
Abstract
Background:
Surgical treatment is usually required for malignant foot and ankle tumors. In this study, we sought to review factors in treatment that may be associated with morbidity and mortality.
Methods:
All malignant foot and ankle tumors at our institution between April 1988 and April 2018 were retrospectively reviewed. The surgical modalities used and clinical outcomes of patients according to the anatomic location (Kirby zone) and clinical stage (Enneking system) of each tumor were described. Extent of surgical resection required, recurrence, and death rates were assessed.
Results:
Between April 1988 and April 2018, 80 patients with malignant tumors of the foot and ankle were treated at out institution. Mean age of patients was 42.6 (range, 3-89) years. Mean follow-up was 30.2 months (range, 24-120). Tumors were primary in 75 patients (94%) and metastatic from another organ in 5 patients (6%). Tumors originated from bone in 18 patients (22%) and from soft tissue in 63 patients (78%). Synovial sarcoma was the most common soft tissue tumor, and osteosarcoma was the most common osseous tumor.
All patients had surgery to resect their tumor. Twenty-one (26%) had unplanned surgical procedures without initial biopsy at an outside institution prior to referral. Those patients were more likely to be treated with amputation or wide excison and free flap surgery (P < .01). The recurrence rate was 50% for the unplanned surgery group and 22% for the planned surgery group. Mortality rate was 10% for the unplanned group and 6% for the planned group. The recurrence and mortality rate was higher in the unplanned group (P = .03).
Conclusion:
Our study suggests that unplanned initial surgeries are associated with higher recurrence and mortality rates and reinforces the notion that these patients should be referred for treatment at a center with specialized expertise in tumor management.
Level of Evidence:
Level, IV, retrospective case series.
Keywords
Introduction
Only about 4% of malignant musculoskeletal tumors involve the foot and ankle.5,12,17 Given their rarity and heterogenous presentation, these lesions are frequently confused with more common benign lesions, resulting in missed or delayed diagnosis.1,3,29,30 Plantar sarcomas have been incorrectly characterized as fibromatosis. Dorsal synovial sarcomas misdiagnosed as ganglions. Malignant melanomas thought to represent chronic ulcerations and primary bone tumors were initially diagnosed as stress fractures.2,4,5,12,16
Missed and delayed diagnoses are likely to increase recurrence rates, treatment-related morbidity, and even mortality.7,21,23 Diagnosis usually starts with a high index of suspicion followed by adequate radiologic imaging.21,23,39 Complex bone and soft tissue anatomy of the foot and ankle necessitates cross-sectional imaging. Magnetic resonance imaging is needed for those tumors within the soft tissues. Computed tomography may be obtained for bone involvement and surgical planning.19,25,37,38 Radiologic workup is usually followed by a fine-needle aspiration biopsy or Tru-Cut biopsy for a clinically reliable cytopathologic diagnosis in a high percentage of foot and ankle mass lesions. 14
Unplanned excisions without appropriate preoperative evaluation and biopsy are not uncommon.9,22,24,28 In the case of a contaminated surgical field in foot and ankle where soft tissues are scarce, negative tumor margins may necessitate amputation or resection of the tumor bed with significant morbidity. These incidents are not rare and a major cause of both disability and medicolegal problems. Surgical treatment is traditionally required for most malignant foot and ankle tumors. Anatomic and clinical classification systems have been helpful in determining the appropriate surgical modality and extent of surgery.10,20
There is a concern about the high frequency of inadequate management of malignant foot and ankle tumors.7,8,21 Therefore, we aimed to analyze the role and the results of surgery in this special group of patients. We retrospectively reviewed histologic diagnosis, initial treatments, radiologic workup, and treatment modalities at a single institution. We hypothesized that unplanned surgery for the purpose of excisional biopsy without fine-needle aspiration or Tru-Cut biopsy is related to increased morbidity and amputation rates.
Patients and Methods
We retrospectively analyzed the records of 80 consecutive patients with 81 malignant foot and ankle tumors that were diagnosed and treated at the orthopaedics and traumatology department between April 1988 and April 2018 with a minimum follow-up of 2 years. One patient had the same tumor located in the same location and treated the same way in each foot, so for the purposes of this report, we considered this patient as a single case. We gathered data concerning pathologic diagnosis, type of treatment, duration of follow-up, and clinical outcomes.
We included patients with malignant tumors involving the bones or soft tissues of the foot up to 12 cm proximal to the level of the ankle joint. We excluded patients with benign tumors. All patients underwent a history and physical examination, routine blood tests, conventional radiologic examinations, computed tomography, and whole body bone scintigraphy. Most patients had magnetic resonance imaging. Angiography was performed when tumors were located near significant blood vessels and/or when needed to help determine level of amputation. Closed or incisional biopsy techniques were performed when patients had lesions that were particularly suspicious for malignancy (ie, unresolving pain, rapid increase in size of the mass or amount of the swelling) and were being considered for amputation. However, 21 patients had unplanned surgical procedures without initial biopsy at an outside institution prior to referral. Fifty-nine patients had planned surgical procedures at our institution.
We used Kirby zones to categorize the location of both soft tissue and osseous tumors (Figure 1). 20 The anatomic locations of the zones were the ankle (zone 1), heel (zone 2), dorsum of foot (zone 3), plantar surface of foot (zone 4), and toes (zone 5).
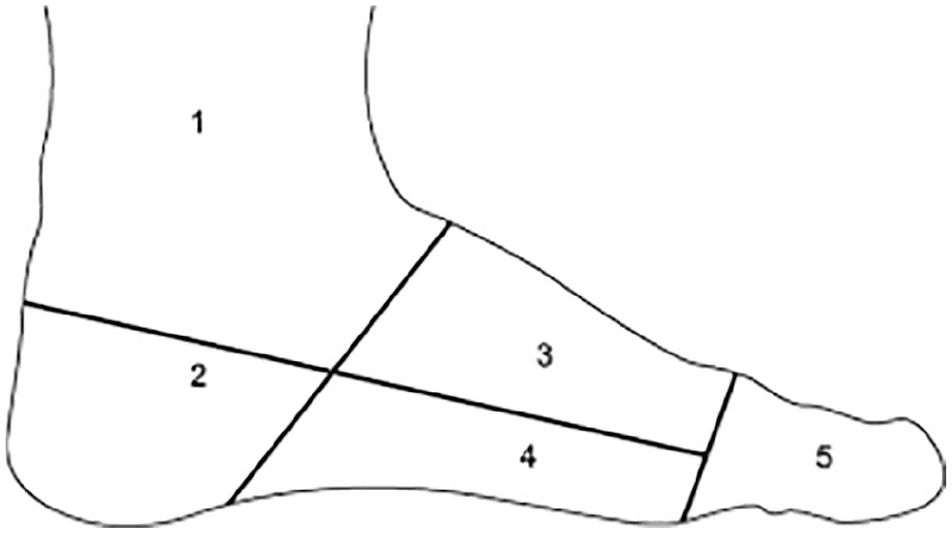
Kirby anatomic zones of the foot and ankle. Kirby zones are used to categorize the location of both soft tissue and osseous tumors of the foot and ankle. 20 These zones are created by drawing 3 lines on a lateral roentgenograph of the foot. A horizontal line is drawn from the heads of the metatarsals to the insertion point of the Achilles tendon, and 2 vertical lines are drawn perpendicular to the first line. One of the vertical lines is drawn from the midtarsal point to the posterior end of the longitudinal plantar arch, and the other vertical line is drawn from the metatarsophalangeal joints down to the sole of the foot. The resulting anatomic locations of the zones are the ankle (zone 1), heel (zone 2), dorsum of foot (zone 3), plantar surface of foot (zone 4), and toes (zone 5).
We staged tumors using the Enneking staging system, which stratifies both bone and soft tissue lesions by grade and local anatomic extent (Supplemental Table S1). 10 We also used the American Joint Committee on Cancer (AJCC) staging system (Supplemental Table S2). AJCC TNM classification is based on the extent of the tumor (T), the extent of spread to the lymph nodes (N), the presence of metastasis (M), and histopathologic grade (G) of the tumor. 34 In this classification (AJCC eighth edition) for bone sarcomas arising in the appendicular skeleton, there are 7 stage groups (IA, IB, IIA, IIB, III, IVA, IVB). On the other hand, there are 6 stage groups for soft tissue sarcomas in the extremity (IA, IB, II, IIIA, IIIB, IV). AJCC system has different stage groups for bone and soft tissue sarcomas of the foot. Therefore, we prefered staging tumors using the Enneking system.
Statistical analysis was performed using SPSS, version 22.0 (IBM Corp, Armonk, NY). Statistical analysis of data focused on the recurrence rates, mortality rates, types of surgery, stages, and locations of tumor. Potential differences were assessed using χ2 analysis. P values <.05 were considered significant.
Results
Among the 7300 patients with bone and soft tissue tumors at our orthopaedics and traumatology department between April 1988 and April 2018, 80 patients (1.1%) had malignant tumors in 81 feet.
Of the 80 patients, 46 (57.5%) were male and 34 (42.5%) were female, resulting in a male to female ratio of 1.35. The age of patients ranged from 3 to 89 years, with a mean age of 42.7 years. A total of 43 patients (53.7%) had a tumor in their right foot, 36 (45.0%) had a tumor in their left foot, and 1 (1.2%) had both feet involved. The mean follow-up was 30.2 (range, 24-120) months.
Twenty-one patients had unplanned surgical procedures without initial biopsy at an outside institution prior to referral. Biopsy was the first step in treatment of the other 59 patients. Among those, fine-needle aspiration was performed in 26 patients (44.1%) and Tru-Cut biopsy was performed in 26 patients (44.1%). Incisional biopsy was applied to 7 patients (11.8%). Tumors were primary in 75 (93.8%) and metastatic from another tissue in 5 patients (6.2%). The most common presentation among the 80 patients was a foot mass or swelling, which occurred in 47 patients (44.3%), followed by foot pain in 34 patients (32.1%), skin lesions in 17 patients (16.0%), deformity in 6 patients (5.7%), and pathologic fracture in 2 patients (1.9%).
Of the 80 patients, 18 (22.5%) had malignant tumors in the bones. The Kirby zone distribution of bone lesions was as follows: zone 1 in 9 patients, zone 2 in 2 patients, zone 3 in 2 patients, zone 4 in 1 patient, and zone 5 in 4 patients. The most frequently involved bone was the calcaneus. On the other hand, 62 patients (77.5%) had malignant tumors in the soft tissues, and these were located in Kirby zone 1 in 17 patients, zone 2 in 12 patients, zone 3 in 12 patients, zone 4 in 10 patients, and zone 5 in 11 patients.
The most frequently identified malignant bone tumor was osteosarcoma, noted in 5 patients (Supplemental Table S3). The most common malignant soft tissue tumors were synovial sarcoma (in 21 patients), squamous cell carcinoma (in 12 patients), and fibrosarcoma (in 7 patients).
Of the 75 primary malignant foot and ankle tumors, 5 (6.6%) were Enneking stage IA, 7 (9.3%) were stage IB, 24 (32.0%) were stage IIA, 34 (45.3%) were stage IIB, and 5 (6.6%) was stage III (Supplemental Table S2). The other 5 patients had bone tumors that were metastases from other primary organs. Of these 75 tumors, 58 (77.3%) were either Enneking stage IIA or IIB.
Surgical procedures were applied to 80 patients. Twenty-one patients had unplanned surgical procedures without initial biopsy at an outside institution prior to referral. Fifty-nine patients had planned surgical procedures at our institution. A total of 125 operations were performed, 45 of which were for tumor recurrences. Of the 59 planned initial operations done, 26 (44.1%) were wide excisions, 13 (22.0%) were major amputations, 7 (11.9%) were minor (heel sparing) amputations, 7 (11.9%) were wide excision with free flap, and 6 (10.2%) involved excision with grafting (Table 1). In our clinic, the council consisting of microsurgery and tumor specialists decides jointly before the operation whether major amputation or free flap surgery will be applied. The age, comorbidities, smoking history, and expectations of the patient are effective in this decision. In addition, 58 patients (71.6%) received postoperative chemotherapy and radiotherapy. Surgical complications were uncommon, primarily involving infections or nerve injuries.
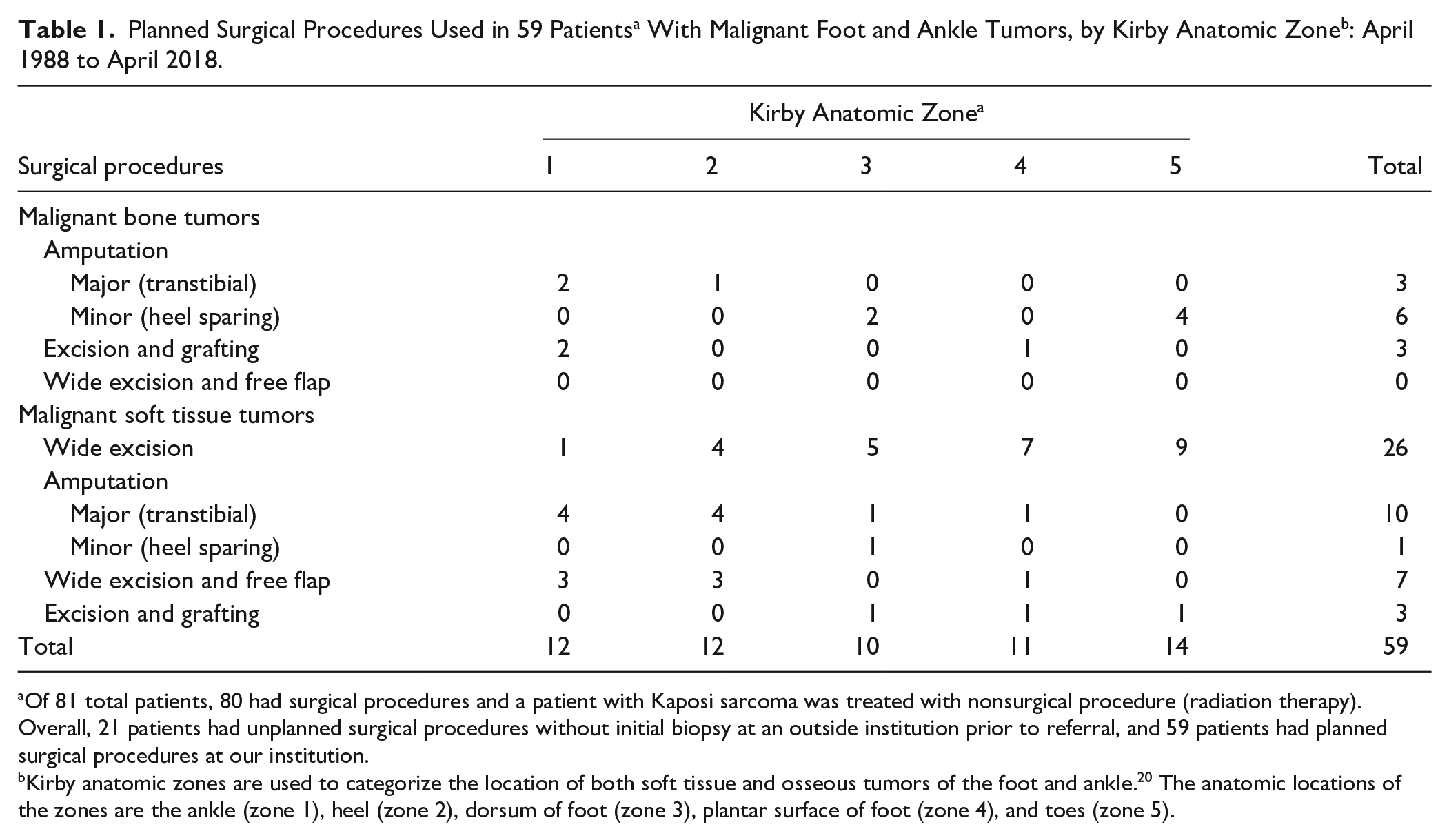
Of 81 total patients, 80 had surgical procedures and a patient with Kaposi sarcoma was treated with nonsurgical procedure (radiation therapy). Overall, 21 patients had unplanned surgical procedures without initial biopsy at an outside institution prior to referral, and 59 patients had planned surgical procedures at our institution.
Kirby anatomic zones are used to categorize the location of both soft tissue and osseous tumors of the foot and ankle. 20 The anatomic locations of the zones are the ankle (zone 1), heel (zone 2), dorsum of foot (zone 3), plantar surface of foot (zone 4), and toes (zone 5).
Major amputations (transtibial) and wide excision with free flap surgery were more common treatments in Kirby zone 1 (ankle) and zone 2 (heel). Major amputations were applied to 13 patients. Of these 13 tumors, 11 (84.6%) tumors were in Kirby anatomic zone 1 or 2. Of 7 tumors that were treated with wide excision and free flap surgery, 6 (85.7%) tumors were in Kirby anatomic zone 1 or 2. Conversely minor amputations (heel sparing) and wide excisions were more common surgical treatment in Kirby zone 3 (dorsum of foot), zone 4 (plantar surface of foot), or zone 5 (toes). Of 26 wide excision procedures, 21 (80.1%) were in Kirby zone 3, 4, or 5. Minor amputations were applied to 7 patients. All of these 7 tumors were in Kirby anatomic zone 3, 4, or 5 (Table 1).
Major amputations (transtibial) were more common in Ennekking stage IIB, stage III, and metastasis from other organs. Of 13 tumors that were treated with major amputation surgery, 11 (84.6%) were in stage IIB, III, or metastasis (8 tumors were in Ennekking stage IIB, 2 tumors were in ennekking stage 3, and 1 tumor had metatasised from other organs) (Supplemental Table S4).
Wide excision with free flap technique was applied to 12 patients. Of these 12 tumors, 7 were treated with initially planned surgery and 5 had unplanned surgical procedures without initial biopsy prior to referral. Eight were in Kirby anatomic zone 1, 3 were in zone 2, and 1 was in zone 4 . Three of the 12 tumors were Enneking stage IIA and 9 of the 12 tumors were stage IIB.
Of the 59 patients treated with planned surgery, 4 had metastatic tumors and the other 55 had primary malignant tumors. Overall, of the 55 patients, postoperative recurrences occurred in 12 patients (21.8%) and deaths occurred in 3 patients (5.5%). The highest proportion of recurrences were in patients with tumors in Kirby zone 3 (4 of 9 patients; 44.4%), zone 4 (3 of 10 patients; 30.0%), and zone 5 (3 of 13 patients; 23.1%), although this difference was not statistically significant (Table 2).
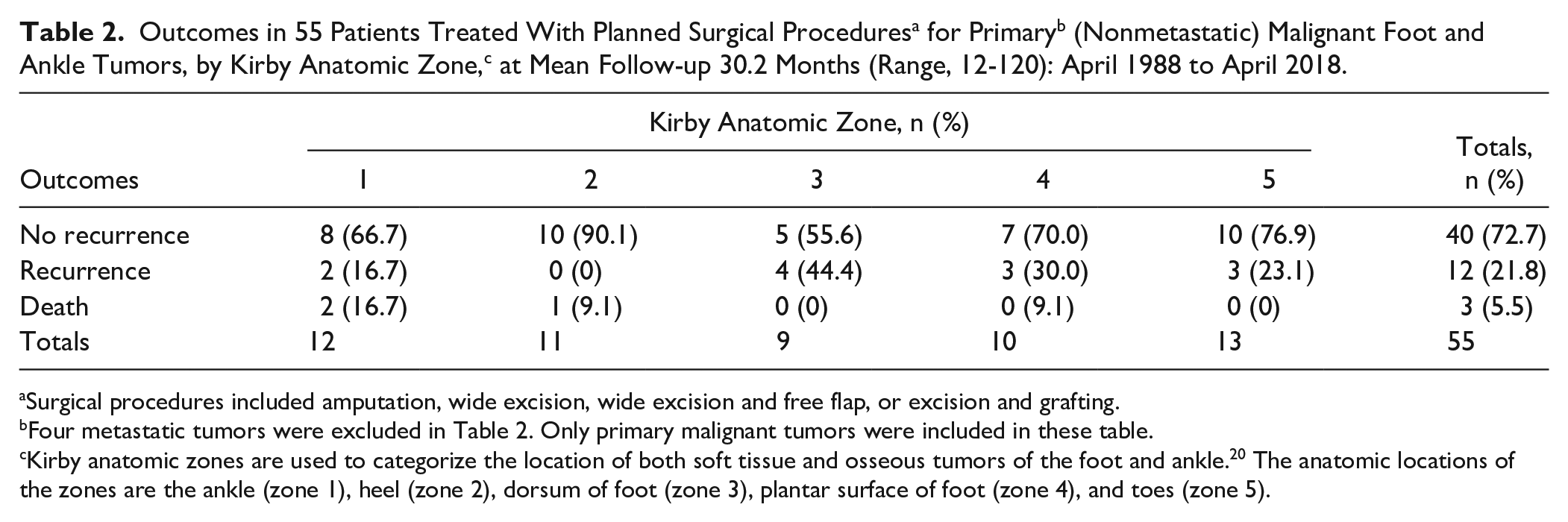
Surgical procedures included amputation, wide excision, wide excision and free flap, or excision and grafting.
Four metastatic tumors were excluded in Table 2. Only primary malignant tumors were included in these table.
Kirby anatomic zones are used to categorize the location of both soft tissue and osseous tumors of the foot and ankle. 20 The anatomic locations of the zones are the ankle (zone 1), heel (zone 2), dorsum of foot (zone 3), plantar surface of foot (zone 4), and toes (zone 5).
The highest proportion of recurrences were in patients with Enneking stage IIB (6 of 22 patients; 27.3%) and III tumors (2 of 3 patients; 66.7%), Highest mortality rates were in those with metastases from other organs (4 of 5 patients; 80.0%) (Table 3). Patients with Enneking stage IIB and III tumors, as well as those with metastases from other organs had higher proportion of recurrence and mortality compared to patients with Enneking stage IA,IB or IIA (P = .01) (Table 3B).
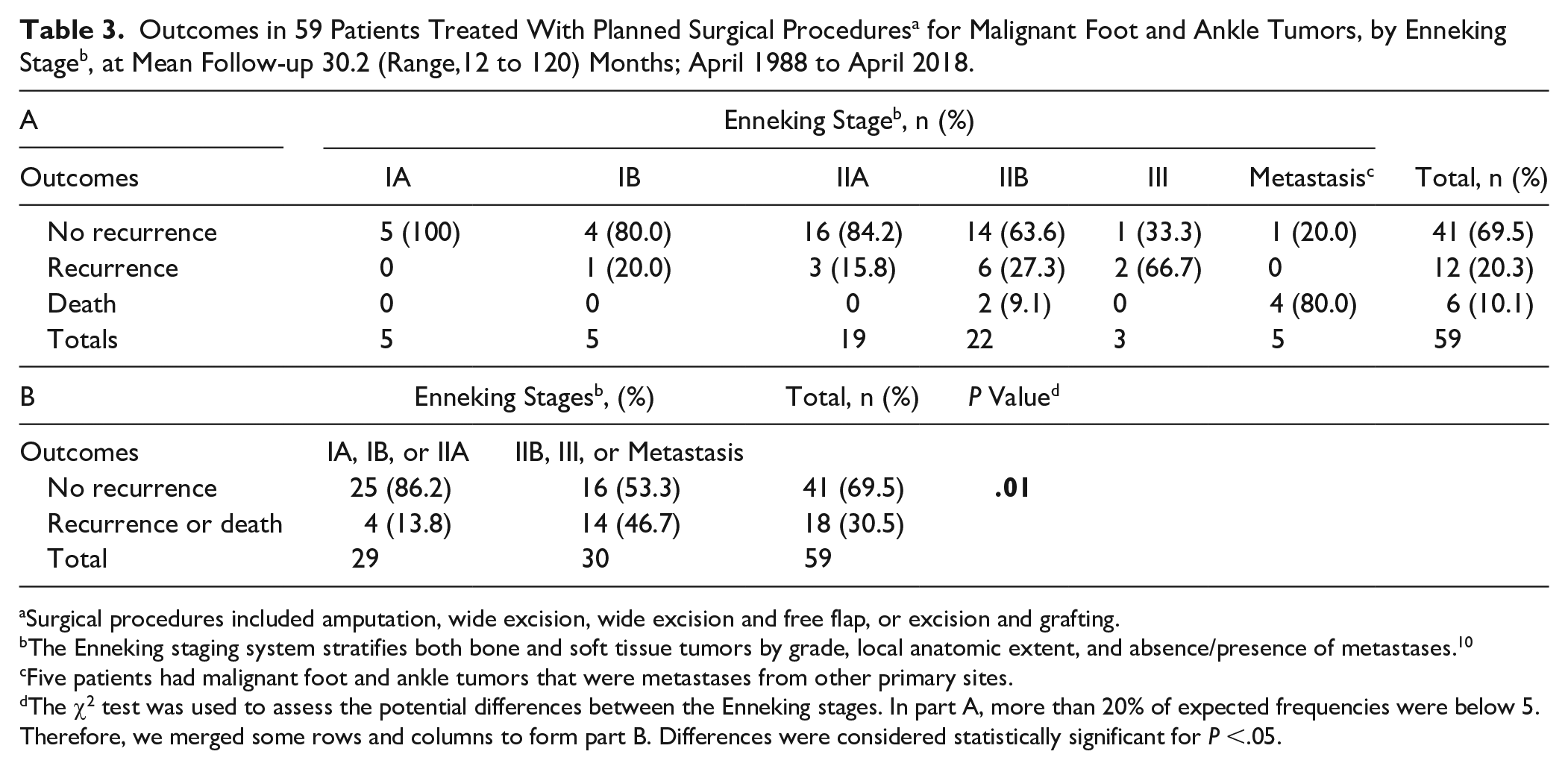
Surgical procedures included amputation, wide excision, wide excision and free flap, or excision and grafting.
The Enneking staging system stratifies both bone and soft tissue tumors by grade, local anatomic extent, and absence/presence of metastases. 10
Five patients had malignant foot and ankle tumors that were metastases from other primary sites.
The χ2 test was used to assess the potential differences between the Enneking stages. In part A, more than 20% of expected frequencies were below 5. Therefore, we merged some rows and columns to form part B. Differences were considered statistically significant for P <.05.
Overall, of the 75 patients with primary (nonmetastatic) malignant foot and ankle tumors, 20 patients had unplanned surgical procedures without initial biopsy at an outside institution prior to referral. Fifty-five patients had planned surgical procedures at our institution. Histopathologic types of malignancy were similar in “planned” and “unplanned” procedure groups. On assessment of the required re-resection of the tumor bed with planned wide margins, 70% of unplanned resection patients required amputation. This decision was based on projected bone loss, loss of soft tissue coverage that could not readily be covered with a free flap, or loss of sufficient vascular supply. Patients with unplanned procedures were more likely to be treated with amputation or wide excison and free flap surgery (P < .001) (Table 4B). We revealed that the recurrence rate was 50.0% for the unplanned surgery group and 21.8% for the planned surgery group. Mortality rate was 10.0% for the unplanned group and 5.5% for the planned group. The recurrence and mortality rate was higher in the unplanned group (P = .03) (Table 4C).
Surgical Procedure Types and Outcomes of 75 Primary a (Nonmetastatic) Malignant Foot and Ankle Tumors, by Planned or Unplanned, at Mean Follow-up 30.2 Months (Range, 12-120): April 1988 to April 2018.
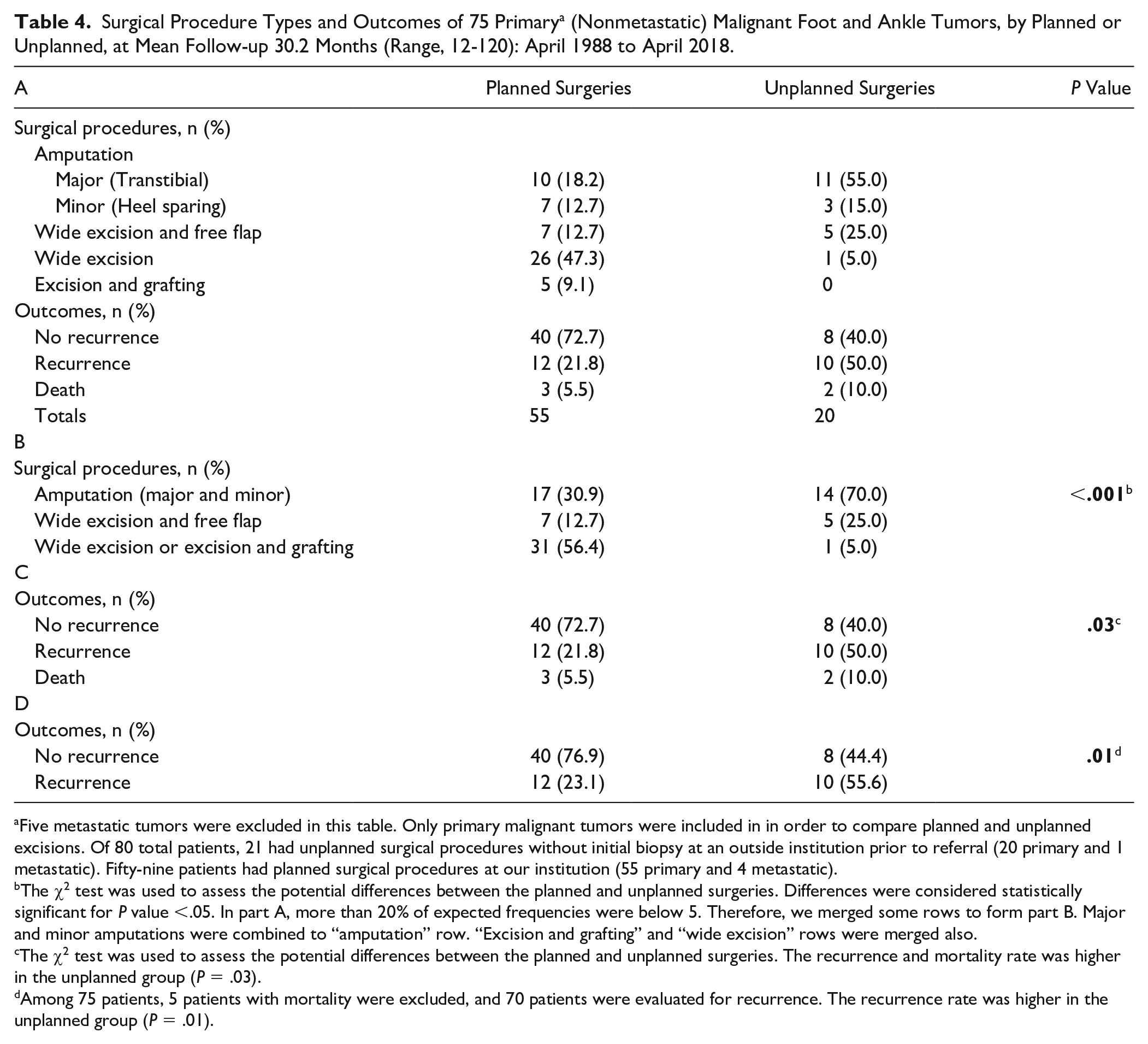
Five metastatic tumors were excluded in this table. Only primary malignant tumors were included in in order to compare planned and unplanned excisions. Of 80 total patients, 21 had unplanned surgical procedures without initial biopsy at an outside institution prior to referral (20 primary and 1 metastatic). Fifty-nine patients had planned surgical procedures at our institution (55 primary and 4 metastatic).
The χ2 test was used to assess the potential differences between the planned and unplanned surgeries. Differences were considered statistically significant for P value <.05. In part A, more than 20% of expected frequencies were below 5. Therefore, we merged some rows to form part B. Major and minor amputations were combined to “amputation” row. “Excision and grafting” and “wide excision” rows were merged also.
The χ2 test was used to assess the potential differences between the planned and unplanned surgeries. The recurrence and mortality rate was higher in the unplanned group (P = .03).
Among 75 patients, 5 patients with mortality were excluded, and 70 patients were evaluated for recurrence. The recurrence rate was higher in the unplanned group (P = .01).
Major or minor (heel-sparing) amputations were applied to 35 patients. Of these 35 tumors, 20 were treated with initially planned surgery and 15 had unplanned surgical procedures without initial biopsy prior to referral (Supplemental Table S5). Major amputation ratio was 22.0% for planned group and 57.1% for unplanned group. Major amputations were performed in 24 patients. Twenty-one of these 24 patients had transtibial amputations, and 3 of these had Syme amputations. Minor (heel-sparing) amputations were performed in 11 patients. Five of these 11 patients had Lisfranc amputations, and 3 of these had ray amputations. Two patients had toe amputation. One patient was treated with Chopart amputation (Supplemental Table S5).
One patient in our series had a metastasis from lung carcinoma located in the first metatarsal, was treated with resection and cementing followed by postoperative chemotherapy, and he died 12 months after surgery. Another patient had metastatic sites in the third and fourth metatarsals from renal cell carcinoma. Amputation was performed because there was an infected wound on the dorsum of the foot. He was without evidence of recurrence 14 months after surgery. Then he was lost to follow-up. A third patient had metastases from ovarian carcinoma to the calcaneus and talus, underwent below-the-knee amputation, but she subsequently died. A fourth patient had metastasis from lung carcinoma to fourth toe, underwent metatarsophalangeal amputation, chemotherapy was applied, and he died 5 months after surgery. A fifth patient had metastasis from lung carcinoma to hallux, underwent metatarsophalangeal amputation, chemotherapy was applied, and he died 6 months after surgery. Clinical treatment plans were decided according to multidisciplinary tumor board recommendations.
Discussion
Inadequate management of the malignant foot and ankle tumors potentially shift the treatment strategies from limb salvage toward amputation. 18 The recurrence rate for the patients in our series who were treated with planned surgery, with a mean follow-up of 30.2 months, was 20.3%, and the mortality rate was 10.1%. The highest proportion of recurrences were in patients with Enneking stage IIB and III tumors. The highest mortality rates were in those with metastases from other organs. Most foot and ankle malignant tumor recurrence rates and mortality rates reported in the literature were based on small patient populations and were stratified by histopathology or tissue of origin, but not by location or clinical stage, making it difficult for us to compare our results. In one recent study, 13 (28.3%) of 46 patients with foot and ankle malignancies who had surgery experienced recurrences, findings similar to ours. 40
Davis et al 7 evaluated whether unplanned excision in patients with extremity soft tissue sarcoma would have an impact on recurrence. They found that recurrence was higher in the unplanned surgical excision group. Munoz et al 23 compared outcomes in patients with soft tissue sarcoma treated by initial planned vs unplanned operation. They reported that local recurrence rate in the unplanned excision group was considerably higher, 73.5% vs 43.8%. Latt and colleagues 21 found that patients with unplanned excision had worse oncologic outcomes compared to others. Dean et al 8 reported that inadvertent excision was associated with a higher rate of amputation. Thacker et al 36 found that unplanned excision more often lead to local recurrence and more often necessitated free tissue transfer. We found that patients with unplanned procedures were more likely to be treated with amputation or wide excison and free flap surgery (P < .01). The recurrence and mortality rate was higher in the unplanned group (P = .03).
A great majority of the patients in our series were Enneking stage IIA (24 patients; 32.0%) or IIB (34 patients; 45.3%), and nearly half of those demonstrated extracompartmental extension. The scarcity of stage I tumors in our series is noteworthy; we suppose that misdiagnosis for more common benign lesions caused this rarity. We found that stage seemed to impact the choice of treatment. Major amputations (transtibial) were more common in advanced stages in our series.
In addition to stage, the location of tumors may also play a role in determining treatment.13,26,27 Major amputations (transtibial) and wide excision and free flap surgery were more common treatment in Kirby zone 1 and 2. Conversely, minor amputations (heel sparing) and wide excisions were more common surgical treatments in Kirby zone 3, 4, or 5. As an example, Syme amputation or wide excision with musculocutaneus flaps must often be applied to even stage IA tumors involving the calcaneus, Syme amputation is used for tarsal region tumor involvement, and below-the-knee amputation is required for lesions proximal to that. 13
Synovial sarcoma was the most common malignant soft tissue tumor, and sarcoma in our series. It represented 33.3% of the malignant soft tissue tumors (and 25.9% of all tumors), substantially lower than its prevalence in other series, which has ranged from 45% to 60% (33). Yet, only 8% of soft tissue sarcomas occur below the knee and 4% occur in the foot. Because sarcomas in general and synovial sarcoma in particular are uncommon in the foot (relative to other areas of the body), and because they are often initially thought to be benign, diagnosis is often only made after surgical excision.2,16,32,35 According to Scully et al, 31 wide resection should be considered for this select group of synovial sarcoma patients. It would seem reasonable to perform wide resection in all patients with Enneking stage IA tumors and some patients with stage IB tumors. However, almost all of the synovial sarcoma patients in our series had either stage IIA or IIB tumors (IB: 2 patients, IIA: 5 patients, IIB: 13 patients), and a great majority of them had amputation. Overall, of the 21 patients with synovial sarcoma, amputation was applied to 14 (66.7%), wide excision was applied to 3 (14.3%), and wide excision with free flap to 4 (19.0%). Nevertheless, one of the patients with synovial sarcoma in our series developed lung metastases and died 12 months after a below-the-knee amputation was performed.
In our series, 5 osteosarcomas (Figure 2) were identified in the foot (6.2%). This osteosarcoma rate is higher than those rates previously reported in the medical literature for the foot and ankle.4,12,15
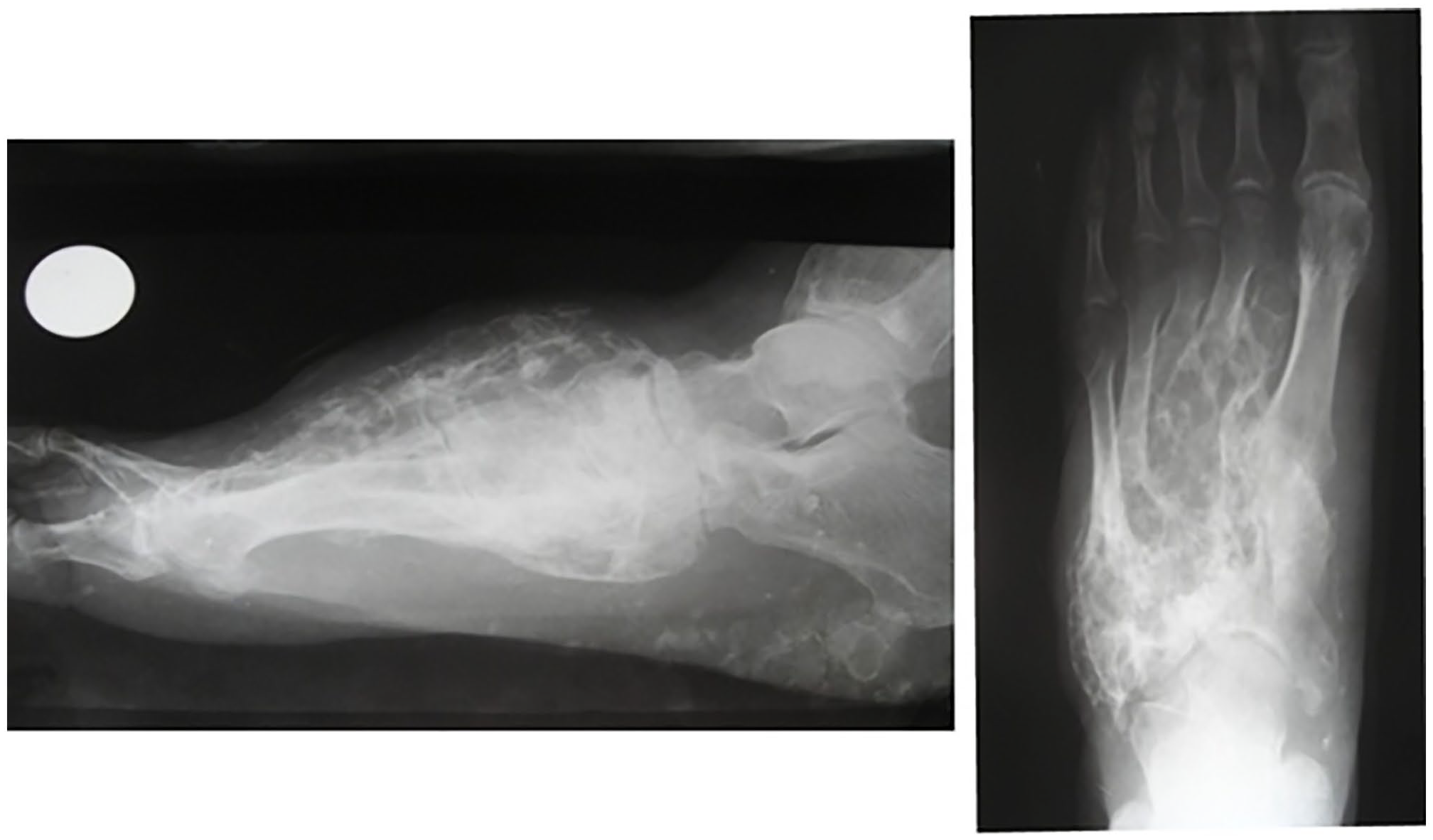
Osteosarcoma of left foot. Lateral and posteroanterior plain radiographic images of left foot, showing a representative case of a 58-year-old man with osteosarcoma involving the calcaneus and distal end of the left tibia (not shown) and all ipsilateral metatarsal bones. He underwent below-the-knee amputation followed by postoperative chemotherapy, with no local recurrence or distant metastases 23 months after surgery.
Squamous cell carcinoma of the foot and ankle was also common in our series, found in 13.5% of patients (Figure 3). Squamous cell carcinoma is found most commonly on sun-damaged skin, and according to one review it rarely occurs on the toes and feet. 6 Of interest, in that review amputation was identified as a treatment of choice for squamous cell tumors involving the foot and ankle, yet in our population only 3 of 12 patients with these tumors underwent amputation.
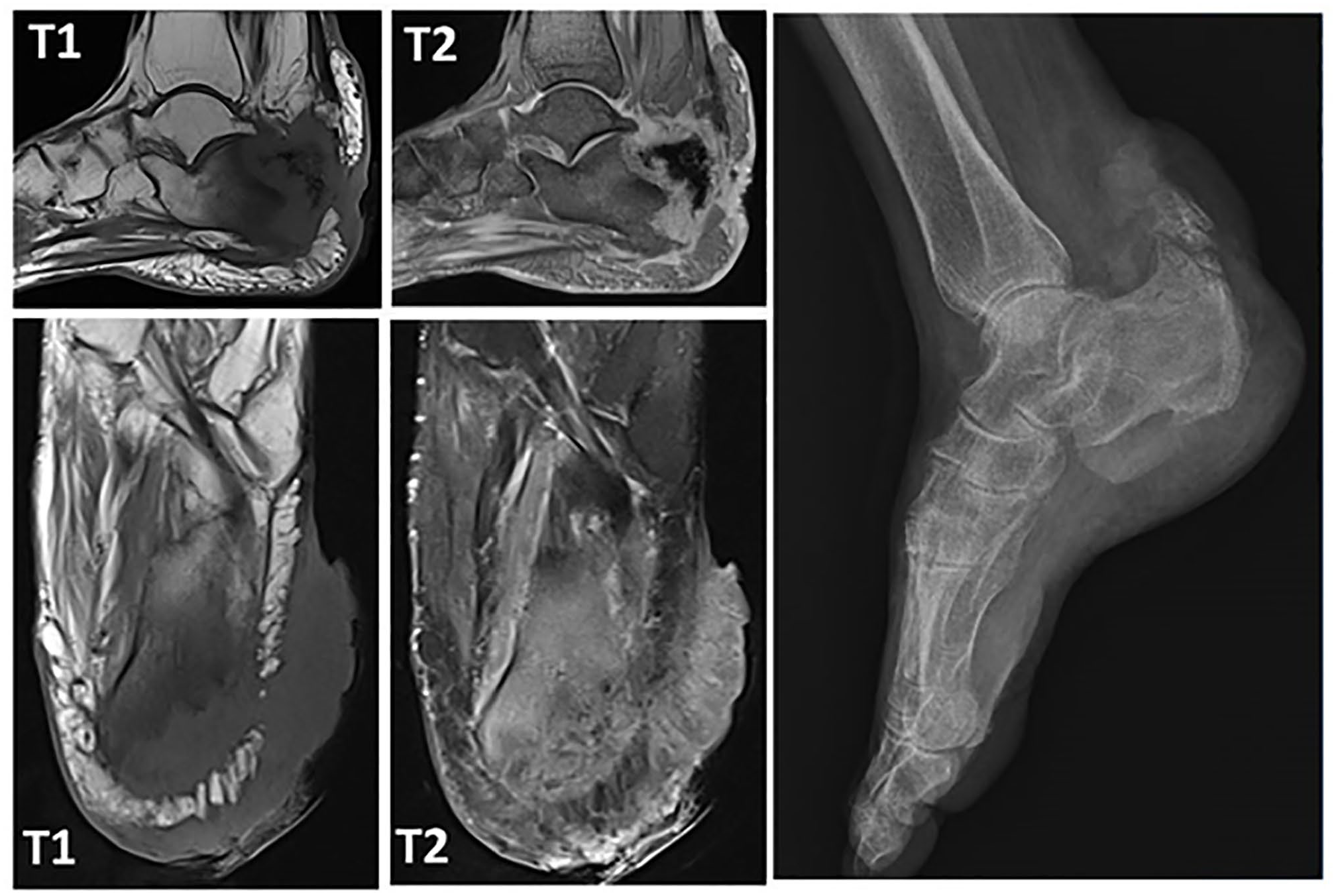
Squamous cell carcinoma of left foot. Axial and sagittal T1- and T2-weighted MRI sequences and lateral plain radiography image of the left foot showing a case of a 68-year-old woman with squamous cell carcinoma (SCC) involving the calcaneus. MRI sequences show a lesion that appears hypointense in T1-weighted and hyperintense in T2-weighted. Tru-Cut biopsy was applied and histopathologic diagnosis was reported as SCC. Transtibial amputation was performed and postoperative chemotherapy was applied. Local recurrence or metastasis was not seen 24 months after surgery. MRI, magnetic resonance imaging.
Although the most common malignant tumors found in the skeletal system are metastates from other primary sites, foot and ankle involvement are uncommon sites of metastatic spread. In our series, we identified 5 patients with malignant bone tumors that were metastases from other organs, including lung, kidney, and ovary. Lung carcinoma has been reported to be the most common malignancy metastasizing to feet.11,33 Metastatic tumors from other organs have been reported to occur in a variety of locations in the foot and ankle. 11
This study is limited by its retrospective design and inadequate number of patients for statistical comparisons of surgical modalities used and outcomes among patients with tumors of different anatomic zones, stages, or histopathologic types. Second, despite 2 years’ follow-up period, many of the malignant tumors identified may be slow to recur or metastasize, raising the possibility that the actual recurrence-free rate may be lower and the actual mortality rate may be higher than we report. The short follow-up period is one of the most important limitations of the study. If the minimum follow-up period was 5 years rather than 2 years, the number of patients in the case series would be reduced and it would be difficult to achieve statistically significant results. As it was a retrospective study, postoperative functional scores of some of the patients could not be reached. Mortality and recurrences that developed during the follow-up period of the patients were investigated. Major amputations that negatively affected the postoperative functional status of the patients were accepted as the cause of morbidity.
Another limitation of our study is we did not evaluate which biopsy techniques were more effective. Fine-needle aspiration, Tru-Cut biopsy, or incisional biopsy were evaluated in a single group as planned surgeries. Nonetheless, this article is among the largest series published to date on surgical treatment for malignant lesions of the foot and ankle in a single institute.
Conclusions
Malignant foot and ankle tumors are uncommon and can be easily missed. In patients with persistent foot and ankle pain, particularly associated with skin changes, masses, swelling, or deformity, malignancy should be kept in mind. On presentation, most tumors are identified in a moderately advanced stage, perhaps related to delayed diagnosis, and likely resulting in the need for more aggressive treatment. Radiologic and histopathologic evaluation should be completed prior to deciding on treatment (Supplemental Table S6). Both tumor location and tumor stage may serve as helpful guides during the formulation of surgical plans for these uncommon tumors, particularly with respect to choosing between limb salvage and amputation. Unplanned surgery was clearly associated with an increase the recurrence and mortality rates.
Supplemental Material
sj-docx-2-fai-10.1177_10711007221097654 – Supplemental material for Malignant Tumors of the Foot and Ankle
Supplemental material, sj-docx-2-fai-10.1177_10711007221097654 for Malignant Tumors of the Foot and Ankle by Mustafa Onur Karaca, Kerem Başarır, Abdullah Merter, Erdinç Acar, Emre ı Özbek, Mustafa Özyıldıran and Hüseyin Yusuf Yıldız in Foot & Ankle International
Supplemental Material
sj-docx-3-fai-10.1177_10711007221097654 – Supplemental material for Malignant Tumors of the Foot and Ankle
Supplemental material, sj-docx-3-fai-10.1177_10711007221097654 for Malignant Tumors of the Foot and Ankle by Mustafa Onur Karaca, Kerem Başarır, Abdullah Merter, Erdinç Acar, Emre ı Özbek, Mustafa Özyıldıran and Hüseyin Yusuf Yıldız in Foot & Ankle International
Supplemental Material
sj-docx-4-fai-10.1177_10711007221097654 – Supplemental material for Malignant Tumors of the Foot and Ankle
Supplemental material, sj-docx-4-fai-10.1177_10711007221097654 for Malignant Tumors of the Foot and Ankle by Mustafa Onur Karaca, Kerem Başarır, Abdullah Merter, Erdinç Acar, Emre ı Özbek, Mustafa Özyıldıran and Hüseyin Yusuf Yıldız in Foot & Ankle International
Supplemental Material
sj-docx-5-fai-10.1177_10711007221097654 – Supplemental material for Malignant Tumors of the Foot and Ankle
Supplemental material, sj-docx-5-fai-10.1177_10711007221097654 for Malignant Tumors of the Foot and Ankle by Mustafa Onur Karaca, Kerem Başarır, Abdullah Merter, Erdinç Acar, Emre ı Özbek, Mustafa Özyıldıran and Hüseyin Yusuf Yıldız in Foot & Ankle International
Supplemental Material
sj-docx-6-fai-10.1177_10711007221097654 – Supplemental material for Malignant Tumors of the Foot and Ankle
Supplemental material, sj-docx-6-fai-10.1177_10711007221097654 for Malignant Tumors of the Foot and Ankle by Mustafa Onur Karaca, Kerem Başarır, Abdullah Merter, Erdinç Acar, Emre ı Özbek, Mustafa Özyıldıran and Hüseyin Yusuf Yıldız in Foot & Ankle International
Supplemental Material
sj-docx-7-fai-10.1177_10711007221097654 – Supplemental material for Malignant Tumors of the Foot and Ankle
Supplemental material, sj-docx-7-fai-10.1177_10711007221097654 for Malignant Tumors of the Foot and Ankle by Mustafa Onur Karaca, Kerem Başarır, Abdullah Merter, Erdinç Acar, Emre ı Özbek, Mustafa Özyıldıran and Hüseyin Yusuf Yıldız in Foot & Ankle International
Supplemental Material
sj-pdf-1-fai-10.1177_10711007221097654 – Supplemental material for Malignant Tumors of the Foot and Ankle
Supplemental material, sj-pdf-1-fai-10.1177_10711007221097654 for Malignant Tumors of the Foot and Ankle by Mustafa Onur Karaca, Kerem Başarır, Abdullah Merter, Erdinç Acar, Emre ı Özbek, Mustafa Özyıldıran and Hüseyin Yusuf Yıldız in Foot & Ankle International
Footnotes
Ethical Approval
The study protocol received institutional review board approval (decree no. İ11-696-20).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.