
Abstract
Mental health has grown increasingly important as an aspect of employee well-being, with organizations expected to address these needs through offerings to support employee mental health. Broad societal forces like stigma and low levels of literacy surrounding mental health make it challenging for many people to understand these offerings. As the marketplace for these offerings grows to meet this demand, employees, HR professionals, and business leaders need better resources to understand, organize, and distinguish among their choices. The current research offers a 3-dimensional taxonomy for organizing these offerings, distinguishing them according to their (a). Primary Purpose-To Restore or Enrich; (b). Delivery Agent Location-External or Internal; (c). Latitude in Providing-Legally Required or Voluntary Provided. We provide theoretical approaches for scholars to consider these offerings’ impact in workplaces, and briefly demonstrate the taxonomy’s value in organizing some of the commonly available offerings in many modern workplaces. Finally, we provide two attainable research avenues for researchers to explore to inform organizational stakeholders on the (1). prevalence, costs, outcomes of these offerings in the workforce and (2). helpers and hurdles to employees' using these offerings.
Warnings of a mental health (MH) crisis are sounding as people report record levels of daily worry and need for MH support (APA, 2021; NSC, 2021; White House, 2022; World Health Organization, 2022). The acceptance, discussion, and need for MH support seems historically high and likely to grow. Given most people access MH support through their employers (e.g., employer-funded health insurance; Luciano & Meara, 2014), organizations are critically important in meeting this surge of needed MH support. In recent years, 90% of polled employers reported a new priority for employee MH (Minemyer, 2022), 78% of employers offered MH resources to employees (SHRM, 2022), and ∼40% of companies expanded their MH benefits since March 2020 (Adams et al., 2021). Organizations considerably increased their investment in these resources (e.g., an almost 40% increase from 2019–2020; Wortham, 2021), and evidence indicates increased spending will continue, with a projected 11% annual growth until 2030 (Skyquest, 2023). This increase in investment corresponds to employees’ heightened expectations for such support (Greenwood & Anas, 2021). Despite the boosts in employer spending on these offerings, employees still expect more than the status quo (Adams et al., 2021; Deloitte, 2022). Whereas top-level leaders (96%) report their companies do enough for employee MH, only 69% of employees feel the same; and half as many (35%) employees (cf. 70% of leaders) believe their companies are accepting of MH issues at work (Deloitte, 2022; Ginger, 2022). Workers often perceive their companies are merely ‘checking a box’ offering these resources, with some labeling organizations’ efforts as ‘wellbeing washing’ by throwing quick fixes at workers’ complicated health issues (IOSH, 2023). Moreover, longitudinally comparing the rates of MH conditions (e.g., depression, anxiety) to corresponding years’ medical claims (e.g., treatment for depression, anxiety) indicates employer-provided medical benefits may miss up to 75% of employee MH issues (Lewis, 2022).
The disconnect between employers’ offerings and employees’ expectations of MH offerings should spur action from organizational scholars to better describe and explain how such offerings can better meet all parties’ needs. Examples of workplace MH offerings include employer-subsidized benefits to support people with mental illness (e.g., health insurance), employer policies to include people with mental illness (e.g., accommodations), and employer programs to promote MH (e.g., mindfulness training). Organizational spending on these offerings follows somewhat from legal mandates, but organizations also make these investments strategically, to capitalize on the benefits of improved employee MH across domains like employee attraction, retention, safety and health management (Deloitte, 2019; LaSalle Network, 2023). Conversely, workers weigh how workplaces’ MH offerings align with their needs, and they discern deeper signals about what the presence/absence of offerings implies about companies’ valuation of employees (Allen et al., 2003; Valcour et al., 2011; Zhang et al., 2012).
The current research acknowledges the need for organization scholars to consider the confluence of employer investments and strategy in offering MH support and employees’ expectations and perceptions in considering the use of these resources. We use social exchange theories, namely psychological contract theory (PCT; Rousseau, 1989) and organizational support theory (OST; Rhoades & Eisenberger, 2002) to better understand the existing landscape of workplace MH offerings. Drawing also from literature on employee trust, the existing research aims to provide a more complete, coherent picture of workplace MH offerings. Specifically, we offer an initial taxonomy for organizing these offerings. Legal and market forces have, historically, shaped the independent evolutions of each offering, leaving stakeholders—organizations and the employees needing support—to face an atheoretical landscape of many possible resources with little coherent guidance to help them understand each in relation to the others (Amwell, 2023; SHRM, 2022). These stakeholders urgently need a framework to better make sense of the entire landscape. As a 2019 spending report elegantly stated the problem, “The layers of overlapping stakeholders and delivery systems in the U.S. MH market […] result in systems that are difficult to describe, much less measure” (Open Minds, 2020, n.p.). Our taxonomy is an initial effort to provide common language for discussing and considering these offerings, to hopefully increase the chances these offerings make impacts in people’s lives. We discuss how social exchange and trust literatures can be useful to understand how workplace MH offerings work, introduce our taxonomy’s dimensions, and demonstrate its application to an example of workplace MH offerings. Finally, we provide future research directions for organizational scholars to address this critical, underserved need (Deadrick & Gibson, 2007; Dulebohn et al., 2009).
What are Workplace MH Offerings?
Academically, subjects of MH, mental illness, and mental wellness span a vast range of literatures (Bodeker et al., 2020). Practically, terms like mental wellness, wellbeing, and MH are used inconsistently (Dimoff et al., 2021). People often consider and speak of MH as the absence of mental illness, which involves sustained maladaptive and/or abnormal patterns of action, mood, or thought (Center for Disease Control and Prevention, 2021). In contrast, others consider MH as flourishing, characterized by hedonia, positive attitudes towards life, and a sense of direction, connection, and purpose (Keyes, 2002). Authors have provided excellent reviews on the areas of mental illness at work (Follmer & Jones, 2018), and MH at work (Kelloway et al., 2023). Treating all MH constructs as a monolithic phenomenon oversimplifies, 1 because the solutions to abate mental illness significantly differ from solutions to enhance MH. For our purposes, we adopt the definition of MH offered by the World Health Organization (2022 n.p.) as a “state of mental wellbeing that enables people to cope with stresses of life, realize their abilities, learn well and work well, and contribute to their community.” In view of this definition and previous reviews on workplace MH (Follmer & Jones, 2018; Kelloway et al., 2023), we consider workplace MH offerings as all formal organizational benefits, programs, actions, and policies that are principally intended to support or improve employee MH. These include both the offerings that aid employees with mental illness to approach more normal functioning (e.g., access to insurance, employee assistance programs) and the interventions to strengthen and grow MH’s positive symptoms of pleasure, meaning, and ability (e.g., mindfulness training, Keyes, 2002). Below, we introduce social exchange theories and explain the role they play in understanding the value and purpose of workplace MH offerings.
Theoretical Approaches to Consider Workplace MH Offerings
Social Exchange Theories
Mental health offerings feature both formal benefit programs (e.g., health insurance coverage) and policy-enacted daily realities (e.g., MH stigma training; Dobson et al., 2019), that comprise the employee experience at work. Employers ultimately invest in, implement, and maintain these offerings across the full HR lifecycle in order to impact the quality of their relationships with workers. Hence, we believe theories that emphasize the exchanges within the employer-employee relationship are especially relevant to understanding workplace MH offerings. Psychological contract theory and OST are two social exchange theories focused on the relationships formed by two parties to maximize their benefits through exchanging resources (Blau, 2017). In the workplace, employees offer work and loyalty in exchange for organizationally offered material and socioemotional rewards. Employees, these theories hold, are motivated to reciprocally match the quality of the rewards that they receive. Exceptional rewards and circumstances motivate exceptional employee contributions, and poor rewards motivate poor employee input (Aselage & Eisenberger, 2003).
Predominantly, PCT has been used to explain the consequences of employers’ failures to uphold their end of this exchange. Psychological contracts capture the unspoken, unwritten agreements between workers and employers, particularly the expectations each holds of the other. These contracts encompass obligations and the tangible and intangible rewards associated with the employer-employee relationship (Lester et al., 2001). Psychological contract theory explores undesirable worker reactions, like absenteeism, turnover, and disengagement, to perceived contract breaches (Zhao et al., 2007). But PCT also highlights how meeting expectations fosters employee motivation and MH (Parzefall & Hakanen, 2010). In addition to tangible, transactional resources, workers hold indefinite expectations of relational resources from employers (Tekleab et al., 2005). So, the domain of employer offerings—from benefits to training—is rife with moments to fulfill or breach the psychological contract (Bartlett, 2001; Lucero & Allen, 1994). Workers can form their expectations even before joining the company (Sutton & Griffin, 2004), and these expectations differ across groups, based on interests and identities (Pant & Venkateswaran, 2019). Workers consider (un)met expectations by their supervisors independently of (un)met expectations by their employer, with each expectation process yielding different consequences (e.g., leader member exchange v. perceived organizational support; Chaudhry & Tekleab, 2013). Thus, organizations providing benefits (e.g., at the organizational level) must also effectively implement the benefits (e.g., at the managerial level) to uphold their obligations in employees’ minds. In the case of MH offerings, these tenets can explain how workers of different groups (e.g., generation, industry) and dispositions (Karagonlar et al., 2016) may expect different things of their employers, and how employers are motivated to provide relevant support for MH, as part of their commitment to support their workers’ flourishing (Tekleab et al., 2005).
Employers can also affect workers’ assessments of their relationship by exceeding what is required. Organizational support theory provides insights into how workers evaluate and interpret company actions to assign attributions and intention to how they are treated at work (Eisenberger et al., 1997). Perceived organizational support (POS) captures workers’ holistic beliefs regarding how well their organization values and cares for them (Rhoades & Eisenberger, 2002). Perceived organizational support exerts a significant impact on workers’ wellbeing, their willingness to engage in positive behaviors within the organization, and their intentions regarding turnover (Kurtessis et al., 2017). Legal requirements, for example, may create a broad expectation for employers to provide some MH offerings (e.g., accommodations for mental illness). But competing in the labor market and meeting worker retention goals by providing these programs leads many companies to offer more than what is required (e.g., paid leave, care giving benefits, personal wellness resources). These voluntarily offered programs exceed expectations and may result in an outsized boost for companies, both from prospective and current workers. For example, applicants are more likely to apply to jobs that feature benefit offerings beyond what is required by law (Garcia et al., 2010). Additionally, the positive impacts of favorable job conditions are six times greater when workers believe the company voluntarily (cf. compulsorily) provided them (Eisenberger et al., 1997). Organizational support theory, then, can explain how workers and employers weigh the value of certain benefits, beyond the threat of a broken expectation.
Trust
The exchange theories discussed above provide important explanations for why employers provide MH offerings, especially those beyond legal requirements, and the mechanisms through which these offerings influence workers’ behavior. Compared to many other types of workplace support, workplace MH offerings raise greater doubt and hesitance for many. For example, a primary reason that workers do not use their free employee assistance programs, a benefit specifically supporting MH, is skepticism about the privacy and professional consequences of seeking such help (Agovino, 2019). Disclosing MH needs or seeking MH support at work carries the real risks of being ostracized, discriminated against, and losing job/responsibility opportunities (Follmer & Jones, 2018; Toth & Dewa, 2014). In considering how these offerings operate in the employer-employee relationship, then, we also must consider the impact of trust.
Researchers have devoted tremendous attention to trust, with ties to many aspects of organizational psychology. We draw from two excellent reviews (Dirks & de Jong, 2022; Fulmer & Gelfand, 2012). Trust fundamentally involves two parties, a trustor, who experiences a psychological state of willingness to be vulnerable towards, without fully knowing the actions and intentions of, the trustee, the person receiving or evoking the trust (Möllering, 2001; Rousseau et al., 1998). Trust involves both a trustor’s rational assessment, based on experiences and collected ‘data’ about the trustee (Schoorman et al., 2007), but also the trustor’s irrational, emotional feelings towards the trustee, which can be influenced by the trustor’s dispositional traits (Colquitt et al., 2007), their situational dependencies on the trustee (Weber et al., 2004), and even aesthetic qualities of the trustee (Baer et al., 2018; Holtz, 2015).
For workers contemplating using their organizations’ MH offerings, trust appears a critical factor. Indeed, employee MH states are positively associated with antecedents and correlates of trust like a supportive organizational climate (Bronkhost et al., 2015), favorable work structure characteristics (e.g., equitable rewards, consideration for employees; Gavin, 1975), and managerial training on MH challenges and stigma (Gayed et al., 2018; Pischel & Felfe, 2023). Seeking support involves the possibility of disclosing one’s MH state, including a mental illness, and workers’ willingness to be vulnerable towards their company and manager merits close focus (Follmer et al., 2022; Follmer & Jones, 2018; Toth & Dewa, 2014). Researchers have identified a robust domain of trust’s relevance to social exchanges in the employer-employee relationship (Fulmer & Gelfand, 2012). Psychological contract breaches (Bal et al., 2008) and POS (Kurtessis et al., 2017) both emerge as pivotal antecedents of trust. Moreover, trust mediates the relationships of these variables with various attitudinal, behavioral, and performance outcomes (Dirks & de Jong, 2022). Social exchange theories offer insights into workers’ expectations of MH offerings and how evaluations of these offerings influence their relationship with employers. On the other hand, trust literature provides critical details on how the drivers of trust may influence workers’ perceptions of this relationship and likelihood to use the offered support. Recently, some researchers have begun discussing organizational-level factors related to trust, expectations, and MH, namely the construct of a MH climate, characterized by formal (e.g., education/training programs, supportive policies) and informal (e.g., norms) social systems that make MH information available and acceptable to discuss at work (Bronkhorst et al., 2015; Kelloway et al., 2023). This nascent concept of a MH climate relates to POS and MH literacy (Hastuti & Timming, 2021), or the knowledge of ‘how to obtain and maintain good MH’ (Kutcher et al., 2016a, p. 567). Here we note MH climate’s likely relationship to correlates of organizational trust as well.
With these theoretical lenses in mind, we next briefly outline eight workplace MH offerings commonly available to workers. Our primary goal in this article is to elucidate a categorization scheme for MH offerings, not an exhaustive inventory of every potential MH offering in workplaces. We therefore present frequently-provided offerings available in many modern workplaces. We begin by providing context on the incidence rate for those who could use these offerings, and a glimpse into how employees will likely need even more support in the future.
Workplace MH Offerings
We earlier referenced a growing MH crisis, which workplace MH offerings are intended to help address. Here we provide more detail to preview the accelerating societal need for and prevalence of these offerings. Approximately 50% of all people will experience a MH issue in their lifetime. In any given year, 20%–29% will experience symptoms of a mental illness (Brouwers, 2020), and approximately 20% of adults will be diagnosed with a mental illness (Fronstin & Roebuck, 2022; Luciano & Meara, 2014), with 5% of adults grappling with serious mental illness (Hasin et al., 2018). Estimates indicate a 30% increase in MH disorders among employed adults from 2013 to 2020, with a 32% increase in these employed adults seeking outpatient MH support (Fronstin & Roebuck, 2022). Recall that MH is not simply the absence of mental illness (Keyes, 2002), although mental illness prevalence rates clearly indicate the demand for MH offerings. Stress, meanwhile, causes 20%–40% of adults to experience daily functional deficiencies (APA, 2022). Moreover, changing workforce demographics are likely to exacerbate these issues. The ‘greying’ of the workforce, where workers defer retirement, results in a labor pool featuring a greater number of older workers, who need greater MH support (Mc Carthy et al., 2017). Simultaneously, younger workers, who are now or soon entering the workforce, are at particularly high-risk for MH threats (LaSalle Network, 2023; Richtel, 2021), and have received unprecedented MH support in their lives: school-offered accommodations for stresses/demands of coursework tripled from 2000–2016 (Belkin et al., 2019) while EEOC claims of discrimination related to anxiety disorders increased by 500% in a similar time period (Weber, 2020). Together, the workforce’s changes show clear links to the surging need for and availability of workplace MH offerings.
Employers are responding to this surging need with a range of MH offerings. Workplace MH offerings appear poised for continued growth as companies will continue to spend on them, with estimated expenditures on support for mental illness reaching $77 billion as of 2020, an increase of 20% since 2013 (Fronstin & Roebuck, 2022). Spending on additional MH resources like meditation and mindfulness is set to reach $7.6 billion by 2031 (Skyquest, 2023). Employees will continue to want these offerings from their workplaces, given 4 out 10 workers say they would leave their current job for one that provided better MH offerings (Mayer, 2023). From all signs, then, workplaces and employees will see more of these MH offerings in professional settings.
Common Workplace MH Offerings
Below we review some major types of offerings commonly provided by employers. In reading this brief review, imagine yourself as (1) an employee who suspects you need help with your MH, but are unsure what resource to use, (2) an HR professional who must advise, administer, and assist employees in navigating these offerings, or (3) a business leader seeking to compete for talent and invest meaningfully, but strategically, in your employees’ MH. All three perspectives merit consideration in discussing workplace MH offerings, such that no offering can produce an effect without the correct stakeholder to choose, administer, or use it.
Health Insurance Coverage for Mental Illness
Almost 90% of workers with a mental illness are enrolled in a health insurance plan to cover costs like prescription drugs, therapy, inpatient and outpatient services arising from treatment (Centers for Medicare and Medicaid Services, n.d.). Employer-funded health insurance provides a critical access point to any type of care for the roughly 55%–70% of workers who receive MH care for themselves or family (Luciano & Meara, 2014), although almost 60% of U.S. adults with a mental illness receive no treatment at all (Reinert et al., 2021). Despite federal laws requiring group health plans to offer equitable coverage for mental illness (cf. physiological health conditions), evidence indicates many people with mental illness still face greater costs to receive care (Kaiser Family Foundation, 2021). Like other legally mandated offerings, health insurance coverage stands as a primary expectation and focus for many workers in making employment decisions (Jones, 2017), especially given the critical effects of access to health insurance coverage for people with mental illness (Baumgartner et al., 2020).
Non-discriminatory Practices and Workplace Accommodations
Because U.S. federal fair labor and employment practices laws (e.g., ADA) cover mental illnesses, non-discrimination and accommodation policies also apply to covered employer interactions with workers with mental illness. Employers must use unbiased recruiting and selection processes to minimize any adverse effects that jobseekers with mental illness experience compared to those without mental illness (U.S. EEOC, 2022). Additionally, workers who meet diagnostic criteria and coordinate with their employers are entitled to work accommodations and scheduling modifications relevant to their mental illness (McDowell & Fossey, 2015). An estimated 23%–65% of all eligible workers receive accommodations for a disability at work (Maestas et al., 2019), although only 16% of workers with a mental illness received a workplace accommodation (McDowell & Fossey, 2015). Interestingly, some research indicates people broadly think accommodations for mental illness are less legitimate, necessary, or reasonable than accommodations for physical disabilities (Telwatte et al., 2017) and that managers still hold biased attitudes against people with mental illness (Janssenns et al., 2021). Reflective of these attitudes, anxiety and depression were the third and fourth highest-ranked causes for ADA-based EEOC claims in 2020, and employment discrimination claims filed by individuals with anxiety disorders have been deemed meritorious in greater percentages than for other disabilities (U.S. EEOC, 2022).
Return to Work
Workers who temporarily leave the workforce due to mental illness may benefit from return-to-work (RTW) offerings. Return-to-work programs aim to safely and gradually ease a worker back into the workplace after a leave of absence, and are often created in collaboration between the worker, supervisor, and an assigned RTW coordinator. Traditionally, RTW programs have centered on individuals with physical disabilities or conditions, although protocols have also effectively been applied to those with mental illness (Dewa et al., 2021; Edgelow et al., 2020; MacEachen et al., 2020).
Employee Assistance Programs
Perhaps the most well-known workplace MH offering is the employee assistance program (EAP). Employee assistance program offerings differ greatly but we use a generic definition for our purposes as “a workplace program designed to assist […]. […] that may affect job performance” (International Employee Assistance Professionals Association). Most commonly, an EAP provides a worker or their family member five to eight sessions of therapeutic intervention to address an acute MH issue (Attridge, 2019), analogous to receiving a finite, scheduled plan of therapy for a physiological need/injury.
Adapting
Organizations may support their workers with mental illness in less programmatic ways, which we loosely capture here as adapting. Compared with other offerings programmatically available to all workers (e.g., health insurance coverage, stress management intervention), adapting offerings are often implemented to adjust to a specific worker’s needs. Organizations may adapt by strategically investing in a work environment that better supports people with MH concerns (Corbière et al., 2015), giving a manager training on how to supervise a person with MH concerns (Dimoff & Kelloway, 2019; Gayed et al., 2018), or implementing programs to reduce MH stigma in their company (Dobson et al., 2019). Companies may even provide unique work arrangements to fit a given worker’s needs, akin to an idiosyncratic work arrangement (Brzykcy et al., 2019). For example, job coaches may be provided to facilitate the transition of a worker with MH issues to assist in complying with work procedures and policies, or companies may provide transportation services to people with MH concerns who cannot obtain a driver’s license (Blitz & Mechanic, 2006).
Some organizations have adopted innovative programs of adapting through neurodivergent staffing practices (Austin & Pisano, 2017). Neurodivergent, or neurodiverse, workers are those people whose abilities and tendencies, viewed in total, differ from ‘normal’, often with extremely high levels of some attributes (e.g., pattern recognition, creative thinking) and below-average levels of others (e.g., working memory, time management). Compared to ‘normal’ workers, whose abilities/tendencies tend to be consistently average, neurodivergent workers possess a pattern of highs and lows across the abilities spectrum that can make them extremely suited for some types of work, but also likely to experience professional ostracism and rejection of candidacy due to their divergence from the norm (Doyle, 2020). MH conditions commonly associated with neurodivergence include autism spectrum disorder or attention deficit disorder (Doyle, 2020). Given 20% of the population is affected by some neurodivergent condition (Weber et al., 2022), organizations using neurodivergent staffing practices can provide strategic value to the company and benefit to employees who are severely underemployed. We direct readers to Khan and coauthors’ (2022) exceptional review on this topic.
Stress Management
Stress management interventions (SMIs) are a common workplace MH offering. Stress management interventions span a broad range of methods, length, and targeted outcomes (Richardson & Rothstein, 2008). They may involve trainings directly offered to employees (e.g., muscle relaxation; Murphy & Sorenson, 1988), programs and policies implemented to reduce organizational sources of stress (e.g., work-family conflict reduction; Lapierre & Allen, 2006), and can focus on reducing the cause of stress (i.e., primary intervention) or on mitigating the consequences of stress (i.e., secondary intervention; Murphy & Sauter, 2003). Compared to the MH offerings described above (i.e., insurance, EAPs), many SMIs are delivered or primarily accessed by work agents (cf. external, MH providers).
Mindfulness-based Interventions
Mindfulness-based interventions (MBIs) involve intentionally regulating one’s attention onto the present and adopting “curiosity, openness, and acceptance” towards one’s current experiences (Bishop et al., 2004, p. 231). Many modern MBIs primarily feature meditation as a practice to foster mindfulness (Hyland et al., 2015), and most MBI research focuses on their effects for clinical/patient populations (Eby et al., 2019). New technologies are placing mindfulness resources in the pocket of employees, with apps like Headspace purporting to be a “science-backed meditation and mindfulness solution for the workplace” (Headspace.com, n.p.). Apps and other tech-driven solutions for workplace MH (e.g., Virtual Reality-based wellbeing solutions; Riches et al., 2023) merit special mention in this section, given the substantial surge in the market for these offerings (Wortham, 2021). The global rise in smart devices and connectivity, paired with an appetite for MH solutions, a commodification of mindfulness (Hyland, 2015), and the democratization of simple MH tools (e.g., MHA, n.d.) are important forces that have coincided with an almost 35% projected annual growth of the mindfulness/meditation apps market to a $7.6 billion industry by 2031 (Skyquest, 2023). We discuss a similarly tech-reliant category below, however the need for a more encompassing, flexible taxonomy stems in part from this burgeoning area of workplace MH offering.
E-Counseling & AI Therapy
An emerging addition to MH offerings is tele-health or e-counseling therapeutic services (surveys indicate ∼20% of organizations are providing them, Leonhardt, 2022). These offerings resemble conventional talk therapy, delivered by web conference technology, or on-demand text-message exchanges with a human provider (Hull et al., 2020). Very recently, a number of AI-based counseling services have also emerged, which allow people to engage in therapeutic conversations with non-human chatbots, who provide text-based responses using AI resources designed to alleviate the user’s current symptoms (Browne, 2020; Hoermann et al., 2017), through conversational tracks and techniques conventionally used by human therapists (e.g., Cognitive-Behavioral or Rogerian Therapy).
Amid the diverse landscape of workplace MH offerings, organizations face more choices than ever. The market of offerings often rolls out options faster than data that clarifies their best uses and efficacy. This increase in options occurs in the context of a general deficit in MH literacy, where most people do not possess the knowledge and beliefs to successfully navigate evaluating, implementing, or using these types of offerings (Furnham & Swami, 2018), especially in coordination or relation to the others. To help stakeholders more easily make sense of these options, despite the growing gap between available offerings and scientific evidence about their applications, we provide a framework for organizing and investigating the diverse options emerging in the market.
Proposed Taxonomy
Need for a Taxonomy
The total range of MH offerings has developed atheoretically, without specific attention to the organization or synchrony of the greater whole. Instead, a host of practical factors like legal mandates, cost models, talent management, acute need or convenience, and labor pool competition have contributed to a landscape of workplace MH offerings that continues to receive greater attention and spending. Despite investments in MH offerings, employees continue to underutilize them. For example, over 70% of employers offer and fund EAPs, but fewer than 10% of employees use them (Brooks & Ling, 2020). We cannot explain this low utilization rate, but evidence holds that MH literacy is a critical, robust antecedent of seeking and receiving MH help (Bonabi et al., 2016; Kutcher, Wei, Costa, et al., 2016). We assert that the management discipline needs to provide a better way to talk about these work-based offerings that prioritizes stakeholders’ practical needs, including their literacy gaps. A critical way to begin improving literacy, and subsequent decision-making, around these offerings is an organizing framework. Ideally, a taxonomy offers a shared, practical language among academics and practitioners, who need more guidance in the area of workplace rewards and support programs (Deadrick & Gibson, 2007; Dulebohn et al., 2009). We consider how Kirkpatrick’s (1994) four-level taxonomy for evaluating organizational training has served practitioners and academics to better understand a diverse landscape of workplace interventions intended to enhance employee capabilities and improve organizational results. Both scholars and practitioners have enjoyed this four-level framework as an effective system to discuss, study, and evaluate training interventions. With similar aims of establishing a more universal language, we propose the following taxonomy that relies on three dimensions to characterize each offering.
Dimension 1: Why? Restoring v. Enriching Mental Health
Our first dimension stems from the historical paths carved by two primary streams, and viewpoints, of MH offerings. As previously discussed, MH has often been considered the absence of mental illness (Keyes, 2002), so the resources to support it have followed similar approaches as physiological health 2 :a reactive focus on fixing dysfunctional, disordered, or deviant symptoms. It would be difficult to overstate the impact of ties between traditional models of physiological health (i.e., pathology, treatment, provider, insurance) and approaches to treating MH conditions (Hogan, 2019). In short, many MH offerings seek to address or resolve what is wrong (Anglin & Polanco-Roman, 2019). Consider a fictional employee with a mental illness (e.g., clinical depression) whose symptoms cause challenges meeting daily life demands. Conventional, modern treatments for this illness include interventions designed to restore ‘normal’ functions and behaviors, similar to an employee with a physiological condition (e.g., diabetes) receiving treatment designed to maximize ‘normal’ functions for daily life. The models—diagnosis based on symptoms, insurance/medical administrative requirements, therapeutic interventions involving pharmaceuticals, monitoring, and behavioral changes—for treating both conditions spring from a similar philosophy. Accordingly, relevant health offerings available to an employee—employer subsidized health insurance coverage for a long-term condition, fair hiring, accommodations, leave—overlap based on their common ancestry for affecting health.
A contrasting view of MH has focused on the positive symptoms of health, where one experiences good spirits, the capacity to adapt to life’s demands, and enjoys personal and social meaning (Keyes, 2002). In short, rather than health as the absence of something wrong, this viewpoint treats health as being strong (Maddux, 2008). The MH offerings aligning with this viewpoint assume everyone can benefit from MH resources, not just people with acute needs or diagnosable illnesses. Consider, for example, the physiological benefits of a healthy diet, which can serve people with illness, but enrich and bolster the health of everyone, even those without a symptom or concern. Programs like primary and secondary SMIs, MBIs, and conversation-based treatments (e.g., talk/chat therapy) can address needs, but they also prophylactically reduce needs, maximizing life’s potentials, bolstering resources and helping people to flourish in the future.
These two perspectives, and the offerings stemming from each, have shaped many of the existing offerings. Our first dimension embraces this difference and considers MH offerings along a continuum of fundamental purpose, from restorative to enriching. Restorative offerings align with the first viewpoint, principally employed to address maladies and needs (e.g., grief, substance disorders), to achieve ‘normal’ functioning. Enriching offerings align with the latter viewpoint. They do not require a problem to receive their benefit, as they functionally build strengths for the ill and well alike. Our first dimension is continuous, but observes the ends as starkly different. As an analogy, although eating well and exercising can enrich anyone’s health, when someone’s life is at critical risk, they need restorative health treatment. A gym cannot most effectively help a person address an auto-immune disorder or heart condition. In contrast, a person seeking to improve their flexibility and physical function does not need to see a medical doctor or visit an emergency room.
Organizational stakeholders, we believe, can begin making more sense of MH offerings through the fundamental distinction of the offering’s primary purpose—restore or enrich? Because many of the existing workplace MH offerings grew from these separate views of MH, this first dimension also dovetails with many people’s common understanding of these types of programs (Carvalho et al., 2022; Furnham & Swami, 2018). The models of the employer-employee relationship previously described are also important for understanding which offerings are provided and how they are perceived by employees. We expect employers likely maintain a greater obligation to provide restorative offerings, to avoid breaking the psychological contract, compared to enriching offerings (Lucero & Allen, 1994). Because the medical model was the predominant approach to addressing mental disorders for many decades, a significant number of restorative offerings align with this approach (e.g., EAPs, health insurance, ADA laws). Given their long history of being provided, most employees likely expect that organizations will support restorative MH offerings and failing to do so could be seen as a breach of the psychological contract.
Moreover, employees who need restoring (cf. enriching) offerings face harder choices in utilizing this support. For example, receiving an accommodation requires disclosing one’s mental illness, and disclosures like these carry tremendous risk of stigma and lost opportunity (Follmer et al., 2022; Follmer & Jones, 2018). Evidence indicates that people experience different levels of stigma based on the type of MH need they carry (Smith et al., 2022). Perceived organizational support plays a critical role in employees’ decisions to disclose and the long-term impacts of receiving support (Hastuti & Timming, 2021). Trust and inclusive decision-making regarding work arrangements after disclosing serious illness have been shown to improve retention among workers with disabilities (Kirk-Brown & Van Dijk, 2014), emphasizing the importance of creating a supportive organizational health climate.
We also hope this difference may increase people’s uptake by simplifying the evaluation of how each program can match their needs (Apolinário-Hagen et al., 2019), or by lowering the stigma that may be associated with treatment for more clinical needs (e.g., psychopharmaceuticals, Schomerus et al., 2019) by those who do not consider themselves ‘ill’ (Coe et al., 2021). Importantly, this continuous dimension provides flexibility for organizations evaluating and communicating these offerings. For example, some aspects of an employee assistance program (EAP) may primarily restore but others can provide some level of enrichment by introducing or relying on positive psychology techniques (Masi, 2020). This distinction allows organizations flexibility to communicate and evaluate an offering’s purpose along this continuum.
Dimension 2: Where? Internal v. External to Organization
Our second dimension considers a primary distinguishing feature prioritized by various stakeholder groups: Whether the offering is delivered by internal or external agents (i.e., who employs the delivery agents; Leong & Every, 1997). In companies, the three primary stakeholder groups previously described—employees, HR professionals, and business leaders—are increasingly encountering these MH offerings (Greenwood & Anas, 2021; Huff, 2021; Pfeffer & Williams, 2020): • Employees must make enrollment decisions and choose how to (not) use the offerings • HR professionals
3
must administer and track these offerings’ usage • Business leaders must strategically evaluate the value of and invest in each offering
Most organizational offerings and benefit programs, ranging from salary, trainings, onboarding, and insurance, live on a continuum of delivery: external or internal to the organization. For decades EAP research and practice has focused on an internal v. external distinction of these programs, similar to other organizational offerings like training. Despite promising similar fundamental purposes, training programs and EAPs delivered internally carry different costs, effects, and considerations than those delivered externally (Sung & Choi, 2014). Mental Health offerings like employee resource groups or mental illness disability accommodations are primarily delivered internally by organizational members, employees encounter and use them at work, and they require organizational staffing/policies to administer. Comparatively, the majority of therapeutic services for mental illness are delivered by an external agent, employees use them off-site and never interact with an organizational member to receive these services. Our second dimension attends to our stakeholders’ (Parmar et al., 2010) practical needs in using, administering, and evaluating these offerings.
For employees, this internal versus external distinction likely factors into their usage behaviors. Simply, employees need to know where and how they will receive these offerings to use them (Freitag & Picherit-Duthler, 2004; Wang et al., 2020). Employment with a mental illness—and choosing to utilize workplace MH offerings—also raises complex use concerns like privacy (e.g., will my coworkers, manager, employer know? Toth & Dewa, 2014), stigma (e.g., how will I be viewed using these offerings? Clement et al., 2015), and convenience (e.g., can I access this resource easily? Dawad & Hoque, 2016).
An offering that can be received completely externally without disclosure or risking crossing paths with a coworker (thus exposing needs) differs greatly from an offering delivered within the company in the presence, or with the knowledge, of other members. Here, concepts like MH climate and individual-level trust merit close attention. Disclosure requires trust that the MH need will not be used against you by your coworkers, supervisor, or company (Hastuti & Timming, 2021; Toth et al., 2022). Likely, utilizing external offerings require less trust between employees and employers. Internal offerings may be used more (cf. external offerings) in organizations where ideal levels of trust or a MH climate gives employees greater cause to receive support in the presence of their trusted coworkers. Organizations should note the implication that to maximize the utility of an internal offering will require closer attention to the trust, POS, or MH climate that employees experience. For instance, organizations that maintain a more transactional approach to employee relationship management will likely not have much success with internal delivery of MH offerings. Strategically, this distinction raises critical decisions for both companies (e.g., to attend to issues of trust/POS if providing internal offerings) and employees (i.e., to use/not use an offering based on their levels of trust and the offering’s risk of disclosure).
HR professionals and business leaders need to know the costs and customizability associated with a program or policy, where internal offerings increase both costs and customization opportunities (Sharar et al., 2013). Beyond the financial aspect, HR and organization leaders must also determine their level of internal capability to provide MH offerings. Deciding how these services can best be provided should align with the overall talent philosophy of the organization. Employee assistance programs provide a useful example to illustrate some of the trade-offs to consider when weighing an internal or external program. For instance, evidence indicates that utilization rates are higher for internal programs and that organizations have greater control over the customization and coordination of these programs; however, internally managed programs also yield greater costs for organizations (Frey et al., 2018).
The second dimension also occurs along a continuum, rather than being a pure dichotomy, as modern MH offerings generally rely at least partially on some element of both internal and external delivery agents. For instance, EAPs may be internal or external, but can also take the form of a hybrid approach whereby some elements are controlled internally by the organization (e.g., promotion of services, collection of payments for certain services) while others are managed by an external agency (e.g., delivery of counseling services). A continuum allows for a more flexible assignment of the primary delivery location (e.g., 60% internal, 70% external) than a binary categorization (i.e., internal or external).
Dimension 3: Latitude? Mandatory v. Discretionary Offering
In our final categorical distinction, we consider the influence of the laws that govern companies’ employment practices and workers’ expectations for their workplaces. A number of offerings are mandatory for employers to provide, whereas others are offered voluntarily. In the U.S., 4 workers primarily access physiological health, MH, and wellness resources through their employer (Baumgartner et al., 2020; BLS, 2022a). Employers serving as the primary access point for these resources follows from legal requirements (e.g., the Affordable Care Act), but also arises from the need to compete for talent in the labor market by providing comparable or superior offerings to other employers (NSC, 2021). Companies typically provide both types of offerings, combining mandatory offerings, like fair hiring and FMLA leave, with discretionary programs like SMIs or meditation rooms. We include this distinction in our taxonomy to help workers and managers alike know which offerings are required and which are discretionary. From the company’s perspective, mandatory offerings require priority in administering the full suite of workplace programs. Different jurisdictions mandate different offerings. For example, EAPs (Masi, 2020) and paid sick leave for mental illness (Blakey-Gray, 2024) are mandatory in some, not all, jurisdictions in the US. Precedent also indicates employers will serve as a primary route for societies to provide people the MH support they will increasingly need (SHRM, 2022; WHO, 2022). Laws dictating the support employers must offer (e.g., more inclusively equitable care for mental illness provided through insurance plans; Noguchi, 2023), merit priority in organizing and discussing these MH offerings across settings.
The distinction between mandatory and voluntary offerings is included in our taxonomy because of the importance of worker expectations. Workers carry common expectations of the environment and rewards they will encounter at work (Guzzo & Noonan, 1994). Although these expectations can differ (Pant & Venkateswaran, 2019), factors like legal requirements and the prevailing market tend to form a set of common expectations in countries, cultures, and industries (Firfiray & Mayo, 2017; Jones et al., 2014). These commonly held expectations can even result in workers feeling they have the right to certain offerings, even if companies are not legally required to provide them (Weathington & Tetrick, 2000). Expectations factor heavily into both PCT and OST perspectives of the employee-employer relationship. Workers’ expectations for the support they should receive, at minimum, can comprise the psychological contract details they hold their employers accountable to meet (Lester et al., 2001). Our taxonomy can better serve employers by helping them efficiently prioritize mandatory offerings in their decision-making, but the legal status of an offering also informs workers about the offerings to which they are entitled and can expect in a given setting (Fedorets & Shupe, 2021). When companies, regardless of their legal responsibilities, do not meet worker expectations, they risk alienating current and prospective workers, by breaking psychological contract expectations. Formal elements of the employer-employee exchange, like health insurance’s financial value or enacted accommodations or leave offering, may be easier to recognize in this contract exchange. Less obvious are the implicit expectations that workers carry, like how a supervisor supports and considers MH among their reports or management’s actual enacted values around MH (Dobson et al., 2019). Evidence indicates that the workforce, through demographics and changes in broader social attitudes, is likely expecting greater workplace support for MH issues (Belkin et al., 2019; Greenwood & Anas, 2021; NSC, 2021). So, organizations’ legal responsibilities provide a starting point and a motivation to identify and meet workers’ baseline expectations. When employers and employees share common awareness of mandatory offerings, expectations are easier to manage due to fewer subjective or personal differences (Guest & Conway, 2002). This clarity, between what is required—thus what employees are entitled to expect—and what is voluntarily offered can also support employers’ capacity to generate positive employee sentiments through providing MH offerings to employees. Employees’ awareness that their organizations are voluntarily offering something not required dramatically increases employees’ reported levels of POS (Eisenberger et al., 1997) and applicant attraction (Garcia et al., 2010). Thus, this dimension can serve to clarify use and communication of workplace MH offerings, while attending to the risk of unmet psychological contract expectations or maximizing the positive impact of exceeding expectations.
In Figure 1 we demonstrate how this taxonomy can be used to better display and organize an example organization’s collection of MH offerings. Compared to the full list of 11 common MH offerings, we believe the taxonomy-organized presentation of offerings dramatically improves understanding and comparison for stakeholders. Organizational leaders and HR professionals can populate a blank version of this Figure, based on the MH offerings in their companies, even issuing new versions annually as offerings/vendors change. The graphic provides a coherent way of initially considering these offerings, but the taxonomy’s dimensions offer more robust, long-term value in strategy and education for organizational stakeholders. Taxonomy of workplace mental health offerings.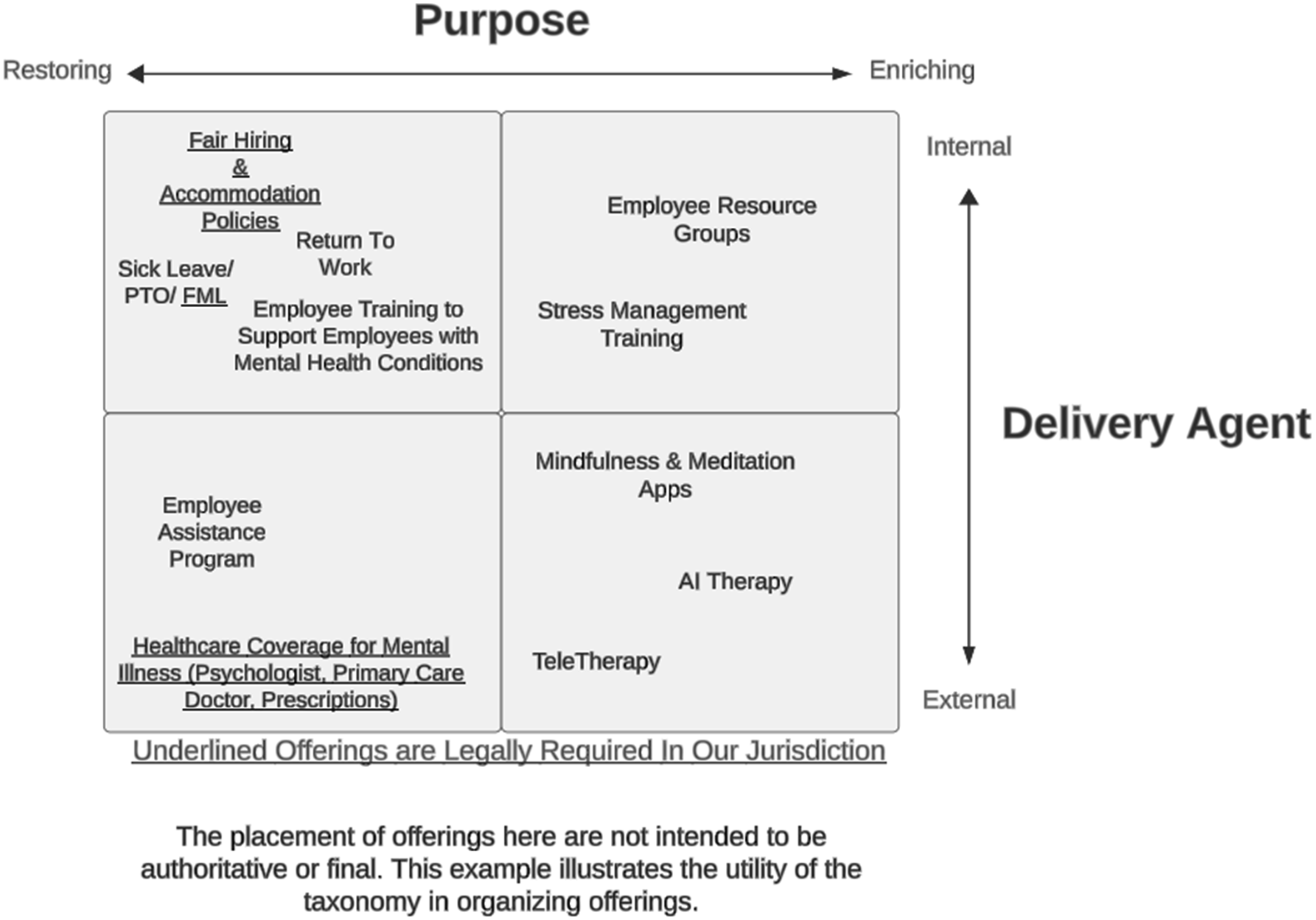
Future Research Directions
Evidence implies companies and employees will increasingly embrace, expect, and spend on MH. Previous researchers have addressed topics of mental illness and health at work (Follmer & Jones, 2018; Kelloway et al., 2023; Rosado-Solomon et al., 2023). These important foundations provide scholars and practitioners guidance on these constructs and the models for supporting employees’ MH. However, the primary mechanisms for this support—the offerings purpose-designed to affect employee MH—have, like most other benefits (Deadrick & Gibson, 2007; Dulebohn et al., 2009; Fulmer & Li, 2022), received little attention from scholars. Organizational stakeholders need more help understanding these offerings (Amwell, 2023; SHRM, 2022), perhaps because of low MH literacy rates (Furnham & Swami, 2018) and persistent stigma surrounding MH (Parcesepe & Cabassa, 2013) that affect how all people, not just employees, engage with MH support. As an initial attempt to provide this guidance, we developed this taxonomy by prioritizing organizational stakeholders’ needs and considering the foundations offered by social exchange theories and trust literature. We believe organizational scholarship can indirectly contribute to addressing the MH crisis (White House, 2022) by increasing the uptake and impact of these workplace MH offerings. Beyond our taxonomy’s primary contribution to simplify and standardize the full landscape of these offerings, we hope researchers can develop the guidance available to companies by tackling two research areas offering great promise for informing the people we serve.
Research Area 1: Clarifying the Prevalence, Costs, and Outcomes of Workplace MH Offerings
Beyond survey results published by commercial groups (e.g., Ginger, 2022; Kaiser Family Foundation, 2021; PWC, 2021), most organizations can access very little information on workplace MH offerings’ prevalence, costs, or outcomes. For example, a company considering offering employees a mindfulness-based app or e-counseling subsidies cannot obtain objective details on (1) normative adoption rates of these offerings, (2) the typical cost of these services, or (3) the effects of these offerings, especially in conjunction with other offerings or as part of a total rewards package (Fulmer & Li, 2022). A common complication limiting available research is the sometimes-loose terminology used by popular sources to name and discuss offerings. Hopefully, our taxonomy can begin standardizing discussions and reduce this problem. Building on the flexible coherence and totality of our taxonomy, researchers can provide leaders and HR professionals better data on these offerings. We do not think research should supplant or compete with commercial sources, but scholars can complement such efforts to use a common language where stakeholders can fairly compare information between offerings, using the same names and promising similar benefits.
First, researchers should better document the prevalence of these offerings in workplaces. They should capture the rates of employers providing a given offering and the rates at which employees use each offering. EAPs provide an ideal, well-documented example, such that estimates establish that 70%–90% of employers offer EAPs (Agovino, 2019). However, even though EAPs typically pose no additional costs to employees to use, fewer than 10% of employees use them annually (Brooks & Ling, 2020). Take for example the confusing case of workplace SMIs. Estimates indicate 20%–50% of companies offer these programs (Business Group on Health, 2020; Linnan et al., 2019), yet only about half of polled employers are even aware of SMIs (Molek-Winiarska & Molek-Kozakowska, 2020), which have existed for nearly 50 years (Murphy, 1996). In a single poll, only 15% of workers reported awareness of their employers’ SMI offerings; of those aware, only 23% (3% total) of workers use their workplace SMIs, and 32% of these polled workers wanted more MH offerings from their companies (Business Group on Health, 2022). How can a business leader make a rational strategy investing in SMI offerings to respond to the one-third of employees wanting more support, based on this confusing picture of the availability and impact of these offerings in the workforce? This evidence could justify an employer’s reticence to invest in an SMI for employees, because most other companies are not offering them and most employees do not know about them or use them.
Despite company leaders repeatedly hearing about the urgent need to invest in MH offerings to meet employees’ need for support (Minemyer, 2022; SHRM, 2022), no clear information can guide them to know what the ‘typical’ offerings are and the extent to which employees use them. Establishing the prevalence of these offerings’ availability and use also may relate to expectations relevant to PCT considerations and usage. Namely, workers whose employers offer a benefit tend to place more importance on the benefit (Horowitz & Parker, 2023), so establishing the availability rates of each offering can reveal more about the types of offerings employees may expect in a psychological contract sense.
Credible prevalence rates can also help employers identify how their choice to (not) provide and support a given offering may differentiate them regarding employee attraction and retention. When organizations provide an offering, they send signals to current and prospective employees about their values or climate (Valcour et al., 2011). But workplaces must practice what they preach in supporting MH, and companies can sometimes formally proffer a new MH offering without enacted support (i.e., managers neglecting MH issues, employees facing difficulty accessing MH offerings). These kinds of hollow gestures also send signals (Klimchak et al., 2020) that likely affect not just employee-employer relations, but employees’ usage rates, via constructs like MH climate, trust, or POS (Kelloway et al., 2023; Zhang et al., 2012). For instance, employees who perceive greater levels of POS and trust may be more likely to take advantage of MH offerings whereas employees who have more transactional relationships with their employers may worry about stigma and backlash for engaging with these offerings. A fuller look at not just the availability of offerings, but each offerings’ rate of usage can reveal more about the gaps between the formal offerings available and employees’ actual behaviors. These gaps have emerged among employees skeptical and underwhelmed by the realities of receiving workplace MH support (Adams et al., 2021; Deloitte, 2022; Ginger, 2022). Researchers should also attend closely to how factors like race, gender, socioeconomic status, and industry affect prevalence rates, because many benefit programs can differ in availability as a function of demographic or vocational differences (Horowitz & Parker, 2023).
Descriptive research efforts would also include capturing the costs, according to payors, of each offering. Organizations spend about 30% of their personnel costs on benefits (BLS, 2022b), and thousands on each employee’s health and wellness offerings. Our taxonomy offers the chance to better itemize, across all workplace MH offerings, the costs each company is incurring. Currently, many of the costs of workplace MH offerings are lumped in with other costs (i.e., health insurance for physiological needs), or not provided at all. Companies, then, cannot objectively quantify or establish ‘normal ranges’ of all the costs for supporting employee MH (Gurchiek, 2017; Job Action Network, 2020). These data ambiguities may be even greater for offerings like accommodations, fair hiring, and adaptations (Barclay & Markel, 2009; Dimoff & Kelloway, 2019). Business leaders need accurate information to strategically fund MH offerings for their companies. HR professionals need accurate data to evaluate the effectiveness and efficiencies of these offerings. These estimates also matter to employees, where offerings’ value can influence decisions on job searches and benefit enrollment, or weighting equity calculations (Kollman et al., 2020).
Researchers should also prioritize capturing both personal and work-related outcomes related to each offering. Some outcomes are clearly established (e.g., stress reduction programs affect employee stress levels; Richardson & Rothstein, 2008) but scholars should be compelled to inductively consider a greater set of outcomes, because of the increasing adoption and need for MH offerings (APA, 2021, 2022; CDC.gov, Minemyer, 2022). Identifying outcomes should begin with the three major stakeholder groups—organizational leaders, HR professionals, and workers—we have repeatedly focused on in developing our taxonomy. Scholars, then, should uncover more outcomes relevant to each group, such as: (1) the criteria leaders use to evaluate offerings and how they demonstrate their support/opposition for an organizational offering, (2) the ease of administering and educating employees on an offering, also the constraints related to counseling on offerings, (3) employees’ perceptions of an offering as part of total rewards and the perceived safety of accessing it. We have mostly focused on these offerings’ benefits, although they may include negative outcomes beyond financial costs. However, establishing the fuller range of outcomes (e.g., Livingston et al., 2022) first will facilitate a more complete examination of their effects. The flexibility of our taxonomy, then, can direct consideration of the fuller landscape of offerings.
Documenting the normative costs, availability, and utilization of offerings is crucial for a comprehensive understanding of their impact within the employer-employee exchange relationship (Lucero & Allen, 1994). Workers and job-seekers expect the more typical, mandatory offerings (e.g., health insurance), and lacking access to those offerings (cf. exceptional, voluntary offerings) can trigger reactions akin to breaches in the psychological contract (Rousseau, 2004). Moreover, a higher-cost offering, although more burdensome for the employer, might engender stronger feelings of POS, as workers may attribute their company’s substantial investment in employee health to a genuine concern for their value (Rhoades & Eisenberger, 2002). Lacking details about the availability and customary expenses associated with these offerings hinders the ability to anticipate workers’ expectations and their levels of POS. Documenting the typical costs and benefits can also help employers assess their investments, balancing an offering’s financial costs against the costs of perceived contract breaches (e.g., withdrawal, turnover; Zhao et al., 2007) and the benefits the offering can provide not only for employees’ MH but their levels of POS. Systematically capturing the prevalence and benefits of these offerings, particularly from the workers’ perspective, is instrumental in establishing the normative expectations that workers hold regarding such support programs. Instances abound where workers have expressed the belief that their employers could do more to bolster their MH, a viewpoint often misaligned with leaders’ sentiments, wherein employers believe they are already providing sufficient resources (Deloitte, 2022; Ginger, 2022). The absence of a broader quantitative description of these offerings makes it difficult to know what is ‘normal’ to expect, from both employers’ and workers’ perspectives, in supporting MH.
Research Area 2: Identifying Helpers and Hurdles to Using MH Offerings
Companies have been escalating their investment in MH offerings for workers. However, evidence clearly reveals workers often are not using these offerings (Brooks & Ling, 2020; Lewis, 2022) or not trusting their employers’ intentions in providing them (Adams et al., 2021; Deloitte, 2022). Available signs point to continued growth in spending on and need for workplace MH offerings. Scholars, then, can help these investments better meet these needs by identifying the factors that (1) limit workers’ using and (2) foster workers’ using the MH offerings in their workplaces.
A majority of people do not fully use many of their available workplace offerings, and researchers have provided a limited amount of evidence to explain why (e.g., Kuykendall et al., 2021). Polling information on benefits can provide some initial ideas. For example, 35% of polled American workers do not understand their benefits (Voya, 2021). Of the roughly 46%–55% of Americans who do not use all the vacation time (U.S. Travel International Employee Assistance Professionals Association, n.d.) to which they are entitled (Paid Time Off (PTO)), workers indicated reasons like worrying about falling behind, displacing load onto coworkers, hurting their own chances for advancement or keeping their job, or a manager who discourages using the PTO they are entitled to (Horowitz & Parker, 2023). With a domain like MH support, workers’ reasons for not using their available offerings are likely more complex. These may include misunderstanding (Danehower & Lust, 1996), lack of MH literacy (Furnham & Swami, 2018), workplace stigma around MH (Follmer & Jones, 2018), and administrative issues with requesting accommodations (McDowell & Fossey, 2015). Privacy concerns deter many employees from using organizational offerings that imply they are anything less than well (Perrault et al., 2020). Research evidence indicates increasing people’s MH literacy (Bonabi et al., 2016), and reducing related stigma can each improve usage rates for mental resources (Lipson et al., 2019) among general populations. The areas of workplace mental literacy and stigma, then, offer great promise to organizational researchers too. We believe employee trust, POS, and the nascent construct of a MH climate, deserve high priority in research examining why employees do not use their workplace MH offerings (Toth & Dewa, 2014). For example, evidence exists that employees participate more in wellness programs in the presence of a supportive workplace health climate (Tringali et al., 2022) and that supervisor-subordinate trust is a key to positive employment relationships and outcomes (Skiba & Wildman, 2019). In addition to their broader competence, the efficacy of HR professionals in administering and communicating these offerings likely plays a role in employees’ trust in using these offerings (Klimchak et al., 2020). Many employees do not use or enroll in a program because they do not know about it, do not understand its relevance to their needs, or do not know how to navigate/use the system (Harkin Institute, 2018) and this education gap may be growing among younger workers (Voya, 2021). Beyond looking at trust in organization and supervisors, then, researchers can empirically describe when (e.g., onboarding) and how (e.g., methods of messaging) to best communicate the company’s MH offerings to employees.
Line-level, direct managers critically impact the successful implementation of all types of employment practices that may originate with an HR professional. However, managers substantially enable or undermine most strategic HR policies and practices (Kuvaas et al., 2014; Purcell & Hutchinson, 2007; Trullen et al., 2016). Hence, even the best-designed and communicated workplace offerings rely greatly on workers’ trust in their supervisors, especially when the employee risks disclosing a MH need (Purcell & Hutchinson, 2007; Triana et al., 2021). As researchers describe and prescribe how HR professionals can best educate employees and managers on workplace MH offerings, they should also consider the information flowing back to HR professionals. This may include how HR professionals evaluate their companies’ workplace MH offerings’ effects, or how these professionals coordinate with line-level managers to implement policies and practices related to MH at work. We hope our taxonomy’s distinctions makes these considerations easier to organize and discuss for HR professionals, through a common framework for discussing a given offering.
Finally, researchers should study how leaders hinder and help employees in using workplace MH offerings. Leaders ultimately decide how much to spend on these offerings and they bear ultimate responsibility in the company’s work to foster or undermine these offerings’ legitimacy. For example, employees are more likely to use formal work-family benefits when their organizations foster a supportive work-family culture (Thompson et al., 1999) primarily through mechanisms like leaders’ behaviors (Kailasapathy & Jayakody, 2018; Wang & Walumbwa, 2007). Recent, prominent examples of high-profile figures who have admitted their need for MH support (Hauff & Powell, 2022) reveal the power that leaders can have when they model MH behaviors. Given the increased demands of leadership and a growing focus on leaders’ MH (Barling & Cloutier, 2017), the nexus of workplace MH offerings and leadership seems generative for identifying how the volume of organizations’ investment in MH can produce greater impact.
Conclusion
The need for and spending on workplace MH offerings are growing, and appear poised to assume a more prominent role in workplaces. Organizational scholars, especially those with backgrounds in psychology and social sciences, can seize this unique opportunity to improve the effectiveness of these offerings, both in awareness/acceptance and uptake/outcomes. Although issues like stigma and MH illiteracy (Furnham & Swami, 2018; Moll et al., 2017) will likely continue to present challenges for workplaces and employees pondering these workplace MH offerings, organization scholars can help to meet the growing appetite and expenditure for these resources by helping our consumers make better sense of these offerings. As societal-level MH crises loom (White House, 2022), workplaces will likely serve as the primary access point for people seeking resources to address their, or their families’, MH. Therefore, providing practical, clear guidance on how to maximize these offering’s accessibility and impact at work should be a scholarly priority. The current research offers an initial catalyst for this conversation. By approaching these offerings with theoretical lenses that consider how relevant stakeholders contemplate these resources—as funders, evaluators, administrators, users—and providing an inclusive means of organizing the entire landscape of these offerings, we hope to lend clarity to an often atheoretical domain.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Associate Editor: Jonathan Pinto