era. (B): Percentage of patients diagnosed with HCC or ICC within the indicated age range. (C): Temporal trends in age-adjusted incidence rates of HCC by age. “Younger than 50” vs “50–69 years,” P value was less than .001; “younger than 50” vs “older than 70” P value was less than .001; “50-69 years” vs “older than 70,” P value was less than .001. (D): Temporal trends in age-adjusted incidence rates of ICC by age. “Younger than 50” vs “50-69 years,” P value was .001; “younger than 50” vs “older than 70,” P value was .249; “50-69 years” vs “older than 70,” P value was less than .001.
The incidence rates of both HCC and ICC were higher in males than in females (Figure 3A and 3B). Furthermore, this founding was more significantly higher in the HCC patients than in the ICC patients. Additionally, among the HCC patients, the increasing trend was more evident in males (APC = 4.12, 95% CI = 3.88 to 4.37; P < .001) than in females (APC = 3.78, 95% CI = 3.54 to 4.03; P < .001). On the other hand, it was less evident in males (APC = 2.81, 95% CI = 2.24 to 3.39; P < .001) than in females (APC = 4.03, 95% CI = 3.49 to 4.57; P < .001) among the ICC patients. Age-adjusted incidence trends over time of HCC. Trends shown according to (A) sex (male vs female, P value was .037) and (C) race (white vs black, P value was less than .001; white vs other, P value was less than .001; black vs other, P value was less than .001). Age-adjusted incidence trends over time of ICC. Trends shown according to (B) sex (male vs female, P value was less than .001) and (D) race (white vs black, P value was .339; white vs other, P value was .008; black vs other, P value was .106).
Among the diverse racial groups comprising whites, blacks, and other races, the incidence rate in the other races subgroup was the highest for both HCC and ICC (Figure 3C and 3D). The incidence in the blacks was moderately higher than that in the whites among the HCC patients, but it did not differ significantly between them in the ICC patients. Notably, the increasing trend of HCC and ICC was more evident in the whites (APC = 4.56, 95% CI = 4.32 to 4.79; P < .001 and APC = 3.41, 95% CI = 2.89 to 3.94; P < .001, respectively) and the blacks (APC = 3.89, 95% CI = 3.51 to 4.27; P < .001 and APC = 3.46, 95% CI = 2.47 to 4.46; P < .001, respectively) than in the other races (APC = 1.31, 95% CI = 1.03 to 1.59; P < .001 and APC = 2.65, 95% CI = 1.96 to 3.34; P < .001, respectively).
Stage Distribution
To investigate the influence of pathologic characteristics on the incidence further, we examined the trend in the four stage groups. HCC was diagnosed more frequently in the early stage whereas ICC was diagnosed more frequently in the advanced stage (Figure 4A). Limiting the number of patients with definite staging information between 2004 and 2015, the proportion of HCC patients diagnosed with stage I or II was more than that of the ICC patients (59.30% vs 30.78%). Furthermore, the increasing trend of HCC was more evident in the stage I patients (APC = 6.86, 95% CI = 5.76 to 7.97; P < .001) than in the other stages. In contrast, the increasing trend of ICC showed the most rapid growth in the stage IV patients (APC = 10.93, 95% CI = 8.10 to 13.83; P < .001) among all the stages. (A) Stage distribution of HCC and ICC, 2004–2015. (B) Age-adjusted incidence trends over time of HCC by stages (2004–2015). (C) Age-adjusted incidence trends over time of ICC by stages (2004–2015).
Survival Analysis
Baseline characteristics
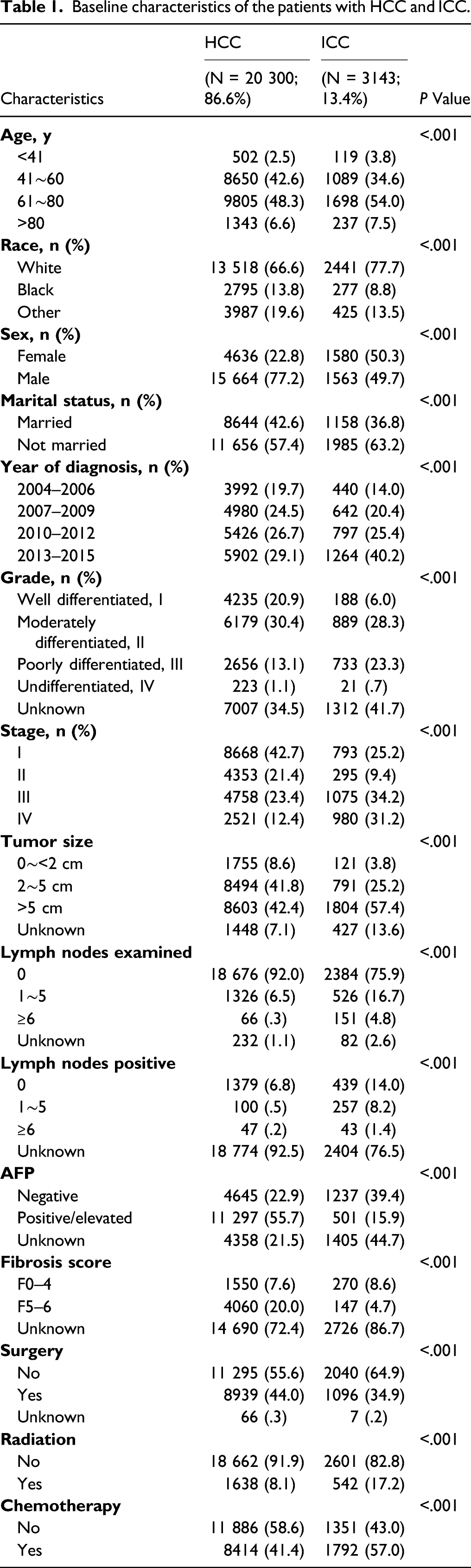
Baseline characteristics of the patients with HCC and ICC.
Prognostic factors
Variables associated with overall survival according to the Cox proportional hazards regression model.

Median OS of HCC and ICC.

Five-year OS
The OS of patients diagnosed with HCC was significantly better than that of patients with ICC (Figure 5A). The 5-year OS rate of the HCC and ICC diagnosed from 2004 to 2012 are shown in Figure 5B. A large improvement in the 5-year OS was observed in the HCC patients from 21.99% in 2004 to 29.85% in 2012. However, there was no significant improvement in the 5-year OS in the ICC patients, which fluctuated in the range of 11–16%. Furthermore, we investigated the impact of surgery, chemotherapy, and radiation on the 5-year OS. The OS of the HCC patients undergoing surgery showed an obvious improvement from 37.31% in 2004 to 56.40% in 2012, while those not undergoing surgery showed a modest improvement during our study period (Figure 6B). Notably, the 5-year OS of HCC patients who underwent surgery present an approximate benefit of 40% as compared to those who did not (A) Kaplan–Meier survival curves for patients with HCC and ICC from 2004–2015. (B) Trends in 5-year overall survival for patients with HCC and ICC from 2004–2015. Overall survival for patients with HCC stratified by (A) surgery as treatment, (E) radiation as treatment, and (I) chemotherapy as treatment. Trends in 5-year overall survival for patients with HCC stratified by (B) surgery as treatment, (F) radiation as treatment, and (J) chemotherapy as treatment. Overall survival for patients with ICC stratified by (C) surgery as treatment, (G) radiation as treatment, and (K) chemotherapy as treatment. Trends in 5-year overall survival for patients with ICC stratified by (D) surgery as treatment, (H) radiation as treatment, and (L) chemotherapy as treatment.

Discussion
This study cohort included patients with two main histologically distinct subtypes of PLC from the SEER database and demonstrated a persistent increase in the incidence of HCC and ICC in the United States from 1975 to 2016. Although it is well acknowledged that the incidence of ICC has increased worldwide,16-18 our study confirmed the veracity of this finding on the basis of the expanding data analysis comprising patients diagnosed up to 2016. Notably, our study points out that the incidence rate of ICC increased rapidly by 109% in the last 10 years as compared to a much more modest increase of 12% in the incidence of HCC.
The reasons for the apparent increase in ICC incidence, especially in the past decade, have not been clearly clarified. Saha et al. revealed that the improved diagnosis of cancer cases that would previously have been classified as cancer of unknown primary (CUP) origin may have contributed to the increase in the number of ICC cases reported. 19 Great advances in diagnostic technology such as imaging diagnosis, histological examination, and molecular diagnostics, are probably a crucial cause for this increasing trend. 20 However, Shaib et al. demonstrated that improved diagnostic technology could not adequately explain the increased incidence of ICC due to an absence in the shift toward increasing diagnosis of ICC at a younger age and more frequently in females in the period from 1975 to 1999. 17 Compared to the relatively short study period of the previous study, our study expanded the study period from 1975 to 2016 to observe the overall incidence of ICC more objectively. According to our study, the proportion of patients with HCC and ICC aged younger than 50 increased from 1975 to 2016 as compared to the patients aged 50–69 years and older than 70. We also found that the incidence of ICC in woman showed a more remarkable increase than that in men from 1975 to 2016, although the incidence rate in the latter was only slightly higher than that in the former. Furthermore, the median age of ICC patients at diagnosis declined since 2000. Therefore, it is reasonable to presume that improved diagnostic technology may be a critical factor accounting for the increased reported incidence of ICC. However, there is insufficient scientific evidence to prove the role of improved diagnostic technology. 21
Unlike ICC, the incidence trend of HCC over the last few decades has apparently slowed down when compared with the past four decades. The implementation of chronic HBV vaccination and HBV antiviral therapy might have reduced the incidence rate of HBV-related HCC worldwide, especially in the Western Pacific regions.22-24 It was reported that HBV vaccination contributed to an estimated 83% reduction in the number of new HBV infections (310 million cases) between1990 and 2020.25,26 We found that the incidence rates of HCC in patients aged younger than 50 years has declined in the last 10 years. Effective prevention of viral hepatitis transmission (such as single-use parenteral injection systems) and HBV vaccination have resulted in low viral hepatitis-HCC in the Western countries.27,28 Nevertheless, the burden of metabolic syndrome gradually emerged as a prominent etiology of HCC in the United States.29-31 Consistent with the results of previous studies, we found that unlike the incidence of ICC, the HCC incidence rate showed an obvious disparity in diverse racial groups and sexes in the United States. Although the highest incidence was reported in males from other ethnic backgrounds, the increase in incidence in the white racial group was the highest, followed by the black and other racial groups. Consequently, HBV vaccination and enhanced management of public health have remarkably reduced the incidence of HCC; however, the non-infectious factors should be given more attention.
It is universally recognized that HBV or HCV infection and metabolic syndrome could cause decompensated cirrhosis, which may eventually lead to HCC. 32 Unlike HCC, the etiology of ICC remains largely unknown as it may occur even without cirrhotic liver or viral infection. 33 However, previous studies have suggested that HBV or HCV infections and liver cirrhosis are associated with an upward trend of ICC incidence. 34 Parasitic infections (e.g., Clonorchis sinensis) occur frequently in Southeast Asia, which is an important cause of the high incidence of ICC in these regions. 35 The migration of the infected population from these areas to the United States could explain the higher incidence in the other racial groups as compared to the white and black racial groups in our study.
For survival analysis, we adopted a cohort of 20 300 HCC patients and 3143 ICC patients diagnosed between 2004 and 2015. Consistent with previous studies, the demographic and clinicopathologic characteristics of the HCC patients such as age, sex, marital status, degree of differentiation, and stage showed a significant prognostic impact. The male patients were more vulnerable to both HCC and ICC as compared to the female patients, which is consistent with the findings of previous studies. It was reported that estrogen deprivation resulted in a decrease in the interleukin-6 production by the peripheral blood mononuclear cells, which reduced the protective effect toward age-related diseases. 36 This result partly explains the relatively high incidence rate of HCC and ICC in the males. Interestingly, individuals with HCC or ICC who were married had a benefit in survival outcomes as compared to the unmarried individuals. This could be attributed to good social support which could partly reduce the occurrence of adverse outcomes. Notably, there was a continued increase in the OS of HCC patients from 2004 to 2015, but no significant increase in that of ICC patients. This could be attributed to the missed diagnosis of ICC and subsequently the ICC patients lost the opportunity for optimal treatment. 19 According to our results, surgery remained the best treatment option to improve the OS for both HCC and ICC when compared with radiation therapy and chemotherapy. Specifically, the 5-year OS of HCC patients who underwent surgery with HCC showed an approximate benefit of 40% as compared to those who did not, and the increasing trend of the 5-year OS was more obvious in patients undergoing surgery than in those not undergoing surgery.
This study has several limitations in nature. As our study was a retrospective cohort study, there were certain unavoidable biases. Furthermore, several associated variables such as HBV or HCV infection and parasitic infections that could affect the survival were not recorded in the SEER database. The SEER database does not provide specific information on chemotherapy, including the course of the treatment and agents/drugs administered. Finally, this study focused on the United States population; hence, these results are restricted to this population and may not be generalizable to other populations worldwide. Despite these limitations, our results provided important insights regarding PLC, as well as valuable information on the incidence, prognostic factors, and survival among PLC patients based on the large number of cases in the SEER database.
Conclusion
This is the most up-to-date population-based analysis that demonstrates the incidence of the two subtypes of PLC over the past four decades in the United States. Although the study filled a crucial knowledge gap concerning recent trends in PLC, there is a lack of essential studies on the potential mechanisms underlying the increased trends in ICC in the United States. Additionally, our study summarized and compared a variety of demographic, clinicopathologic, and treatment variables that had a significant prognostic impact on the OS of patients with HCC and ICC. It might assist clinicians to accurately estimate prognosis and eliminate the restriction of the AJCC staging. Particularly, surgery, the current critical factor associated with the improvement of 5-year OS, should be recommended for HCC and ICC patients as the optimal therapeutic method in clinical practice.
Supplemental Material
sj-pdf-1-ccx-10.1177_10732748211051548 – Supplemental Material for Trends in Incidence and Prognostic Factors of Two Subtypes of Primary Liver Cancers: A Surveillance, Epidemiology, and End Results-Based Population Study
Supplemental Material, sj-pdf-1-ccx-10.1177_10732748211051548 for Trends in Incidence and Prognostic Factors of Two Subtypes of Primary Liver Cancers: A Surveillance, Epidemiology, and End Results-Based Population Study by Jiping Yao, Xue Liang, Yanning Liu and Shuangshuang Li, Min Zheng in Cancer Control
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (U20A20348, 81871646), Key R & D Projects of Zhejiang Province (2021C03039).
Ethics Approval
This study was conducted using SEER database. We have got permit for the purpose of research before study.
Informed Consent
The informed consent was not required for our study because no personal identifying information was public.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.