
Abstract
The financial cost to workplaces associated with mental health conditions is considerable. Consequently, this article explores the last two decades of Australian data pertaining to work-related psychological injuries, work capacity and benefit/compensation pathways. The presented data highlights the increasing costs and duration of mental health-related workers’ compensation claims, indicating a steady intensification of the complexity or severity of psychological injury claims. Equally, psychiatric conditions form the largest proportion of longer-term incapacity benefits received in the working population. This article then considers why there has not been reduction in rates of work-related psychological injury, and moreover, why are workers who functional recovery appears to be worsening in recent years. Firstly, despite regulatory reform, there is little practical direction available to guide preventative change, as such, establishing an evidence base for effective tools to mitigate workplace psychosocial hazards is critical. Secondly, an increased focus on workers who are already unwell is urgently needed. Multi-component work interventions, upskilling managers, and rehabilitation-focused treatments have demonstrated effectiveness and require considered implementation. Finally, at a policy level, it is important to redress aspects of the Workers’ Compensation Scheme that may be impeding recovery.
Keywords
Mental health conditions are the leading cause of long-term disability worldwide (World Health Organization, 2017). In addition to the substantial personal consequences, the annual national cost to the Australian economy is estimated at AUD$70 billion (Productivity Commission, 2020). More than half of this cost, AUD$39 billion, is attributed to lower economic participation and loss of productivity (Productivity Commission, 2020), highlighting the link between mental ill-health and loss of human capital. However, national trends both in true prevalence rates and functional sequelae remain contentious, as does the role of workplaces in addressing this issue (Harvey et al., 2017b). Additionally, greater focus on mental health and mental health awareness has occurred in most developed countries, but the impact of this increased attention on population health remains unclear. The most recent data from the latest wave of the National Mental Health and Wellbeing Study indicated that 21.5% of Australian adults had a 12-month mental disorder (Australian Bureau of Statistics, 2023a), consistent with findings from the 2007 survey (Australian Bureau of Statistics, 2008), with slight increases in 12-month anxiety and affective disorders. While it is overly simplistic to merely compare prevalence rates, such data suggests no discernible positive impact of mental health awareness in lieu of implementing solutions. Similarly, occupational disability associated with mental illness has continued to rise even where population prevalence appears relatively stable (Harvey et al., 2017a).
Over recent years there has been an increased focus on workplace mental health in Australia and internationally. Work health and safety laws have been strengthened to focus on psychosocial hazards (aspects of work which have the potential to cause psychological or physical harm) and large-scale national promotional programmes encouraging workplaces to do more to support employee mental health have been rolled out (Safe Work Australia, 2022). Given this rapidly changing landscape, it is important to continue to explore and describe the prevalence and patterns of work-related psychological injuries, work capacity and impairment and benefit/compensation payment pathways. Within Australia, two key indicators need to be examined: (1) mental health-related workers’ compensation claims for psychological injury and (2) longer-term incapacity benefits received (Disability Support Pension, DSP).
Workers’ compensation claims
Current workers’ compensation laws in Australia differ by jurisdiction regarding the contribution played by work in the injury, however, in most schemes, a compensable injury is defined as one arising out of, or in the course of employment, many schemes qualify this for diseases (including psychological illness) by specifying that employment must be a (or in some cases, the) main or major contributing factor (Safe Work Australia, 2021; Safe Work Australia, 2010). The rates of approved workers’ compensation claims, therefore, provide an indication of trends in work-related mental health conditions. There are two main metrics captured in national data regarding workers’ compensation claims: (1) the number of claims accepted and (2) the time taken for workers to recover. An important caveat here is the consideration that different jurisdictions use different indicators to determine recovery. In many cases the end of the claim, or cessation of payments is not a true indicator of recovery. Between 2001 and 2021, the absolute number of claims for mental health conditions increased by 84% (6607 to 12,155) and accounted for over 70% of all disease-related claims in 2021 (Safe Work Australia, 2022). Conversely, the absolute number of claims for all other disease types decreased over the same period. However, considering the Australian population has grown over that same 20-year period (Australian Bureau of Statistics, 2023b), a more appropriate way to measure the trends of work-related mental ill-health is to examine the number of accepted claims per 1000 workers. This standardised trend is illustrated in Figure 1 which suggests a fluctuation over time but no overt increase in incidence rates of mental health-related claims over the entire 20-year period. Differences in reporting between early (2001–2006) and later years (2007–2021) mean direct comparison can only be made from 2007, when considering this adjustment we see a recent increase in claims within the last decade. Furthermore, and perhaps more concerning is the steady increase in median working weeks lost per claim (illustrated on the second y-axis of Figure 1). Median time taken off work for paid mental health-related claims increased by 175% between 2001 (11.2 working weeks) and 2020 (30.8 working weeks), comprising the highest amount of time lost compared to all health conditions in recent years (2014–2020). Correspondingly, mental health-related claims have also been associated with the greatest median costs over recent years, increasing by 288% between 2001 and 2020 (Safe Work Australia, 2022).
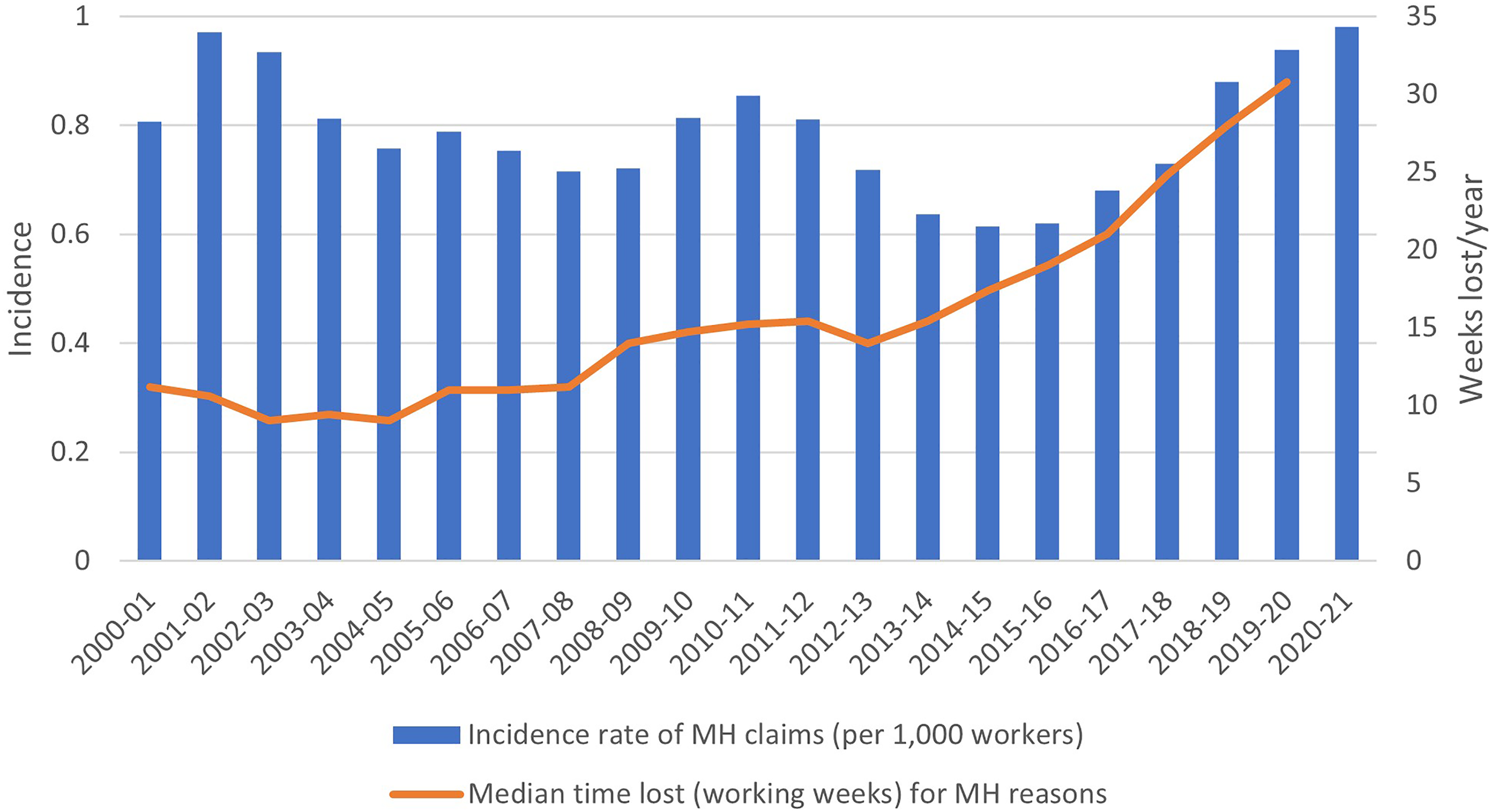
Rates of workers' compensation claims for mental health conditions per 1000 workers and median working weeks lost per year for mental health reasons (2001–2021*). Note: *Due to differences in reporting, data from 2001 to 2006 and 2007 to 2021 are not directly comparable. Most recent data sources were utilised where available, due to changes in accepted claims over time. 2021 data is considered preliminary. Data sources: Years 2001, 2016–2021 (Safe Work Australia, 2022); 2006 (Safe Work Australia, 2013a); 2007 (Safe Work Australia, 2013b); 2008 (Safe Work Australia, 2014); 2009 (Safe Work Australia, 2015a); 2010 (Safe Work Australia, 2015b); 2011 (Safe Work Australia, 2018a); 2012 (Safe Work Australia, 2018b); 2013 (Safe Work Australia, 2020a); 2014 (Safe Work Australia, 2020b); 2015 (Safe Work Australia, 2021). Incidence data 2002–2005 (Safe Work Australia, 2013a); Time data: 2002 (Australian Safety and Compensation Council, 2009); 2003 (Safe Work Australia, 2012); 2004 (Safe Work Australia, 2010); 2005 (Safe Work Australia, 2012).
These figures suggest that, while the overall occurrence of mental health-related compensation claims may have risen in line with the Australian working population over the same period, the severity and complexity of work-related mental health conditions appears to have intensified, with early recovery and return-to-work (RTW) becoming increasingly less likely. The most commonly reported sub-category of mental stress claims in Australia is work-related harassment and/or bullying (n = 2280; 2.6 per 10,000 employees), followed by work pressure (n = 2075; 2.3 per 10,000 employees) and workplace violence (n = 1130; 1.3 per 10,000 employees) (Safe Work Australia, 2021). Data reported by Safe Work Australia shows that rates of claims for harassment and/or bullying in Australian workplaces have steadily increased, from 6.6 claims per 100 million hours worked in 2002–2003 to 17.5 per 100 million hours worked in 2018–2019 conditions (Safe Work Australia, 2020). Furthermore, female workers have been more than twice as likely to submit claims relating to harassment, bullying or exposure to workplace violence compared to males (Safe Work Australia, 2020). These claim types reflect not only key psychosocial hazards that need to be addressed but highlight the significant impact of interpersonal hazards and hazards that are neither inherent to job roles (e.g., trauma exposure) nor the result of mere inattention (e.g., poor support or role clarity) and which should be eliminated.
Disability support pension
The DSP is Australia's primary benefit for individuals with long-term disabling conditions that inhibit their capacity to work (i.e., are unable to work at least 15 hours a week over a 2-year period) (Services Australia, 2023). In mid-2023, more than 245,000 people aged 16–64 years were receiving a DSP for a mental health condition, compared to just under 141,000 in 2001. These figures in isolation, however, can be misleading, given the overall proportion of the population receiving a DSP for any reason has decreased over time (Australian Institute of Health and Welfare, 2022), particularly after 2012 (Collie et al., 2022). This was partly due to various policy changes aimed at restricting access to the DSP (Australian Institute of Health and Welfare, 2022; Collie et al., 2022). The broad DSP restrictions were accompanied by a substantial increase in the proportion of working-age population accessing an alternative, albeit lower rate of incapacity benefit, through the Newstart Allowance (now called JobSeeker Payment). However, it is noteworthy to consider that mental health conditions surpassed musculoskeletal/connective tissue conditions as the most common reason for DSP payments in 2011 (Department of Social Services, 2013). Furthermore, among those receiving DSP benefits, the proportion of recipients claiming for a mental health condition has steadily increased by 76.7% (22.6% to 39.9%) from 2001 to 2023 (Australian Department of Social Services, 2023; Department of Social Services, 2013).
Figure 2 illustrates that, when considering DSP rates as a proportion of the working-age population, DSP rates specifically for mental health conditions increased considerably between 2001 and 2014 and then declined slightly between 2015 and 2018, although at a slower rate compared to most other medical conditions (Australian Department of Social Services, 2023; Collie et al., 2022; Department of Social Services, 2013). Since 2018, DSP rates for mental health conditions appear to have stabilised, however, these rates remain highest across all medical conditions. These changes coincided with a substantial increase in rates of people receiving the Newstart allowance due to mental health conditions (Australian Department of Social Services, 2023).
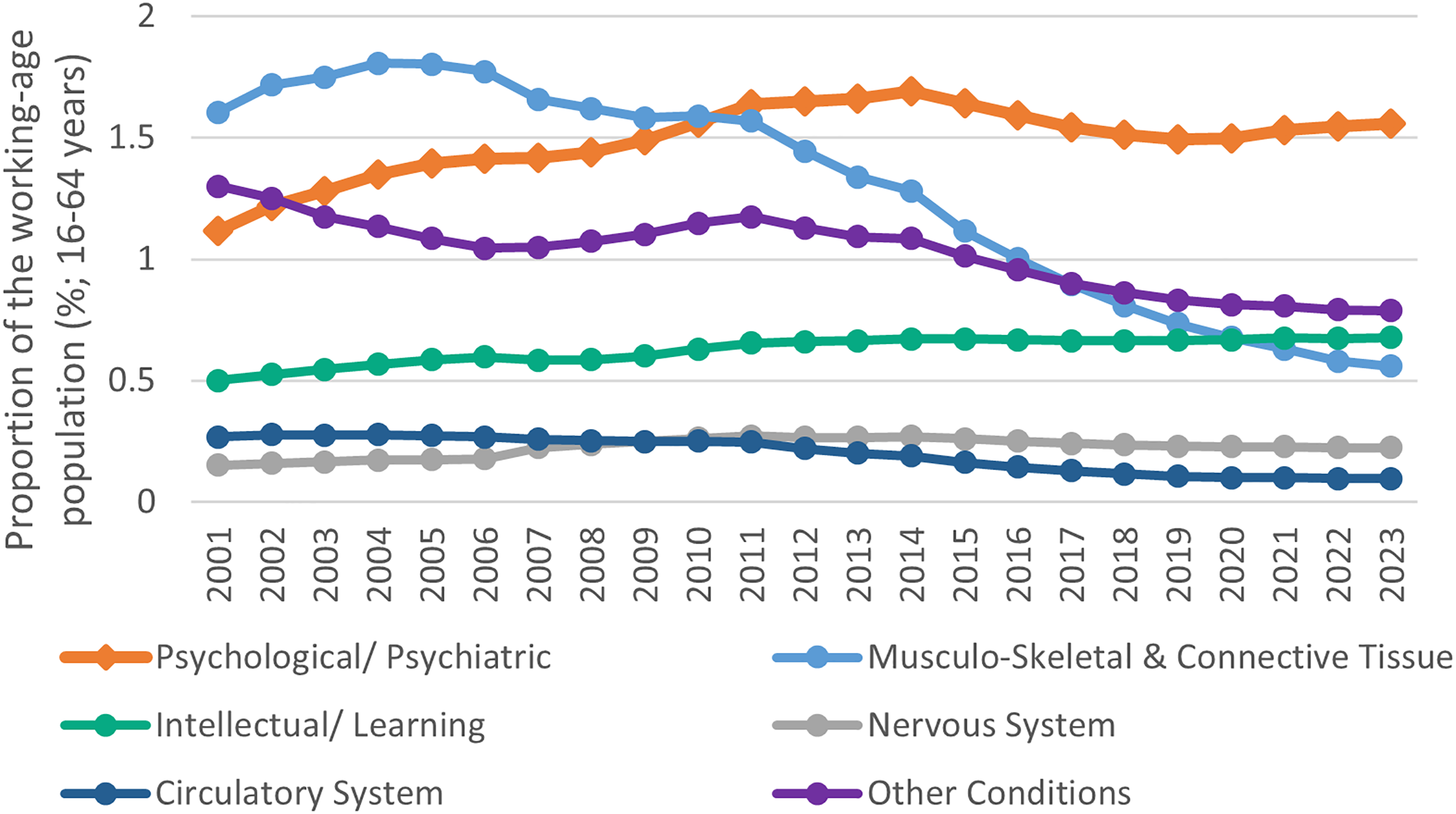
DSP recipients by top 5/other medical conditions as a proportion of the working-age population (16–64 years) between 2001 and 2023. Note: All annual population data reflects June figures. DSP data reflects most recently reported figures: September (2023), December (2015–2022), June (2001–2014). Data sources: Department of Social Services (Department of Social Services, 2013, Australian Department of Social Services, 2023, Australian Department of Social Services, 2014); Australian Bureau of Statistics (Australian Bureau of Statistics, 2023a, 2023b). DSP: Disability Support Pension.
Where are we now?
Taken together these data suggest that although historically, the major cause for workplace incapacity in Australia was musculoskeletal and connective tissue injuries, mental health issues are now not only an ongoing major cause of sustained functional impairment, but perceptions of work and work stress continue to be a major driver of this incapacity (Safe Work Australia, 2021). Although rates and impairment associated physical injury appear to be declining, the opposite is true for mental health conditions, with an increasing number of people remaining out of work following a serious injury or illness of this kind.
These findings raise two important questions. Firstly, why have we not been more successful in reducing the rates of work-related psychological injury? Specifically, why have mental health initiatives and policies not been able to emulate the success seen in workplace physical safety? Secondly, why are workers who develop a mental illness experiencing worse functional recovery outcomes now compared to 10 years ago? How and why is our increasingly expensive and intensive workers’ compensation system leading to slower and poorer recovery for workers? We will consider each of these issues in turn.
Why are rates of work-related psychological injury not reducing?
The steady reduction in rates of physical injury in the workplace should be viewed as a major public health success. In particular, it is reasonable to assume that much of the decline in musculoskeletal and connective tissue injury claims may indicate increases in workplace physical safety regulations and reduced risk exposures (Oakman et al., 2019), as there is little evidence that increasing awareness or implementing manual-handling training programmes have had a beneficial impact (Martimo et al., 2008). This raises the important question of what is the mental health equivalent of physical safety regulations?
Over recent decades there has been a procession of regulatory changes and guidance interventions to try and reduce the level of psychosocial hazards in the workplace. To illustrate this, we plotted the progression of major workplace mental health initiatives in Australia over the past 20 years in Figure 3. Whilst this list of initiatives is not exhaustive, it is evident that there has been an increased focus on workplace mental health and particularly on preventing psychological injury by reducing work-related risk factors. The most recent, and arguably the most important, of these changes has been the implementation of new work health and safety legislations in most states and territories that now mandate workplaces to manage psychosocial risks and implement control measures to eliminate (or minimise) psychosocial risks so far as is reasonably practicable (Australian Parliamentary Counsel’s Committee, 2023). Despite progressive changes culminating in the new legislation, the best available data shows that, to date, only 7% of Australian workplaces have integrated sustainable practices aimed at promoting employee wellbeing and mental health (Safe Work NSW, 2020). Most workplaces were within the ‘limited actions’ category, which is denoted by an incident-driven response to mental health problems, or the ‘intention category’ with limited psychosocial support services (Safe Work NSW, 2020). Overall, this increased national attention and intention, with little discernible impact, draw parallels with the suicide prevention space (Jorm, 2019), and warrant equivalent consideration.
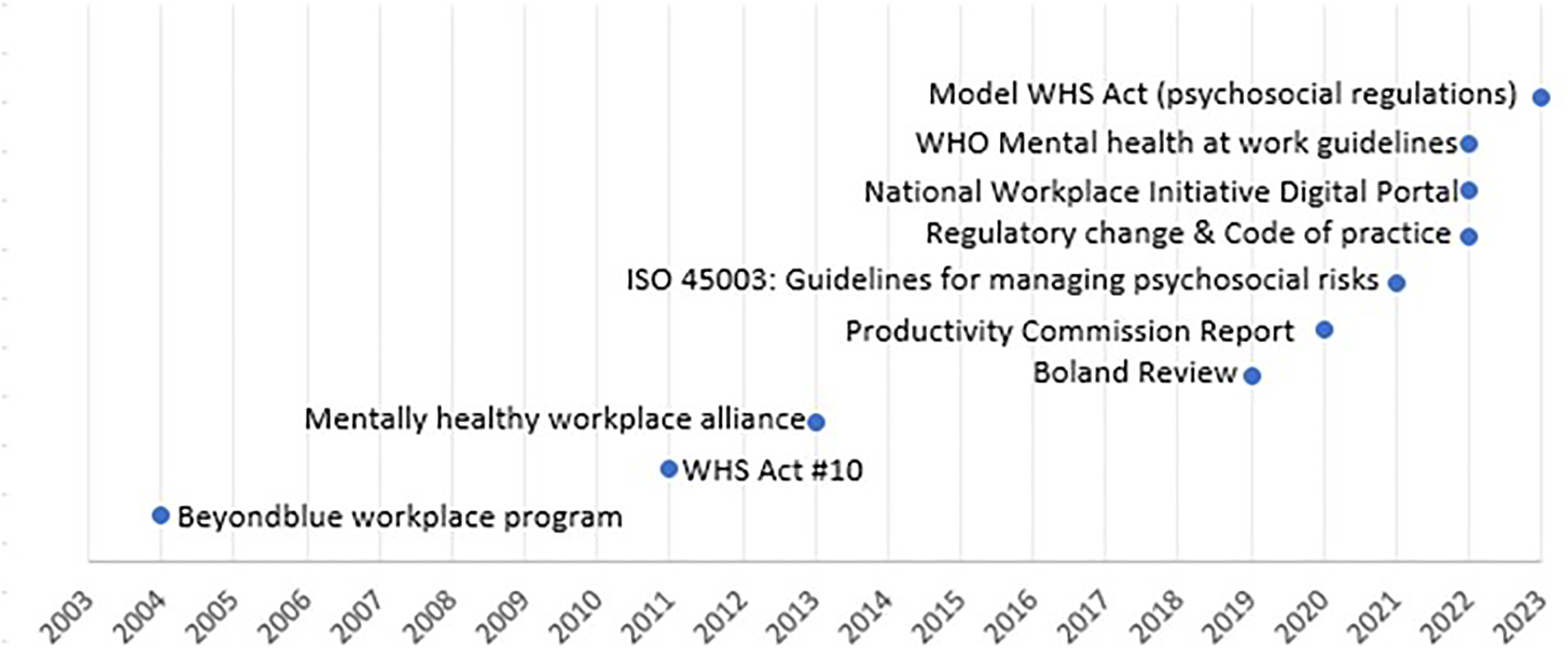
Major workplace mental health initiatives in Australia 2003–2023.
A key issue that has delayed wider implementation (and potentially effect) of prevention practices in workplaces has been that psychosocial risk factors are much more complex than physical risks. Such factors are difficult to measure and rarely have a simple cut-off where a challenge within the working environment becomes a risk (e.g., job demands). Furthermore, risk itself is not static across all individuals or even within individuals and factors which may be harmful at one point in time or for some individuals may not for others or may in fact be desirable (e.g., remote work). Perhaps even more challenging is that, although we have ample evidence of the risk associated with various work factors (Harvey et al., 2017b), we have limited evidence of how to manage these factors and even less evidence around whether these reductions will lead to a reduced rate of work-related psychological injury (World Health Organization, 2022). Such concerns should not be viewed as academic handwringing. Policies focused on raising awareness about mental health are not without risks and are, in isolation, insufficient (Wessely et al., 2008). There is an urgent need to develop and test workplace interventions aimed at reducing psychosocial hazards. Without this evidence base we cannot provide employers or policy makers with sound advice.
Why are workers not recovering?
The most striking aspect of the presented data is how over the last decade, rates of recovery from work-related mental ill-health have slowed dramatically. This is problematic as not only is long-term sickness absence a predictor of poor future physical and mental health, and reduced work capacity (Gustafsson and Marklund, 2011), but longer absenteeism is associated with a reduced probability of eventual RTW and subsequent economic and social deprivation (Henderson et al., 2005). The median time taken off work for a mental health-related claim is now over 6 months, more than double that of 10 years prior. This is despite improvements in mental health treatment, new models of recovery-focused care and a shift towards earlier intervention (e.g., Malhi et al., 2021). Considering the majority of claims in this space are for conditions such as depression, anxiety and posttraumatic stress disorder, for which effective evidence-based treatment is available the rates of recovery captured in these figures cannot be accepted. These trends demand that we look in detail at our Workers’ Compensation Scheme and examine why it is not promoting faster recoveries for affected workers. Some potential mechanisms of failure may relate to comorbidity, as this is known to complicate recovery, or where conditions occur subsequent to the compensable condition, they may not be funded (Franche et al., 2009; Kilgour et al., 2015a). Similarly, there is evidence to show that among workers with accepted compensation claims a variety of factors (being off work, poor general health, low work ability, financial stress, stressful interactions with healthcare providers) are associated with the highest levels of psychological distress, suggesting a complex clinical profile (Collie et al., 2020). There is also overwhelming evidence that suggests that rather than fostering recovery of injured workers, the claims process is often implicated in negative outcomes. A recent review of 27 studies on experiences of injured workers found that the majority of interactions were negative and resulted in considerable psychosocial harm (Kilgour et al., 2015b). Relatedly, issues with healthcare providers are a potential driver. Gray and Collie (2020) report that among workers claiming for mental illness, those who experienced healthcare accessibility issues, saw multiple providers and had psychological or financial stress, were significantly more likely to experience stressful healthcare provider interactions and these stressful interactions were associated with reduced rates of RTW. There may also be specific failures at the workplace and systems level that play a role in delayed RTW. Holley et al. (2015) argue that in many cases instead of support, work adjustment, and reintegration, injured workers often face a culture of hostility and stigmatisation by employers and other stakeholders, along with legislative restrictions placed on payment of medical expenses. It is likely that a combination of financial and systemic stressors inherent to the claims process, workplace and the healthcare system may play a critical role in this protracted recovery. Sadly, even after claim finalisation evidence shows injured workers have significantly poorer outcomes than those not injured, including unstable work status, and increased risk of reinjury, ongoing symptoms, chronic health conditions, and mortality (Weir et al., 2024).
Future work and worker-focused interventions
Although the nature of psychosocial risk is multifaceted (Potter et al., 2019), these data provide clues as to where action (be it, research, policy, or implementation) is required. It is possible that the changes in mental ill-health rates/complexity inferred in this article may reflect other underlying factors rather than true severity. For instance, decrease in stigma might have increased the acceptability of reporting psychological injury, either as new cases or a shift in the way workers report it (previous physical ailments may more accurately be reported as psychological in origin after reduction in stigma concerns). Nonetheless, it is evident that appropriate mental health care intervention(s) are now more urgently needed than ever, and a number of important directions are apparent for both protecting workers from workplace hazards and responding effectively when they become unwell.
At the prevention end of the spectrum, considering the major causes of work-related mental stress include work pressure, work-related harassment and/or bullying and workplace violence, developing an evidence-base for effective intervention across these areas is critical. While the idea of ‘work pressure’ is often ill-defined, complex, and falls on a subjective spectrum (whereby both low and high levels can be problematic), work harassment, bullying and violence, are indisputable hazards requiring elimination (Boudrias et al., 2021; Dworkin, 2020). At a policy level, the 2022 amendment to Australia's Sexual Discrimination Act to introduce a positive duty on all employers to take reasonable and proportionate measures to eliminate gender-based discrimination, sexual harassment and victimisation is an important step and with the net benefit flow-on effect on psychological work, health and safety outcomes for employees nationwide yet to be known (Jenkins, 2020). Bullying has proved to be a difficult area to establish efficacious interventions. A notable Cochrane review (Gillen et al., 2017) found only five randomised controlled trials in the area, with little or no change found, especially in co-worker bullying. More work is needed in this important area, as it is for developing interventions targeting other key psychosocial work hazards.
The available data suggests that an increased focus on workers who are already mentally unwell is urgently needed. We suggest three key areas where attention is necessary. Firstly, in the workplace, upskilling managers have been shown to be an effective means of supporting recovery and RTW. Evidence indicates this training is associated with significantly improved rates of managerial supportive behaviours, especially for employees experiencing mental health problems (Gayed et al., 2018) and reduced rates of work-related sick leave (Milligan-Saville et al., 2017). There is also some suggestion that optimal results require multi-component work interventions incorporating work modification and support (Gray et al., 2019; World Health Organization, 2022). Secondly, there is increasing evidence that clinical treatments need to be modified if functional recovery is going to be achieved alongside symptom reduction (Chokka et al., 2023; Lundqvist et al., 2023). Ideally, an effective psychological intervention should reduce both functional (i.e., work-based) and clinical outcomes, however, this is not the case in many instances (Finnes et al., 2019). Evidence from the United Kingdom and Scandinavian countries suggests that additional training of clinical staff and provision of work-focused rehabilitation services are needed (Cullen et al., 2018), and similarly, combining supportive interventions with clinical interventions is indicated on the back of promising results (Nieuwenhuijsen et al., 2020; Salomonsson et al., 2018). Finally, the data presented here demands that the Workers’ Compensation Schemes in Australia need to be re-examined to determine how a scheme that was designed to facilitate rapid recovery now appears to be achieving the opposite.
There is capacity and increasing appetite for intervention in this area, but resources must be directed to where they are most essential and likely to have impact (e.g., where strong evidence exists and where rates are highest). Similarly, further research is required to determine how to effectively respond to specific risks and facilitate RTW. Time will determine the impact of recent regulatory changes, but guiding workplaces on how to effectively modify and minimise risk where it is present is essential. It is only through such action that we can hope to arrest and reverse these concerning trends.
Footnotes
Declaration of conflicting interests
All authors are based at and/or employed by the Black Dog Institute which provides workplace training. The authors receive no financial or other benefit from these programs. The authors declare no other potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: State Insurance Regulatory Authority (SIRA) and National Health and Medical Research Council (grant number 1178666).