
Abstract
Children with attention-deficit/hyperactivity disorder (ADHD) are at increased risk for developing secondary anxiety symptoms. While interpersonal functioning has been implicated in this comorbidity, the specific peer-related factors contributing to anxiety in youth with ADHD remain unclear. This study examined the roles of social problems, ADHD-related cognitive biases associated with peer difficulties (i.e., negative social information processing [SIP] and rejection sensitivity), and functional impairment in the relation between ADHD and anxiety symptoms. A group of U.S. parents (N = 120; 95% mothers) of 8- to 12-year-old children with elevated ADHD symptoms (58.3% [n = 70] with ADHD diagnoses) completed questionnaires, while a subset of their children (n = 69, Mage = 9.70 years, SD = 1.38; 62.3% boys) completed questionnaires and a virtual SIP task. Results indicated that social problems, anger rejection sensitivity, and functional impairment each moderated the relation between ADHD and anxiety symptoms. These findings highlight the potential role of specific peer difficulties in the development of anxiety among children with ADHD and underscore the importance of regular anxiety screening for those experiencing social challenges and functional impairment.
Attention-deficit/hyperactivity disorder (ADHD) is a chronic neurodevelopmental disorder characterized by persistent patterns of inattention, hyperactivity, and impulsivity that interfere with daily functioning (American Psychiatric Association [APA], 2022). Attention-deficit/hyperactivity disorder symptoms typically emerge before the age of 12 and can be identified as early as toddlerhood (Brown et al., 2022). Boys are typically diagnosed with ADHD earlier in childhood, whereas girls are often identified in early adolescence, partially due to boys displaying more overtly disruptive symptoms that may be more readily identified and problematic to others than girls’ early symptoms (Martin et al., 2023). Earlier onset of symptoms is often associated with more severe and persistent symptoms, as well as a greater likelihood of developing comorbidities compared with later onset (Connor et al., 2003; Karam et al., 2009; Willoughby et al., 2000). Anxiety affects approximately 40% of youth with ADHD in the general population, increasing to 57% in clinical settings, with higher prevalence among girls and far surpassing the 2% to 15% rate of anxiety found in the general pediatric population (Choi et al., 2022; Danielson et al., 2024). Co-occurring anxiety in youth with ADHD is associated with a broad range of long-term negative consequences including poorer academic performance, increased sleep disturbances, self-harm, suicide attempts, other comorbidities and treatment challenges, as well as lower quality of life in adulthood compared with ADHD alone (Bériault et al., 2018; Orm et al., 2023; Schein et al., 2023; Yoshimasu et al., 2019). Growing evidence suggests that peer relationships increase the risk of anxiety among adolescents with ADHD (Havewala et al., 2022; Mrug et al., 2012), yet few studies have examined this possibility during middle childhood.
The presentation of ADHD evolves over time, with hyperactivity and impulsivity typically being more prominent in early childhood and declining toward adolescence, whereas inattention increases over time and persists (Holbrook et al., 2016). This shift in ADHD symptoms during middle childhood and adolescence may affect peer interactions in distinct ways, which can, in turn, differentially influence the risk of anxiety. Investigating the role of peer functioning in co-occurring ADHD and anxiety earlier in development is important for determining whether youth are at risk prior to adolescence, identifying critical windows for intervention, and pinpointing modifiable targets to reduce this co-occurrence. The present study examined social problems, ADHD-related cognitive biases associated with peer difficulties (i.e., negative social information processing [SIP] and rejection sensitivity), and functional impairment in relation to co-occurring ADHD and anxiety in 8- to 12-year-old children with elevated ADHD symptoms. These data can offer developmentally sensitive insights into potential risk factors that may inform detection and prevention efforts aimed at reducing anxiety risk in children with ADHD.
Social Problems in Children With ADHD
Peer dynamics play a pivotal role in child development (Bronfenbrenner, 1971) and can significantly influence the likelihood of developing anxiety. Positive peer relationships (e.g., support and collaboration), which have been shown to reduce the risk of anxiety in youth with ADHD (Havewala et al., 2022), foster critical social and emotional skills—such as perspective-taking, problem-solving, and conflict resolution—that are essential for adaptive functioning and successful social integration in children (Davis & Allen, 2023). In contrast, negative peer relationships (e.g., bullying and exclusion), which are associated with increased anxiety risk in youth with ADHD (Mrug et al., 2012), can create a hostile social environment that disrupts the development of positive social skills and contribute to long-term adverse effects such as sleep difficulties, academic underachievement, poor quality of life, and mental health problems (Davis & Allen, 2023; D. M. Gardner & Gerdes, 2015). Children with ADHD face significantly more social problems than those without ADHD, often experiencing even greater difficulties than children with depression, anxiety, or learning disorders (Asarnow, 1988; Ekornås et al., 2011; Heiman, 2005). Increasing evidence indicates social challenges are more extensive and persistent in girls with ADHD compared with boys with ADHD (Becker et al., 2013; Blachman & Hinshaw, 2002; Owens et al., 2017; Thurber et al., 2002). Two prominent social problems faced by children with ADHD are peer rejection and a low peer support.
Peer Rejection
Peer rejection refers to the exclusion of a child from social activities or relationships by one or more of their peers (Davis & Allen, 2023). Peer rejection during middle childhood has been linked to increased anxiety, depression, aggression, hostility, and social biases (LoParo et al., 2023; Mrug et al., 2012). Approximately 56% to 82% of children with ADHD experience peer rejection, a rate that is more than three times higher than the 15% of children without ADHD (Hoza et al., 2005; Solanto et al., 2009). The association between ADHD and peer rejection can develop early in life; for example, a longitudinal study found that ADHD symptoms at age 4 predicted peer rejection by age 6, and vice versa (Stenseng et al., 2016). These findings suggest that ADHD symptoms and peer rejection are intertwined, with associations emerging as early as preschool and potentially continuing into middle childhood and beyond (Mrug et al., 2007). In addition to these negative peer interactions, children with ADHD often lack positive peer interactions, such as peer support.
Peer Support
Peer support refers to peers’ providing emotional (e.g., empathy, trust), instrumental (e.g., concrete acts), informational (e.g., advice), and/or appraisal (e.g., information that influences self-evaluation) assistance (Davis & Allen, 2023). Children with ADHD typically receive significantly less peer support than children without ADHD, even when they have comparable numbers of friends (Rokeach & Wiener, 2020; Spender et al., 2023). Generally, as children with ADHD age, their ratings of peer support and friendship quality decrease, whereas ratings by the same age children without ADHD increase (Rokeach & Wiener, 2020). Therefore, children with ADHD likely do not receive the same level of the social or emotional benefits from peer support as children without ADHD.
Peer support can have a protective role. For instance, a longitudinal study of 5- to 13-year-old children found that higher levels of peer support not only reduced the impact of ADHD symptoms on social difficulties a year later but also served as a buffer against peer rejection in children with ADHD (Mustafina et al., 2022). Similar protective effects were observed in relation to peer victimization in adolescents with ADHD (Monopoli et al., 2020). However, low peer support is associated with several negative consequences in children with ADHD, such as higher school drop-out rates, delinquent and antisocial behavior, internalizing difficulties, and an increased risk of peer victimization (Harris-Lane et al., 2021; McQuade et al., 2014). Given the impact that social problems can have on children with ADHD, it is crucial to consider the mechanisms underlying these difficulties.
Cognitive Biases Associated With Peer Difficulties in Children With ADHD
Children with ADHD are prone to exhibiting specific cognitive distortions that contribute to peer difficulties (Sibley et al., 2010; Uekermann et al., 2010). Among these, two cognitive biases are negative SIP and rejection sensitivity.
Social Information Processing
Social information processing refers to a series of mental processes through which individuals perceive, interpret, and respond to social cues and situations, influencing their behavior and interactions with others (Dodge, 1980). Children with ADHD often experience significant SIP difficulties, even when controlling for conduct problems (Andrade et al., 2012; Hammad & Awed, 2016; King et al., 2009). These difficulties can manifest in several ways, such as struggling to accurately encode social cues, interpreting neutral or ambiguous actions as hostile, and having a heightened sensitivity to negative social cues (Andrade et al., 2012; Ros & Graziano, 2018). Consequently, these SIP difficulties often lead children with ADHD to respond with inappropriate or aggressive behaviors, contributing to misunderstandings and conflicts (Hammad & Awed, 2016; Ros & Graziano, 2018; Sibley et al., 2010). For example, a child with ADHD may misinterpret a peer’s neutral facial expression or a pause in conversation as a sign of anger or rejection, prompting an outburst such as shouting or withdrawing, which can escalate the situation and lead to further social friction. In addition, SIP deficits limit social self-awareness, causing children with ADHD to struggle with accurately monitoring and assessing their own behavior, resulting in an underestimation of their peer difficulties and an overestimation of their social competence (McQuade et al., 2011; Parke et al., 2021). In contrast, peers without ADHD are generally more adept at recognizing and actively disliking behavior demonstrated by children with ADHD (Erhardt & Hinshaw, 1994). Therefore, deficits in SIP likely contribute to and exacerbate peer difficulties for children with ADHD.
Rejection Sensitivity
In addition to SIP deficits, children with ADHD often exhibit heightened rejection sensitivity. Rejection sensitivity refers to the tendency to anticipate and perceive rejection, triggering intense defensive emotional responses of either anxiety (i.e., anxious rejection sensitivity) or anger (i.e., anger rejection sensitivity) when rejection is perceived (Downey & Feldman, 1996). For example, a child with ADHD may interpret a peer’s failure to invite them to join a game as deliberate rejection, even if the peer simply forgot or was already engaged with others. This perceived rejection could prompt a defensive reaction, such as name-calling or attempting to disrupt the game, which in turn escalates the situation and further alienates the child from the group. From a social cognitive perspective, rejection sensitivity determines which social cues will be noticed and the likelihood that an interpersonal interaction will be interpreted as a “rejection” (Downey et al., 1998). This heightened sensitivity can also lead to behaviors that cause actual rejection by peers (Meehan et al., 2018). For instance, a child’s excessive worry about being left out can lead to overly clingy or controlling behaviors that push others away. This constant vigilance for rejection not only limits the benefits children with ADHD can gain from positive social relationships but also contributes to difficulties in emotion regulation, increased peer rejection, victimization, and social isolation. Importantly, rejection sensitivity also increases the risk of anxiety, as it both hinders the ability to form new friendships and distorts perceptions of existing relationships. For example, a child may believe a peer who has been distant recently is rejecting them, even if that peer is dealing with issues unrelated to the child. This sensitivity and misperception can lead to increased worry and anger about social interactions (Downey et al., 1998).
The literature is mixed regarding which specific aspects of SIP deficits and rejection sensitivity contribute to peer difficulties in youth with ADHD. Boys with ADHD are more attentive to negative peer cues and often misinterpret them as hostile, triggering aggressive reactions (Andrade et al., 2012; Waschbusch et al., 2002). Girls with ADHD, on the other hand, are more likely to anticipate negative peer reactions, resulting in defensive or inappropriate responses (Mikami et al., 2008; Thurber et al., 2002). Other youth with ADHD fail to interpret peer cues altogether, leading to poorly regulated behavior (Matthys et al., 1999; Sibley et al., 2010). Regardless, these cognitive biases create a cycle of misinterpreted social cues, defensive reactions, and social withdrawal, contributing to ongoing challenges across various environments (Ros & Graziano, 2018; Sibley et al., 2010).
While SIP deficits and rejection sensitivity play a central role in peer difficulties, their pervasive nature suggests they extend beyond peer relationships, affecting other critical areas of daily functioning. These cognitive biases shape patterns of negative thinking that contribute to functional impairment, which refers to difficulty or inability to perform routine tasks or meet demands and expectations across a range of domains (e.g., social, academic, familial; Lollar, 2008). As a result, these challenges can create long-term barriers to personal, educational, and professional success, reinforcing a cycle of impairment that persists into adulthood.
The developmental cascade theory helps explain how these chronic peer difficulties and functional impairment in multiple areas of daily life during childhood may accumulate over time (Masten & Cicchetti, 2010), leading to increased risk for anxiety and other mental health issues in adolescence and beyond. According to this theory, early challenges, such as those related to SIP deficits and rejection sensitivity, trigger a chain of negative outcomes that interact and build upon each other (i.e., cascade; Lansford et al., 2010; LoParo et al., 2023; Murray-Close et al., 2010). This cascading effect can shape broader developmental trajectories, such as career prospects, physical health, and overall mental well-being (Murray-Close et al., 2010). For example, peer rejection may lead to chronic stress, low self-esteem, and maladaptive coping strategies (e.g., avoidance, school disengagement, substance use), which limit social and academic development, ultimately contributing to lower educational attainment, employment challenges, and long-term interpersonal difficulties. To disrupt the cascade of effects that stem from ADHD-related difficulties, it is essential to identify specific areas of impairment and mechanisms of these pathways, enabling the identification of malleable intervention targets that can effectively reduce anxiety risk in children with ADHD.
The Current Study
The goal of the current study was to examine whether social problems, ADHD-related cognitive biases associated with peer difficulties (negative SIP and rejection sensitivity), and functional impairment are associated with and moderate the relation between ADHD and anxiety in a sample of 8- to 12-year-old children with elevated ADHD symptoms. This study extends the literature on anxiety risk among youth with ADHD in three main ways: (a) both peer problems and cognitive biases that contribute to these difficulties were considered, helping to identify underlying risk factors that could inform early intervention and prevention efforts before peer problems emerge; (b) the cumulative effect of functional impairment across multiple domains on anxiety risk was assessed, providing initial empirical support for this theory; and (c) school-age children, a younger population than in prior studies, were examined to explore whether there are critical developmental windows during which peer functioning increases vulnerability to anxiety.
Our hypotheses were structured cumulatively, with each building on the previous to examine an additional layer of the proposed model. This approach reflects prior research indicating that ADHD symptoms are linked to cognitive biases and peer difficulties which may subsequently contribute to anxiety (Havewala et al., 2022; Mikami et al., 2011; Mrug et al., 2012; Sibley et al., 2010). First, we hypothesized that social problems and ADHD-related cognitive biases (i.e., negative SIP and rejection sensitivity) would be independently associated with both ADHD and anxiety symptoms. Second, we hypothesized that these peer factors, along with functional impairment, would strengthen the association between ADHD and anxiety symptoms. Although the pattern of associations (e.g., ADHD predicting peer problems that, in turn, contribute to the development of anxiety) may suggest mediation, the cross-sectional design limits testing hypotheses of causal inference. Instead, moderation analyses were used to test whether peer difficulties and functional impairment intensified the relation between ADHD and anxiety symptoms, consistent with the developmental cascade theory (Masten & Cicchetti, 2010).
Method
Participants
Participants were parents (N = 120, Mage = 39.75, SD = 5.51) of 8- to 12-year-old children with elevated ADHD symptoms (M = 11.21 years, SD = 3.06), and a subset of their children (n = 69, Mage = 9.70 years, SD = 1.38). Parents reported that 58.30% of their children (n = 70) had previously been diagnosed with ADHD; 46.70% of their children (n = 56) were prescribed psychiatric medication at the time of the study. Parents were 95% mothers (n = 114) and 5% fathers (n = 6), with 79.2% (n = 95) being married, 78.33% (n = 94) holding a bachelor’s degree or higher, and 68.33% (n = 82) reporting household incomes of $75,000 or more; their racial/ethnic identification was reported as 11.67% (n = 14) Black/African American, 0.83% (n = 1) Pacific Islander/Native Hawaiian, 80% (n = 96) White/Caucasian, 5.83% (n = 7) multiracial, 0.83% (n = 1) as Other, and 0.83% (n = 1) preferred not to answer.
Children included 37.70% (n = 26) girls and 62.30% (n = 43) boys; their racial/ethnic identification was reported as 10.10% (n = 2) Black/African American, 1.40% (n = 1) Pacific Islander/Native Hawaiian, 78.30% (n = 54) White/Caucasian, 2.90% (n = 7) multiracial, 4.32% (n = 3) as Other, and 2.88% (n = 2) preferred not to answer. Children had the following grade distribution: 14.20% (n = 17) in 2nd, 19.20% (n = 23) in 3rd, 23.30% (n = 28) in 4th, 22.50% (n = 27) in 5th, 12.50% (n = 15) in 6th, and 8.30% (n = 10) in 7th; 75.80% (n = 91) attended public school. Parents reported that 71.01% (n = 49) of children have begun puberty.
A priori clinical inclusion criteria stipulated that children have a total of at least six symptoms across the two ADHD clusters (i.e., inattention or hyperactivity/impulsivity) and impairment in at least one functional domain (e.g., family, peers, school). In addition, both parents and children needed to be proficient in written and spoken English, have access to the internet, and live in either the Eastern or Central Time zones. Children with prior diagnoses of autism spectrum disorder or intellectual developmental disorder, as well as parents who did not have at least 50% custody of their child, were excluded from the study.
Although a total of 368 screeners were submitted, only 18.80% (n = 69) of these individuals completed all stages of the current study. Among the remaining 81.30% (n = 299) who did not complete the study: 1.10% (n = 4) did not complete enough screener items to assess eligibility; 19.60% (n = 72) were ineligible per predetermined study criteria; 20.40% (n = 75) were lost to follow-up after the screener; 13.90% (n = 51) were lost to follow-up after the parent questionnaires; and 26.40% (n = 97) were later deemed ineligible (e.g., no child in the required age range) after initial screening procedures.
Measures
Demographics
Parents reported the parent and child’s age, and the child’s sex assigned at birth, gender identity (these responses were identical to sex assigned at birth for the present sample), race, ethnicity, clinical psychiatric diagnostic status, child psychiatric medication status, pubertal status, grade level, and school type (e.g., public, private). In addition, parents reported their level of education, relationship status, and family household income.
ADHD and Anxiety Symptoms
The Vanderbilt ADHD Parent Rating Scale (VAPRS; Wolraich et al., 2004) was administered as a screener of children’s ADHD symptoms for study eligibility. Parents rated their child’s ADHD symptoms (18 items) on a 4-point scale (0 = Rarely or never, 1 = Sometimes, 2 = Often, 3 = Very Often), with responses of 2+ indicating the presence of a symptom. At least six symptoms were required to be present for children to be included in the current study.
For the main analyses, the DSM-oriented subscales of the Child Behavioral Checklist (CBCL; Achenbach & Edelbrock, 1981) were administered. Parents rated their child’s ADHD (7 items) and anxiety (6 items) symptoms on a 3-point scale (0 = not true, 1 = sometimes true, 2 = very often or often true), with higher values indicating greater symptom severity. Items were summed to yield scores for the ADHD subscale (α = .78; N = 120, M = 10.28, SD = 2.92, Minimum = 1, Maximum = 14) and the anxiety subscale (α = .82; N = 120, M = 5.12, SD = 3.31, Minimum = 0, Maximum = 12).
Functional Impairment
The Impairment Rating Scale (IRS; Fabiano et al., 2006) was administered as a screener of children’s impairment for study eligibility. Parents rated their child’s level of problems in different domains (i.e., peers, siblings, parents, academics, self-esteem, overall family functioning, overall severity of impairment; 7 items) on a 7-point scale (anchors of 0 = No problem—Does not need intervention and 6 = Extreme problem—Needs intervention), with scores of 3+ indicating clinical impairment. To be included in the study, parents must have rated their child as being clinically impaired (i.e., 3+) in at least one functional domain. Functional impairment scores were calculated by counting the number of domains in which a score of 3 or higher was rated (α = .90; N = 120, M = 4.60, SD = 1.96, Minimum = 1, Maximum = 7 domains).
Social Problems
An aggregate of three measures was used to assess social problems. First, parents (N = 120) completed the Social Problems subscale of the CBCL (Achenbach & Edelbrock, 1981), in which they rated their child’s social functioning (10 items) on a 3-point scale (0 = not true, 1 = sometimes true, 2 = very often or often true). Second, children (n = 69) completed several items that assess peer rejection: one item from the Social Interactions Survey (DeRosier, 2002; 2004), the single-item version of the Peer Affiliation scale (Gavin & Furman, 1989), and two items previously used to assess peer rejection among school-age children (Zimmer-Gembeck et al., 2013). A meta-analysis on peer rejection indicated that it is common to assess peer rejection using a few items drawn from multiple measures (Yue & Zhang, 2023). And third, children (n = 69) completed the Survey of Children’s Social Support (Dubow & Ullman, 1989), in which they rated their peer support (14 items) on a 5-point scale (1 = Never, 2 = Hardly ever, 3 = Sometimes, 4 = Most of the time, 5 = Always); this measure was reverse scored to match the valence of the other indices before creating a composite measure.
These three indices of social problems (i.e., parent report of social problems, child report of peer rejection, child report of peer support) were z-scored and then combined using a weighted average to yield a composite score of social problems (α = .87; n = 120, M = .01, SD = .65, Minimum = −1.48, Maximum = 2.30) with higher values indicating greater social problems. This approach standardizes individual measures to ensure each report is properly weighted according to its sample size. When child-report data were missing, the available parent-report was used instead. Retaining available ratings, rather than discarding incomplete cases, is recommended when data are not missing at random, as it helps reduce bias and improve accuracy, particularly in psychological and social science research (Blozis et al., 2013; Little et al., 2012; Park et al., 2023). Multi-informant composite measures provide distinct yet complementary information, mitigate the effects of missing data, enhance reliability and validity, reduce the number of analyses (minimizing Type 1 errors) without losing information, and offer better predictions of psychopathology than single-informant measures (McKenna & Heaney, 2020; Van Dulmen & Egeland, 2011).
Rejection Sensitivity
The Children’s Rejection Sensitivity Questionnaire (CRSQ; Downey et al., 1998) was administered during the virtual lab visit. Children read six hypothetical vignettes describing social situations and reported how nervous and angry they would feel on a 6-point scale (anchors of 1 = Not nervous/mad and 6 = Very very nervous/mad), with higher values indicating greater rejection sensitivity. Items were averaged to yield scores for the anxious rejection sensitivity subscale (α = .80; n = 69, M = 10.94, SD = 5.09, Minimum = 1.83, Maximum = 26.83) and the anger rejection sensitivity subscale (α = .80; n = 69, M = 14.37, SD = 5.79, Minimum = 4.22, Maximum = 32.44).
Social Information Processing
The SIP Task (Dodge, 1980) was used to assess children’s SIP for the main analyses. The use of social vignettes has been well-validated to evaluate the steps of SIP in male and female children with ADHD (Andrade et al., 2012; Hammad & Awed, 2016; King et al., 2009).
SIP Task Administration
Children listened to a series of eight short stories about children engaging in various ambiguous social interactions while being shown a cartoon picture that helped depict the story. Study staff read the stories in a randomly generated order to avoid order effects. Children were instructed to pretend as if they were the protagonist in each of the stories. Immediately after each story and picture, children were asked the following three questions: 1. What happened in the story? 2. How could you tell whether this was a nice way to act or a mean way to act? 3. What could you say or do if this happened to you? Tell me as many ways as you can.
SIP Coding
Children’s responses were double-coded, where the second coder was masked to the initial coding. The frequency and negative valence of the four domains of SIP were coded and interrater reliability (intraclass correlation coefficients [ICC]) were computed: social cue detection (ICC = .92), intent attribution (ICC = .90), outcome attribution (ICC = .91), and response generation (ICC = .87). Scores for each SIP domain were summed across the stories, and a composite average of the four negative SIP indices was calculated to yield an overall negative SIP score (n = 69, M = 4.27, SD = 1.05, Minimum = 1.35, Maximum = 6.69), with higher values indicating greater negative SIP. This method is commonly used to compute total valence scores from cognitive bias tasks with children, including the SIP task (Van Cappellen et al., 2023).
Procedures
This research was supported by the University of Louisville research funds (Bufferd). All study procedures were approved by the Institutional Review Board at the University of Louisville. Parental consent was obtained during the study screener, and child assent at the start of the virtual lab visit. The study was conducted entirely online, utilizing secure programs to administer questionnaires (REDCap), schedule (Calendly) and conduct (Microsoft Teams) the virtual lab visit. Participants were recruited using the following methods: flyers shared with psychology clinics/mental health practices, pediatricians, and school parent–teacher associations; paid Facebook advertisements; and the snowball sampling method (i.e., participants were asked to send the survey to other families). Interested parents completed an online screener survey, and eligible participants were sent links to parent questionnaires and virtual lab visit scheduling. During the virtual lab visit, children were administered the SIP task by trained study staff and then completed the child questionnaires. Children were shown a brief video of baby animals to restore their pre-survey state. Virtual lab visits were recorded for later task coding. Parents were compensated upon completion of the virtual lab visit ($15 gift card).
Data Analytic Plan and Preparation
All questionnaires mandated item completion, excluding aspects of the demographics form, to limit missing data. As a result, there were no missing data within completed parent or child questionnaires. However, a considerable proportion of families were lost to follow-up after completing the parent questionnaires, leading to fewer corresponding child responses. Given that missing child data resulted from study attrition rather than partial item nonresponse, and entire measures were missing rather than individual data points, data imputation was not appropriate. Instead, analyses proceeded with all available parent- and child-reported cases. Child measures contributing to the composite social problems score were standardized and combined using a weighted average to account for differences in sample size. Independent child measures were analyzed using robust statistical methods. All analyses were conducted in SPSS.
Attrition analyses (two-tailed) were conducted to determine whether participants who completed the virtual lab visit and those who were lost to follow-up significantly differed across demographic and clinical characteristics. Independent samples t-tests were computed to compare children’s ADHD, anxiety, functional impairment, and puberal status, while chi-square tests of independence were computed to compare children’s age, psychiatric diagnostic and medication status, sex assigned at birth, family income, parent education, and parent marital status.
Bivariate correlations were computed to examine associations between each of the primary and demographic variables, and to identify potential covariates. Covariates were included based on significant associations with the outcome variables in the present sample to prevent model overfitting and maintain statistical power (Hripcsak et al., 2024; Witte & Didelez, 2019). Next, a series of hierarchical regression analyses were computed to examine whether ADHD symptoms uniquely accounted for variance in social problems, negative SIP, anxious rejection sensitivity, and anger rejection sensitivity while controlling for demographic covariates. Additional hierarchical regression analyses were computed to assess whether these peer variables (social problems, negative SIP, anxious rejection sensitivity, and anger rejection sensitivity) uniquely accounted for variance in anxiety symptoms, while controlling for demographic covariates.
Finally, moderation analyses were computed using Process Macro model 1 (with 5,000 bootstrapping samples and mean centering) to examine social problems, negative SIP, anxious rejection sensitivity, anger rejection sensitivity, and functional impairment as moderators of the relation between ADHD (independent variable) and anxiety symptoms (dependent variable), while controlling for demographic covariates.
Results
Attrition Analyses
Among the 120 families who completed parent questionnaires, 57.5% (n = 69) also provided child data during the virtual lab visit, whereas 42.5% (n = 51) were lost to follow-up and had only parent-reported data. Anxiety symptoms were significantly higher among participants lost to follow-up (M = 5.97, SD = 3.45) compared with those who completed the virtual lab visit (M = 4.92, SD = 3.24, p = .011). In addition, children diagnosed with ADHD were more likely to be lost to follow-up (54.29%; n = 38) compared with those without an ADHD diagnosis (42.86%; n = 30). No other significant differences in demographic or clinical characteristics were found between those who completed the virtual lab visit and those lost to follow-up (Supplemental Table 1 presents all attrition analyses). Considering the central role of anxiety symptoms and ADHD diagnosis in this study, excluding participants with only parent data could reduce the generalizability and clinical relevance of the findings to populations most at risk. Therefore, these cases were included in the primary analyses.
Bivariate Correlations
Bivariate correlations were computed between all the primary and demographic variables (see Table 1). Correlations between dependent variables and relevant demographic characteristics were examined for covariates to be included in regression analyses. Child age (r = .11, p = .045), child psychiatric medication status (r = .20, p = .029), child psychiatric diagnostic status (r = .19, p = .036), and child grade (r = .20, p = .025) were significantly associated with social problems. Child sex assigned at birth (r = .29, p = .015) was significantly associated with negative SIP. Child age (r = .24, p = .044) was significantly associated with anxious rejection sensitivity. Parent marital status and child psychiatric diagnostic status were significantly associated with functional impairment (r = −.19, p = .043 Parent Marital Status ; r = .14, p = .040 Child Diagnostic Status ) and anxiety symptoms (r = −.24, p = .009 Parent Marital Status ; r = .30, p = .005 Child Diagnostic Status ). No significant demographic covariates emerged for analyses estimating anger rejection sensitivity, and thus a correlation analysis was used to examine whether it was significantly associated with ADHD symptoms.
Descriptives and Bivariate Correlations Among Primary and Demographic Variables
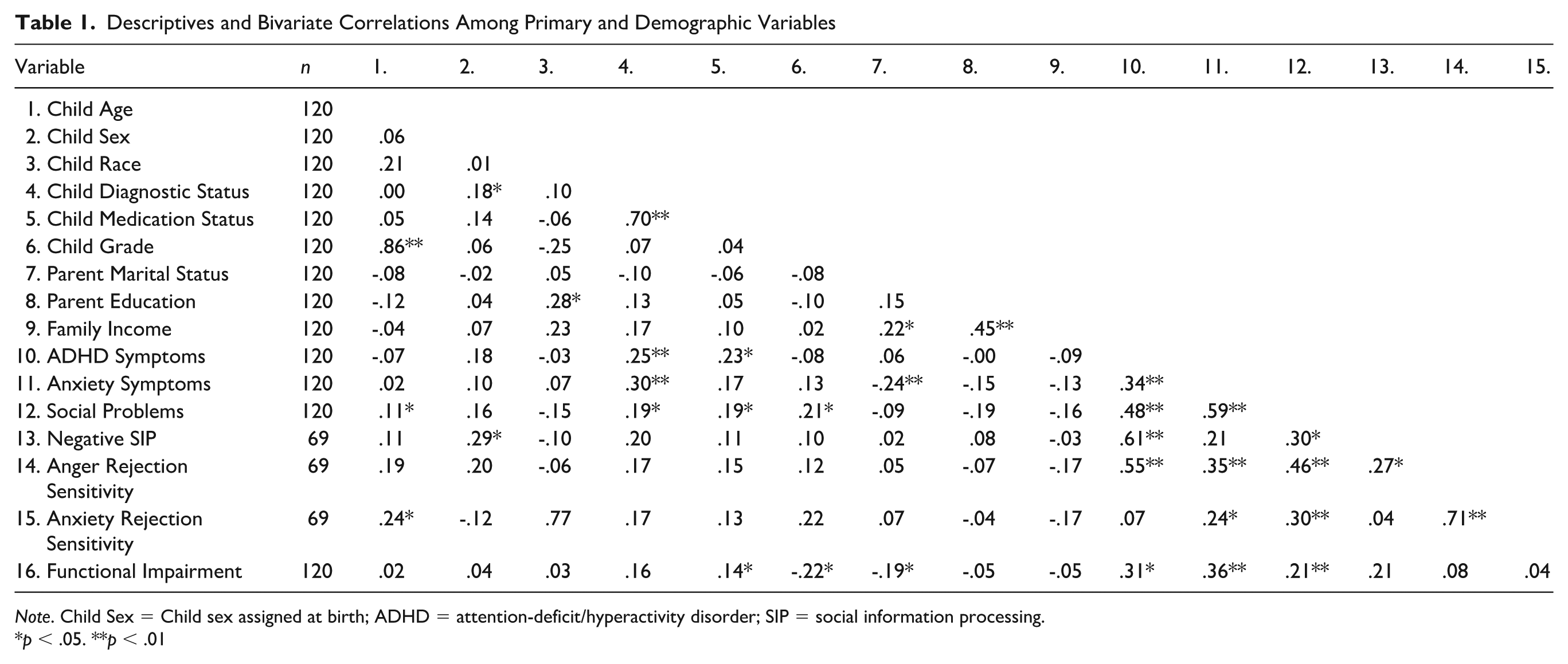
Note. Child Sex = Child sex assigned at birth; ADHD = attention-deficit/hyperactivity disorder; SIP = social information processing.
p < .05. **p < .01
Associations Between ADHD Symptoms, Anxiety Symptoms, and Peer Factors
Full hierarchical regression statistics for models examining ADHD as a predictor of peer factors are presented in Table 2.While controlling for demographic covariates, ADHD symptoms accounted for significant variance in social problems (B = .15, SE = .02, t = 6.00, p < .001), negative SIP (B = .22, SE = .04, t = .5.71, p < .001), and functional impairment (B = .85, SE = .24, t = 3.51, p < .001), but did not significantly estimate anxious rejection sensitivity. ADHD symptoms were significantly positively associated with anger rejection sensitivity (r = .553, p < .001; a regression was not run given the absence of associations between demographic variables and anxious rejection sensitivity). Full hierarchical regression statistics for models examining peer factors as predictors of anxiety symptoms are presented in Table 3. While controlling for demographic covariates, social problems (B = 2.76, SE = .37, t = 7.45, p < .001), anger rejection sensitivity (B = .18, SE = .06, t = 2.79, p = .007), and functional impairment (B = .12, SE = .04, t = 3.43, p < .001) each independently accounted for significant variance in anxiety symptoms. In contrast, neither anxious rejection sensitivity nor negative SIP significantly estimated anxiety symptoms.
Summary of Regressions Estimating Associations Between ADHD Symptoms and Peer Factors
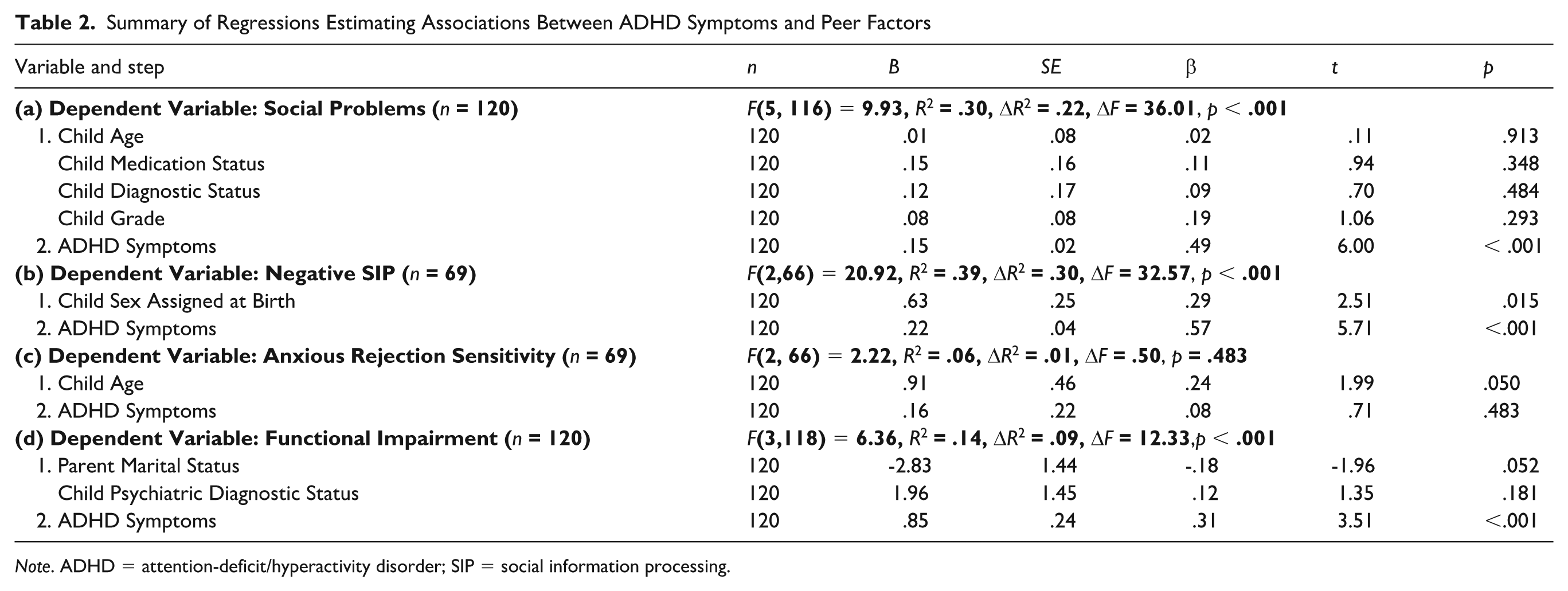
Note. ADHD = attention-deficit/hyperactivity disorder; SIP = social information processing.
Summary of Regressions Estimating Associations Between Anxiety Symptoms and Peer Factors
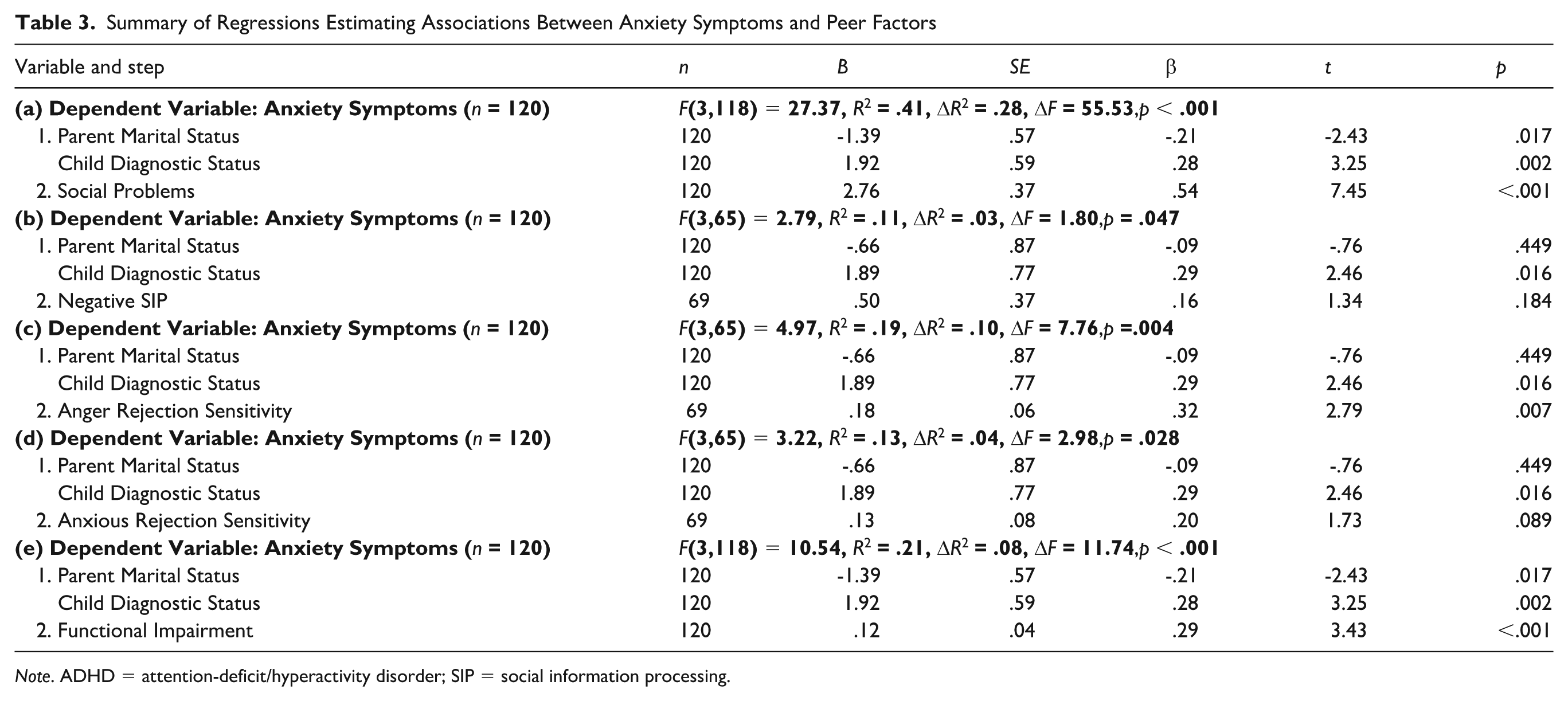
Note. ADHD = attention-deficit/hyperactivity disorder; SIP = social information processing.
Moderators of the Relation Between ADHD and Anxiety Symptoms
Five moderation models were tested, each controlling for parent marital status and child psychiatric diagnostic status; complete moderation statistics can be found in supplemental tables. There was a significant and positive ADHD × Social Problems interaction on anxiety symptoms (b = .28, SE = .16, t = 1.81, 95% confidence interval [CI] = [−.03, .59], p = .017). The relation between ADHD and anxiety symptoms was significant only at higher levels of social problems (b = .28, SE = .15, t = 1.86, 95% CI = [−.02, .57], p = .010), but not at lower levels social problems (b = −.09, SE = .13, t = −.70, 95% CI = [−.34, .16], p = .317). This moderation suggests that the relation between ADHD and anxiety symptoms is strengthened as children experience more social problems (see Figure 1).
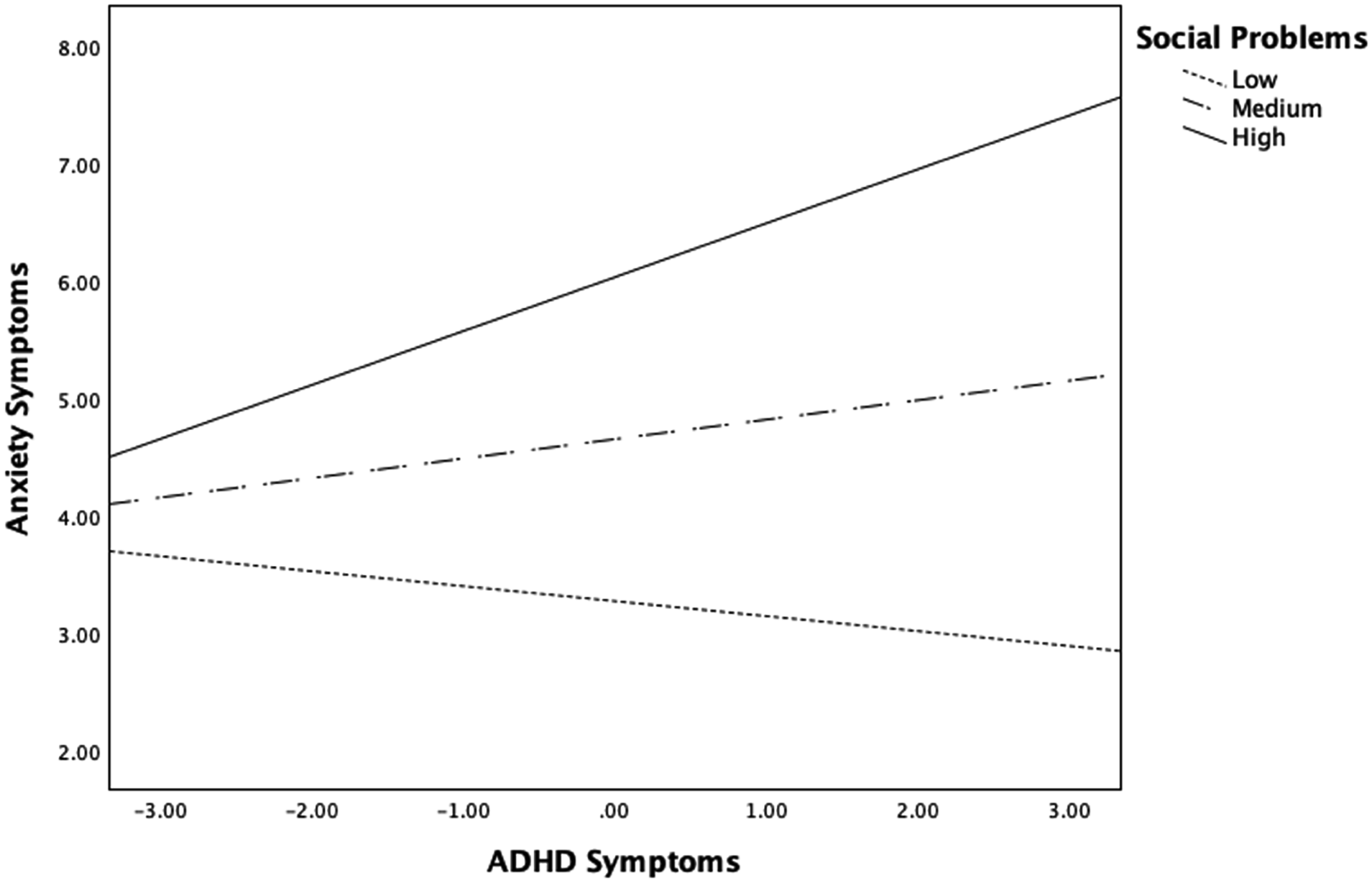
Social Problems Moderates the Relation Between ADHD Symptoms and Anxiety Symptoms
Although approaching significance, a significant ADHD × Negative SIP interaction on anxiety symptoms did not emerge (b = .18, SE = .09, t = 1.98, p = .051).
A significant ADHD × Anxious Rejection Sensitivity interaction on anxiety was not found (b = −.03, SE = .03, t = −1.06, p = .295), indicating that a moderation was not observed.
There was a significant ADHD × Anger Rejection Sensitivity interaction on anxiety (b = .21, SE = .01, t = 2.55, 95% CI = [.03, .41], p = .011). The relation between ADHD and anxiety symptoms was significant only at higher levels of anger rejection sensitivity (b = .55, SE = .15, t = 3.60, 95% CI = [.25, .86], p < .001), but not at lower levels of anger rejection sensitivity (b = .14, SE = .09, t = 1.48, 95% CI = [−.05, .32], p = .144). This moderation suggests that the relation between ADHD and anxiety symptoms is strengthened as children experience greater anger rejection sensitivity (see Figure 2).
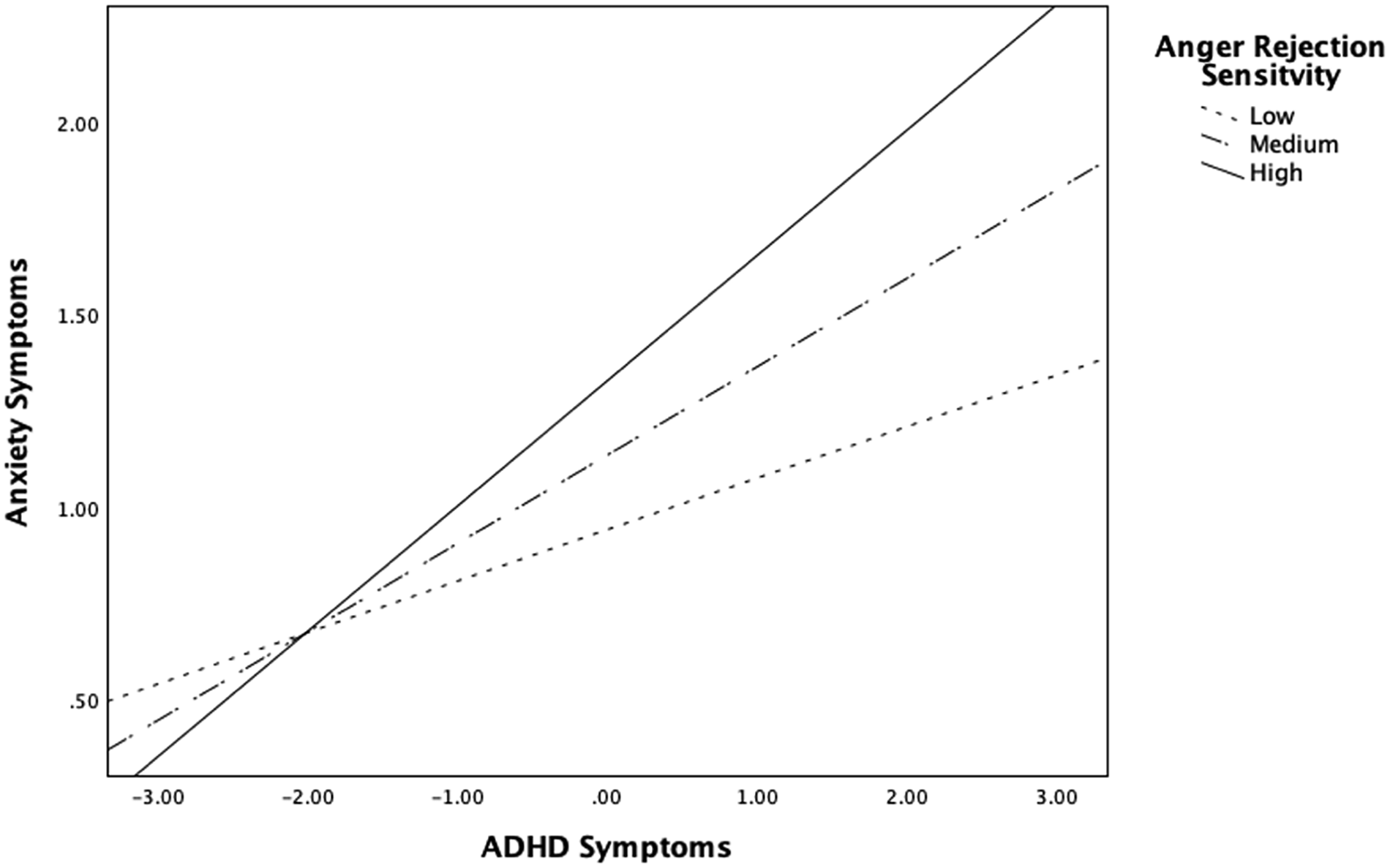
Anger Rejection Sensitivity Moderates the Relation Between ADHD Symptoms and Anxiety Symptoms
There was a significant ADHD × functional impairment interaction on anxiety (b = .11, SE = .05, t = 2.35, 95% CI = [.02, .20], p = .020). The relation between ADHD and anxiety symptoms was significant only when children experienced functional impairment in a greater number of domains (b = .36, SE = .10, t = 3.63, 95% CI = [.16, .55], p < .001) but was not significant when children experienced clinical impairment in a fewer number of domains (b = .09, SE = .13, t = .72, 95% CI = [−.17, .35], p = .476). This moderation suggests that the relation between ADHD and anxiety symptoms is strengthened as children experience impairment across a greater number of functional domains (e.g., school, interpersonal, family; see Figure 3).
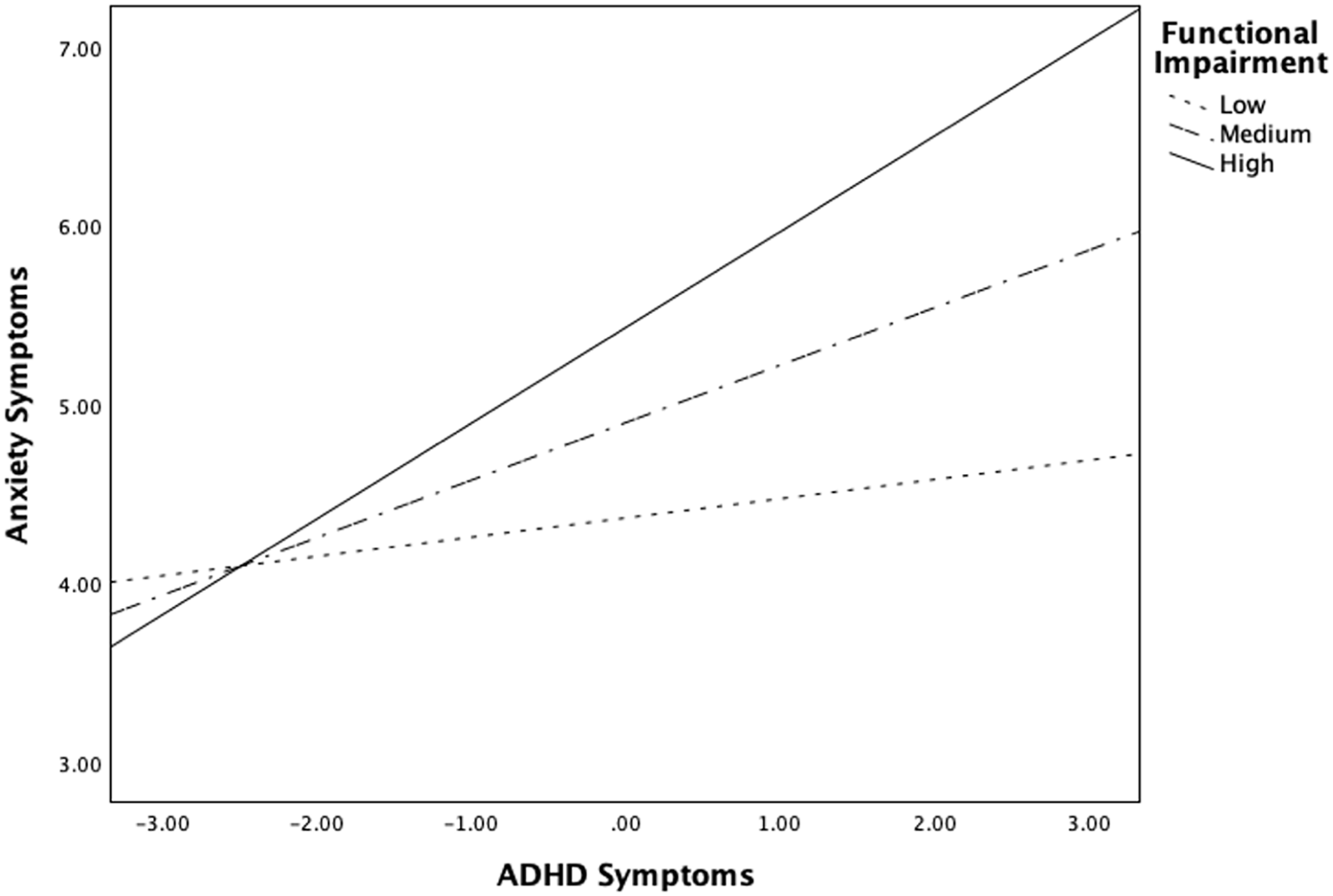
Functional Impairment Moderates the Relation Between ADHD Symptoms and Anxiety Symptoms
Discussion
To our knowledge, this is the first study to examine social problems, ADHD-related cognitive biases associated with peer difficulties (i.e., negative SIP and rejection sensitivity), and functional impairment in relation to co-occurring ADHD and anxiety in school-age children with elevated ADHD symptoms. Results revealed that, while accounting for relevant demographic covariates, ADHD and anxiety symptoms were independently associated with social problems, anger rejection sensitivity, and functional impairment. In addition, social problems, anger rejection sensitivity, and functional impairment significantly moderated the relation between ADHD and anxiety symptoms.
Bivariate correlations revealed several significant demographic covariates. Child age, psychiatric diagnosis, medication status, and grade were positively correlated with social problems, aligning with research indicating that social difficulties increase with age and are more common in youth with mental health concerns (Blachman & Hinshaw, 2002; Davis & Allen, 2023; McQuade et al., 2014). In addition, parent marital status and child psychiatric diagnosis were positively correlated with functional impairment and anxiety, highlighting the role of family dynamics in children’s well-being. For instance, changes or instability in family structure, such as divorce, may introduce additional stressors, reduce social or emotional support, or alter caregiving, all of which can contribute to heightened anxiety and impaired functioning. As predicted, ADHD symptoms estimated social problems, and social problems estimated anxiety symptoms. However, due to the cross-sectional nature of analyses, causality cannot be inferred from our results. Despite this limitation, these findings are consistent with prior work showing that ADHD symptoms predicted greater social problems, peer rejection, and lower peer support in youth with ADHD (Bustinza et al., 2022; Mrug et al., 2007), and that these peer-related factors predicted greater anxiety in children (Havewala et al., 2022; LoParo et al., 2023).
Furthermore, social problems significantly moderated the relation between ADHD and anxiety symptoms, such that the association between ADHD and anxiety was strengthened as children experienced more social problems. This finding is consistent with a previous study in which peer support at age 12 years buffered the effects of ADHD symptoms at age 7 years on anxiety symptoms at age 15 years in youth with low behavioral inhibition (Havewala et al., 2022) and builds on the literature by identifying a negative peer relationship as a moderator of the relation between ADHD and anxiety in school-age children. Notably, peer victimization was not a significant moderator in this previous study. This difference in findings may be explained by methodological variations (such as their longitudinal design and a sample with low behavioral inhibition) or developmental factors, as they assessed peer factors and anxiety during adolescence. However, it could also reflect that multiple or co-occurring peer problems might have a stronger impact on anxiety than a single, though severe, type of peer problem, like peer victimization.
Negative SIP was independently associated with ADHD, but not with anxiety symptoms, and it did not moderate the relation between ADHD and anxiety. While the association with ADHD is consistent with existing literature on SIP in children with ADHD (Andrade et al., 2012; Hammad & Awed, 2016; King et al., 2009), the lack of an association with anxiety differs from previous studies that found negative SIP to be a significant predictor of anxiety (Luebbe et al., 2010). This discrepancy may be due to the current study focusing on children with elevated ADHD symptoms, while prior research often involved community samples. It is possible that ADHD symptoms reduce the relationship between negative SIP and anxiety. For instance, many children with ADHD display a positive illusory bias, overestimating their abilities and underestimating their difficulties (Bourchtein et al., 2017). In addition, children with ADHD tend to attribute their challenges to external factors (e.g., others’ actions, situational causes) rather than their own behavior (Hoza et al., 2000). These cognitive patterns may reduce the likelihood that children with ADHD internalize difficulties associated with negative SIP, potentially buffering against anxiety and partially explaining the lack of a moderating effect in this study.
Interestingly, the results showed that ADHD and anxiety symptoms were independently associated with anger rejection sensitivity, but not with anxious rejection sensitivity. Furthermore, anger rejection sensitivity, but not anxious rejection sensitivity, moderated the relation between ADHD and anxiety symptoms. Specifically, the association between ADHD and anxiety symptoms was stronger as children experienced higher levels of anger rejection sensitivity. The null findings related to anxious rejection sensitivity were unexpected, given the substantial evidence linking anxiety rejection sensitivity to ADHD symptoms (Bondü & Esser, 2015) and the development of anxiety in children and young adults, both cross-sectionally and over time (Downey et al., 1998). However, studies on ADHD have typically examined total rejection sensitivity (anxious and anger). It is possible that the anger component influenced the results in these previous studies, whereas the anxious component may be less strongly associated with ADHD.
The findings from the present study suggest that the relation between anger rejection sensitivity and anxiety may be more pronounced in children with elevated ADHD symptoms, compared with community samples of youth, where similar associations emerge between anxiety and both anxious and anger rejection sensitivity (McDonald et al., 2010). This discrepancy may be explained by the high levels of emotion dysregulation common in youth with ADHD (Anastopoulos et al., 2011), as these children are more likely to experience and express anger intensely when feeling rejected. This impulsive anger response can escalate rapidly (A. A. Gardner et al., 2020), leading to stress and worry that contribute to anxiety. In contrast, anxiety-driven rejection sensitivity may involve more internalized, slower-building emotional responses, which are less typical of children with ADHD, making the anger component a more influential factor in the co-occurring ADHD and anxiety.
Finally, the results showed that functional impairment was independently associated with and moderated the relation between ADHD and anxiety symptoms. Specifically, we found that the association between ADHD and anxiety symptoms is strengthened as children experience impairment across a greater number of functional domains (e.g., interpersonal, academic, family, self-concept). This finding supports theories suggesting that chronic and pervasive impairment in children with ADHD may heighten the risk of anxiety (Alacha et al., in press; Lilienfeld, 2003). In addition, this novel finding indicates that addressing difficulties in peer relations alone may not fully mitigate anxiety risk in children with ADHD, highlighting the importance of considering a broader range of functional domains and their interactions.
Strengths, Limitations, and Future Research Directions
The current study used a multi-informant, multi-method approach to examine how social problems, underlying cognitive biases, and functional impairment are associated with the relation between ADHD and anxiety symptoms in a clinical sample of youth during a potentially sensitive developmental period. Despite these strengths, several limitations should be considered.
First, the cross-sectional design of the current study limits the ability to draw causal or directional conclusions. As a result, it is unclear whether ADHD symptoms lead to peer difficulties that subsequently increase anxiety symptoms, as hypothesized, or if the relationship works in the opposite direction. Second, while participants had elevated ADHD symptoms, we did not conduct an evidence-based assessment to determine whether they met the full diagnostic criteria for ADHD, relying solely on parent report. Therefore, it is uncertain whether the participants experienced the same level of social problems, cognitive biases, and/or impairment as children who meet the full criteria for ADHD. The associations between ADHD, anxiety, and peer factors may be stronger in cases of more severe ADHD. In addition, children with elevated ADHD symptoms—rather than peer functioning or anxiety difficulties—were recruited. Consequently, 54.2% (n = 65) of participants scored in the bottom 25% on social problems (M = 6.75, SD = 4.70), and while the average number of anxiety symptoms was moderate (M = 5.12, SD = 3.31), it is unclear whether these anxiety symptoms developed before or as a result of the ADHD symptoms. Therefore, if children did not experience significant social difficulties or if their anxiety was unrelated to their ADHD symptoms, this may help explain the null results.
Third, the measures used to assess ADHD and anxiety did not capture the full range of symptoms within these diagnostic categories, which may limit the generalizability of our findings to children with other symptoms of these disorders. In addition, the use of questionnaires and a virtual lab task may not fully capture all aspects of children’s peer functioning. Alternative methods, such as peer nominations and peer-related tasks in natural environments, could provide a more comprehensive assessment of these constructs. Finally, the homogeneity of the participant demographics limits the broader applicability of the findings. Future research should include longitudinal studies with more diverse samples of children who meet the full diagnostic criteria for ADHD, using comprehensive measures of ADHD and anxiety and objective assessments of peer functioning (e.g., peer nominations) in naturalistic settings.
Clinical Implications
Findings emphasize that the relation between ADHD and anxiety is complex and likely involves multiple factors. Clinicians working with children who have elevated ADHD symptoms should screen for, and address peer factors associated with both ADHD and anxiety (i.e., social problems, peer rejection, peer support, and anger rejection sensitivity). Early identification of these factors may help reduce the risk of anxiety in these children. Given that functional impairment moderated the relation between ADHD and anxiety, addressing impairment across various domains might be particularly beneficial. A comprehensive treatment approach should target challenges in social skills, emotion regulation, relaxation techniques, and coping strategies. Addressing these areas earlier may help children improve interpersonal skills and manage distressing social situations before peer difficulties significantly impact anxiety risk. For example, the Regulating Emotions Like An eXpert (RELAX) intervention (Breaux & Langberg, 2020) has shown promise in addressing emotion dysregulation and interpersonal challenges in youth with ADHD using cognitive-behavioral therapy techniques (e.g., thoughts, emotions, behavior triangle). Ultimately, an integrative treatment focused on multiple anxiety risk factors is likely to be the most effective until more precise intervention targets can be identified.
Supplemental Material
sj-docx-1-ebx-10.1177_10634266251363946 – Supplemental material for Peer Functioning and Anxiety Risk in Children With Elevated Attention-Deficit/Hyperactivity Disorder Symptoms
Supplemental material, sj-docx-1-ebx-10.1177_10634266251363946 for Peer Functioning and Anxiety Risk in Children With Elevated Attention-Deficit/Hyperactivity Disorder Symptoms by Helena F. Alacha and Sara J. Bufferd in Journal of Emotional and Behavioral Disorders
Footnotes
Ethical Considerations
This study was approved by the Institutional Review Board of the University of Louisville and conducted in accordance with the Declaration of Helsinki.
Author Contributions
Conceptualization: H.F.A.; Visualization: H.F.A., S.J.B.; Methodology: H.F.A., S.J.B.; Resources: H.F.A., S.J.B.; Validation: H.F.A., S.J.B.; Formal analysis: H.F.A.; Investigation: H.F.A.; Writing—original draft preparation: H.F.A.; Writing—review & editing: H.F.A., S.J.B.; Supervision: S.J.B.; Project administration: H.F.A.; Funding acquisition: S.J.B.
Funding
This research was supported by University of Louisville research funds (Bufferd).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available upon reasonable request to the first author.
Informed Consent
All participants provided informed consent (parents) and assent (youth).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.