
Abstract
Burnout is a challenging issue among surgeons. Many factors have been linked to burnout, such as an inadequate work-life balance, high stress levels, and the frequency of on-call, overnight shifts. There is a lack of research on factors in surgeons’ daily lives associated with burnout. This study observed trauma surgeons with daily surveys assessing stress and fatigue over 9 days (6 day shifts, three night shifts). This study analyzes surgeons’ stress and fatigue levels. The study population was compared to the population of US critical care surgeons to ensure representativeness based on age, sex, and rates of burnout. Overnight shifts showed high stress and fatigue levels relative to off days, day shifts, the 3 days before, and the 3 days after overnight shifts. Days performing surgery were also more stressful and fatiguing than non-surgery work days and off days. Fatigue and stress levels were minimized during off days.
Introduction
Burnout, defined as “a work-related syndrome involving emotional exhaustion, depersonalization, and a sense of reduced personal accomplishment” (West et al., 2018), is a widely prevalent and challenging issue among physicians (Chopra et al., 2004) and especially among surgeons (Coleman et al., 2021; Dimou et al., 2016). Multiple factors have been linked to burnout (Patel et al., 2018). Through previous research, some primary factors that influence burnout are known, such as not having an adequate work-life balance (Johnson et al., 2020; Mahoney et al., 2020; Troppmann et al., 2009), high stress levels from work (Patel et al., 2018) or personal lives (Dyrbye et al., 2011), and the frequency of on-call, overnight shifts (Coleman et al., 2021; Shanafelt et al., 2009).
Most previous studies on physician and surgeon burnout or stress have been limited to a single point in time using either subjective psychological survey results or objective physiological (biometric) evaluations. Additionally, many of these studies, such as Sochacki et al. (2019), focused on surgeons over long periods (i.e., weeks or months) and observed how their feelings of burnout changed. This approach does not enable exploration of surgeons’ day-to-day lives and potential physiological and psychological drivers of burnout and stress from daily life events.
Some studies observed surgeons more granularly but were not focused on burnout specifically; for example, four studies investigated the physiological effects (heart rate variability, circadian rhythm) and performance of night shifts on surgeons (Amirian, Andersen, Rosenberg, et al., 2014; Amirian, Mortensen, Rosenberg, et al., 2014; Amirian et al., 2015) but did not attempt to associate these factors with burnout. There is a lack of research on the various factors in surgeons’ daily lives associated with burnout. Thus, we wished to analyze the subjective data from daily surveys (self-evaluations of stress and fatigue levels) over 9 days (including regular workdays and overnight shifts). Our goal was to explore the effects of shift scheduling, the number and types of stressful events, and personal factors on surgeons’ stress and fatigue levels. This preliminary work centers on stress and fatigue levels, demographic parameters (e.g., sex, age), and burnout of participating surgeons. Additionally, trends in stress and fatigue levels comparing the types of work being done (e.g., surgery work vs. non-surgery work, day shifts vs. night shifts) would set the stage for the eventual analysis of the physiological (biometric) data.
We hypothesized that overnight shifts and the frequency of days spent operating would lead to the greatest reported fatigue and stress levels.
Methods
Eight attending trauma surgeons at a Level 1 Trauma Center were enrolled, and data on demographics, burnout, and extracurricular involvement (exercise, hobbies, treatment) were collected. The surgeons were then observed for nine consecutive days (3 days before, 3 days during, and 3 days after night shifts). Demographic results of age and sex were compared with those of critical care surgeons in the US, according to the Association of American Medical Colleges’s (AAMC) (2023) report on Physician Professional data. This study was reviewed and approved by our Institutional Review Board (IRB).
Burnout was assessed using Mayo Clinic’s Well-Being Index, a survey to assess physician distress (Dyrbye et al., 2013). Surgeons were asked to answer yes or no to “During the past month, have you felt burned out from your work?” and “During the past month, have you been bothered by emotional problems (such as feeling anxious, depressed, or irritable)?” Additionally, they were asked whether they participated in any extracurricular activities. These results were compared with Medscape’s 2024 Physician Burnout & Depression Report (McKenna, 2024).
Surgeons were also asked to complete a daily “Environmental Momentary Assessment” (EMA) survey assessing stress and fatigue levels. EMAs were electronically administered at 6:00 a.m. following each night shift and at 7:00 p.m. each day of the study period (9 days). Surgeons’ responses were based on the period (12 to 36 hr, depending on scheduling between day and night shifts) between their last completed and current EMAs. Stress and fatigue levels were reported on a seven-point Likert Scale from one to seven, with one being the lowest level of stress and fatigue and seven being the highest. Surgeons were asked what their stress and fatigue levels were “currently” (at the time of completing the survey) and “since waking” (changes in stress and fatigue since they last awoke).
ANOVAs were used to compare fatigue and stress levels over specific periods and between work settings. Tables report mean ± standard deviation (when applicable). F scores and p-values for ANOVAs and effect tests for variables of interest are also reported in relevant tables; the significance level was set as a p-value of .05. Data analysis was conducted using JMP17 (SAS Institute Inc., NC, USA).
Results
Table 1 provides demographic information of our study’s sample and compares it with the US population of critical care surgeons, as reported by the Association of American Medical College (AAMC) (2023). This study enrolled five women and three men (Age: 43.5; SD = 8.2 years).
Demographic Information of Eight Participating Surgeons Compared to US Critical Care Surgeons in 2022 as Reported by the AMA.
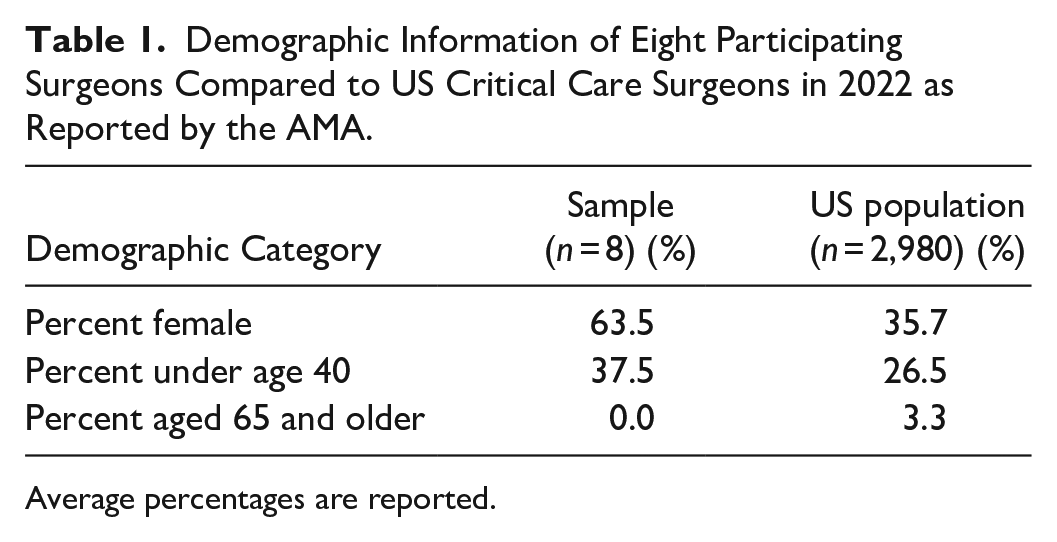
Average percentages are reported.
Table 2 presents the percentage of surgeons who experienced burnout, had emotional problems, and participated in non-surgery-related activities. These results from our sample are compared with US general surgeons, as reported by Medscape (McKenna, 2024).
Percent of Surgeons’ Burnout and Extracurricular Involvement Compared to US General Surgeons in 2023 as Reported by Medscape.
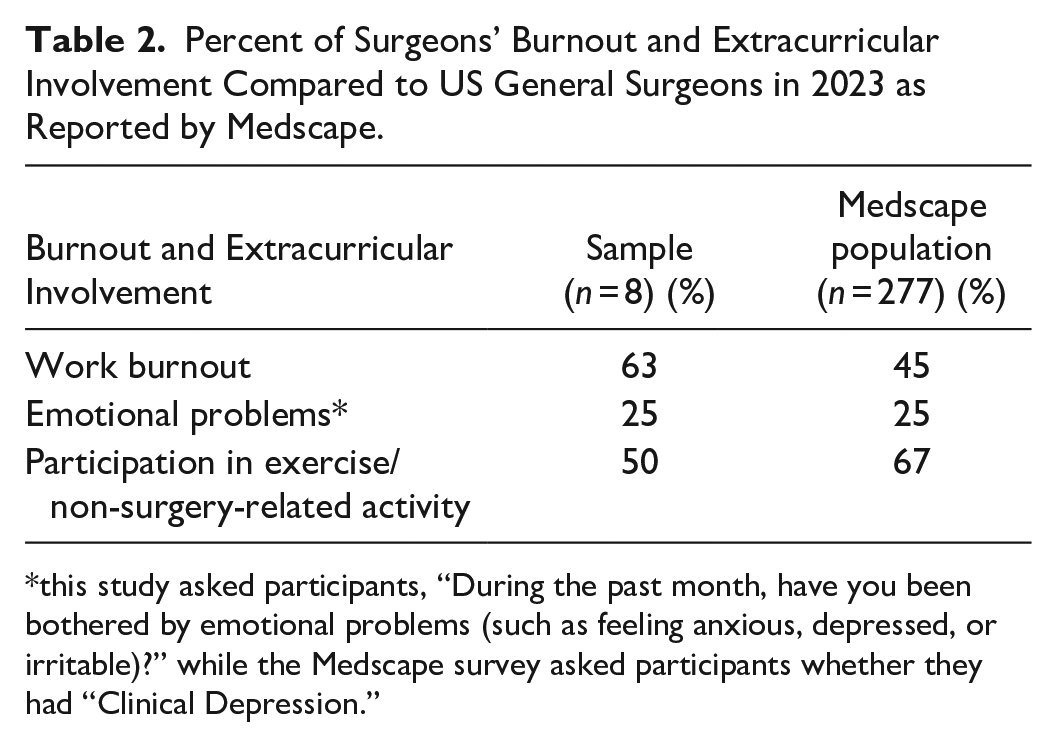
this study asked participants, “During the past month, have you been bothered by emotional problems (such as feeling anxious, depressed, or irritable)?” while the Medscape survey asked participants whether they had “Clinical Depression.”
Surgeons were also asked whether they had any chronic or recurring pain and, if so, to select specific body parts. Three of the eight (37.5%) surgeons reported having chronic/recurring pain, and all three noted pain in their right arm and lower back.
Table 3 compares off days to day shifts and night shifts. Current stress, current fatigue, and the fatigue since waking had significant ANOVAs and effect test results. Night shifts led to the greatest stress and fatigue levels in all three of these factors, while off days led to the lowest.
Mean ± Standard Deviation and Statistical Tests of Stress and Fatigue Comparing Off Days versus Day Shifts versus Night Shifts.
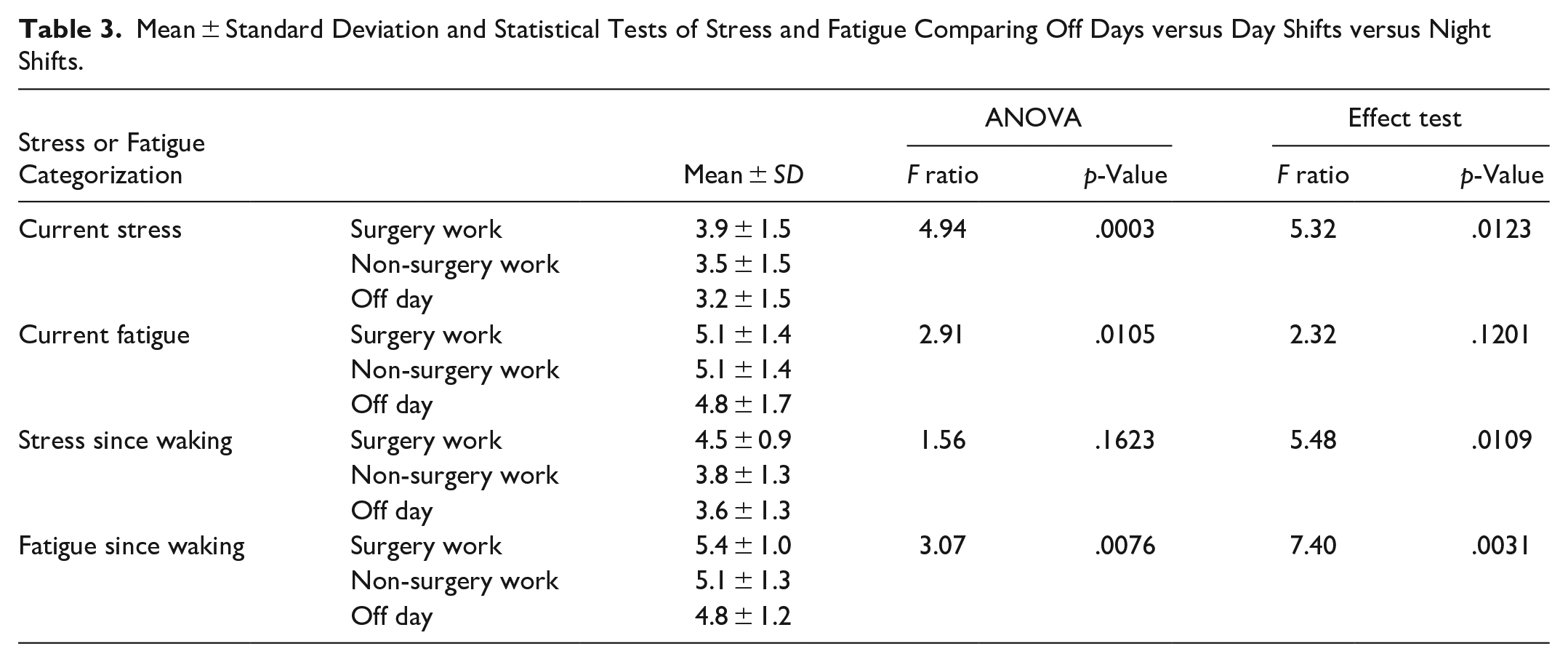
Table 4 analyzes days performing surgery to workdays without surgery and off days. Current stress and fatigue since waking were statistically significant. Days with surgery led to the highest stress and fatigue levels since waking, followed by non-surgery and off days.
Mean ± Standard Deviation and Statistical Tests of Stress and Fatigue Comparing Surgery Work versus Non-Surgery Work versus Off Days.
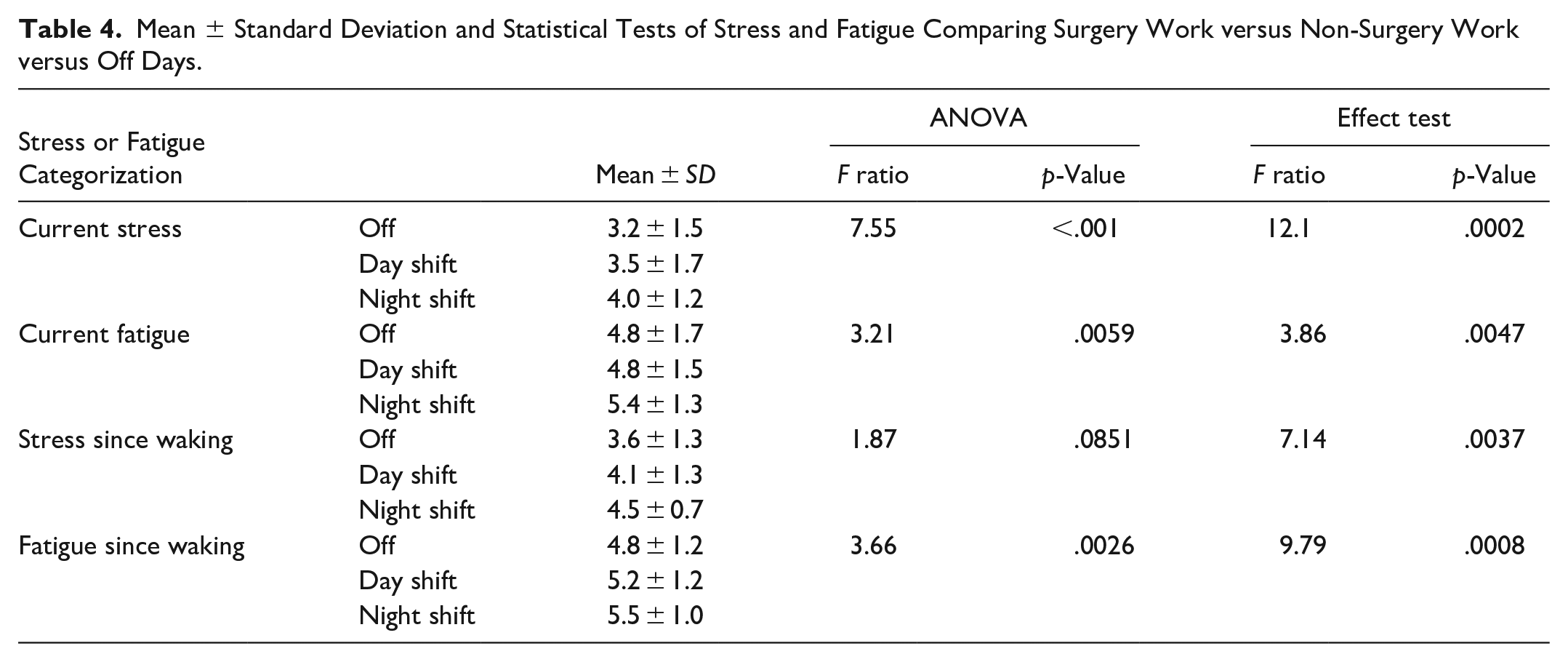
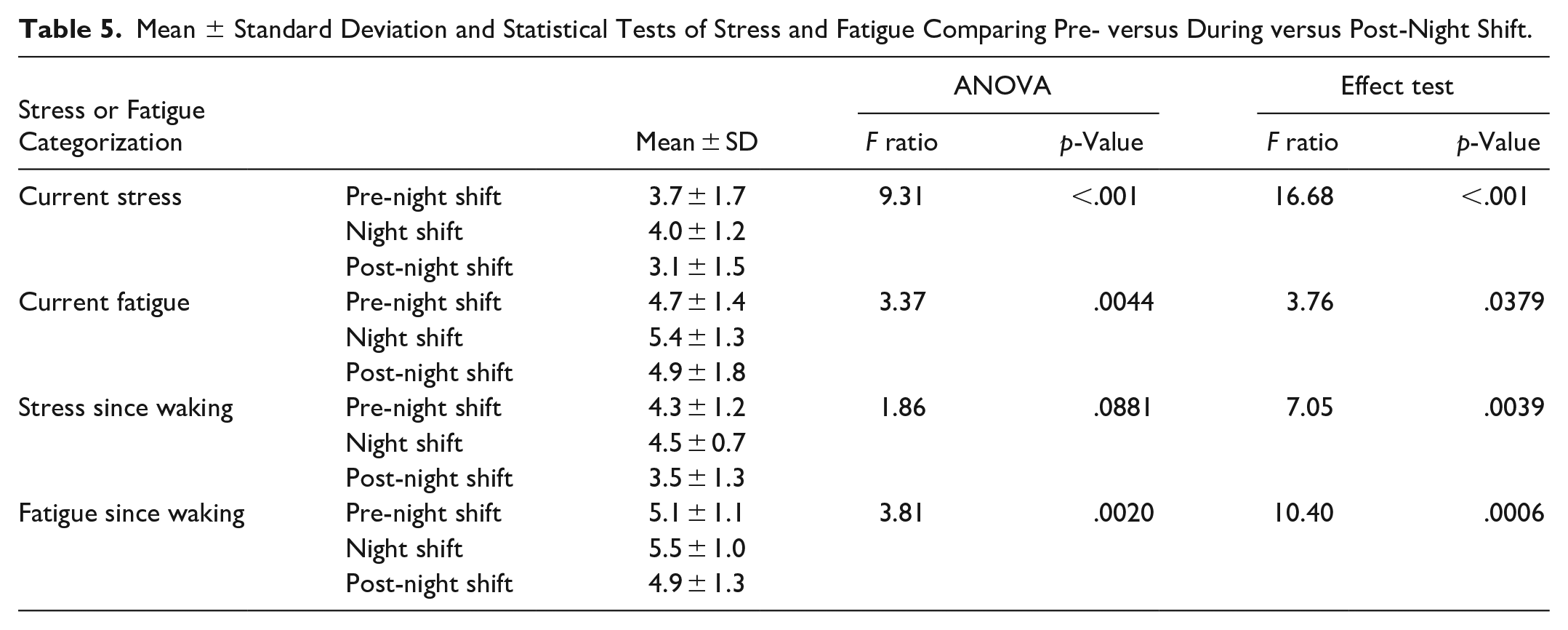
Table 5 compares the three consecutive days before, during, and after night shifts. Current stress, current fatigue, and fatigue since waking had statistically significant differences. In each case, overnight shifts maximized stress and fatigue. Current stress had greater levels pre-night shift than post. Prior to night shifts, the surgeons’ current fatigue levels were lower than post-night shift; however, fatigue since waking was lower post-night shift than pre-night shift.
Mean ± Standard Deviation and Statistical Tests of Stress and Fatigue Comparing Pre- versus During versus Post-Night Shift.
Discussion
Demographic data revealed that the surgeons’ responses were similar to those reported in previous literature, with participation in extracurricular activities, notably exercise, and age similar to those reported by critical care and general surgeons in the US. Rates of work burnout were slightly higher in our sample relative to the entire population; however, this difference between our sample and the population’s varied by less than 20%. The only demographic feature that varied by a considerable amount (>20%) was the percentage of female surgeons, with 63.5% of our sample being female, while the population only had 35.7%.
The study has several limitations, including a small sample size from a single institution, exclusion of physiologic (biometric) data, and a limited period of 9 days. Overall operating time and types of surgery performed were not assessed. Future work will include analysis of the effects of overnight shifts and the type of work performed on surgeons’ physiological (biometric) data. These results will then be compared with these subjective stress and fatigue levels.
Our preliminary study revealed statistically significant differences in stress and fatigue levels between surgery versus non-surgery days and schedules (day vs. night shifts and before vs. during vs. after night shifts). In comparing stress and fatigue levels, overnight and surgical shifts had the greatest levels of stress and fatigue, which confirmed our hypothesis. These results are logical, as performing surgeries can be physically demanding, especially considering the prevalence of chronic pain/musculoskeletal disorders. Furthermore, when combined with the difficulty of working consecutive day shifts and then having to suddenly work consecutive night shifts and perform emergent surgeries during atypical working hours, it is no surprise that stress and fatigue levels are maximal during this time. These results suggest potential opportunities for improvement in surgical shift work scheduling among trauma surgeons. The results of this study will provide a framework for further analyses of stress and fatigue levels using physiological (biometric) parameters and additional surgeon characteristics.
Footnotes
Acknowledgements
We would like to thank Lockheed-Martin’s Advanced Technology Laboratories for their financial support of their project and their involvement in conducting this study. Additionally, we would like to thank the trauma surgeons who participated in this study; this study would not be possible without their help.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by and performed in collaboration with Lockheed-Martin’s Advanced Technology Laboratories.