
Abstract
Objective
To evaluate the outcomes of intermediate stage varus ankle arthritis treated by supramalleolar osteotomy.
Methods
Clinical data of 57 patients with varus arthritis who underwent supramalleolar osteotomy at our hospital between March 2018 and December 2019 were retrospectively analyzed. The patients were grouped according to the Takakura classification, and assessed using the American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Score and the Visual Analogue Score (VAS). Tibial anterior surface (TAS) angle and talar tilt (TT) angle were measured at the weight-bearing anteroposterior view. Tibial lateral surface (TLS) angle was measured at the weight-bearing lateral view. The differences in the above indicators of patients with different stages of varus ankle arthritis before and after treatment were analyzed.
Results
The patients were followed up for an average of 31.9 ± 5.8 months. Upon the last follow-up, the AOFAS score was 84.1 ± 9.7, the VAS score 2.2 ± 1.3, the TAS angle 92.4 ± 5.5°, the TLS angle 79.3 ± 5.3°, and the TT angle 3.7±3.4°, which were significantly different from the preoperative levels (64.2 ± 14.6, 4.5 ± 1.8, 80.5 ± 6.7°, 74.9 ± 4.6°, and 5.2 ± 64.1°, respectively) (p < .05). There were significant differences in AOFAS and VAS scores before surgery and upon the last follow-up in each group (p < .05). The postoperative TT angle was significantly different from the preoperative level in stage IIIb patients (p = .003).
Conclusions
Supramalleolar osteotomy achieved good short-to mid-term clinical outcomes for intermediate stage varus ankle arthritis. This procedure could significantly improve the TAS and TLS angles of the patients at any stage and the TT angle of stage IIIb patients.
Introduction
Ankle arthritis is a common chronic disorder that affects the ankle joint, and the most common etiology is trauma. 1 Ankle arthritis is usually combined with an abnormal alignment.2–4 The malalignment on the coronal plane is divided into valgus and varus.5–7 Varus ankle arthritis, the more common type, 8 is featured by varus angulation of the distal tibial articular surface and arthritis mainly involves the medial compartment.7,9 Varus deformity usually results in eccentric loading distribution in the intra-articular space, which further aggravates the wear and degeneration of the medial compartment.10,11 For early- and mid-stage varus ankle arthritis, joint-preserving surgery may be performed if the conservative treatments fail.
Takakura first performed supramalleolar osteotomy for the treatment of varus ankle arthritis in 1998. 6 The osteotomy shifts the weight-bearing axis laterally, thus more load is distributed on the lateral side of the dome of the talus, where there is still cartilage to protect the medial side. Through this mechanism, supramalleolar osteotomy can delay or even halt the progression of arthritis.6,12–14 For non-end-stage ankle arthritis, supramalleolar osteotomy relieves pain, and improves function restoration and the radiographic manifestations of arthritis. In addition, this procedure can delay ankle fusion or replacement.6,14–17 However, controversies still exist regarding supramalleolar osteotomy, especially in indications and validities for stage IIIb ankle arthritis. In the present study, we analyzed clinical data of patients receiving supramalleolar osteotomy for varus ankle arthritis at our hospital. The clinical and radiographic efficacy of this procedure for intermediate stage varus ankle arthritis was assessed.
Materials and methods
Inclusion and exclusion criteria
Inclusion criteria: 1. age≥18 years; 2. signed informed consent from patients; 3. varus ankle arthritis, with TAS angle <89°, medial clear space narrowing or disappearance; 4. suffering from pain and unresponsive to conservative treatment for over six months; 5. follow-up ≥1 year; and 6. no history of ankle surgery.
Exclusion criteria: 1. end-stage ankle arthritis; 2. infectious arthritis; 3. history of congenital deformity of the lower limbs and ankles; 4. neuroarthropathy; and 5. incomplete clinical or radiographic data or lost to follow-up.
General information
Clinical data of 69 patients with varus arthritis who received supramalleolar osteotomy at our hospital from March 2018 to December 2019 were retrospectively analyzed. Fifty-seven patients were finally enrolled according to the inclusion and exclusion criteria. There were 18 males and 39 females, and the average age upon surgery was 53.0±14.0 years (range, 19 - 75 years). In terms of etiology, 35 cases (61.4%) were caused by trauma, and 22 cases (38.6%) were of primary ankle arthritis.
All cases were classified using the Takakura classification system modified by Tanaka et al. 14 There were 13 cases at stage II, 30 cases at stage IIIa, and 14 cases at stage IIIb. In the present study, 31 patients underwent medial opening wedge osteotomy, 12 lateral closing wedge osteotomy, and 14 dome osteotomy.
The present study was approved by the Medical Ethics Committee of Beijing Jishuitan Hospital (approval No.:202102-08). The informed consent form was signed by all patients.
Surgical procedures and postoperative treatment
Thigh tourniquet was used, and second-generation cephalosporins were prescribed prophylactically. The patient took a supine position, with the hip on the operated side slightly higher and the patella facing upwards.
For patients with mild to moderate varus deformity (TAS >80°) and the CORA located above the ankle joints (more than 1 cm), we used the medial opening wedge osteotomy, because it’s easier and more convenient. But if the medial soft tissue might compromise after osteotomy (due to contracture or previous scars) or the deformity is severe (TAS <80°) and the CORA was above the ankle joint, we chose the lateral closing wedge osteotomy. At last, if the deformity is severe and the CORA is located near the ankle joint (less than 1 cm), we utilized the dome osteotomy for its advantages of greater power for deformity correction and ability of correcting the deformity at the CORA.
The medial approach was selected for the medial opening wedge osteotomy. If there were osteophytes on the medial side or requires for release, the joint capsule should be open. Starting at 3–4 cm above the ankle joint, a Kirschner wire was drilled towards the upper 1/3-1/2 portion of the syndesmosis. The position of the Kirschner wire was confirmed by fluoroscopy. Osteotomy was performed using a drill and osteotomes, with the contralateral cortex kept intact. A small incision was made on the lateral aspect of the fibula proximal to the tibial osteotomy line in the fibular osteotomy. The tibial osteotomy was then gradually and meticulously performed until the TAS angle reached 92°–95°. The result was confirmed by fluoroscopy before the tibial fixation was completed. In our early clinical practice, we used the allograft for bone grafting in the osteotomy defect, but later we didn’t use any bone grafting. A typical case of this procedure is shown in Figure 1. A 66-year-old woman suffering from left ankle pain for 9 months and diagnosed with Takakura stage II ankle arthritis. She received medial opening-wedge osteotomy. Before surgery, the anteroposterior weight-bearing radiograph revealed a medial clear space narrowing in the left ankle, with a smaller TAS angle (a); at 19 weeks after surgery, the osteotomy was healed, with the TAS angle restored to normal (b).
The anterolateral or anterior midline approach was adopted for dome osteotomy. All the osteophytes in the ankle were removed. A Kirschner wire was placed at the center of rotation of angulation (CORA). After confirmation by fluoroscopy, the osteotomy line was drawn using a contoured plate and a locking sleeve. The lateral exit of the osteotomy line was usually located at 2–3 cm above the ankle joint. Tibial osteotomy was performed using the drill and the thin osteotome. Fibular osteotomy was completed using the same incision. The deformity was corrected, and the result was confirmed by fluoroscopy before the tibial fixation was completed. One case of this procedure is shown in Figures 2 and 3. A 54-year-old woman with Takakura IIIb ankle arthritis caused by repeated sprains. The anteroposterior weight-bearing radiography of the ankle joint revealed varus deformity, with medial clear space narrowing (a): the lateral weight-bearing radiography revealed mild anterior dislocation of the talus, with conspicuous osteophytes (b). Dome osteotomy was performed. Incision for the anterolateral approach (c); osteophytes were removed from the distal tibia, and significant cartilage wear was shown in the anteromedial aspect of the talus (d); the Kirschner wire was placed at CORA, with fluoroscopy confirmation (e); the osteotomy line was depicted and the drilling was performed using the sleeve and the drill (f); osteotomy was completed using an osteotome (g). Takakura IIIb ankle arthritis was corrected by surgical treatment. Deformity was corrected with temporary fixation and fluoroscopy confirmation (a, b); fixation completed (c, d); the osteotomy was healed at 15 months after surgery. The TAS angle was corrected, and the normal medial clear space was restored (e); the anterior dislocation of the talus was corrected (f).

The anterolateral or anterior midline approach was selected for the lateral closing wedge osteotomy. The neurovascular bundles, and tendons were retracted to the medial aspect. According to the preoperative plan, the lateral closing wedge osteotomy of the tibia was performed at 3–4 cm above the ankle mortise. Fibular osteotomy was performed at the same level, and the result was confirmed by fluoroscopy before tibial fixation was completed.
After osteotomy and fixation, the hindfoot alignment was assessed by intraoperative fluoroscopy. If there was an abnormal hindfoot alignment, medial/lateral displacement calcaneal osteotomy would be performed. The dorsiflexion of the ankle joint was examined. If the dorsiflexion was restricted, achilles tendon lengthening by Hoke’s triple hemisection would be performed. Those with elongated anterior talofibular ligament (ATFL) were treated by the Brostrom procedure.
After surgery, a cast in the neutral position or a walking boot was applied for 2 weeks to protect the soft tissues. The sutures were removed 2–3 weeks later. The patients were encouraged to take ankle range of motion exercises after the sutures were removed. Gradual weight-bearing exercises began at 4–6 weeks after surgery. Full weight-bearing exercises started at 8–12 weeks after surgery.
Follow-up and efficacy evaluation
The patients were followed up at 3, 6 and 12 months and then every year after surgery. But due to the COVID-19 pandemic, the last follow-up was conducted by phone in some patients. According to the previous reports, telephone follow-ups have comparable reliability as those via the outpatient clinic. 18 As for the clinical assessments, American Orthopaedic Foot and Ankle Society (AOFAS) ankle hindfoot scale and Visual Analogue Score (VAS) were used before surgery and at the last follow-up. The patients were radiographically assessed by the tibial anterior surface (TAS) angle, tibial lateral surface (TLS) angle, and talar tilt (TT) angle before and after operation. The TAS angle is the medial angle between the tibial axis and the distal tibial articular surface on the anteroposterior weight-bearing view of the ankle; the TLS angle is the anterior angle between the tibial axis and the line connecting the anterior and posterior margins of the distal tibial articular surface on the lateral weight-bearing view of the angle; TT angle is the angle between the distal tibial articular surface and the tangential line of the upper surface of the talus. Postoperative complications and satisfaction rates were recorded.
Statistical analysis
Statistical analyses were conducted using the IBM SPSS25.0 software. The measurement data were analyzed by the Shapiro-Wilk test for normality. If the measurement data were normally distributed with homogeneity of variance, they were expressed as mean±standard deviation; otherwise, they were expressed as M(P2, P75). Parameters of normal distribution were analyzed by the paired-samples t-test. Those not obeying normal distribution were analyzed by the paired-samples Wilcoxon rank-sum test. p < .05 indicated a significant difference.
Results
The average follow-up time was 31.9 ± 5.8 months (24–45 months) in 57 patients. The patients were divided into three groups according to Takakura classification: stage II, stage IIIa and stage IIIb. There were significant differences in age (F = 7.33, p = .002) or gender (chi-square value=9.804, p = 0.007) among the three groups of patients. However, there were no significant differences in the affected side (chi-square value = 0.643, p = .725), BMI (F=1.213, p = .305), etiology of ankle arthritis (chi-square value=0.074, p = .964), and follow-up duration (F = 2.456, p = .095).
AOFAS and VAS scores in patients at different stages.
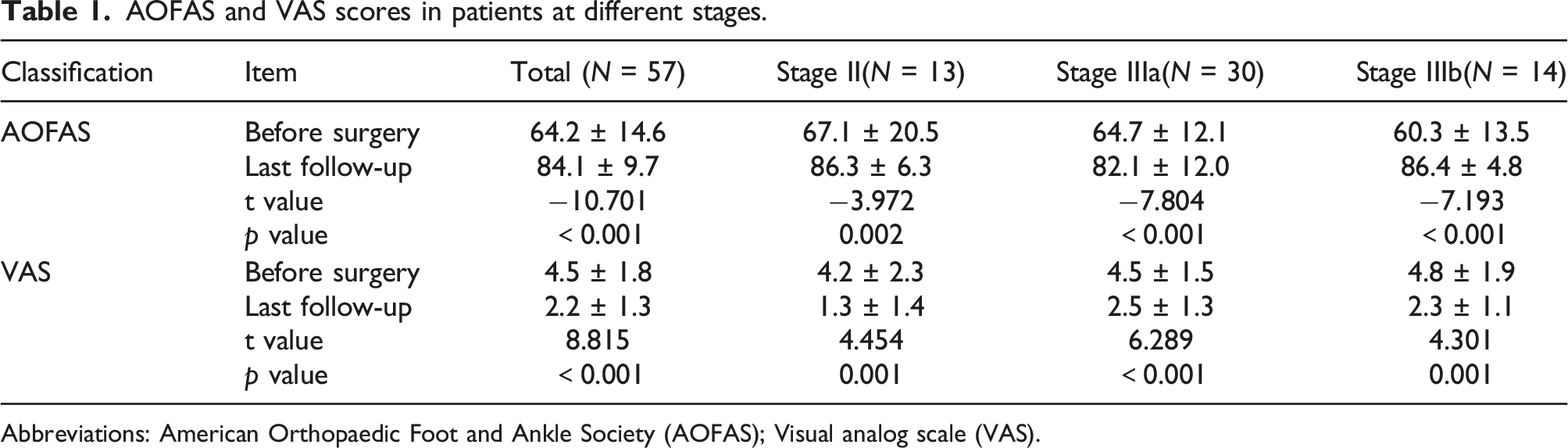
Abbreviations: American Orthopaedic Foot and Ankle Society (AOFAS); Visual analog scale (VAS).
Preoperative and postoperative TAS, TLS and TT.

The TAS angle is the tibial anterior surface angle; the TLS angle is the tibial lateral surface angle; the TT angle is the talar tilt angle.
All patients achieved bone union upon the last follow-up; 8.8% (5/57) of the patients had skin paresthesia in the wound area; superficial wound infection was found in 3.5% (2/57) of the patients, and healing was achieved after debridement, dressing, and oral antibiotics. The overall satisfaction rate of the patients was 87.7% (50/57).
Discussion
The present study showed that supramalleolar osteotomy achieved good short-to mid-term clinical outcomes for intermediate stage varus ankle arthritis. The patients were generally satisfied with the procedures, and the incidence of complications was not high. Radiographically, supramalleolar osteotomy effectively corrected the TAS and TLS angles in all patients and the TT angle in stage IIIb patients.
It has been reported in many studies that supramalleolar osteotomy has good clinical outcomes for varus ankles. Several mid-to long-term follow-up studies by Takakura6,15 and Tanaka 14 confirmed that pain was relieved and functions were improved in most patients after medial opening wedge osteotomy, accompanied by a downgrading of the arthritis stage. In the study by Hongmou et al., 17 medial opening wedge osteotomy was performed in 39 patients who were followed up for an average of 36.6 months. The pain and functions were significantly improved. Haraguchi 19 studied 27 patients, among whom medial opening wedge osteotomy was performed on 12 patients and dome osteotomy on 15. They were followed up for an average of 2.8 years. All of them achieved favorable outcomes, and there was no significant difference in the efficacy between the two groups. All the abovementioned studies included the stage IIIb patients and reported good clinical outcomes. In a study which focused on the stage IIIb varus ankle arthritis, the author found that supramalleolar osteotomy combined with auxiliary procedures can achieve functional and radiographic stages improvement. 20 One study investigated supramalleolar osteotomy for varus ankle arthritis in 99 patients, which had the largest sample size so far, also reported favorable mid-to long-term outcomes, with a 5-years survival rate of 88%, however, stage IIIb was pointed out as one of the risk factors for failure 21 Other scholars, including Tanaka, 14 also did not recommend supramalleolar osteotomy for stage IIIb patients, because the articular clear space was unfavorable after surgery for patients of this stage, which was hardly improved to stage I or II. Krahenbuhl 22 found that the 5-year survival rate of IIIb stage patients was less than 50% after surgery. In the present study, the postoperative AOFAS and VAS scores were significantly improved regardless of the stages (p < .05). The postoperative TAS and TLS angles were also improved considerably (p < .05). The above results indicated that supramalleolar osteotomy achieved good short-to mid-term clinical outcomes for intermediate stage varus ankle arthritis, including stage IIIb. Lee 16 also found noticeable improvements in pain and functions of most stage IIIb patients whose arthritis stage was not changed. Therefore, it is important to fully inform the stage IIIb patients, especially the young patients, of the potential short-to mid-term outcomes of this surgery. Supramalleolar osteotomy is quite beneficial from the perspective of improving pain and function, delaying joint fusion or replacement.
In the present study, the TAS angle increased from 80.5 ± 6.7° preoperatively to 92.4 ± 5.5° postoperatively and the TLS angle increased from 74.9 ± 4.6° preoperatively to 79.3 ± 5.3° postoperatively, both indicating significant differences (p < .001). In addition, the improvements of all groups showed significant differences. The above results indicate that supramalleolar osteotomy can correct both coronal and sagittal plane deformities in varus ankle arthritis. Lee believed that overcorrection of the TAS angle might lead to subfibular pain and he suggested that the TAS angle correction should not exceed 95°. 16 Hintermann also corrected the varus deformity to 2°–4° valgus. 23 We generally correct the TAS angle to 92–95°. If the hindfoot was still in varus, calcaneal osteotomy would be added. Hintermann showed that properly increasing the TLS angle was conducive to correcting anterior dislocation of the talus. 24 Based on this, we usually increase the TLS angle to 80° for those with a small TLS angle and talus anterior dislocation, but excessive correction more than 80°should be avoided, and lest cause restricted ankle joint dorsiflexion. Despite the significant difference in the TT angle before (5.2 ± 64.1°) and after surgery (3.7 ± 3.4°), the improvement was actually only significant in stage IIIb patients (p = .003), which was reasonable as talar tilt was mild in stage II and IIIa patients. The result confirmed the strong ability of supramalleolar osteotomy for TT angle correction in patients with stage IIIb ankle arthritis.
The present study had several limitations: (1) there were some intrinsic defects due to the retrospective nature of the study; (2) the sample size was small, and some baseline parameters were significantly different across the groups; (3) due to small sample size, intergroup comparisons were not performed and the prognostic risk factors were not analyzed, and different kinds of osteotomies might also have influence on outcomes.
Conclusion
In conclusion, supramalleolar osteotomy achieved good short-to mid-term clinical outcomes for intermediate stage varus ankle arthritis. Radiographically, supramalleolar osteotomy effectively corrected the TAS and TLS angles in all patients and the TT angle in stage IIIb patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.