
Abstract
The term rejection sensitive dysphoria has gained popularity recently, providing a language to discuss a phenomenon and find solace in shared experiences. Despite this, there is a lack of consensus in definition and application across medical, academic, and informal environments. This study addresses this research gap, centralising lived experiences of a small group of neurodivergent adults, alongside the shared neurodivergent standpoint of the researcher. Exploring what rejection sensitive dysphoria means to the individual and how it is experienced. By employing this novel approach, this research proposes a new conceptualisation of Rejection Sensitive Dysphoria as a phenomenon impacted by biological and environmental factors. This critical insight challenges the current essentialist positionality and associated terminology, which could positively impact policy and practice. While this research is limited in scale and therefore not statistically generalisable, the significant findings offer an important foundation for future research. Highlighting that such research, should prioritise the neurodivergent experience, within a balanced biological and environmental framework. Recognising that people, and environments, like schools, cause, trigger and sustain the experiences labelled as rejection sensitive dysphoria is a vital first step towards better support for adults now and creating more inclusive environments to improve the lives of future generations.
Lay Abstract
Over recent years the term Rejection Sensitive Dysphoria has grown in popularity, especially among the neurodivergent community. Despite this, we know very little about what Rejection Sensitive Dysphoria means to the people that are using it. We also know that the term is used differently by different people, which can cause confusion and limit our understanding further. Within this research, a neurodivergent researcher worked alongside seven other neurodivergent adults to discuss what Rejection Sensitive Dysphoria meant to them and how they experienced it in their day-to-day lives. Through the sharing of these experiences the researcher was able to identify that environmental factors, such as other people, were central to how Rejection Sensitive Dysphoria developed and was experienced. This is an important finding, as it challenges current literature that may discuss it as an unavoidable part of being neurodivergent or with language that can suggest neurodivergent emotional responses are in some way faulty, therefore unfairly placing the blame for these experiences solely on the neurodivergent individual.
This research includes the experiences of a small group of neurodivergent adults, so it is recognised that more research is needed. It is important however, that such research embraces the balanced biological and environmental viewpoint proposed based on the findings shared here. As recognising that other people, and environments, like schools, cause, trigger and sustain the experiences we label as Rejection Sensitive Dysphoria is a vital first step towards better support for adults now, and towards creating more inclusive environments that will improve the lives of future generations.
Keywords
Introduction
Much of the language we use to discuss the experiences of being neurodivergent originates from people who do not have lived experiences of the phenomenon of which they speak. However experienced, and well-meaning professionals may be, there remains significant questions over the legitimacy of knowledge that relies solely on observations and interpretations. Through the application of the standpoint theory (Harding, 1991), it is argued that neurodivergent individuals hold different social positions to neurotypicals, especially in relations to power and injustice. This results in a different perception and understanding of the world, which can only be understood through lived experience.
This study employs a novel approach to researching rejection sensitive dysphoria (RSD) by embracing these principles. The neurodivergent author worked with a small group of neurodivergent individuals, to explore their lived experiences and personal understanding of the phenomenon termed RSD. By centring lived experiences, alongside the epistemic privilege of a shared neurodivergent standpoint, this research addresses a critical gap in existing literature. Facilitating an important opportunity to consider the accuracy of current understanding and the terminology used to explain this phenomenon.
Rejection Sensitive Dysphoria (RSD)
Over recent years the term RSD has grown in popularity, especially among the neurodivergent community (Dobson, 2024). Informally it is discussed as a feature of neurodivergence, especially autism and ADHD, which presents as a predisposition to expect, sense, and react strongly to rejection. Indeed, the word ‘dysphoria’ stems from ancient Greek etymology, describing a strong feeling of pain or discomfort (Dwyer, 2022). Despite this, there remains a significant lack of formal consensus in its definition and application. In the DSM-5 (American Psychiatric Association, 2013), RSD is an atypical specifier for depression, bipolar and related disorders. In academic literature, definitions of RSD vary considerably: some describe it as an intense emotional response to perceived failure (Beaton et al., 2022), others as a heightened sensitivity to perceived rejection (Craddock, 2024), and still others as a disruption in goal-oriented attention triggered by social threat (Berenson et al., 2009). Potentially reinforcing this lack of clarity, are some different, but similar, terminologies that are often used interchangeably: ‘rejection-sensitive hysteroid dysphoria’ (Liebowitz & Klein, 1981); ‘rejection sensitivity’ (Downey & Feldman, 1996); ‘negative interpersonal sensitivity’ (Boyce & Parker, 1989); and ‘high fragile self-esteem’ (Koszegi et al., 2021). Such varied terminology and interpretations of RSD has the potential to hinder understanding of this phenomenon, not only within academic research but also for the neurodivergent individual trying to navigate their experiences within existing terminology.
Many of the terminologies associated with RSD present neurodivergence and emotionality through a deficit-based cognitive lens (McMahon et al., 2022), using language such as ‘dysregulation’, ‘dysfunction’, or ‘sensitivity’. Although evolutionary theorists propose human emotions serve as functional alertors and regulators of behaviour (Gilbert, 2015). These terms label the neurodivergent individual's alerting processes as ‘overreactions’, ‘impairments’, or ‘deficient’. In doing so, some argue that the positioning of RSD as a static entity that characterizes the individual's neurodivergence reflects an essentialist understanding of humanity, enabling the division between ‘normal’ and ‘impaired’ individuals (Hosking, 2008). While some argue the essentialist biocertification of a phenomenon like RSD can reduce blame towards individuals (Bogart et al., 2019), they also note that it can lead to assumptions that change is unattainable.
In contrast to an essentialist positionality, some have proposed that rejection sensitivity as defined by Downey and Feldman (1996), which predates associations with neurodivergence, is a cognitive-affective process (Mischel & Shoda, 1995). It proposes that human personalities are not static but are altered in response to the environment they find themselves in (Irving et al., 2013). In particular, Downey and Feldman (1996) drew upon attachment theory (Bowlby, 1985) to argue that early rejection experiences have a long-term psychological influence, resulting in a cognitive-affective processing biased towards a sensitivity to rejection. Similarly, the shift in relational emphasis, in adolescence, from caregivers to peers has been argued to result in rejection experiences from social interaction that also have a significant influence on cognitive-affective processing leading to a biased sensitivity to rejection (Shin et al., 2016; Sjåstad et al., 2021).
The defining feature of these two positionalities would appear to be whether RSD is impacted by environmental factors. Much like the divide between the medical and social model of disability. While some research has explored RSD from an essentialist positionality (Beck et al., 2024), there remains a gap in research that considers whether environmental factors impact RSD. By centralising lived experience, this research addresses the gap in existing literature seeking to explore individual interpretations of RSD and the experiences they relate to it.
Present Study
The present study is a qualitative investigation founded within the principles of the standpoint theory that lived experience is foundational to knowledge (Harding, 1991), especially when socially situated within a marginalised group. This research asserts that the standpoint of the researcher as neurodivergent, alongside the neurodivergent participants, facilitates an epistemic authority within the knowledge produced. It offers unique insights into recognising realities within social practice that non-neurodivergent researchers may miss (Bertilsdotter Rosqvist et al., 2023). By employing the standpoint theory, the study includes the emancipatory aims that the sharing of lived experiences from marginalised standpoints can produce knowledge to challenge the power dynamics between what is claimed to be true and what is really experienced (Harding, 2004).
Researcher
In alignment with standpoint theory the positionality of researcher is articulated to demonstrate its connection to the research, and the power and privileges held (Jackson et al., 2024). The neurodivergent (autism, ADHD and dyslexia), and physically disabled researcher is a late diagnosed white female, socially positioned within the neurodivergent community personally but also associated through their role as parent and their professional research.
The initial impetus for this research was the author's lived experiences, which were shared within a neurodivergent staff group. Subsequent discussions revealed commonalities in experiences, which served as the catalyst for the research. It subsequently received ethical approval from The University of Birmingham: Humanities and Social Sciences Committee.
Participants
Recruitment occurred within the same neurodivergent staff group, with inclusion based on neurodivergence and willingness to share experiences. Sample size was determined by the number of volunteers. Ten individuals initially volunteered, three subsequently withdrew, resulting in a final sample of seven who were assigned pseudonyms to maintain anonymity. An overview of participant profiles is presented in Table 1.
Participant Profiles.
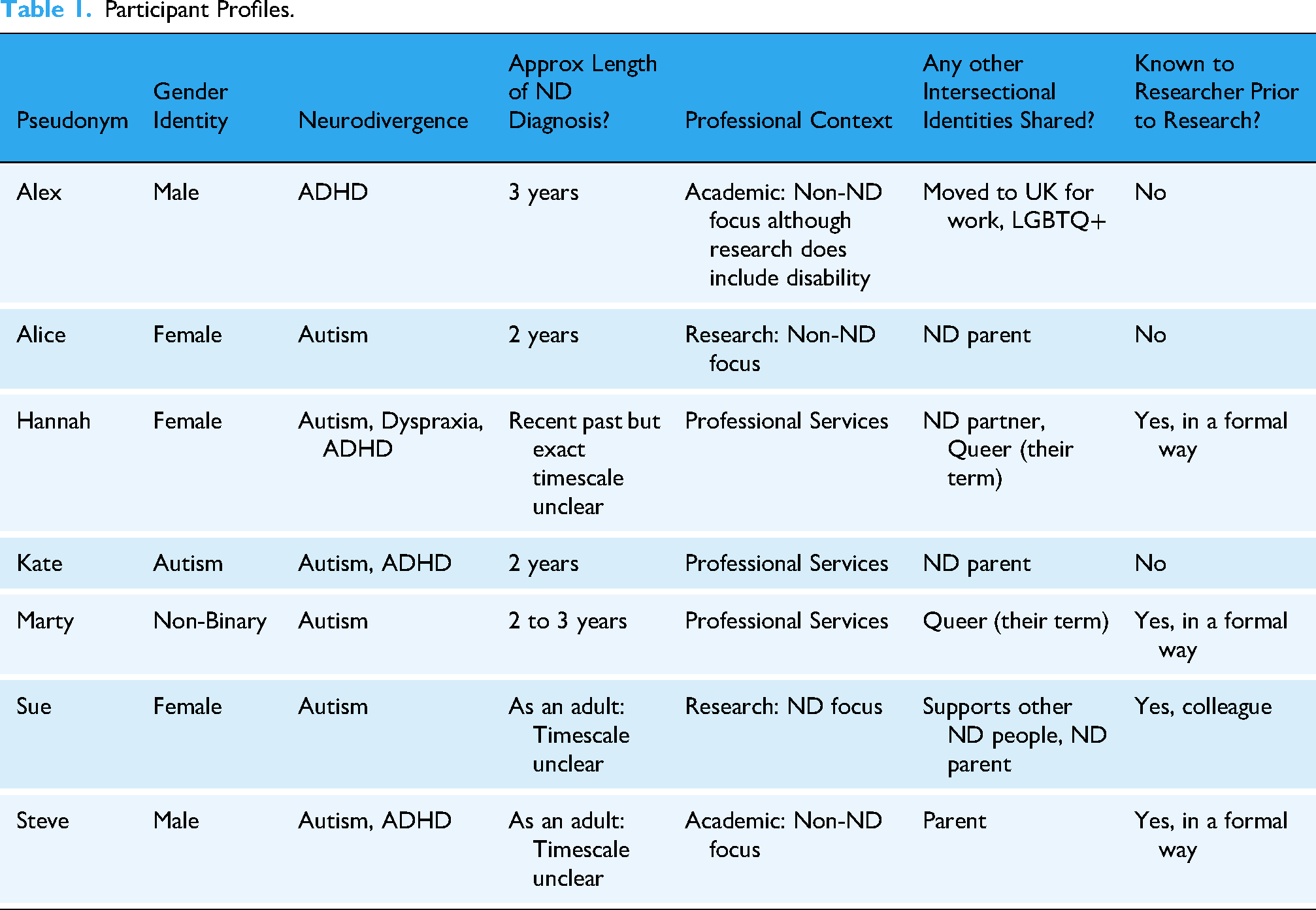
While small, this sample provided the opportunity to gather richly textured information, enabling a depth of case-oriented analysis that aligns with the research positionality (Staller, 2021). However, the limited number of collaborators may restrict the generalisability of these findings beyond the immediate context; therefore, research to explore this topic further is both warranted and welcomed.
Data Collection
Priority was given to qualitative methods to facilitate more capacity for collaborators to have autonomy over their words and thus shape the direction of the research (Barnes & Sheldon, 2007). Participation options of 1-2-1 spoken interview, group discussion, or written questionnaire were provided to all. All participants chose a 1-2-1 spoken interview which was delivered via TEAMS to aid convenience and flexibility. Interviews were 1.15 to 1.47 h, depending on the collaborator's availability and depth of responses. Post interview, all participants were provided the opportunity to email any additional comments. One participant did so which were added to the bottom of their transcript to be included in the analysis process.
Data Analysis
The interview data were approached using reflective thematic analysis (RTA) (Braun & Clarke, 2019), as it reinforces the standpoint theory positionality of the researcher being active in knowledge production. At the same time, it also prioritises rich interpretations of meaning over a simple consensus of meaning. A critical orientation approach was employed, to allow for the interrogation of patterns and themes with the theoretical understanding that language can create, not just reflect, a phenomenon (Byrne, 2022). This was particularly pertinent given the potential uncertainties surrounding RSD terminology, and the potential impact of social contexts on individual interpretation and understanding.
A flexible, yet systematic, approach was undertaken to employ the six stages of thematic analysis (Braun & Clarke, 2020), allowing a ‘back and forth’ between data sets while also providing space to reflectand re-evaluate conclusions to ensure they accurately represent the participant's experiences. Given the standpoint of the researcher as an ‘insider’, ensuring a ‘thoughtful engagement with the analytic process’ (Braun & Clarke, 2019, p. 594), became as important as the data analysis in ensuring the interpretations were accurate, unbiased, and appropriately evidenced.
The familiarisation stage began with the review of interview recordings and automatic transcripts to correct inaccuracy. During this time all non-verbal communications and displays of emotions were noted, combined with in-interview researcher observations. Once transcripts were finalised, a process of open coding was employed, using semantic codes to describe content through single words or short descriptions. Notable word choices were also coded to facilitate richer interpretation (Braun & Clarke, 2006). Once completed, a process of interpretation across transcripts occurred. The researcher's standpoint was used to review the coded data to explore which codes could be combined, or better labelled with latent coding, identifying potential hidden meanings or understanding beyond what was said, or not said. Codes were also checked to ensure they were not too wide ranging and were focused on the research questions set. For example, initial codes of: Features of RSD, RSD triggers, Impact of RSD, and Strategies were deemed too large and resulted in reassessment and fragmented into either pre-existing or new codes. Given the diverse nature of neurodivergence, some experiences, while noteworthy, were specific to the given individual and therefore had to be deemed outliers in the formation of themes. A wealth of data arrived from the interviews, so a significant amount of time was needed to reflect on the range of codes and map out how codes informed themes, and if each theme was appropriate to inform the interpretation of the dataset in relation to the research questions (Braun & Clarke, 2006). Once final themes were named and defined, this was shared with each participant for an accuracy of interpretation check to strengthen validity and reliability of conclusions. The RTA process from initial coding to final themes is outlined in Table 2.
Reflective Thematic Analysis Process.

Results and Discussion
In line with the RTA approach, results are contextualised within wider literature, moving beyond describing the data to providing theoretically informed arguments as to how the data addresses the research questions (Terry et al., 2017). Direct quotations are used throughout to demonstrate the original intellectual contribution of the participants while also providing transparency in the data analysis process.
‘What I’ve Read Impacts how I Interpret What I do’
Participants were told in advance that they would be asked what RSD meant to them, so most came prepared with an answer which was discussed as a ‘settling’ question to transition into the interview. Despite the evident research undertaken to formulate their answers, the question highlighted a variance in interpretation. Which has significant implications when terminology is use based upon assumptions of shared understanding.
Reflecting the previously noted prominence of RSD within the neurodivergent community, all participants reported becoming aware of RSD through engagement with other neurodivergent people. Provoking an ‘oh my gosh, that's my experience’ (Sue). Having a shared language to discuss and validate experiences was positioned by all as significant, illustrated succinctly in the repetition of word choices by Kate ‘really really really positive’. Similarly, when reflecting on her engagement in the research, Hannah shared If RSD as a term were to gain more traction and understanding, that this is something we experience, to validate it. Because how can what we are feeling not be real and not be true? How can you tell us that this is not a valid thing?
Start of Interview Definition of RSD.

These findings advance our understanding by showing that a shared language for RSD experiences is fundamental in validation, and self-acceptance, while the absence of a shared understanding of such language risks excluding experiences and inadvertently hindering individual wellbeing.
An Intense Visceral Emotional and Physical Reaction
The emotional and physical responses to triggers was one area where all participants agreed with their initial definitions of RSD. Fear, shame, upset, anxiety, overwhelm, and anger were common terms used to categorise feeling like an ‘emotional wreck’ (Alex) or ‘maladjusted in the moment’ (Steve). Physical sensations were reported less frequently, and when present, they typically co-occurred with the emotional response. Examples given included: ‘I have a pressure here [head]’ (Kate), pain, tension, ‘tight chest’ (Alice), feeling unwell, exhaustion and nausea. The word ‘pain’ was used frequently by participants to refer to both physical and emotional experiences, with two people also choosing the adjective ‘visceral’. These purposeful language choices suggest that responses were intense and instinctual. ‘it makes me physically react… an intense feeling of wanting to burst into tears or wanting to rant and rage’ (Steve). Mirroring Steve's experiences, all participants reflected on a lack of control over their responses, which was often viewed as more problematic than the event that triggered it. Participants expressed shame towards their uncontrolled responses which had significant long-term consequences. For example, Marty's relationships were impacted because they did ‘not trust my emotions’ (Marty). However, Alice, when recounting her emotional response to an event that occurred 15 years ago, began to cry, because she still felt ‘embarrassed about my reaction at the time’ (Alice). Both accounts highlight the complexity of RSD, showing that immediate strong emotional reactions represent only one aspect of a phenomenon which actually has a much more long-term influence. This sustained impact beyond the initial trigger was commonly discussed using the words ‘shame’ and ‘spiral’, for example: ‘spiral of shame’ (Kate), ‘it's like the world is spiralling inwards’ (Hannah), ‘shame doom: the feeling of imminent doom, that shame is coming’ (Sue). It was queried whether spiral may be indicative of an escalating impact; however, Alice clarified this was inaccurate. Rather than one issue becoming more problematic it was actually more of a joining of one problem to another, it ‘feels like a lot of bad feelings that are not even connected to the initial trigger at all’ (Alice). This explanation holds similarities to the notion of triggers within psychology, where the initial event is linked to past experiences and impacts the response (Bonior, 2019). A factor that will be explored further within the theme of ‘scar tissue’. It is also significant to note the association between the common use of ‘shame’ and the proposed role of judgement as a central facet to RSD. If viewed from a psychological perspective, shame is interpreted as a judgement of oneself, that is often related to the individual's perception of external judgement. This definition would appear to relate to the significant number of transcript extracts that were coded as ‘inner voice feeding the RSD’. Participants shared that the role of negative self-talk was judgement and blame, Kate shared the example of her inner-voice saying: ‘You’re an absolute idiot. Look what you did earlier’, which was indicative of a response to a trigger that was routed in memories of past negative experiences (Zaccari et al., 2024). Steve described his inner voice at work asking ‘What is wrong with me? Why can I not get this right?’ explaining how he felt this related more to past experiences of struggle at school due to his undiagnosed ND. The role of past negative experiences and living as a neurodivergent person in a neurotypical world, are two key factors that weave their way through all the themes.
All participants felt the physical and emotional aspects of RSD were intense and ‘disabling’ (Alex), impacting internal experiences as well as their ability to manage employment and socialisation. Importantly, beyond immediate responses, emotions translated into shame and anxiety which had long term consequences, impacting future responses (Feinstein, 2020). These findings advance understanding of the prevailing impact of RSD, providing knowledge that can inform policies and practices to better support neurodivergent individuals.
‘Yuckiness That is Learnt From Being Rejected by People’
All participants began their exploration of RSD with the belief that it directly related to being ND, indeed for one participant it was RSD that had led them to pursue a diagnosis. Participants reflected that their neurodivergence caused ‘big emotions’ which was likely to significantly impact their RSD. This is a commonly reported neurodivergent trait (Conner et al., 2020; Todzia-Kornaś et al., 2024) and may impact on a fear of rejection and an overinterpretation of others’ intentions (Kelly et al., 2023). However, the line between these emotions and when it was deemed RSD was unclear. For example, Steve initially described a RSD experience as an ‘emotional response packed into a very intense, very short burst, a really sort of spiky response’ which may be suggestive of what is often termed a ‘melt down’. Through discussion Steve further articulated that he felt a secondary component to RSD was ‘a real struggle to let go of things’ suggesting the emotions became RSD if they were prolonged because of his self-judgements which were a product of past external judgements. In fact, despite his initial definition (table 3), Steve went on to say, ‘judgement is the core of rejection sensitivity’, which is another example of how initial definitions and shared experiences often did not align.
In contrast to the assumed link between RSD and ND, it is significant that all participants’ reported RSD has a social prerequisite. Evidenced by experience of RSD linked to social interaction, but also by a lack of RSD without a social element. Both Kate and Sue reflected on the difference between computer and human delivered criticisms at work. Feeing that while both may provoke an initial negative response, only the human interaction would provoke RSD because the social interaction would trigger intrusive memories and provoke a spiral of emotions. Correlating with research that suggests interpersonal trauma can severely affect trust and social functioning, impeding the development and maintenance of interpersonal relationships (Nickerson et al., 2014). Steve also provided examples of when he had experienced RSD in an environment where he thought other people could see him ‘really super, super frustrated, really angry at myself, because I think people might be watching and judging me’ but also provided comparable experiences where he knew no-one could see him and feeling ‘frustrated in that neurodivergent spiky way, but then back to normal because I know nobody's judging me’. It is interesting to note that in Steve's first experiences the use of the words ‘think’ and ‘might’ are indicative of perceived judgement only, which is an important aspect to be returned to.
Participant's experiences also revealed how different types of social situations can impact RSD. The language ‘open loop’ was used by a couple of participants to describe rejection by another person who subsequently refused to engage in resolution activities, resulting in a feeling of being ‘stuck in a loop that I can’t get out of’ (Hannah). In such situations RSD experiences were worse and sustained for significant periods of time. Alex described it as ‘an open wound that I can’t heal’ with the words ‘wound’ and ‘heal’ meaningful symbolisations of how he was evidently stuck within the pain of a social interaction that had occurred two years prior, becoming so problematic he was advised to seek help from a ‘psychologist specifically about this issue’ (Alex).
In direct contrast, participants also spoke of experiences where other people had reduced their RSD. For example, Kate shared with her line manager that her RSD is provoked by her asking for a quick meeting ‘I’ve told her that in that instant it's like ****, this is it. I’m getting sacked now’. As a result, the line manager approaches meetings differently and the RSD is reduced. RSD was also reported as less pronounced in neurodivergent groups, with participants contrasting these supportive contexts with the challenges they encountered in neurotypical settings. Experiences indicated that neurodivergent groups ‘normalised’ what had previously been defined as weird, “there's a positive spin on it. It's like that's weird… Keep doing it” (Marty) and because everyone is ‘weird’ it felt safe to embrace their authentic selves, which they termed ‘neuropositivity’. Hannah builds on the impact of such groups by powerfully stating ‘I think not feeling alone is enormous’ indicating there is an isolation in having experiences such as RSD, because if it is not discussed you may feel as if you are the only one experiencing it. Sue reflected on the different communication experienced within neurodivergent groups. She felt the ‘direct and honest’ style of communication she associated with her autism, helped to reduce RSD when others also used the same communication style. This style of communication, often categorised as ‘impaired’ by the NeuroMajority, nurtured a trust that there was no hidden meaning in the interaction while also ‘normalising’ the seeking of clarification where needed. Hannah, Alice and Kate also referred to this communication style, with Hannah reinforcing its importance by sharing that ‘direct communication has to be baked into my relationship, or it won’t work’. For all, this was because the ‘normal’ indirect communication style of neurotypicals perpetuated RSD as it left room to fear a hidden message behind what was being said, which triggered past negative experiences of someone saying one thing but then acting in a contrary manner.
As previously noted, awareness of RSD for the participants, originated from the neurodivergent community. It is unsurprising therefore that they would understand one in relation to the other. However, like the mismatch between initial definitions and subsequent discussions, the findings reveal a mismatch between this assumption and the lived experiences discussed. While some neurodivergent features were identified as impacting their emotional responses to triggers, the data analysis indicates that RSD responses were inconsistent, suggesting a fundamental environmental proponent. The identification of environmental factors within RSD challenges the assumption that these experiences are inherently inevitable for neurodivergent individuals, offering a new perspective that informs both scholarly debate and practical approaches.
‘It's Kind of Like Scar Tissue’
When reflecting on whether RSD was part of being neurodivergence, Hannah replied ‘it feels like it's one of the core, it shouldn’t be, but it feels like it's one of the core experiences of being a neurodivergent human in this world’. While this was said to validate the existence of RSD, the incorporation of ‘in this world’ is significant, as it implies that in a different world, things would be different. Which is reflective of the biggest group of themes across the interviews: RSD and being neurodivergent in a neurotypical world.
Being diagnosed late, was an important factor to the experiences all participants shared (Attoe & Climie, 2023), as this led to growing up with an awareness of being different but without an understanding as to why. ‘I was cast as weird, never supported to know anything about what that weird was’ (Hannah). All acknowledged past interpersonal trauma, such as bullying, marginalisation and judgement by others, mirroring research that consistently evidences neurodivergent individuals are bullied more than their neurotypical peers (Brake, 2025; Masland et al., 2019). While some chose not to discuss this, others were able to give examples that aided in the recognition of this as an importance theme. Alice spoke of peers at school ‘pretending to be friendly for a while and then turning around and making fun of me’, which could link to the assumptions of rejections hidden behind what people say, as previously discussed. Marty also discussed ‘Experiences of exclusion and rejection from peer groups growing up because I found it incredibly hard to relate to their way of being in the world’. They went on to explain that such challenges existed at primary school but were left unsupported. Resulting in future isolation, as they felt they had missed the opportunities to learn how to build social connections. To substitute for this, they sought validation from people in authority, such as teachers, an approach that Sue also reflected that she used and her son uses. However, even relationships with ‘trusted’ people retrospectively emerged as a form of hidden interpersonal trauma. Marty self-discovery had allowed them to realise they weren’t to blame for the negative experiences with their peers, while also highlighting mistreatment by authority figures they trusted: the same teachers that I was looking up to and using as my point of validation and sense of belonging, where the exact same people who were also letting me down on multiple levels. (Marty) I was bullied horrendously by teachers. One of my teachers used to spend her days making pompoms to throw at me, and I know that might not sound like a lot, but who literally spends their day creating things to throw at one particular child. I cannot defend myself from that. (Hannah)
It is hoped that such alarming experiences would not be allowed to happen today, that the participant's experiences are more reflective of an 1980s ‘education system that was structured to not allow anything outside the norm to exist’ (Hannah). However, this would still indicate a population of adults that may need support now for RSD linked to trauma of being children in the 80 s. Furthermore. the participants who were also parents highlighted that there is evidence of a lack of understanding that continues to impact neurodivergent children at school. Such as Sue's observation that her child was ‘desperately people pleasing with teachers that don’t get him’. These findings advance understanding of the relationship between RSD and attachment (Bowlby, 1985), demonstrating how such early experiences shape one's sense of trust, safety and self. These critical findings extend the ongoing debate regarding inclusive practice in our education system by highlighting the long-term impact negative experiences can have on the individual.
The metaphor of ‘scar tissue’ used by Steve, captures how ongoing experiences of interpersonal trauma and feeling ‘different’ without understanding accumulates over time, producing profound emotional effects for the individual; ‘I imagine it as something akin to complex PTSD…. Doesn’t arise out of one traumatic incident, but a series of incidents’ (Marty). All participants either specifically referenced ‘trauma’ as the reason for their current experiences, or provided examples that validated prolonged interpersonal trauma led to the ‘learned response’ (Sue) evident in RSD (Ginapp et al., 2023; Knauft, 2022). Two themes that reflect this impact was ‘perceived rejection’ and the intrusive memories linked to ‘trauma’ (Iyadurai et al., 2019). All but one participant discussed that perceived or anticipated rejection sensitivity was more common than actual rejection, ‘perceived rejection, not even real rejection, but just in my head somebody doesn't like me and then it just spirals from there’ (Alice). Reflecting how a social interaction triggers memories of past trauma and provoke their RSD, ‘a kind of emotional echo or ghost’ (Steve) mirroring the ‘spiral’ as previously discussed. Furthermore, that this spiral negates the need for evidence of current rejection as it uses the ‘mental catalogue’ (Hannah) of past rejection to provoke emotional distress ‘I must have done something terrible, there's no evidence I did, but I feel I did’ (Sue). This process was sustained over time because participants felt they did not deal with the triggers or past trauma, but merely ‘boxed it up and put it aside’ (Alice) as a coping strategy. This reinforces the concept of RSD relating to scar tissue that builds over time through ‘continued negative reinforcement, systematic abuse of power, and[or] ongoing intimidation and emotional pain’ (PTSDUK, 2024) which results in feelings such as powerlessness and fear (Stone et al., 2024). Providing important evidence for the need for systems of support for neurodivergent individuals with these experiences.
‘What I Feel is Being Rejected is me, as a Person’
Within interviews the participant experiences largely focused on judgement and criticism, which led the interviewer to ask, ‘what does the rejection in RSD mean?’. Participants shared that rejection was indistinguishable from judgement because underneath it all was the fear of being negatively judged for being neurodivergent ‘I suppose what I feel is being rejected is me, as a person. Being insufficient and inadequate’ (Sue). As previously noted, this fear was driven by past negative experiences of interpersonal trauma and ‘living in a world that's not set up for us’
Like other themes, knowledge came not only from analysing direct answers, but also from within examples of where RSD had not occurred or factors that reduced RSD. Most notably were the ways understanding and acceptance both from within themselves and from others could change RSD experiences. All participants had undergone a period of self-discovery which they deemed fundamental to unravelling the long-term implications of being neurodivergent in a neurotypical world. For some being diagnosed had a significant impact ‘One of the biggest things my diagnosis gave me was self-compassion, it has allowed me to just go, this is who I am’ (Hannah) mirroring the feedback seen in similar research (Huang et al., 2020). For others, life experiences such as parenthood or meeting other neurodivergent people had been central to their self-awareness (Øverland et al., 2024). Self-understanding and acceptance empowered individuals to be kinder to themselves, metaphorically providing permission to feel strong emotions and in turn reduce the ‘shame spiral’ (Cai & Brown, 2021). Offering an interesting correlation to the work of Shahar (2015), who suggests self-criticism originates not only from the judgement of others but from a lack of self-knowledge and authenticity.
The newly identified environmental aspect of RSD is used as further evidence for ‘rejection’ being linked to a judgement of neurodivergence. Participants discussed how environments could either increase the fear of judgement and result in self-silencing as a safety mechanism (Harper et al., 2006; Jack, 1991) ‘a fear that they wouldn’t respect me if I didn’t mask’ (Marty) or could be ‘nurturing [of] authenticity’ (Hannah) which reduced a fear of judgement. As previously noted, participants found neurodivergent groups embraced ‘NeuroPositivity’ which reduced experiences of RSD (French & Cassidy, 2024). However, examples were also given of neurodiverse spaces that were also able to reduce RSD because they evidenced a celebration of individual and cultural diversity, such as Hannah's description of her current team: ‘I think this is the first place, I have felt safe to be even a fraction of myself’. The use of the word safe here is illustrative of the fear normally associated with sharing one's neurodivergence with others. A culture of acceptance and inclusion was believed to reduce experiences of RSD, providing crucial support to the argument that experiences of threat are different when an individual feels connected and supported (Cacioppo & Patrick, 2008; Gilbert, 2015).
Conclusion
This research sought to advance understanding of RSD by using the shared standpoint of researcher and participants to interpret lived experiences. By employing this novel approach this research provides critical insights that can inform policy and practice, while also highlighting the need for future research.
Participant experiences highlighted that experiences categorised as RSD were complex, ‘visceral’, and pervasive, involving both emotional and physical distress. Intense responses to perceived or anticipated rejection were frequently experienced (Nakazawa et al., 2021) and resulted in behavioural changes (Romero-Canyas et al., 2010) such as self-silencing or avoidance. RSD was thought to be associated with being neurodivergent but was also seen as a learnt response to the experiences of being neurodivergent in a neurotypical typical world, such as marginalisation, and judgement. The impact of experiencing RSD was significant in all areas of the individual's lives, however no support mechanisms were available to them to understand their experiences or manage them. Resulting in a ‘spiral’ of impact that often-lasted decades.
This research provides critical insights into inconsistencies within terminologies associated with RSD which impedes our understanding. Demonstrating the need for more research to unpick these confusions, focusing on lived experiences, as they constitute critical foundations in the development of understanding, acceptance and support. The current use of RSD, across the neurodivergent community, reflects an essentialist model (Hosking, 2008) because of its deficit-based assumptions of being ‘too sensitive’. This study provides original evidence that RSD does not always occur, indicating a fundamental environmental proponent to this phenomenon which would counter such essentialist positionality. This research has demonstrated how fear of judgement from others is a learnt, pervasive state, that has a substantial impact on the way the neurodivergent person thinks, feels and behaves, causing a ‘significant impairment in personal, family, social, educational, [and] occupational functioning’ (World Health Organisation, 2019). Potentially therefore, reflecting the original construct of rejection sensitivity being a cognitive-affect process (Downey & Feldman, 1996). Evidence from this study, however, also reinforces that emotionality may be different in neurodivergent people when compared to their neurotypical counterparts, which also impacts RSD experiences. By viewing these factors together, this research proposes employing a biopsychosocial model as a new approach for RSD research, integrating essentialist and cognitive-affective perspectives to generate a more comprehensive and theoretical understanding.
Viewing RSD through this balanced approach elicits important questions relating to the terminology used to discuss this phenomenon which would impact both policy and practice. All participants recognised the importance of having shared language to understand their own experiences, and to find solace in the understanding that others have similar experiences. However, concerns are raised over the potential problematic nature of the language of RSD that not only reflects a deficit-based framework but may also not accurately represent lived RSD experiences. Judgement from others was discussed more frequently than ‘Rejection’, however ‘rejection’ may be appropriate if it was conceptualised as a form of interpersonal judgement. ‘Sensitivity’ was deemed to imply a deficit; however, to be accurate it needs to be conceptualised as a learnt response to interpersonal trauma. ‘Dysphoria’ was problematic for some, due to its use in gender dysphoria which did not match the experiences they were discussing. These findings can contribute to future research that considers the language we use to discuss this phenomenon. A critical topic as language powerfully frames understandings of neurodivergence, shaping ableist interpretations and carrying far-reaching implications for social attitudes, therapeutic practices and disability policy (Bottema-Beutel et al., 2021).
While the sample is limited in scale, the findings of this research offer important implications for understanding and provides a foundation for future research on a broader population using the new framework these findings proposed. These insights can guide policy and practice to support those with RSD and transform environments like schools to prevent similar challenges for future generations.
Footnotes
Acknowledgements
I would like to thank the collaborators for sharing their experiences and for helping me to develop and complete this study. Without them, none of this would be possible. I would also like to thank my neurodivergent colleague, and family, for supporting me in managing the fear of anticipated journal rejection, without whom this article would never have been submitted!
Ethical Approval
Ethical approval for this research was granted by The University of Birmingham: Humanities and Social Sciences Committee. ERN_1886-Mar2024. Written informed consent was provided by all collaborators to participate in the study and for the author to publish the findings in a format that would maintain they anonymity.
Authors’ Contributions
Barbara Sandland contributed to conceptualization, methodology, validation, formal analysis, investigation, data curation, writing–original draft, writing–review and editing, visualization, and project administration. Participants contributed to conceptualization, methodology, validation, and writing–review and editing.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data that support the findings of this study are available on request from the corresponding author (Barbara Sandland). The data is not publicly available due to restrictions e.g., they contain information that could compromise the privacy of research collaborators.