
Abstract
Background
The current surgical treatment plan for medium-term varus-type ankle arthritis is primarily supramalleolar osteotomy (SMOT), but the reliability of this procedure still lacks high-quality evidence-based medical studies, such as randomized controlled clinical trials and meta-analyses of comparative studies.
Objective
The current study explored whether significant differences were present in the clinical effect, reoperation rate, complications, and failure rate of this type of surgery.
Method
Two researchers searched the relevant literature in seven databases, including PubMed, Cochrane Library, EMBASE, the China Biomedical Literature Database, the China Academic Journals Full-text Database, the Wanfang database, and the Weipu Chinese Science and Technology Journal Database. The retrieval time spanned the establishment of the specific database up to September 2020, and the literature was screened to determine their final inclusion in the study.
Results and conclusions
A total of 20 studies were included, including one Chinese and 19 English language studies. The primary indicators included a definitive effect of SMOT on the treatment of medium-term varus-type ankle arthritis. Concerning secondary indicators, although the surgery effect was satisfactory, some patients may require follow-up surgery, which may be unsuccessful with complications. The study results showed that, based on existing literature reports, the effect of SMOT for varus-type ankle arthritis was a satisfactory surgical method with some clinical value for correcting the ankle force line and relieving or even reversing ankle arthritis. However, its risk of complications and failure rate were comparatively high and, accordingly, requires good preoperative planning and close communication with patients. Due to the limited sample size of this study, more data and longer follow-up times involving this type of surgery should be reviewed to confirm this conclusion.
Introduction
According to statistics, nearly 1% of adults worldwide suffer from ankle osteoarthritis (OA). 1 Several pathogenic factors are involved in this condition, including congenital abnormalities of the tibia, deformed healing following a distal tibial fracture, distal tibial epiphysis injury, infection, ankle instability, and neuromuscular disease. 2 Ankle varus and valgus deformities are the primary manifestations of common ankle malalignment. 3 In patients with symptomatic ankle osteoarthritis, it has been reported that varus and valgus ankles account for 70%–80% 3 of symptomatic ankle osteoarthritis. Valderrabano et al. 4 found that 55% of ankle OA patients had combined ankle varus and 8% had combined ankle valgus.
In 1936, Speed and Boyd 5 published a clinical study on designing a method for treating post-ankle trauma deformity and identified three key targets for supramalleolar readjusted surgical procedures as follows: (1) restore the proper force line; (2) restore the proper arrangement of the tibial pitch joint surface; 3) restore the physiological and pain-free activity range of the tibiotalar joint. Subsequently, Takakura and colleagues 6 were the first to systematically report the application of SMOT in 1995 and proposed the classification of varus ankle OA. This was mainly classified into four types as follows: stage (1) the joints are parallel, without joint space stenosis, early subchondral osteosclerosis or osteophyte formation; stage (2) the medial joint space is narrow without subchondral bone contact; stage (3) (a) the medial ankle space is occluded, and the subchondral bone contact is medial; (b) subchondral bone contact extends to the fornix of the talus; stage (4) a varus ankle joint with complete bone contact.6,7
In the reports of these scholars, the effect of SMOT on the treatment of medium-term ankle arthritis was predictable.
4
Nonetheless, there are currently no systematic reports that confirm these results. Supramalleolar osteotomy for ankle arthritis still lacks high-quality evidence-based ST, e.g. randomized controlled clinical trials and meta-analyses of comparative studies. Meta-analysis is increasingly being recognized as a key tool for obtaining high-quality evidence.8,9,10 Accordingly, this study adopted a meta-analysis approach to perform a comparative investigation of existing studies to determine whether there were significant differences in clinical scores and reoperation rates. The aim of doing so was to better understand the application of SMOT in varus-type ankle arthritis.
Data and methods
Search strategy
The current study was conducted according to the Preferred Reporting Items of Systematic Review and Meta-Analysis set. Two researchers conducted searches for the relevant literature in seven databases, i.e. PubMed, Cochrane Library, EMBASE, the China Biomedical Literature Database, the Chinese Journal Full Text Database, the Wanfang database, and the Weipu Chinese Science and Technology Journal Database. The retrieval time spanned the establishment of the specific database up to September 2020.
The search was performed in strict accordance with the PICOS (population, intervention, comparison, outcome, study) design principles, and the remaining relevant literature was searched manually. Subject-related terms were combined with free words; the English search terms were ‘supramalleolar osteotomy’, ‘osteotomy’, ‘low tibial osteotomy’ and ‘ankle’, ‘ankle arthritis’, ‘ankle osteoarthritis’, ‘varus ankle’, ‘varus ankle arthritis’, ‘varus ankle osteoarthritis and/or ‘treatment’. The Chinese search terms included ‘supramalleolar osteotomy’, ‘ankle arthritis’, ‘varus’ and ‘treatment’. The literature search results were not limited in terms of time, country or region. Following an initial electronic search, the authors searched other relevant articles by scanning the bibliographies of all the selected full-text articles.
Selection criteria
Inclusion criteria
The study’s inclusion criteria were as follows: (1) the literature study reported on patients diagnosed with varus ankle arthritis who were treated with SMOT; (2) the study reported on the treatment efficacy of SMOT, preoperative and postoperative effect comparisons, and provided a complete description of various pre-and post-surgery; (3) the study included American Orthopaedic Foot and Ankle Society (AOFAS) scores; (4) the study included pain scores.
Exclusion criteria
The study’s exclusion criteria were as follows: (1) repeated studies; (2) case reports, reviews, meta-analyses, editorials, letters, non-English studies, non-human study cohorts/cadaver experimental studies; (3) studies from which data could not be extracted; 4) literature that was not relevant to the current study.
Data extraction
The data extracted by the researchers included the following: (1) the name of the first author, the publication date, the average age of participants, sample size, patient gender, follow-up time, and the primary indicators (SMOT, varus ankle arthritis) and secondary indicators (complete preoperative and postoperative description, AOFAS score, pain score, postoperative complications elaboration). If disagreement occurred among the researchers during the data extraction process, they sought the help of corresponding authors.
Statistical analysis
Statistical analysis was performed using the SPSS Statistics 21.0 software program. Measurement data were expressed as
Results
Literature screening process
Using the electronic system search, a total of 1591 Chinese documents and 3725 foreign language documents were retrieved. Subsequently, reviews, meta-analyses, case reports, books and repeated literature were excluded. Following additional review of the article’s title and abstract, 1590 Chinese documents and 3705 foreign language documents were excluded. After further reading of the full article, one article with incomplete data was excluded. Finally, 20 retrospective study articles that met the study criteria were selected for analysis (see Figure 1). Literature screening process.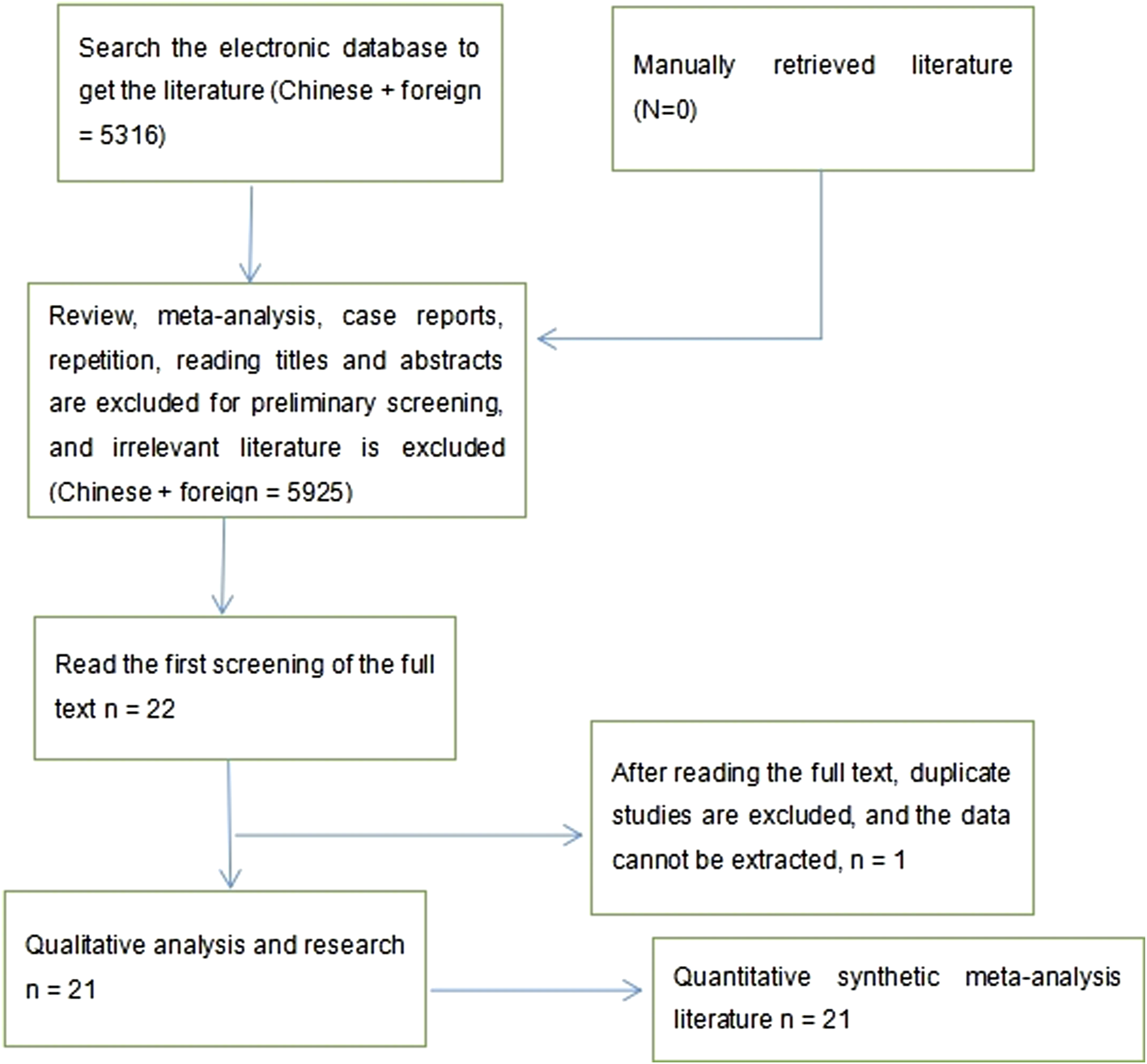
Characteristics of the included studies
Basic information of literature.

Note: SMOT: supramalleolar osteotomy; SMOT WITH MDA: supramalleolar osteotomy with medial distraction arthroplasty; TOT: tibia osteotomy; TFOT: tibia and fibula osteotomy
Results of the meta-analysis
The correction effect of supramalleolar osteotomy
Corrective effect of supramolecular osteotomy (SMOT).

According to the statistical software results, the three perspectives noted above showed significantly better postoperative results compared with before surgery. The TAS improved from 84.2° preoperatively to 91.5° postoperatively (p < 0.001), TLS improved from 79.7° preoperatively to 82.15°, (P < 0.002) and TT improved from 9.55° preoperatively to 4.78° (p < 0.001). It was concluded that the effect of supramolecular osteotomy on varus ankle arthritis had been clearly indicated.
Ankle function score
The AOFAS scores in the literature data were included for statistical analysis (the relevant data were not recorded in selected papers and were automatically screened out in the SPSS software) (see Figure 2). Score of ankle function.
According to the statistical analysis results using the SPSS 21.0 software, the AOFAS score improved from 54.05 preoperatively to 79.67 postoperatively (p <0.001), inferring the conclusion that supramolecular osteotomy benefitted functional improvement in patients with varus ankle arthritis.
Pain score
The visual analogue scale (VAS) scores in the literature data were included for statistical analysis.
(the relevant data were not recorded in some literature and were automatically screened out in the SPSS software) (see Figure 3). Pain score.
Based on the statistical analysis conducted using the SPSS software, the VAS pain score decreased from 5.82 preoperatively to 2.45 postoperatively (p < 0.001), inferring the conclusion that supramolecular osteotomy is conducive to pain relief in patients with varus ankle arthritis.
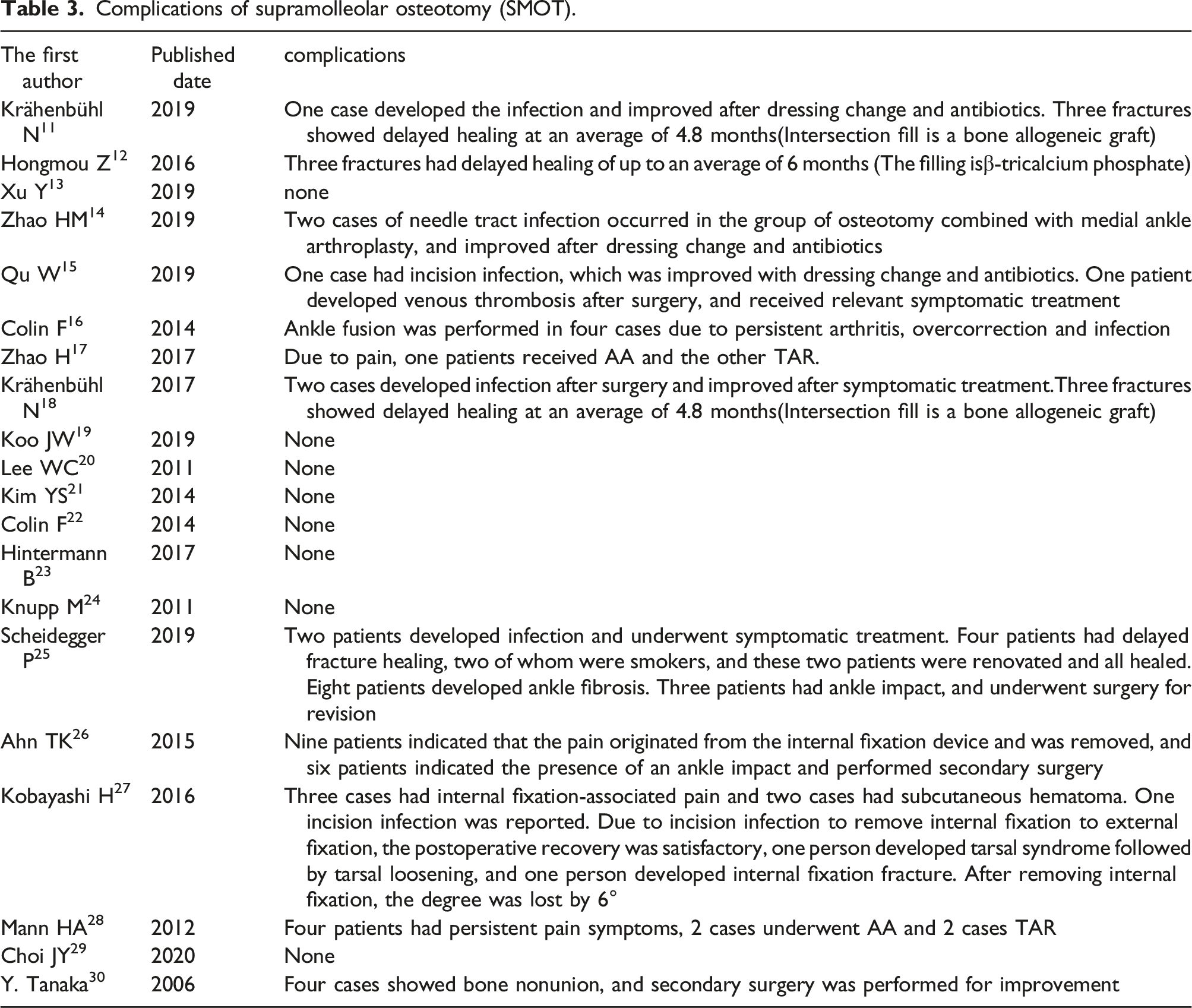
Complications
Complications of supramolleolar osteotomy (SMOT).
Revision rate
Revision rate of supramolecular osteotomy (SMOT).

Failure rate
Failure rate of supramolleolar osteotomy (SMOT).

Discussion
In the 20 literature studies on varus ankle arthritis, the bulk reported on the progression of ankle arthritis slowing, maintaining its current state, or even indicating reversal. A study by Zhao 12 showed that at an average follow-up of 36.6 months, a total of 22 (57%) cases indicated slowed varus ankle arthritis, 13 (33%) cases remained unchanged, and 4 (10%) cases indicated a worsening condition. A study conducted by Qu 15 showed a mean follow-up time of more than 32.2 months; the arthritis stage was improved in 11 (65%) cases, in which 2 cases ranged from stage 2 to 1, 7 cases ranged from stage 3a to 2, and 2 ranged from stage 3b to stage 3a. Six cases indicated no changes, and there was no aggravated cases. A study conducted by Hintermann 23 had an average follow-up of 4 years, during which time 3 ankles deteriorated by one stage (1 ankle, phase I–Ⅱ; 2 ankles, phase Ⅱ–Ⅲ), 11 ankles improved by one stage (3 ankles, phase Ⅱ–I; 7 ankles, phase Ⅲ–Ⅱ; one ankle, phase Ⅳ–Ⅲ) and 6 ankles were unchanged. In these reports, more than 50% of ankle arthritis showed improvement, and a small number of patients had made progress.
Although SMOT can delay the progression of ankle arthritis, the surgical failure rate is as high as 9% and cannot be ignored. According to the mid-term follow-up results reported by Krahenbuhl, 18 the 5-year survival rate was 75%, while the 5-year survival rate of stage 3b was only 47%, i.e. the patient was very likely to undergo ankle degeneration within 5 years, or persistent symptoms requiring ankle fusion or an ankle replacement. Kim 21 retrospectively assessed 31 patients who received varus wedge SMOT. In all patients, arthroscopic bone marrow stimulation was performed on the medial cartilage lesions. Secondary arthroscopy revealed progressive ankle degeneration in 13 (42%) patients, while follow-up after 1 year revealed a deterioration in both the VAS and AOFAS scores. For SMOT, cartilage lesions were identified as a risk factor for adverse outcomes. 30 Following the failure, the ankle will be sacrificed to improve function.
The statistical method applied in the present study tested the surgical effect of 20 research papers and found that the TAS, TLS and TT angles had been significantly improved, and the AOFAS and VAS pain scores were also significantly improved and with statistical significance. Accordingly, the effect of this surgery on varus ankle arthritis can be considered as positive. However, the procedure also presents common complications, primarily infection, thromboembolism, incision healing problems (including deep infection) and the delayed/non-healing of the fracture, pain and aggravated symptoms. 31 Complications should be actively treated, based on symptomatic presentation. Early superficial infections can be improved by regular cleaning of the surgery area and dressing changes or the application of antibiotics. However, in the case of deep infections, these should be eradicated; this may require removing internal fixtures and performing surgical debridement to prevent infection.
The reasons for delayed fracture healing or non-healing (up to 22%) included anatomical reduction, periosteal dissection, whether the section was fixed, the osteotomy technique, the bone filling material that was used, and completing early functional exercise. Depending on the patient’s condition, secondary bone grafting surgery should be performed if necessary to accelerate healing of the fracture. If the pain or symptoms worsened and could not improve, final amendment surgery will be required, e.g. joint fusion or replacement.24,32,33,34
Supramalleolar osteotomy is an ankle-preserving procedure that is conducted in cases of ankle arthritis; it has good short-and medium-term results in terms of pain relief, improved function, and restoring exercise ability, and can also delay and may even reverse the progress of OA. Concurrently, the procedure requires several surgical techniques with high technical requirements. Additionally, surgical complications are not uncommon and are accompanied by surgical failure and the need for amendment procedures.12,21,35 The current authors considered SMOT to be a viable option when the following symptoms are present: (1) imaging manifestations of varus ankle OA; (2) force line adjustment before and after ankle arthrodesis or joint replacement; (3) distal tibial fracture malunion. Additionally, SMOT can also be used to correct ankle varus caused by ankle instability or congenital ankle varus.
In conclusion, SMOT of the ankle is an effective and reliable ankle-preserving surgery that can correct the displaced ankle force line and the ankle malalignment in the coronal plane. However, we should bear in mind that this procedure cannot relieve the ankle pain completely in varus ankles. Therefore, more high-level studies such as randomized control trials are needed in the future for a more precise assessment of the indications of the procedures to delay or reverse the progress of varus degeneration of the ankle.
Footnotes
Acknowledgements
We would like to express our gratitude to all those who helped us during the writing of this manuscript.
Authors’ contributions
Xue Wang, Conceptualization, Data curation, Project administration, Writing - original draft, Supervision, Writing - review and editing; Tiannan Chen, Conceptualization, Data curation, Writing - original draft, Writing - review and editing; Paerhati Wahafu, Formal analysis, Investigation, Writing - original draft, Writing - review and editing; Fei Li, Formal analysis, Investigation, Methodology, Writing - original draft, Writing - review and editing; Ayiding Xiahatai, Formal analysis, Investigation, Methodology, Writing - original draft, Writing - review and editing; Aikeremu Wufuer, Investigation, Methodology, Writing - original draft, Writing - review and editing; Yanan Tuo, Methodology, Resources, Software, Writing - original draft, Writing - review and editing; Bo Zhao; Methodology, Resources, Software, Writing - original draft, Writing - review and editing; Chengwei Wang, Investigation, Supervision, Validation, Visualization, Writing - original draft, Writing - review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of The Sixth Affiliated Hospital of Xinjiang Medical University. All participants signed an informed consent form for inclusion in the study.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.