
Abstract
Background:
The aim of this study was to investigate the clinical and radiologic outcomes following supramalleolar osteotomy for early varus ankle arthritis with the medial translation of the talus, wherein the lateral translation of the talus center to the tibial axis was used as a correction target. Another aim was to compare the results between the ankles with a normal range of medial distal tibial angle (MDTA) and overcorrected MDTA at the postoperative period to investigate the role of overcorrected MDTA after the supramalleolar osteotomy.
Methods:
The study comprised 90 patients (93 ankles) with Takakura stage 2 or 3a varus ankle arthritis with the medial translation of the talus, which underwent medial opening supramalleolar osteotomy with fibular osteotomy, and the mean duration of follow-up was 50.7 (range, 24-84) months. Clinical assessments were done with a visual analog scale for pain and the Foot Function Index. The correction target was set at the lateral placement of the talus center to the tibial axis. Radiographic parameters, talus center migration (TCM) and tibial axis–talus ratio (TT ratio), were used to evaluate talus positioning related to the tibial axis. Two groups were established based on postoperative MDTA: a neutral group (MDTA < 94 degrees) and an overcorrected group (MDTA ≥ 94 degrees).
Results:
Postoperatively, clinical and radiographic outcomes improved in all patients (P < .01). TCM and TT ratio showed a lateral shift of the talus (TCM: from 2.0 ± 1.7 mm to −1.3 ± 1.6 mm, TT ratio: from 55.5% ± 5.4% to 44.7% ± 5.0%, both P < .01). As expected, the overcorrected MDTA group had a larger MDTA than the neutral group preoperatively (P < .01). However, there were no differences in clinical outcomes or changes in various radiographic parameters between the groups.
Conclusion:
Lateral translation of the talus center relative to the tibial axis can be used as a correction target for medial opening supramalleolar osteotomy to treat early varus ankle arthritis with medial translation of the talus. Overcorrection of the tibial plafond to valgus does not seem necessary.
Level of Evidence:
Level IV, retrospective case series study.
This is a visual representation of the abstract.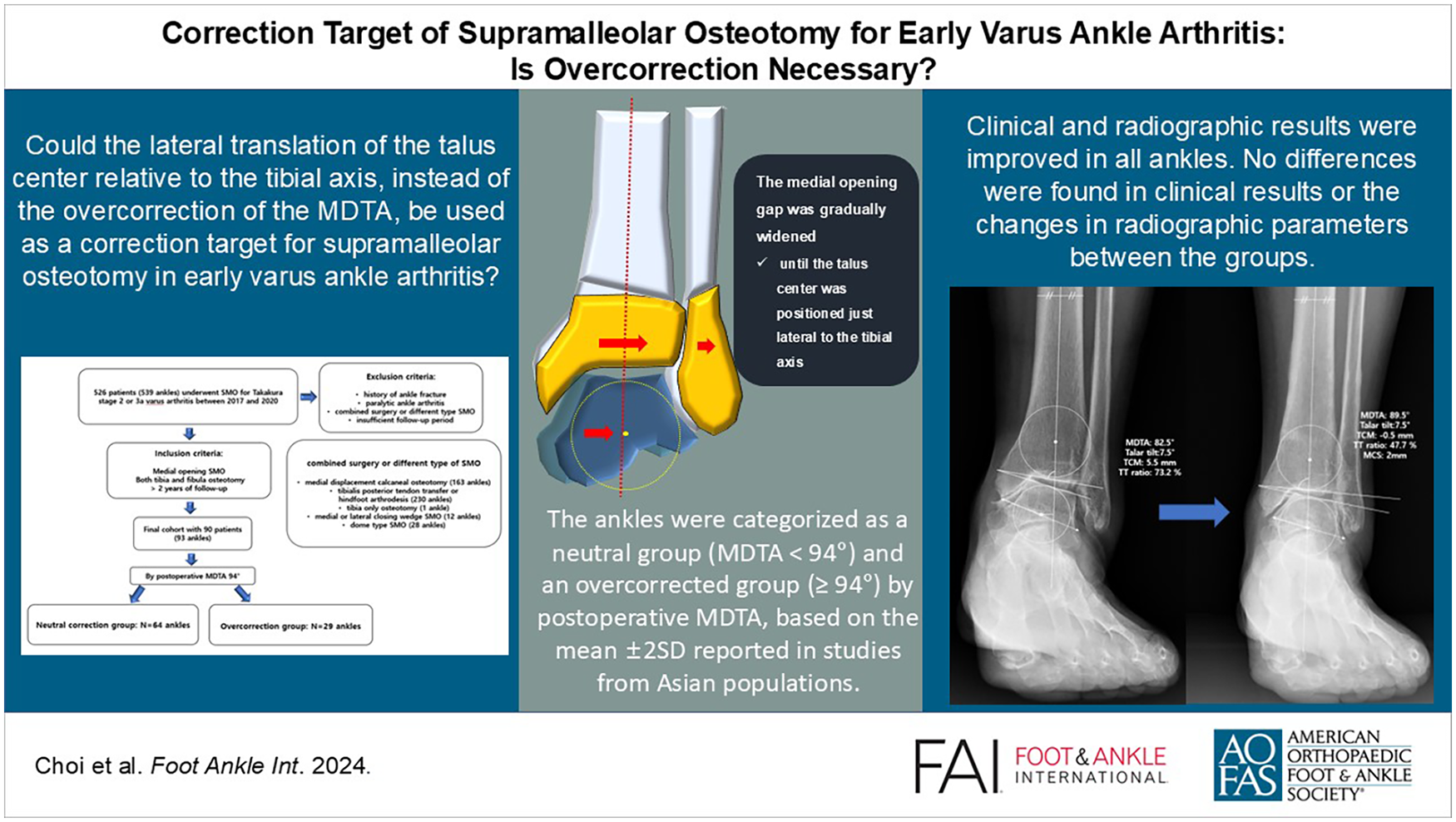
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.