
Abstract
Keywords
Introduction
Anticoagulants are the foundation of therapy for venous thromboembolism (VTE). The emergence of direct oral anticoagulants (DOACs) for the management of thromboembolic disorders worldwide represents a major paradigm shift from oral vitamin K antagonists (VKAs), such as warfarin. Dose-response during VKA treatment varies considerably because of delayed onset, need for parenteral anticoagulation overlap, narrow therapeutic window, interactions with dietary vitamin K and numerous drugs, and genetic variations in VKA pharmacokinetics.1-4 Given these limitations with the VKAs, the DOACs are considered to be a more convenient and potentially safer option for VTE treatment. In this article, we review the current evidence for the new-generation DOACs: rivaroxaban, dabigatran, apixaban, and edoxaban for the acute treatment and secondary prevention of VTE as compared with warfarin and offer the clinician practical considerations when using each agent.
Data Sources and Selection
The data included in this review were identified by searches of PubMed and Google Scholar (publications from 1966 to December 2015) for VTE, deep vein thrombosis (DVT), pulmonary embolism (PE), drug international nonproprietary names, and related search terms. Additional online searches were conducted for prescribing/label information. ClinicalTrials.gov was used to identify relevant clinical trials.
DOACs in the Treatment of Acute VTE
Within the past 5 years, 4 DOACs have been approved in the United States for the treatment and secondary prevention of VTE: the direct thrombin inhibitor dabigatran and direct factor Xa inhibitors rivaroxaban, apixaban, and edoxaban (indications and dosing in Table 1).5-10 The principal advantages of these agents over warfarin are a rapid onset of action, reaching maximal anticoagulant activity within 1 to 4 hours11-13; predictable and stable pharmacokinetics and pharmacodynamics with exposure-proportional increases in anticoagulant response; and the lack of need to routinely dose monitor (Table 2).5-37
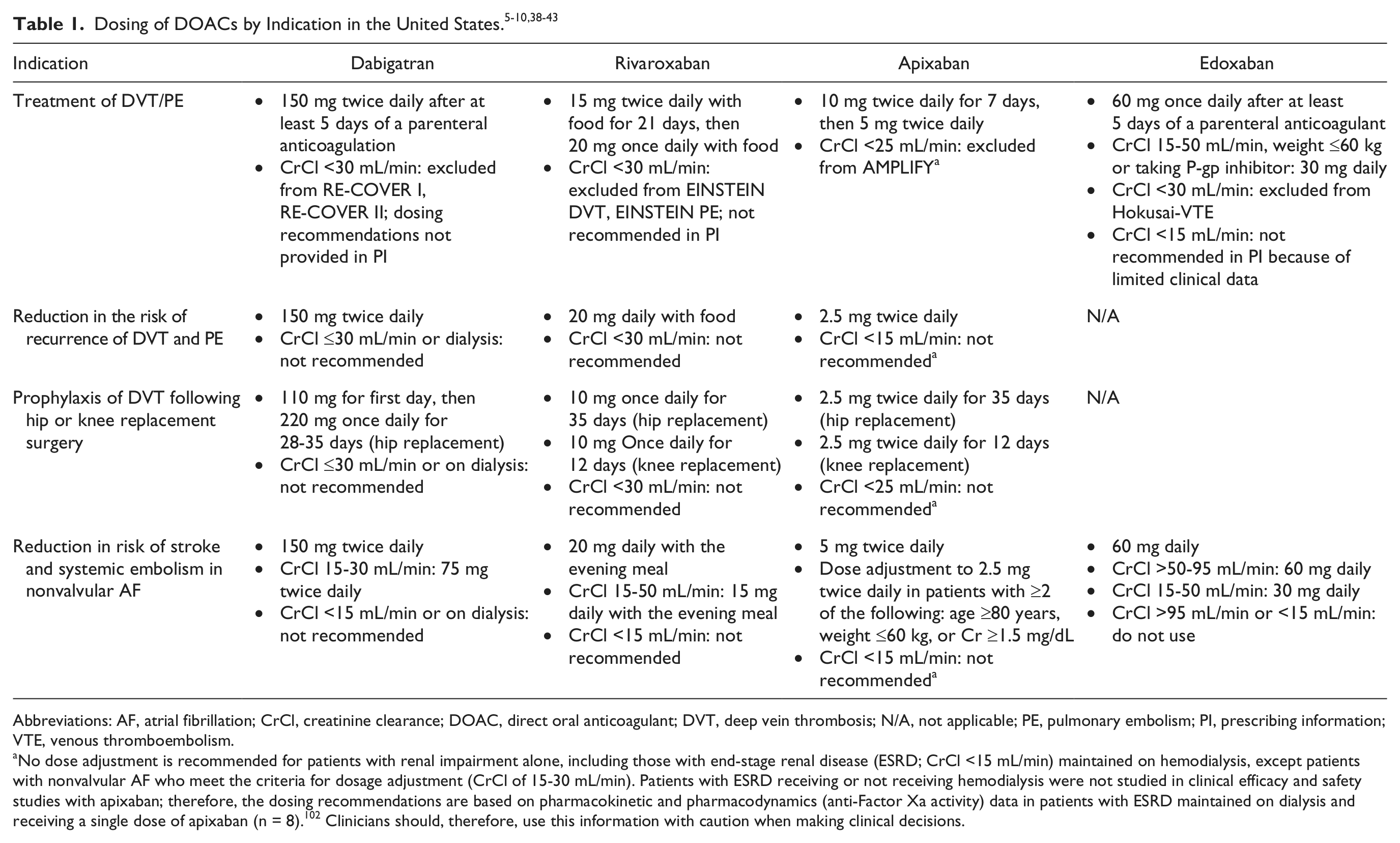
Abbreviations: AF, atrial fibrillation; CrCl, creatinine clearance; DOAC, direct oral anticoagulant; DVT, deep vein thrombosis; N/A, not applicable; PE, pulmonary embolism; PI, prescribing information; VTE, venous thromboembolism.
No dose adjustment is recommended for patients with renal impairment alone, including those with end-stage renal disease (ESRD; CrCl <15 mL/min) maintained on hemodialysis, except patients with nonvalvular AF who meet the criteria for dosage adjustment (CrCl of 15-30 mL/min). Patients with ESRD receiving or not receiving hemodialysis were not studied in clinical efficacy and safety studies with apixaban; therefore, the dosing recommendations are based on pharmacokinetic and pharmacodynamics (anti-Factor Xa activity) data in patients with ESRD maintained on dialysis and receiving a single dose of apixaban (n = 8). 102 Clinicians should, therefore, use this information with caution when making clinical decisions.
Key Pharmacological Parameters of Dabigatran, Rivaroxaban, Apixaban, and Edoxaban.
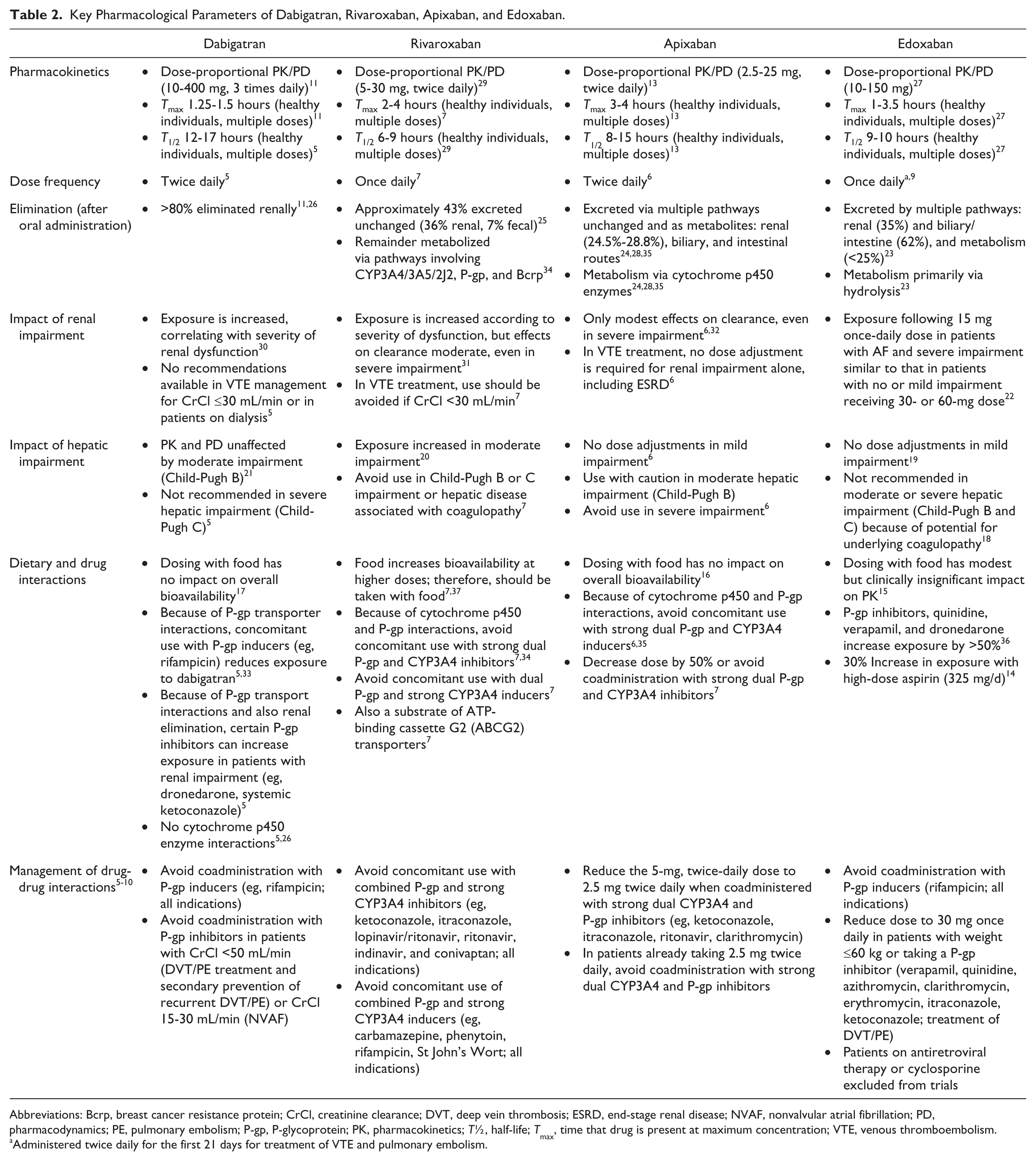
Abbreviations: Bcrp, breast cancer resistance protein; CrCl, creatinine clearance; DVT, deep vein thrombosis; ESRD, end-stage renal disease; NVAF, nonvalvular atrial fibrillation; PD, pharmacodynamics; PE, pulmonary embolism; P-gp, P-glycoprotein; PK, pharmacokinetics; T½, half-life; Tmax, time that drug is present at maximum concentration; VTE, venous thromboembolism.
Administered twice daily for the first 21 days for treatment of VTE and pulmonary embolism.
When selecting an appropriate agent, a clinician must take into account the safety and efficacy profile of individual DOACs as they compare with warfarin. Although no head-to-head comparative trials exist for DOACs in VTE, the DOAC trials have involved similar patient populations and demonstrated similar efficacy and safety results compared with conventional therapy (Table 3).38-43 The mean time in therapeutic range (TTR) for patients receiving VKA in the comparative trials was approximately 60% (57% to 64%), which is comparable with the TTR in other trials and better than what is achieved in clinical practice.44,45 The phase 3 trials supporting approval for these agents used similar primary efficacy end points but differed with respect to the use of parenteral anticoagulation, which was required in the dabigatran and edoxaban trials in both the conventional treatment and DOAC arms. Trials with rivaroxaban and apixaban allowed the DOAC to be started without initial parenteral anticoagulant therapy but required a subsequent dose adjustment 1 to 3 weeks into therapy. Similar exclusion criteria shared by all the trials included any active bleeding, high risk for bleed, or prior oral anticoagulation (beyond 1-2 doses) and limited parenteral anticoagulation prior to randomization. Patients with severe renal dysfunction were excluded from all studies.
Comparison of Venous Thromboembolism Treatment Trials.
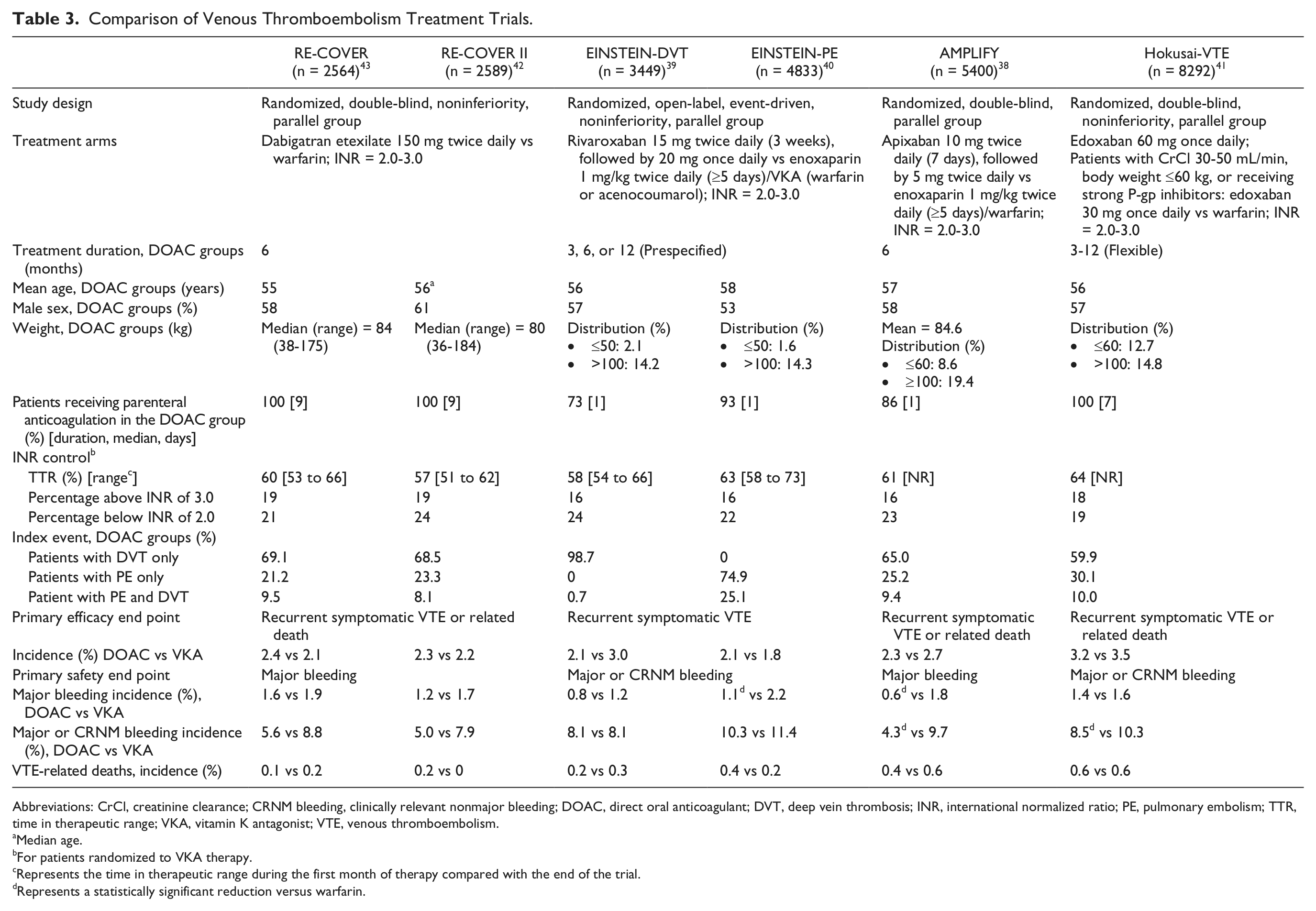
Abbreviations: CrCl, creatinine clearance; CRNM bleeding, clinically relevant nonmajor bleeding; DOAC, direct oral anticoagulant; DVT, deep vein thrombosis; INR, international normalized ratio; PE, pulmonary embolism; TTR, time in therapeutic range; VKA, vitamin K antagonist; VTE, venous thromboembolism.
Median age.
For patients randomized to VKA therapy.
Represents the time in therapeutic range during the first month of therapy compared with the end of the trial.
Represents a statistically significant reduction versus warfarin.
Dabigatran
Dabigatran for the treatment of VTE was evaluated in the RE-COVER (n = 2564) and RE-COVER II (n = 2589) trials, both of which had similar designs. Patients with objectively confirmed acute VTE were randomized to receive dabigatran 150 mg twice daily or warfarin (international normalized ratio [INR] = 2.0-3.0) for 6 months (average treatment duration = 164 days). All patients initially received parenteral anticoagulation for a median of 9 days. In both trials, dabigatran was noninferior to warfarin for the primary efficacy end point (recurrent symptomatic, objectively confirmed VTE and related deaths; RE-COVER: hazard ratio [HR] = 1.10; 95% confidence interval [CI] = 0.65-1.84; RE-COVER II: HR = 1.08; 95% CI = 0.64-1.8; P < 0.001 for both trials).42,43 Major bleeding was not significantly different between groups in either trial. However, there were significant (37% and 38%) relative reductions in the rate of major and clinically relevant nonmajor (CRNM) bleeding in RE-COVER (HR = 0.63; 95% CI = 0.47-0.84) and RE-COVER II (HR = 0.62; 95% CI = 0.45-0.84) trials. In terms of adverse events, dyspepsia was more prevalent in the patients receiving dabigatran than in those receiving warfarin in RE-COVER (2.9% vs 0.6%; P < 0.001) but not in the RE-COVER II trial (1.0% vs 0.2%; P value not provided).
A pooled analysis of the RE-COVER trials found that dabigatran maintained its noninferiority compared with warfarin (2.4% vs 2.2%; HR = 1.09; 95% CI = 0.76-1.57; P < 0.001). 42 As in the individual trials, major bleeding was not different between the groups (1.4% vs 2.0%; HR = 0.73; 95% CI = 0.48-1.11), but there was a significant reduction in major and CRNM bleeding with dabigatran compared with warfarin (5.3% vs 8.5%; HR = 0.62; 95% CI = 0.50-0.76). There was also a significant 30% relative reduction in any bleeding with dabigatran (HR = 0.70; 95% CI = 0.61-0.79). Interestingly, when excluding events occurring during parenteral therapy, there was a significant 40% relative reduction in the rate of major bleeding (HR = 0.60; 95% CI = 0.36-0.99) during oral anticoagulant therapy. In this analysis, significantly less major and CRNM bleeding were seen (HR = 0.56), as was any bleeding event (HR = 0.67), with dabigatran compared with warfarin.42,43
Rivaroxaban
Rivaroxaban was the first oral factor Xa inhibitor available for the management of VTE 7 and the only DOAC to be evaluated in separate DVT (EINSTEIN-DVT) and PE (EINSTEIN-PE) trials.39,40 In the EINSTEIN-DVT trial, 3449 patients presenting with DVT without PE were randomized in an open-label fashion to rivaroxaban 15 mg twice daily for 21 days followed by 20 mg once daily or conventional therapy with enoxaparin 1 mg/kg administered subcutaneously every 12 hours and a VKA (INR = 2.0-3.0). The treatment duration could have been 3, 6, or 12 months and was left to the discretion of the investigator but was defined at the time of enrollment; 3 months (12% of patients in both treatment groups), 6 months (63%), and 12 months (25%). The study design and outcomes of the EINSTEIN-PE trial were identical; however, the 4833 patients had to present with symptomatic PE with or without DVT. The intended durations of study treatment in both arms were 3 months (5%), 6 months (57%), and 12 months (37%). Patients randomized to conventional therapy received enoxaparin for a median of 8 days in both trials.
In the EINSTEIN-DVT trial, the occurrence of symptomatic, objectively confirmed recurrent VTE (primary efficacy end point) was found to be noninferior between rivaroxaban and conventional therapy (HR = 0.68; 95% CI = 0.44-1.04; P < 0.001). 39 Patients receiving rivaroxaban demonstrated a numerical decrease in major bleeding and a numerical increase in CRNM bleeding, providing an 8.1% rate of major and CRNM bleeding (primary safety outcome) for both groups (Table 3). The combination of the primary efficacy end point and major bleeding, defined as net clinical benefit, was significantly improved with rivaroxaban compared with conventional therapy (2.9% vs 4.2%; P = 0.03).
In the EINSTEIN-PE trial, the primary efficacy end point was also found to be noninferior between rivaroxaban and conventional therapy (HR = 1.12; 95% CI = 0.75-1.68; P = 0.003). 40 Major bleeding was significantly reduced by 50% with rivaroxaban compared with conventional therapy (HR = 0.49; 95% CI = 0.31-0.79; P = 0.003). The occurrences of CRNM bleeding and the combination of major and CRNM bleeding were not different between the groups (Table 3). Net clinical benefit was not different between those receiving rivaroxaban or warfarin, respectively (3.4% vs 4.0%; P = 0.28).
In a pooled analysis of the EINSTEIN trials, the primary efficacy outcome maintained its noninferiority for rivaroxaban compared with conventional therapy in 8282 VTE patients (2.1% vs 2.3%; HR = 0.89; 95% CI = 0.66-1.19; P < 0.001). Rivaroxaban was associated with a significant 46% relative reduction in major bleeding versus conventional therapy (1.0% vs 1.7%; P = 0.002). This reduction in major bleeding was largely responsible for the significant reduction in net clinical benefit with rivaroxaban compared with conventional therapy (HR = 0.77; 95% CI = 0.61-0.97). No difference in the primary safety outcome of major and CRNM bleeding was observed between the groups (9.4% vs 10.0%; P = 0.27). 46
Apixaban
In the AMPLIFY trial, more than 5000 patients with objectively confirmed VTE were randomized in a double-blinded fashion to apixaban 10 mg twice daily for 7 days, followed by 5 mg twice daily or conventional therapy with enoxaparin 1 mg/kg administered subcutaneously every 12 hours started with warfarin. 38 Enoxaparin was discontinued after a minimum of 5 days and achieving an INR of 2 or more. Treatment was continued for 6 months in both groups. The primary efficacy end point of recurrent symptomatic VTE or death related to VTE at 6 months was found to be noninferior between apixaban and conventional therapy (relative risk [RR] = 0.84; 95% CI = 0.60-1.18; P < 0.001). 38 Patients presenting with PE demonstrated a similar reduction (RR = 0.90) compared with patients presenting with DVT (RR = 0.83; P value for interaction = 0.8198). Major bleeding was reduced by almost 70% in patients receiving apixaban compared with conventional therapy (RR = 0.31; 95% CI = 0.17-0.55; P < 0.001). There was also a significant reduction in major and CRNM bleeding with apixaban versus conventional therapy in these VTE patients (RR = 0.44; 95% CI = 0.36-0.55).
Edoxaban
In the Hokusai-VTE trial, patients (n = 8292) with VTE were randomized in a double-blinded fashion to edoxaban 60 mg once daily or warfarin titrated to an INR of 2.0 to 3.0. 41 A reduced edoxaban dose of 30 mg daily was given to patients (17.8%) with a creatinine clearance (CrCl) of 30 to 50 mL/min, with a body weight of ≤60 kg, or receiving a potent P-glycoprotein (P-gp) inhibitor (quinidine, dronedarone, or verapamil). Patients in both groups received parenteral treatment for a median of 7 days. Treatment duration could have been between 3 and 12 months; 40% of patients received treatment for 12 months (mean treatment duration: 8.3 months).
The primary efficacy outcome (symptomatic recurrent VTE at 12 months, regardless of treatment duration) met the predefined definition of noninferiority (P < 0.001) for edoxaban compared with warfarin. 41 Most of the difference between these groups can be attributed to the 40% of patients presenting with PE (2.8% vs 3.9%; HR = 0.73; 95% CI = 0.50-1.06), whereas patients presenting with DVT demonstrated almost identical results between groups (3.4% vs 3.3%; HR = 1.02; 95% CI = 0.75-1.38). The P value for interaction between these groups was 0.1772. Interestingly, patients presenting with more severe PE, defined as right-ventricular dysfunction determined by a NT-proBNP (N-terminal of the prohormone brain natriuretic peptide) ≥500 pg/mL, had a significantly reduced risk of symptomatic recurrent VTE with edoxaban versus warfarin (3.3% vs 6.2%; HR = 0.52; 95% CI = 0.28-0.98). The potential of edoxaban to have more impact on patients with PE and more severe PE warrants further study. Whereas the occurrence of major bleeding was not different between the groups (HR = 0.84; 95% CI = 0.59-1.21), there was an almost 20% relative reduction in major and CRNM bleeding with edoxaban compared with warfarin (HR = 0.81; 95% CI = 0.71-0.94; P = 0.004).
In summary, all DOACs have been found to be noninferior to dose-adjusted VKA for the treatment of DVT or PE. Furthermore, rivaroxaban and apixaban (initiated alone) showed noninferiority in comparison with standard therapy initiated with parenteral anticoagulants. In terms of safety, all agents demonstrated better bleeding profiles than VKA.41-43,46-48
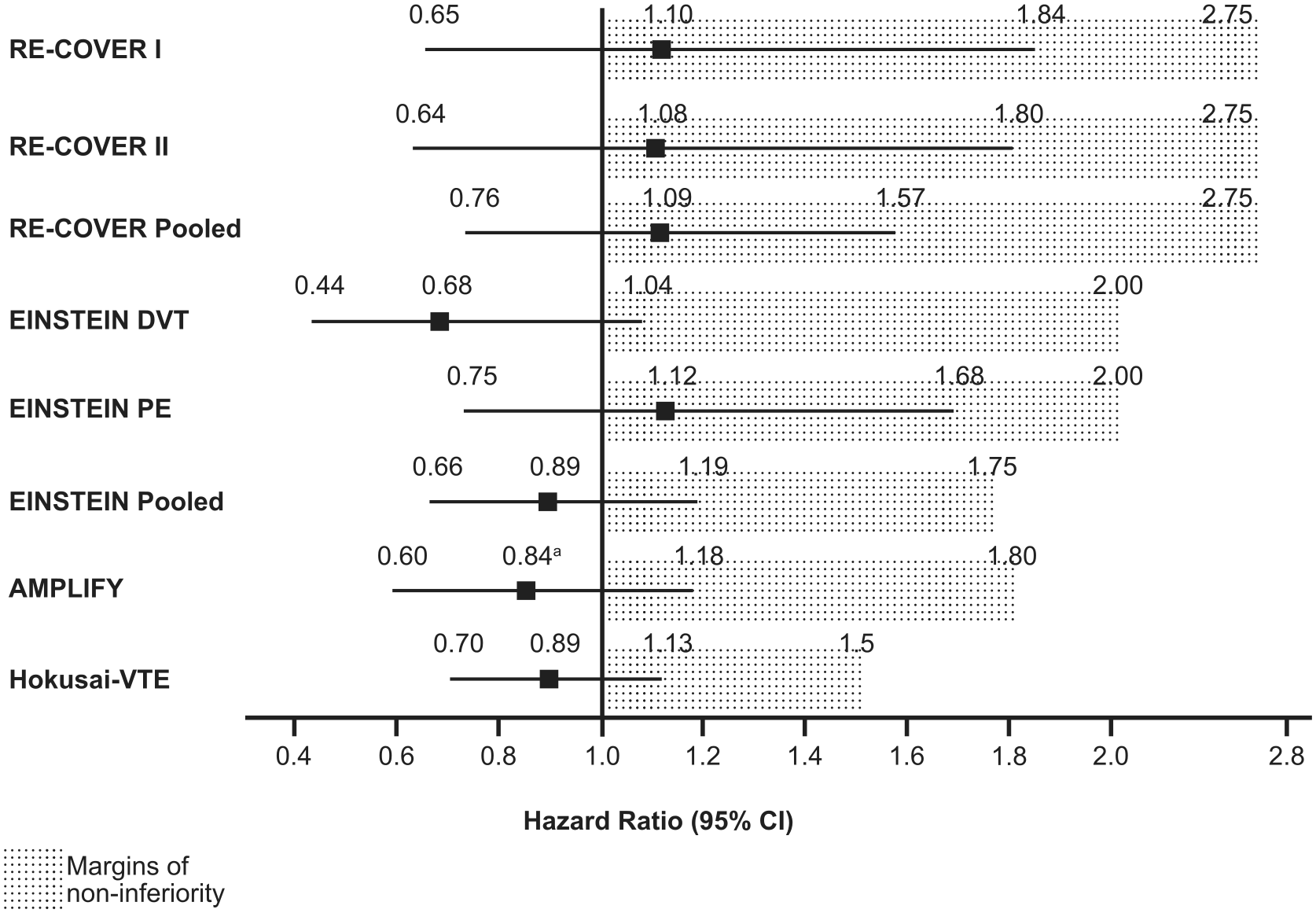
The primary end point in each of these trials was the noninferiority of the DOAC compared with standard of care. Noninferiority trials are designed to show that a treatment is “as good as” current therapy and are commonly implemented when the use of placebo would be unethical. The definition of noninferiority did differ between the trials. Noninferiority margins are determined by considering the uncertainty associated with the estimated treatment benefit as well as a tolerable margin for similarity between the tested and established therapy. The RE-COVER trials had the highest boundaries for noninferiority, with the HR for noninferiority being out to 2.75 (Figure 1). Both trials met this definition; the outer 95% CIs achieved with dabigatran were 1.84 and 1.80 in the RE-COVER I and II trials, respectively.42,43 Although this definition of noninferiority is wider than any of the other trials, this is a reflection of the smaller sample size of the RE-COVER trials compared with the others. In the pooled RE-COVER analysis, the outer 95% CI is narrower, at 1.57. 42 In the EINSTEIN trials, the definition of noninferiority was an outer 95% CI of 2.0. In the EINSTEIN-DVT and EINSTEIN-PE trials, the outer 95% CIs achieved with rivaroxaban were 1.04 and 1.68, respectively.39,40 Once again, with the larger sample size, the pooled analysis has a narrower outer 95% CI of 1.19. 46 In the more recent AMPLIFY and Hokusai-VTE trials, the noninferiority margins were decreased to a RR of 1.80 and a HR of 1.50, respectively.38,41 It is also important to note that the mean HR for all of these trials range from 0.68 (EINSTEIN-DVT) to 1.12 (EINSTEIN PE). Overall, the trial results support the noninferiority of DOACs to standard of care as well as a lack of any real difference between these management strategies in terms of efficacy.
Clinical Trials for Extended Secondary Prevention of VTE
Long-term trials of secondary prevention of VTE have been conducted for all DOACs except edoxaban and have demonstrated superiority of the DOACs in preventing their primary efficacy end point versus placebo (Table 4).39,47,48 Although a significant increase in major bleeding was not observed in the DOAC arms in any of these trials, the rates of major/CRNM bleeding were increased with each of these agents (Table 4), with most differences found in hematuria, epistaxis, and/or rectal bleeding.39,47,48 Furthermore, the incidence of major/CRNM bleeding was numerically lower for apixaban 2.5 mg twice daily than for 5 mg twice daily (RR vs placebo = 1.20 and 1.62, respectively). 48 Therefore, use of a DOAC for long-term secondary prevention of VTE is effective, with some increase in CRNM bleeding. Based on the AMPLIFY-EXT data, a dose reduction after 6 months of full-dose treatment is justified with apixaban and should be evaluated with the other agents.
Comparison of Long-term Secondary VTE Prevention Trials.
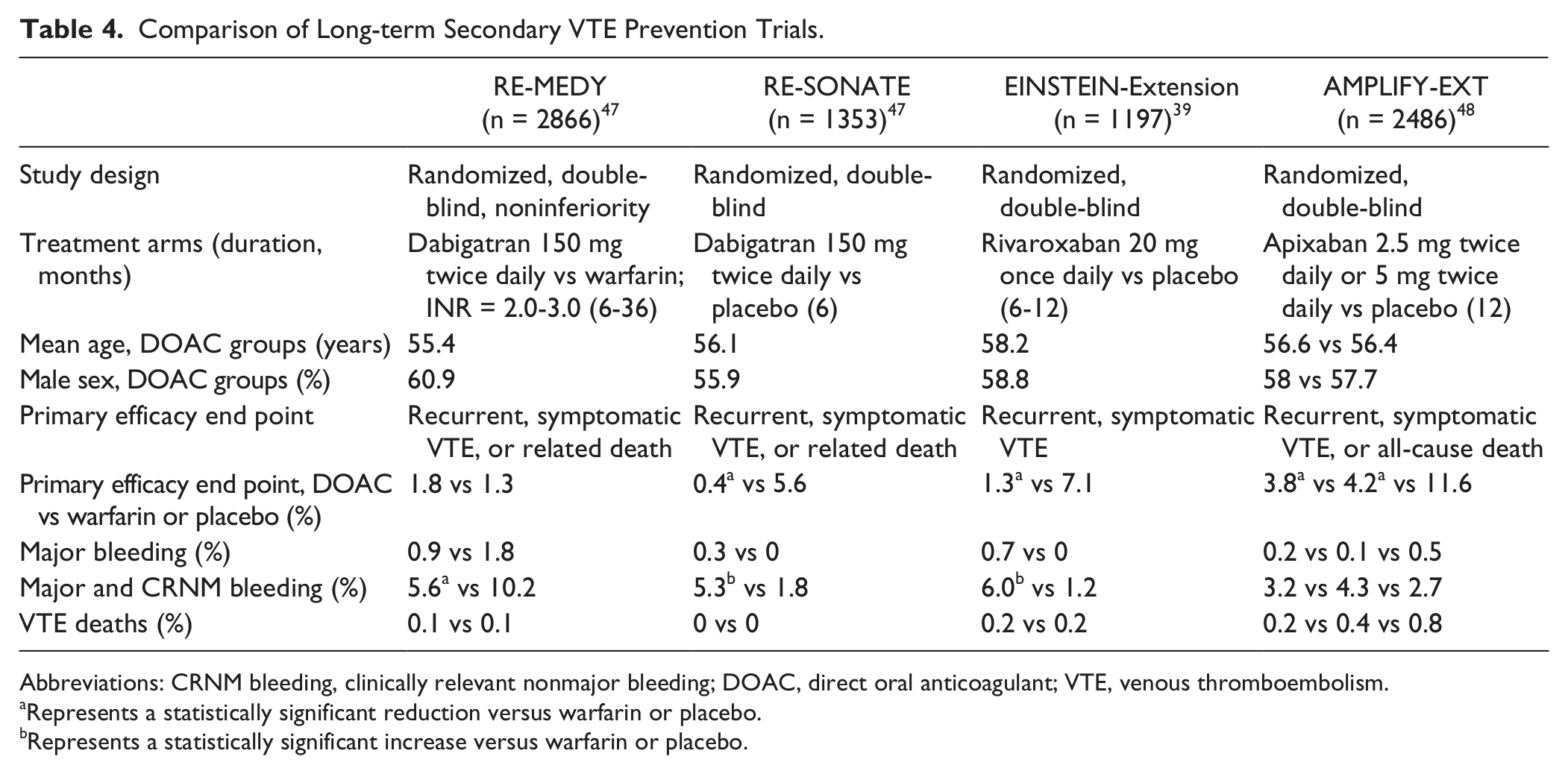
Abbreviations: CRNM bleeding, clinically relevant nonmajor bleeding; DOAC, direct oral anticoagulant; VTE, venous thromboembolism.
Represents a statistically significant reduction versus warfarin or placebo.
Represents a statistically significant increase versus warfarin or placebo.
To date, only 1 trial has evaluated the efficacy and safety of a DOAC in comparison with warfarin for the long-term secondary prevention of VTE. In the RE-MEDY trial, dabigatran demonstrated noninferiority (P = 0.01) compared with warfarin for the primary composite efficacy outcome of recurrent symptomatic and objectively verified VTE or death, either unexplained or by VTE. Major bleeding was reduced by 50% but was not able to achieve statistical significance (P = 0.06). There was a significant reduction in major/CRNM bleeding (Table 4) compared with warfarin (HR = 0.54; 95% CI = 0.41-0.71). As reported in other investigations of oral direct thrombin inhibitors and dabigatran, there were significantly more acute coronary events in patients receiving dabigatran than in those receiving warfarin (0.9% vs 0.2%; P = 0.02). 47
Clinical Considerations in Incorporating DOACs in the Management of VTE
Recently published antithrombotic guidelines support the use of DOAC agents over VKA therapy (Grade 2B recommendation) in patients with DVT or PE without cancer. 49 Despite the significant advance that DOACs represent, they are not without risk, and thus, clinicians need to consider a number of clinical issues to optimize treatment. Assessment of the following factors may be helpful in selecting one DOAC over another or, alternatively, oral anticoagulation with a VKA.
Pharmacokinetic and Dosing Considerations
The pharmacokinetic characteristics of DOACs have been well described. 50 Because the DOACs have predictable and stable pharmacokinetics and pharmacodynamics, unlike VKAs, routine monitoring of anticoagulant activity is not required.11,28,29,50 However, it is important to note that in clinical scenarios where the pharmacokinetic/pharmacodynamic response may be altered significantly (eg, organ dysfunction or drug-drug interactions), there currently is no readily available coagulation assay approved in the United States that can precisely assess the level of anticoagulation for any of the DOACs. For information on currently available coagulation assays to measure the level of anticoagulation with DOACs, the reader is referred to several recent reviews.51,52 Despite this gap, the great majority of patients can be appropriately managed with standard fixed doses for each DOAC, which greatly simplifies many aspects of patient management compared with VKAs. The potential for dosing errors with DOACs is still present, however. The 4 agents have achieved regulatory approval in the United States for the treatment of acute or chronic VTE, each with a different dosing scheme that may differ by indication, adding some complexity for the clinician when selecting the appropriate dose. Table 1 highlights the approved dosing regimens per indication for the DOACs available in the United States.
Depending on the health care setting, clinicians may routinely interact with patients on different DOACs, and care must be taken to ensure appropriateness of the chosen therapy and initial dose. In addition, transition from injectable agent to oral DOAC (dabigatran, edoxaban) or from oral high dose to oral maintenance dose (rivaroxaban at 21 days, apixaban at 7 days) should be implemented at the appropriate juncture. Particularly at times of transitions of care (ie, bridging), the practitioner may be faced with multiple decisions regarding switching agents or alternative anticoagulation. Data to support best practice in switching from VKA to a DOAC or vice versa are, however, limited, although the phase 3 DOAC trials in VTE and atrial fibrillation (AF) as well as best practice reports provide some information.51,53-56
Considerations With Organ Dysfunction
Altered renal or hepatic function may require dose adjustment of DOACs or perhaps consideration of an alternative agent or treatment strategy. All the DOACs rely to some degree on the kidneys for elimination, with dabigatran the most heavily dependent on renal clearance (Table 2). As such, renal function should be assessed prior to initiation of and periodically during therapy as well as whenever there is a potential for a decline in renal function, to identify patients who may be at risk of drug accumulation and adverse events. 50 Moderate renal impairment (CrCl = 30-50 mL/min) increases dabigatran exposure approximately 3-fold. 30 Because rivaroxaban is partially excreted by the kidneys (Table 2), drug exposure is increased to a lesser degree with decreased renal function (eg, 1.5-fold increase with moderate renal impairment). 31 Increases of 44% in apixaban plasma concentrations have been observed in patients with severe renal impairment (CrCl < 15 mL/min) as compared with individuals with normal CrCl.32,57 Modeling observations in dose-ranging trials for edoxaban suggested that a 50% dose reduction would be appropriate for patients with a CrCl of 30 to 50 mL/min. 58 Dose adjustment practices for renal dysfunction varies depending on agent and indication. Currently, there are no recommended dose reductions for renal impairment in patients with VTE with dabigatran, rivaroxaban, or apixaban in the United States. Dosing adjustments in VTE are available for edoxaban (Table 1). Dose adjustments are recommended for all 4 agents in other indications (eg, AF). This is important given that all the VTE studies excluded patients with CrCl <25 or 30 mL/min, depending on the study. Although these differences in dose adjustment recommendations (Table 2) have generated some controversy with clinicians, data from phase 3 clinical trials have confirmed that the strategies in VTE are appropriate. 46 Nevertheless, clinicians will need to be cognizant not only of assessing renal function in patients initiated on DOACs, but also that recommendations for the management of each agent will vary depending on level of renal dysfunction as well as indication.
Clinicians must also consider underlying hepatic function when prescribing DOACs for VTE. As a number of coagulation factors are produced in the liver, coagulopathy is a risk in severe hepatic impairment. 59 Hence caution needs to be exercised when any anticoagulant agent is considered in patients with severe hepatic dysfunction. Furthermore, because patients with moderate to severe hepatic dysfunction were typically excluded from phase 3 clinical trials, the overall risk in these patients is not well characterized. Clinicians may expect to encounter patients with VTE who have varying degrees of hepatic dysfunction from alcoholic cirrhosis or hepatitis C infection. Table 2 depicts recommendations from the US prescribing information for patients with varying degrees of hepatic dysfunction.
The ability to accurately measure the level of anticoagulation and subsequently adjust the dose of any DOAC would facilitate the optimal management of patients with moderate to severe organ dysfunction. However, as previously stated, the availability of such an assay for each agent is lacking in the United States, and clinicians should rely on current regulatory guidelines appropriate for the practitioner’s jurisdiction for adjusting the dose of any DOAC for renal or hepatic dysfunction.
Drug-Drug Interactions
Although fewer in number as compared with VKAs, pharmacokinetic drug-drug interactions for each DOAC pose a potential for significant plasma concentration alterations. The management of drug-drug interactions with VKAs historically has involved the adjustment of maintenance doses to maintain a therapeutic INR to successfully mitigate the risk for adverse events. However, the lack of a readily accessible coagulation assay that precisely estimates the degree of anticoagulation with DOACs prevents clinicians adopting a similar approach. Therefore, an alternative approach to the management of drug-drug interactions with DOACs is needed, whereby drug-drug interactions are considered as precautions or contraindications.
Dabigatran, rivaroxaban, apixaban, and edoxaban all interact with P-gp transporter proteins (Table 2).33-36,60 Certain P-gp inhibitors can increase anticoagulant exposure,5,6,33-35,60,61 and conversely, certain P-gp inducers can reduce bioavailability, and concomitant use should be avoided (Table 2).5-7,33 Rivaroxaban and apixaban are metabolized via cytochrome p450 pathways, and strong dual P-gp and CYP3A4 inhibitors can increase exposure, whereas strong dual inducers can decrease anticoagulant exposure (Table 2).6,7,34
It is important to recognize that for each individual DOAC, there may be differing recommendations for managing drug-drug interactions depending on the indication. In addition, many recommendations for managing drug-drug interactions require the simultaneous consideration of renal function. Table 2 contains the current available recommendations from US prescribing information in handling drug-drug interactions for the DOACs.
Similar to other anticoagulants, the potential for pharmacodynamic drug-drug interactions exists when DOAC therapy is coadministered with other drugs that can affect hemostasis. Concomitant use of nonsteroidal anti-inflammatory drugs (NSAIDs), antiplatelet agents, other anticoagulants, and fibrinolytic therapy increase bleeding in patients receiving anticoagulants.5-7,62-65 Pooled analysis of the dabigatran RE-COVER and RE-COVER II trials, however, showed no impact of low-dose aspirin or NSAIDs on treatment effects, but patients on long-term antiplatelet therapy were excluded from these trials.42,43 Use of NSAIDs and antiplatelet drugs were discouraged but allowed in the EINSTEIN studies.39,40 Patients on dual antiplatelet or daily low-dose aspirin were excluded from the AMPLIFY program.38,48 Therefore, the impact of these agents on the efficacy and safety of the DOACs in VTE treatment has not yet been determined. Similarly, patients requiring fibrinolytic therapy for acute VTE treatment were excluded from the RE-COVER, EINSTEIN, and AMPLIFY programs.38-40,42,43,48 Regardless, the risk of bleeding would be expected to increase with DOACs in the presence of other antithrombotic agents, and careful risk assessment should take place prior to initiating DOAC therapy in patients taking additional agents that can affect hemostasis.
Bleeding Risks
Bleeding and reduced hemostatic responses are risks with the DOACs, and the management of bleeding events with these agents is in many ways similar to that with VKAs.54,66,67 There are some agent-specific options, such as maintenance of diuresis by fluid replacement or hemodialysis, to support renal clearance of dabigatran as well as general procedures, including supportive treatment, general hemostatic measures, and transfusion of blood products.54,66,67 The rapid-acting reversal agent idarucizumab (aDabi-Fab; Boehringer Ingelheim, Ingelheim, Germany) was approved by the US Food and Drug Administration (FDA) in October 2015 for use in patients treated with dabigatran when reversal of the anticoagulant effects of dabigatran is needed (ie, for emergency surgery/urgent procedures or if there is life-threatening or uncontrolled bleeding).68,69 In the RE-VERSE AD study, idarucizumab demonstrated complete reversal of dabigatran within minutes of administration, as demonstrated by normalization of ecarin clotting time and dilute thrombin time. Of the patients with elevated baseline values, dilute thrombin time was normalized in 98% of those with serious bleeding (group A) and in 93% of those requiring urgent surgery or intervention (group B), and ecarin clotting time was normalized in 89% and 88% of patients in these respective groups. 70 Two other reversal agents, andexanet alfa (r-Antidote, Portola Pharmaceuticals Inc, San Francisco, CA) and ciraparantag (PER-977, aripazine, Perosphere Inc, Bedford, MA) are in late-phase clinical development and have been granted accelerated approval status by the FDA.71-75 Two phase 3 trials in healthy older volunteers (50-75 years old) have demonstrated the efficacy of andexanet alfa in reversing the anticoagulant effects of apixaban (ANNEXA-A) and rivaroxaban (ANNEXA-R). 76 Additionally, in a phase 1 study, hemostasis was restored within 30 minutes and was sustained for 24 hours after administration of ciraparantag after edoxaban exposure. 77
Additional Clinical Considerations
Patients Requiring Dual-Antiplatelet Therapy
As previously discussed, the addition of antiplatelet therapy to oral anticoagulation with DOACs can increase the risk of bleeding. Whereas antiplatelet monotherapy (generally aspirin at doses of <100 mg/d) was allowed in phase 3 clinical trials, the presence or need for dual antiplatelet therapy (DAPT) was an exclusion criterion in the VTE clinical trial programs. 78 As such, there is limited information in the VTE population on the balance of risks and benefits of using DOACs in patients requiring DAPT. Available acute coronary syndrome clinical trial data demonstrate a significantly increased risk of major bleeding when DOACs are coadministered with DAPT. 79 Until further information becomes available, patients requiring DAPT and who experience VTE events should be managed with VKAs for at least the duration that the DAPT is indicated.
Patients With Underlying Valvular Heart Disease
Clinicians will need to assess for underlying valvular heart disease and determine if anticoagulation with a DOAC is appropriate, especially in those patients with concomitant AF. Clinicians should avoid using DOAC therapy in patients with mechanical heart valves and/or moderate to severe mitral stenosis based on exclusion criteria in clinical trials, subgroup analyses, and current US prescribing guidelines.80,81 These patients should be managed with VKA therapy. Patients with other forms of valvular heart disease such as aortic/mitral regurgitation, aortic stenosis, or bioprosthetic valve replacement are more challenging because it is not clear from phase 3 clinical trials if DOAC therapy should be avoided in such patients. However, there is some evidence from trials including such patients that the efficacy and safety results did not differ from the overall patient populations, indicating that DOAC therapy could be used safely. 80 Although further information with patients with valvular heart disease would be welcome, at this time, clinicians may consider DOAC therapy an option for VTE management in patients who have certain types of valvular heart disease, such as aortic/mitral regurgitation, aortic stenosis, or bioprosthetic valve replacement.
Extremes of Body Weight
Although currently available information does not suggest a need for dose adjustment in overweight/obese patients, additional information on the pharmacokinetic/pharmacodynamic response in patients weighing >150 kg would be valuable. 50 There are limited data in dabigatran-treated patients with weights of <50 or >100 kg showing that trough concentrations may be ~20% lower at weights >100 kg compared with patients with body weight of 50 to 100 kg. 82 Data from analyses in other indications (eg, orthopedic surgery) suggest no clinically significant impact of overweight or obesity; thus, there are no requirements for dose adjustments.5,82-84 Similarly, low body weight (ie, ≤50 kg) caused changes of <25% in rivaroxaban peak plasma concentration, although rivaroxaban exposure was not affected by body weight (≤50 kg vs 70-80 kg vs >120 kg), and so no dose adjustments were considered necessary. 85 There were also variations in apixaban exposure with extremes of body weight (≤50 or ≥120 kg) of approximately 20% to 30%. 86 No dose adjustments because of weight alone were considered necessary with apixaban, although, when combined with other factors, dose reduction at low weights may be prudent. 86 Table 3 contains the range of body weights seen in phase 3 clinical trials; if clinicians encounter patients weighing outside of these ranges, appropriate management should be considered on an individual basis.
Dietary Interactions/Drug Administration
Numerous dietary interactions cause variability in the anticoagulant response to VKAs. In contrast, the DOACs are free of such interactions, although food increases the bioavailability of higher doses of rivaroxaban.5-7,11,13,37 Dabigatran etexilate is formulated in capsules with tartaric acid to provide the acid environment necessary for its efficient absorption, rendering it independent of gastrointestinal acidity.11,87 Patients, however, need to be warned not to break open or chew capsules because this can increase drug exposure. Also, capsules should be stored in their original packaging to protect them from deterioration caused by moisture. 5
Patients at Risk for Medication Nonadherence
Although once-daily regimens may theoretically be associated with greater medication adherence than twice-daily formulations, missing a dose from either a once-daily or twice-daily regimen can likely result in subtherapeutic anticoagulation and pose short-term risk of VTE recurrence. 88 Risk for nonadherence should be considered in selection of anticoagulant for each patient. In addition, programs that can improve medication adherence are vital. Recent information from the Veterans Health Administration system demonstrated that high-quality anticoagulation management practices (such as appropriate patient selection and education, ensuring good transitions of care and routine follow-up monitoring of clinical status) are associated with improved rates of adherence to dabigatran for the prevention of stroke in patients with AF. 89 Similar interventions would be likely to produce the same benefits in patients on DOAC therapy for the management of VTE.
Management of VTE in Active Cancer/Malignancy
Cancer and its treatment have been recognized as risk factors for VTE. 90 Furthermore, treatment of cancer-associated VTE provides greater challenges than treatment in noncancer populations, because patients with cancer have a greater risk of VTE recurrence during anticoagulation as well as an increased risk of bleeding. 91 The 2014 clinical practice guideline update of the American Society of Clinical Oncology recommends low-molecular-weight heparin (LMWH) for the initial treatment of VTE (5-10 days) as well as for long-term (≥6 months) secondary prophylaxis in patients with cancer. 92 Similarly, the CHEST guidelines, which were recently published by the American College of Chest Physicians, recommend LMWH over VKAs in patients with cancer and VTE. 49 This is based on evidence that LMWH is more effective than VKAs in this patient population as well as for practical reasons such as the difficulties of keeping VKA-treated patients with cancer in therapeutic range and the fact that LMWH is easier to withhold or adjust than VKA if invasive interventions are required. Use of DOACs, however, is not currently recommended in patients with VTE and cancer in either of these guidelines.49,92 The CHEST recommendations suggest that LMWH may be more effective than DOACs in patients with cancer, based on indirect comparisons. 49 However, findings from meta-analyses concerning the relative effectiveness of LMWH versus DOACs in patients with cancer are conflicting.93,94 Therefore, results from ongoing trials comparing DOACs with LMWH are required before the role of DOACs in patients with cancer and VTE can be established.
Role of the Pharmacist in VTE Treatment
In both inpatient and outpatient settings, the literature supports the role of the pharmacist in VTE management. 95 Pharmacist-led services can improve anticoagulation management and have been associated with cost savings relative to physician control. 96 Findings from health care database analyses and audits suggest that more than 25% of patients do not start VKA therapy, more than 25% of patients on VKA do not have their therapy adequately monitored, and treatment is taken for a shorter duration than recommended (median = 61 days).83, 84 Similar drop-out rates have been reported with the DOACs in other indications; 21% of patients stopped treatment in the RE-LY trial at 2 years. 97 Because withdrawing from therapy or nonadherence with anticoagulation poses great risk to the patient, the role of the pharmacist in activities to improve adherence for these agents is paramount. 89
Pharmacists can be involved in a number of evidence-based measures to improve outcomes and avoid adverse events in patients receiving anticoagulation. 98 Ensuring that patients’ medications are communicated at transitions in care has been proposed as a measure to improve quality of care in DVT or PE. 99 The transition from parenteral to DOAC or VKA therapy and its subsequent continuation need to be carefully managed to ensure dose appropriateness and follow-up. For example, the pharmacist can help facilitate the required dosage adjustments at days 7 and 21 with apixaban and rivaroxaban, respectively. According to Joint Commission National Patient Safety Goal 03.05.01, education of patients about their anticoagulant therapy is “vital” in reducing the risk of adverse events with heparins and VKAs. 100 Pharmacists can also ensure safety of DOAC administration both in the inpatient and outpatient populations, specifically monitoring for drug-drug interactions, providing dosing recommendations for those with organ dysfunction or extreme weights as well as monitoring for adherence and opportunities for education reinforcement. Pharmacists are known to contribute substantially to enhanced medication education and the improvement in achieving performance measures and overall care for VTE.95,98
Errors in the prescribing, administration, and monitoring of the DOACs have been identified recently in the outpatient setting. 101 For example, the administration of rivaroxaban inappropriately without food or lack of attention to specific storage requirements for dabigatran can be addressed simply by pharmacist interaction and education. Errors related to inappropriate baseline monitoring and dose selection have also been reported in clinical practice. 101 Many clinicians have not yet developed a familiarity with the DOAC class and would benefit from having readily available guidelines and/or decision support tools that facilitate appropriate dose selection for each agent. Development of such protocols or decisions based on formulary restrictions will require pharmacist input. As with warfarin therapy, transitioning from injectable therapy is still necessary for dabigatran and edoxaban in the treatment of VTE, and pharmacists can play an invaluable role in ensuring successful bridging with parenteral therapies and transition to the proper dose of oral anticoagulation.8,95 Finally, pharmacists should be committed to monitoring and reporting any significant side effects seen with these agents because this will ultimately improve overall patient safety with these agents.
Conclusion
In summary, clinicians now have multiple anticoagulant options for the treatment of VTE. DOACs represent a step forward in the management of VTE, with similar efficacy and improved safety compared with VKAs. Although the limitations of VKAs seem to concede DOACs as superior agents, attention is still required to appropriately select dosing based on indication, avoid drug-drug interactions, and consider dose adjustments for particular clinical circumstances such as organ dysfunction or concomitant medications. Clinicians treating VTE need to be familiar with the intricacies of anticoagulation therapy used in this setting. The pharmacist has unique knowledge to improve the care and successful treatment of VTE through interactions with both providers and patients.
Footnotes
Acknowledgements
The authors would like to acknowledge Joanne Vaughan, BSc, of Envision Scientific Solutions, who provided editorial support, with funding from Boehringer Ingelheim Pharmaceuticals, Inc. BIPI was given opportunity to check data used in the manuscript for factual accuracy only; the authors meet full criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Finks reports no conflicts of interest, including, but not limited to, consulting fees, paid expert testimony, employment, grants, honoraria, patents, royalties, stocks, or other financial or material gain that may involve the subject matter of the manuscript. Dr Trujillo serves as a consultant for Boehringer Ingelheim, Janssen, and BMS/Pfizer. Dr Dobesh serves as a consultant for Boehringer Ingelheim, Janssen, BMS/Pfizer, and Daiichi Sankyo and has received research funding from Daiichi Sankyo.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author received no direct compensation related to the development of the manuscript. Editorial support was provided by Joanne Vaughan, BSc, of Envision Scientific Solutions, which was contracted and funded by BIPI.