
Abstract
Globally, extensive research has been conducted on psychological trauma. The main intention of this scientific enquiry was to provide insights into the explanatory and etiological factors of such trauma, as well as provide measures of how to manage and treat it effectively. However, much of these research studies on psychological trauma have focused primarily on victims and witnesses of trauma, completely overlooking and neglecting offenders (perpetrators) and their trauma. This study set out to explore perpetrator trauma among juvenile offenders incarcerated for violent offenses. The study was qualitative in nature, using descriptive phenomenology to provide descriptive accounts of perpetrator trauma as experienced by the participants. A single case study design was utilized as a research design. The data were collected using semistructured audio-recorded individual interviews with 10 participants. The findings supported the existence of perpetrator trauma as the offenders experienced multidimensional consequences from their actions. They experienced various symptoms related to or associated with their offenses and victims, including reliving symptoms, psychotic symptoms, psychogenic amnesia of the offense and the victims, and experienced a persistent negative emotional state. They also engaged in reckless and self-destructive behaviors, avoidant behaviors, and significant behavioral changes could be noted in their behavior.
Introduction
The world history of violence, wars, apartheid, holocausts, and genocides has led to the development of the concept of psychological trauma (Karam, 2019; MacNair, 2002a; Tsutsui, 2009). These various acts of violence, which encompass human history, have led to immense psychological consequences and lasting emotional harm (Archer, 2017; Dinisman & Moroz, 2017; McBrearty, 2011; Travis, 2009). As a result, scholars worldwide have conducted extensive research (Archer, 2017; Dinisman & Moroz, 2017; Huemer et al., 2012; McBrearty, 2011; Monson et al., 2007; Sadock et al., 2015; Travis, 2009) in this field to understand this kind of trauma, with the American Psychiatric Association (APA) identifying and recognizing explanatory diagnoses known as post-traumatic stress disorder (PTSD) and acute stress disorder in efforts to effectively manage, treat, and help individuals suffering from this kind of trauma (APA, 2013, 2022; Sadock et al., 2015). However, most of these trauma studies and trauma-related disorders have focused primarily on victims and witnesses of trauma, with trauma argued to be an experience primarily belonging to victims (Mohamed, 2015; Morag, 2012; Robinson, 2018). Trauma and victimhood have always been deemed synonymous. As a result, it was, and still is, considered unimaginable how an offender or perpetrator might experience psychological trauma when inflicting violence and pain on others (Karam, 2019; Mohamed, 2015; Morag, 2012). Instead, only victims are argued to experience this psychological response (Mohamed, 2015). This argument was further enforced by the exclusion of perpetration as a possible cause for trauma development, particularly PTSD and acute stress disorder (MacNair, 2001, 2002a, 2015).
In recent years, the question of whether causing an adverse event or perpetrating violence might lead to psychological trauma has been posed, with various scholars attempting to generate both empirical and theoretical literature to understand and assess its probability. Scholars who sought to explore this phenomenon have identified that perpetrators might also experience trauma due to their own violent acts (Anderson, 2018; Glover, 1988; Gray et al., 2003; Grossman, 1995; Harry & Resnick, 1986; Karam, 2019; MacNair, 1999, 2001, 2002a, 2007, 2015; McGlothlin, 2020; Mohamed, 2015; Morag, 2012; Robinson, 2018; Roldán-Sevillano, 2021; Ternes et al., 2020; Travis, 2009; Tsutsui, 2009)—establishing that exposure to one's violent acts causes lasting psychological harm and leads to a disruption to the individual's moral compass (Anderson, 2018; Karam, 2019; Litz et al., 2009; MacNair, 2001, 2002a, 2007, 2012, 2015; Mohamed, 2015; Morag, 2012; Robinson, 2018; Travis, 2009; Tsutsui, 2009). These findings have led to the concept of perpetrator trauma, which refers to the psychological response experienced by perpetrators following their own violent offending (Mohamed, 2015). This psychological response is characterized by hallucinations, disorientation, unexplained bodily ailment, autonomic responses, memory lapses, flashbacks, nightmares, hypervigilance, anger outbursts, and personality changes (Chung et al., 2016; Karam, 2019; MacNair, 1999, 2001, 2002a, 2002b, 2002c, 2008, 2015; McGlothlin, 2020; Mohamed, 2015; Roldán-Sevillano, 2021). Although perpetrator trauma has been established, the available literature has focused primarily on people who have perpetrated violence in their line of duty (Karam, 2019; MacNair, 2001, 2002b, 2007, 2012, 2015; Mohamed, 2015), with comparatively limited focus on offenders, in particular juvenile offenders.
Mental health studies on the juvenile offender population established that approximately 6% to 19% of juvenile offenders tend to suffer from PTSD or trauma-related symptoms (Facer-Irwin et al., 2019; Gottfried & Christopher, 2017; Tsang, 2018; Wilson et al., 2013). However, in much of these findings, emphasis was placed on childhood adverse events and previous victimization as possible causes for their trauma (Cauffman et al., 1998; Dutton, 1995; Farina et al., 2018; Wilson et al., 2013). The offenders’ violent acts have been overlooked as an explanatory factor for the trauma, with minimal research (Gray et al., 2003; Harry & Resnick, 1986; Ternes et al., 2020) focusing on the offenders’ violent offending as a possible cause for their trauma. This study aimed to explore and describe the presence of perpetrator trauma among violent juvenile offenders.
Perpetrator Trauma Among Combat Veterans and Beyond
The bulk of perpetrator trauma research has been conducted among combat veterans as the point of reference. Various military-based studies and literature exploring the post war adjustment of Vietnam veterans, as well as studies conducted among Israeli combat veterans and combat veterans returning from Operation Iraqi Freedom (in Iraq) and Operation Enduring Freedom (in Afghanistan), established that the combat veterans directly involved in the killing or harming of others during their deployment presented with some psychological reactions. These reactions were characterized by severe personality changes, confusional states, depressive and anxiety symptoms, alcohol and drug abuse, interpersonal difficulties as well as significant functional impairments, especially postdeployment (Grossman, 1995; Levi-Belz & Zerach, 2018; MacNair, 2001, 2002a, 2015; Maguen et al., 2010; Seal et al., 2009; Solomon et al., 1994; Zerach & Levi-Belz, 2018). In efforts to conceptualize the veterans’ experiences during their deployment, Litz et al. (2009) argued that most of these veterans experienced what they coined as moral injury, a term closely associated with perpetrator trauma. Moral injury refers to the lasting psychological, emotional, and cognitive harm caused by transgressing one's moral values and beliefs (Griffin et al., 2019; Litz et al., 2009; Zerach & Levi-Belz, 2018). This injury might be caused by the commission, omission, or witnessing of an act that is deemed as morally injurious, which in their nature, shatters one's existing moral and ethical schemas and these schemas are rooted in religion, spirituality, culture, organizations or group-based rules and norms about fairness, justice, the value of life, and many others (Griffin et al., 2019; Litz et al., 2009; Maguen et al., 2020; Zerach & Levi-Belz, 2018). Transgressions to these shared moral codes or deeply held beliefs about morality lead to dissonance or moral conflict, causing self-destruction, disequilibrium, shame, guilt, and many other symptoms consistent with perpetrator trauma (Atuel et al., 2020; Litz et al., 2009). While moral injury shares many characteristics with perpetrator trauma and might have similar symptom sequelae, it differs from perpetrator trauma in that moral injury is a broader term not only limited to carrying out a violent act but can also include failing to act morally or witnessing an immoral act (Griffin et al., 2019; Litz et al., 2009), while perpetrator trauma is solely perpetration based (Mohamed, 2015).
Although perpetrator trauma and moral injury have their roots in military-based studies and literature, there exists empirical literature and evidence of its presence among various individuals who perpetrated various acts of violence and atrocities (Dillard, 2008; MacNair, 2001; Rohlf & Bennett, 2005; Vice, 2014). Studies among gang members established that violent perpetration among youth gang members is associated with developing PTSD-like symptoms such as dissociation and emotional numbing (Kerig et al., 2016; Robinson, 2018). Another study among police officers who either killed or caused serious injury to another in the line of duty revealed that these officers experienced symptoms congruent to those of PTSD, concluding that their perpetration might contribute to their traumatic sequelae (Komarovskaya et al., 2011). Furthermore, scholars who studied the mass killings and holocausts perpetrated by the Nazi party found that those actively involved in the atrocities experienced psychological consequences and several consistent nervous breakdowns from their participation (MacNair, 2001; Vice, 2014).
Perpetrator Trauma Among Violent Juvenile Offenders
Although extensive literature indicating that violent perpetration might lead to psychic suffering exists, this exploration on offenders, specifically juvenile offenders, is relatively scant despite research proving that a significant number of young people tend to engage in violent behaviors (Bhorat et al., 2017; Booyens et al., 2018; Clark, 2012; Simmons et al., 2019; Souverein et al., 2016). The World Health Organization (2020) reported that juvenile violence and offending are visible in many countries and are a widespread, ever-present phenomenon. In South Africa, juvenile offending is deeply entrenched and has evolved from typical misbehavior and petty crimes to more serious, violent, and organized criminal activities (Booyens et al., 2018; Clark, 2012). This is evidenced by the increasing number of juveniles convicted and incarcerated for violent crimes from the late 1990s to date (Bezuidenhout, 2018; Clark, 2012; Hoosen et al., 2022; Souverein et al., 2016) and the increasing number of incidents involving violence in schools (Burton & Leoschut, 2013; Kutywayo et al., 2022; Mncube & Madikizela-Madiya, 2014; Ncontsa & Shumba, 2013; Qwabe et al., 2022). Their involvement in these violent offenses increases their risk of developing perpetrator trauma symptoms.
Their increased risk of developing perpetrator trauma symptoms is largely associated with their susceptibility to violent offending. They are susceptible to violent behaviors through their age, immature neuropsychological functions, exposure to volatile socioeconomic conditions, poverty, adverse childhood experiences, use of substances, peer influences, and gang affiliations (Bhorat et al., 2017; Booyens et al., 2018; Clark, 2012; Jordaan & Hesselink, 2018, 2022; Simmons et al., 2019; Souverein et al., 2016; Ward, 2007; Ward et al., 2012). These factors might lead them to engage in violent acts without fully comprehending the consequences of their actions, or they might act without full intention only to realize the implications of their actions at a later stage. Thereby precipitating and perpetuating their perpetrator trauma symptoms.
Purpose of the Study
Perpetrator trauma seems to exist. However, the development, manifestation, and impact of perpetrator trauma among the offender population remain a mystery. The uniqueness of the offender population in their motivation to carry out violent offenses and the different circumstances in which such violent events and incidents are carried out might differ from those of combat veterans, police officers, soldiers, or perpetrators of holocausts and genocides whose traumatic experiences were largely explored. Therefore, this warrants a different approach and further proves the importance of exploring perpetrator trauma among juvenile offenders. Furthermore, the study of perpetrator trauma among juvenile offenders is important for clinical practice and empirical, rehabilitation, and reintegration purposes. The presence of perpetrator trauma among violent juvenile offenders poses a threat to their process of rehabilitation and, if not addressed, might lead to substance abuse, increased risk of reoffending (Morgan et al., 2012), and lead to vicious cycles of violence, particularly against significant others (Dutton, 1995). Mohamed (2015) argued that once offenders return to society without addressing their trauma, such trauma becomes more than a personal experience and negatively affects their larger environment through aggressiveness and violence directed toward others. Moreover, exploring perpetrator trauma will aid in distinguishing between such trauma and PTSD. It could also influence the therapeutic processes to address perpetrator trauma and contribute to debates around making it a recognized and diagnosable disorder.
Research Methodology
Research Aim and Objectives
This study aimed to explore and describe perpetrator trauma among violent juvenile offenders with the following research objectives:
To explore and describe the presence of perpetrator trauma among violent juvenile offenders. To explore and describe the development of perpetrator trauma symptomatology among violent juvenile offenders.
Research Design
This study was qualitative in nature and used descriptive phenomenology to provide a detailed concrete description of perpetrator trauma as the participants experienced it (Merriam, 2009). The nature of the study was both explorative and descriptive, while a single case study (Yin, 2003) was utilized as a research design.
Procedure and Sampling
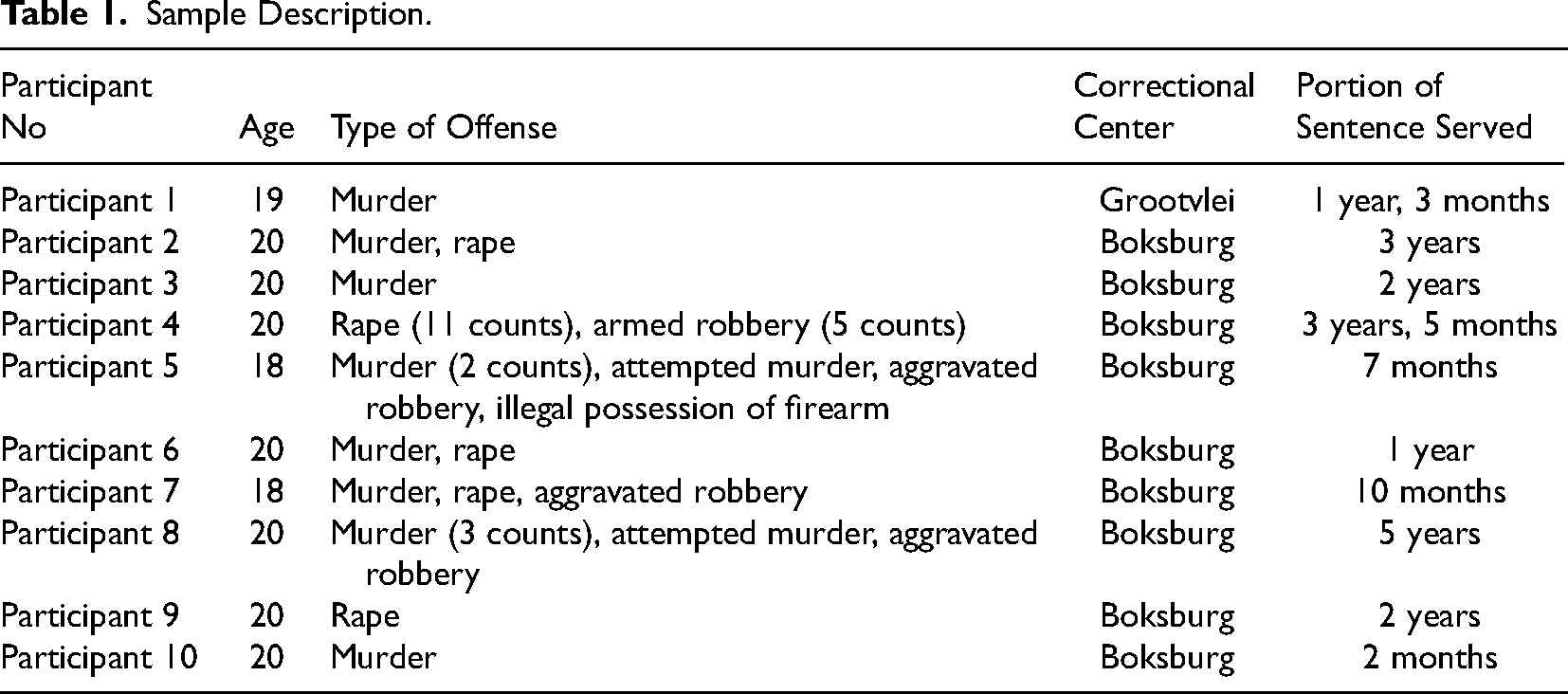
Permission to conduct the study was obtained from the General and Human Research Ethics Committee (GHREC) at the University of the Free State and the Department of Correctional Services (DCS), South Africa. A two-phase sampling procedure was utilized to recruit the participants, with the first phase characterized by convenience sampling and the second phase characterized by purposive sampling (Kumar, 2011; Merriam, 2009). During the first sampling phase, 60 juvenile offenders from Grootvlei Correctional Center (GCC) and Boksburg Correctional Center (BCC) were recruited from a total of 71 available juvenile offenders. The 60 juvenile offenders were recruited based on their availability on the day and their willingness to participate in the study. These offenders were given the study's information leaflet, detailing information pertaining to their participation, including the purpose of the study, the exact nature of their participation, potential risks, benefits, and the voluntary nature of their participation. The participants then gave their written informed consent and thereafter completed a perpetrator trauma symptomatology screening questionnaire developed by the researchers to aid in the recruitment process. The screening questionnaire was divided into two sections, with section A consisting of biographical and offense-related questions, while section B was based broadly on the symptoms of perpetrator trauma as outlined and described by previous perpetrator trauma scholars. Examples of the symptoms participants had to choose from included: (i) I often experience flashbacks or relive the offense I have committed as if it was happening again; (ii) I often made/make efforts to avoid everything related to the offense that I have committed, for example, avoiding thinking or talking about it; (iii) I often see things related to the offense and/or the victim(s), and these things are not seen by others; and (iv) I often have difficulty falling asleep or maintaining sleep because of what I have done. In responding to these symptoms, the participants had to choose from four options that best described their experiences since their commission of their offenses. The options ranged from “never” to “five or more times since I have committed the offense.” The screening questionnaire assisted the researchers with screening the participants and ensuring that the participants who experienced symptoms consistent with perpetrator trauma were identified. The screening questionnaire also assisted in ensuring that the participants’ trauma responses were directly linked to the offenses they have committed and not trauma due to childhood experiences and/or victimization. It is important to note that the screening questionnaire was only utilized as a sampling instrument to ensure the selection of suitable participants and was not used for analysis purposes. After phase 1, phase 2 was initiated, where offenders who reported that they experienced symptoms consistent with perpetrator trauma were recruited to participate in the interviews. Ten participants, who are male, were eventually recruited. Nine participants were from BCC and one participant was from GCC. The 10 participants were recruited based on their age, type of offense, and the fact that they reported the most perpetrator trauma symptoms that were more frequent than the other participants. Table 1 indicates biographical information pertaining to the participants.
Sample Description.
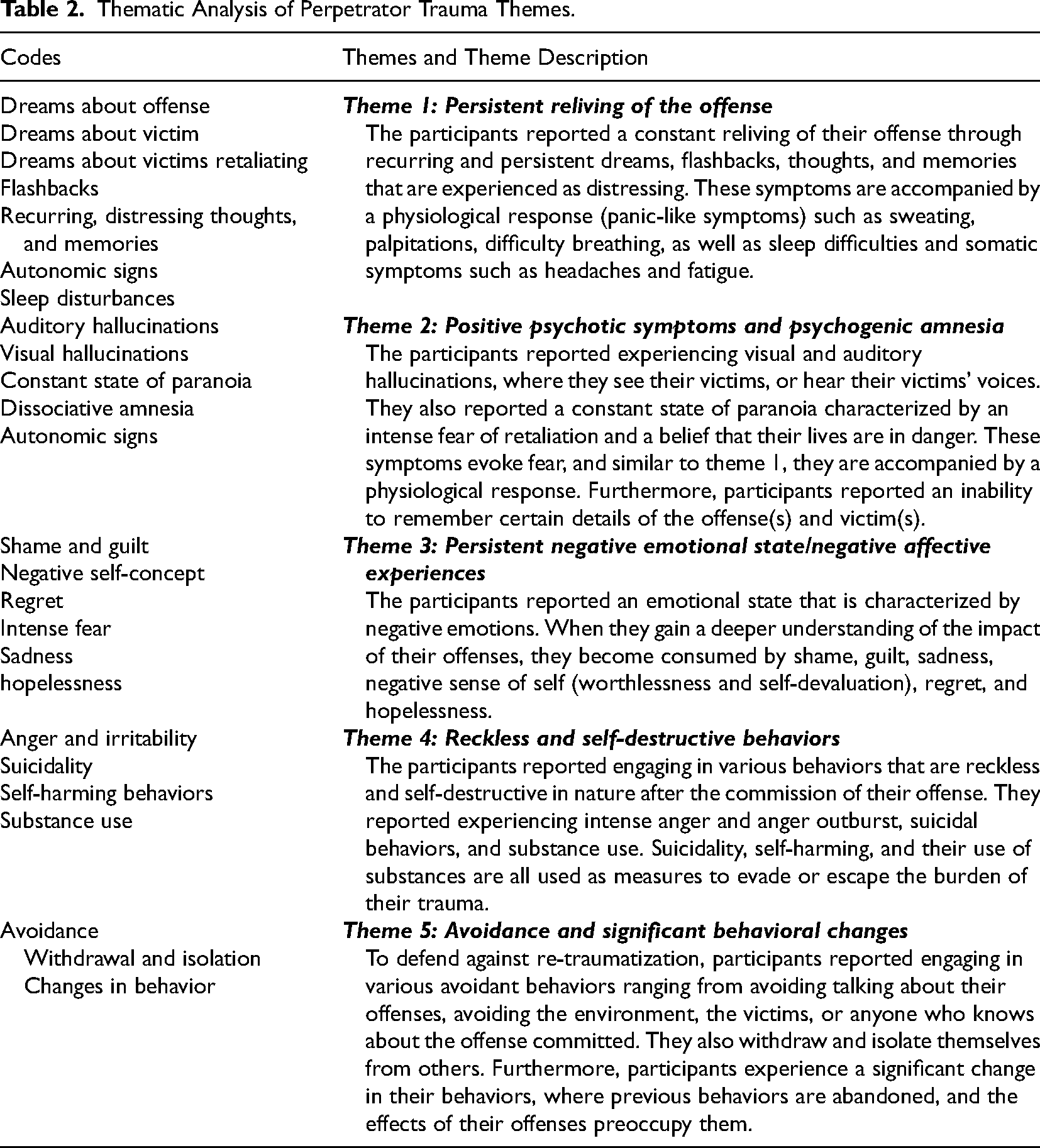
The data from the 10 participants was collected by the first author using semistructured individual audio-recorded interviews (Merriam & Tisdell, 2016; Terre Blanche et al., 2006), which lasted 46 min on average per interview. The interview schedule consisted of questions on: (i) the details of the actual offenses, (ii) the offenders’ longitudinal emotional, cognitive, and behavioral responses to the offenses, and (iii) the range of perpetrator trauma symptoms usually experienced by perpetrators, as outlined in perpetrator trauma literature. The interview recordings were transcribed verbatim and analyzed deductively using Braun and Clarke's (2006, 2022) six-phase framework for thematic analysis. The first author read and re-read the transcripts, and the audio-recordings were occasionally listened to in order to capture the essence and depth of the participants’ responses. The first author shared extracts of the interview transcripts with the other two authors. All three of the authors conducted the analysis independently and they worked from the perpetrator trauma theory and literature to the data in generating codes. The authors then identified preliminary themes. All the generated codes and identified themes were scrutinized, reviewed, modified, and the final codes and themes were decided upon and defined. Five themes, which are discussed in the findings section, were deduced from the literature and the data. The codes and themes are summarized in Table 2.
Thematic Analysis of Perpetrator Trauma Themes.
The active involvement of all the authors in the analysis assisted in ensuring the study's credibility and to eliminate possible researcher biases that might have contaminated the analysis. The authors also ensured trustworthiness by providing details of the recruitment and data collection processes to ensure that proper research guidelines were followed. This will allow future researchers to replicate the study and possibly yield the same results. The results and discussion section will also provide thick descriptions of perpetrator trauma and contextual data about the participants to allow other researchers within the field to make a transfer. In addition, the thick descriptions will enable the reader to understand perpetrator trauma fully and possibly apply it to situations they have encountered or witnessed.
Findings
Five themes which focus specifically on the psychological repercussions of committing murder or causing serious harm to others were deduced from the literature and were similarly experienced by the participants. All 10 participants suffered from persistent and recurring symptoms related to or closely associated with their offenses and their victims; these contributions resemble and echo various accounts of perpetrator trauma symptomatology literature (Chung et al., 2016; Evans et al., 2009; Grossman, 1995; Karam, 2019; MacNair, 2002a, 2008; McGlothlin, 2020; Mohamed, 2015; Roldán-Sevillano, 2021). The five themes were summarized in Table 2. Quotations from the raw data will be included and used to substantiate the themes and support the presence of the symptoms outlined in the literature. Literature will also be incorporated in the reporting of the findings to aid in the discussion and support the participants’ contributions.
Persistent Reliving of the Offense
All the participants reported a constant reliving or re-experiencing of their offenses through recurring and persistent dreams, flashbacks, and thoughts and memories experienced as distressing. The data concurs with the works of Glover (1988), Grossman (1995), MacNair (1999, 2001), McGlothlin (2020), and Roldán-Sevillano (2021), who established that perpetrators of violence constantly have to deal with the haunting repetitions of their actions through intrusive imagery that disrupts their memory and identity. It is very common for individuals who committed murder to experience symptoms that propel them to relive the most painful parts of their actions relating to their victims, in particular, the anguish and helpless state of their victims (Glover, 1988; MacNair, 1999, 2001; McGlothlin, 2020; Roldán-Sevillano, 2021). The first and most frequent symptom reported in perpetrator trauma literature and similarly experienced by the participants is recurrent, persistent, and distressing dreams about their offense(s) and victim(s). Each participant persistently dreamt of their offense, with themes of their dreams and nightmares related to their unconscious processes of guilt and their fears and anxieties. The participants’ responses confirmed the arguments of Glover (1988), Grossman (1995), and MacNair (2008) that there are various dream motifs with the dream content relating to the victim and the offense. Although this is true, literature is deficient in the different kinds of dream motifs that offenders and perpetrators experience, with Glover (1988) identifying two dream motifs: dreaming of the actual event or offense and dreaming one is a victim of the very offense he/she has committed. Similarly, MacNair (2008) identified or expanded on the two dream motifs, where the individuals dream of themselves being confronted and accused by the victims, and secondly, where the perpetrators dream of themselves as victims of the offense(s) they have committed. However, this population experienced various kinds of dream motifs relating to the actual event and the victims. Of the 10 participants, six participants reported dreaming about their offenses as it occurred, particularly the most gruesome parts of the offenses, while other participants reported dreaming about their offenses, however, altered events of the offenses. The participants who reported dreaming about the offenses as it occurred mentioned that: I used to have nightmares about what happened. (Participant 4)
I started having [pause] nightmares, I would dream about everything that I used to do with the guys. (Participant 9)
While those who dreamt of the altered events of their offense echoed their experiences by stating: I dreamt this child was screaming, screaming for help, screaming for help, screaming for help, and I closed her mouth, but I didn’t dream the way, like how I killed her that time, I closed her mouth, I stabbed her by the throat multiple times, I stabbed her by the throat, I stabbed her by the throat, after I stabbed her by the throat, I took the rock, and I threw it on her body, and I threw it this time on her stomach, this was last month, I threw it on her stomach, I took it up again, I threw it on her head. (Participant 2)
Another participant only stabbed his victim once in the neck. However, he reported that: I often dream about the day I committed this offence; it's like I am on top of this lady, and I’m stabbing her multiple times. (Participant 7)
While other participants reported dreaming about their offenses as they occurred in real-time or altered events of the offense, others dreamt about their offenses in symbols, where they dreamt about darkness or their hands covered in blood. For example, participant 7 reported that: Sometimes I would dream it's dark, and when I look at my hands, they are covered in blood. (Participant 7)
This might symbolize various themes. It might even be open to various interpretations as it can literally mean having killed and having blood on one's hands or it can also be interpreted as underlying processes of guilt or anxiety.
Other dream motifs that became evident from the participants’ contributions are dreams about the victim. Nine of the 10 participants reported distressing dreams about their victims where they dreamt of their victims in three ways. Firstly, seeing their victims in their dreams as though they are seeing them: This thing of dreaming, like the victim… I don’t, he is not someone I knew, like he, if I was to picture him or to point him out, he was not someone I knew, I only saw him then, and I was drunk… I used to dream about him…I would see him and know that “Here is the person that we killed!” (Participant 1)
Some of the victims I didn’t know, I don’t remember, but I, when dreaming, you know how dreams are, they would appear as those victims now… I will remember…okay, it's them. (Participant 4)
I have been dreaming dreams about you know, the people that I have murdered…they keep on popping up in my dreams. Like I see them. (Participant 8)
Secondly, dreaming about their victim(s) as though their victims are calling or talking to them. Participant 9 expressed this by stating: I would dream… I am walking, but I’m not getting anywhere…when I look back, I would see the person we killed, like I can see him, in such a way that [pause] “Come” like the person is calling me. (Participant 9)
Thirdly, the participants reported dreaming about their victims or the victim's families retaliating. The participants mentioned: I once dreamt about this guy wanting, strangling me like this, strangling me and saying, “Today you are sleeping with me, today you are coming with me, you are dying just as I died.” (Participant 3)
I once dreamt it was them, 5 of them; they were there now. They were with their fathers, they were having swords, knives, golf sticks, they wanted to beat me up. I was alone there, in the street, and then as I was running, I was running, and they were busy throwing those things at me…And then I found a big tree, I climbed that tree, and when I was climbing the tree, they were busy throwing those things there, and then that's when I woke up… even the following night when I go to sleep, I would dream again. (Participant 4)
While many participants reported being confronted by and reliving their actions in their sleep, many also expressed reliving their offenses when they are awake. They experience it through painful and intense flashbacks, during which they involuntarily get to relive their offenses as though they are happening again. Participants 2 and 6 reported that: Like it comes back to my, to my, to my mind this thing that I’ve done, especially the, the, the moment where I picked up the rock and threw it on top of her face, it's always coming back to my mind. (Participant 2)
It would appear…the time when I was stabbing her… it was like she was standing right in front of me…and I am stabbing her…it would be like it just happened, and I just threw the knife on the, on the floor…I would just keep quiet and stare at her… it's as if I am stabbing her… it's like I just committed the murder now…I see that she has blood on her back, and here is the knife. I just threw it on the floor…and I see her physically collapsing. (Participant 6)
The last reliving symptom that participants experienced is recurring and distressing thoughts and memories about the offense(s) and victim(s). They reported: I see her, like I can picture her in my head, the time I was looking at her… When she was lying there on the floor. (Participant 2)
Like seeing what happened and now like…I’m seeing those victims… they are, they are crying, they are begging me to stop, begging me not to. (Participant 4)
This is in accordance with various sources in perpetrator trauma literature who established that perpetrators are often enthralled by flashbacks and intrusive and involuntary thoughts and memories of their actions and the victims (Glover, 1988; MacNair, 1999, 2001; McGlothlin, 2020; Mohamed, 2015; Roldán-Sevillano, 2021). Moreover, Grossman (1995) and MacNair (1999, 2001) argued that physical proximity between the perpetrator and the victim during the act is closely associated with severe reliving outcomes characterized by horrible and haunting nightmares, flashbacks, thoughts, and memories. This was evident from the analysis, as the participants used more personalized and intimate (close/knife range) means of killing or harming others and reported haunting imagery of these moments.
Furthermore, literature indicates (Chung et al., 2016; Grossman, 1995; MacNair, 1999, 2001; Roldán-Sevillano, 2021) that these symptoms that propel them to relive their offenses are often accompanied by a physiological response (panic-like symptoms) such as sweating, palpitations, difficulty breathing, sleep difficulties, and somatic symptoms (e.g., headaches and fatigue). The participants’ responses corroborated perpetrator trauma symptomatology literature. They stated: When I wake up, remember like as I was having those nightmares, I would wake up I couldn’t breathe sometimes, like now, I would, like I would be sweating, and maybe sometimes [pause] it's cold, but I would be sweating where I couldn’t even wear a blanket, like I’m sweating, I am frightened. (Participant 4)
But when, when I wake up every time my heart is pounding. I don’t really like seeing them to tell you the truth. (Participant 8)
Additionally, sleep difficulties were the most prominent difficulty experienced by the participants as a result of their reliving symptoms. This is consistent with perpetrator trauma symptomatology literature as it was found that a core symptom feature of perpetrator trauma is sleeplessness which is described as the sufferer's inability to escape the haunting repetitions of their actions (Grossman, 1995; Mohamed, 2015). The participants reported that they often have difficulty initiating sleep due to overwhelming thoughts, flashbacks, or memories about the offense or the victim or they woke from nightmares during the night and couldn’t return to sleep. To express this, participant 6 reported: Like now I couldn’t even close, like when I try to close my eyes, it would appear again, and then I would open them, when I open them, I would think about it. (Participant 6)
Another participant reported fatigue when he woke up: I wake up tired, you find that I slept around 7 right, but around 5, when they wake us up…even after they switched on the lights, I am still sleeping…my body would be so tired, it would be like I was doing something at night, I was exercising or something. (Participant 7)
In conclusion, symptoms that propel offenders to relive their offenses through intrusive imagery are among the most prominent symptoms characterizing their trauma. The most prominent theme is the reliving of painful moments of the offense and a constant confrontation with the victims and the offenses through nightmares, flashbacks, thoughts, and memories that are experienced as distressing and are accompanied by autonomic signs and sleep difficulties. Similar to these reliving symptoms, participants experience constant confrontations with their offense and victims through various psychotic symptoms, which are explained in the next theme.
Positive Psychotic Symptoms and Psychogenic Amnesia
Another symptom feature that was prominent in perpetrator trauma symptomatology and present among the current population are positive psychotic symptoms and psychogenic amnesia, where participants reported various hallucinatory moments and expressed an inability to remember certain aspects or details of their offenses. This is supported by Glover (1985, 1988), Grossman (1995), and MacNair (1999, 2001), who established that perpetrators experienced a constant confrontation with their victims through overt psychotic symptoms in the form of hearing the voices of victims confronting them with why they killed or harmed them. The voices also offered a warning to the perpetrator that bad things would happen to them and their families (Glover, 1988). Similarly, participants reported auditory hallucinatory states characterized by similar confrontational themes, where they reported hearing voices of their victims calling them to “death” while others reported hearing their victims’ voices confronting them. They stated: I would hear his voice screaming, “Don’t kill me man, I told you that we will meet again, and today here I am, let's meet.” (Participant 3)
I would hear voices saying, “why did you kill us?” … “why did you kill us?” … “Whose child deserves to be killed?” (Participant 5)
Perpetrator trauma symptomatology literature lacks the descriptive nature to ascertain the most prevalent and prominent hallucinations. However, from this sample, auditory hallucinations were the most common hallucinations, while visual hallucinations were rare and were only spoken of by two of the 10 participants. Participants 3 and 6 reported visual hallucinations by stating: I told the guy I share a cell with, that “Here he is”, “here is the guy, the guy that I killed, here he is.” (Participant 3)
I would see her physically while I am standing. (Participant 6)
These symptoms evoke fear and terror, and similar to reliving symptoms, they are accompanied by physiological responses. Participant 3 reported on the terror he experiences following seeing his victim by expressing: This guy wants to come closer, the guy that I killed, he wants to come closer, he wants to come closer, then I scream, I scream, I cry.
Another prominent feature in the participants’ symptom sequelae is the constant state of paranoia, characterized by an intense fear of retaliation and a belief that their lives are in danger. They are continuously on the lookout for a pending attack and have developed an intense suspicion of others. Their constant state of paranoia supports perpetrator trauma symptomatology literature which states that delusions of reference and persecution are most common where individuals believe some level of threat to their lives by others or that others are talking about or looking at them (Glover, 1988). One of the participants, participant 9, used the metaphor of a small bird in rural South Africa who is constantly at risk of being shot at or hunted. He stated:
But I would be like a bird you see… [demonstration of a startling sound] …do you understand that the life of a bird…was always at risk because we always wanted to shoot it…I also feel the same… like even if you stand behind me, I would push you, like, “What do you want behind me?”
Similarly, participant 6 echoed this by expressing: And then I would just stay awake; others are sleeping, I would just sit alone, and ask myself, like now I was busy looking left, and right, it felt like she would come and avenge herself. (Participant 6)
Lastly, under this theme, the participants reported an inability to remember certain details of their offense(s). Below are extracts from the participants’ transcripts that speaks to their inability to recall certain details of their offenses. Others I don’t remember…Things like, for example, this guy, I tripped the guy and stabbed him, but he said I stabbed him with one hole, but I remember stabbing him with two holes. (Participant 5)
But I remember the five holes that I initially stabbed her with…So, in court, I was told of 30 holes. (Participant 6)
I don’t know how many times I stabbed her after that, I don’t know when and how… even the knife…I don’t even remember where I threw it. (Participant 6)
Persistent Negative Emotional State/Negative Affective Experiences
The participants did not only experience positive psychotic symptoms, psychogenic amnesia, and reliving symptoms, but also described an emotional state characterized by various negative emotions. This finding supports the theory that individuals who kill and cause serious harm to others present with various emotional and affective disturbances, including severe feelings of guilt, self-hatred, and self-condemnation (Glover, 1985, 1988). Schaal et al. (2012) reported that perpetration-based events evoke severe and intense feelings of disgust in oneself. To Schaal et al. (2012), these emotions are preceded by fully realizing one's action and its impact. This is similarly true to the participants’ accounts of their negative affective experiences, as these emotions came soon as they realized the seriousness (magnitude), extent, and impact of their offenses. This realization came with a negative response characterized by a negative evaluation of self, a negative sense of self, feelings of sadness and hopelessness, as well as intense and overwhelming guilt, shame, and regret for one's actions. They reported an internal conflict where they battle with the fact that they have committed such serious, violent, and high-impact offenses, leading to overwhelming regret, sadness, shame and guilt, and a negative sense of self. Participants 4, 8, and 9 reported: I’m feeling guilty, being shameful now, shameful to talk about; at first, I didn’t like to talk about it because okay, it was, it's a, it's a shame, you can also see, what I did is a shame. So I was shameful to talk about it, felt like maybe I am exposing myself. (Participant 4)
I would actually think about how much of a terrible human being…I am… I feel like I am not really, I don’t deserve to be alive. (Participant 8)
When people were sleeping, I would cry, like I was feeling sorry for myself, but at the same time, I am feeling sorry for the people I’ve hurt. (Participant 9)
Reckless and Self-Destructive Behaviours
Many of the participants reported that they started engaging in behaviors deemed reckless and self-destructive after the commission of their offense. These behaviors consist of aggression, suicidality, and substance abuse. Most participants reported that following the commission of their offenses, they started experiencing intense anger, became more aggressive, engaged more in fights, and experienced difficulties with impulse control. In elaborating on this, participants 2 and 7 stated: There are times where when I wake up in the morning, I just have a lot of anger …I just have a lot of anger; I don’t want to talk to nobody. (Participant 2)
It made me short-tempered, I would just sit with the gents, like we are just chilling, but I am already thinking about harming someone; if someone makes a joke, I take it personal…I am already thinking of hitting him, stabbing him, things like that. (Participant 7)
The participants also expressed that they become easily angered when asked about their offenses or when others talk about them. Participant 5 stated: I once fought, but not here, during my trial, you see, because I have, I have an assault case where I stabbed someone; he was talking about this thing. Like I found him [pause] talking about it in my absence, in my absence.
The findings concur with the work of Litz et al. (2009), MacNair (1999, 2001), and Glover (1985, 1988) who observed temper and violent outbursts or violent-prone behaviors among perpetrators following perpetration. According to Glover (1988), the perpetrator's anger and aggression are largely directed toward others than themselves. However, the data shows a different argument as it became evident that for the participants this anger is both directed toward the self and others. For Glover (1988), anger can serve the psychological function of a displacement defense against the unconscious process of guilt and also present as unconscious projections of self-hatred, where anger and aggression are used to dramatize the perpetrators’ negative perceptions of self and their identity as a perpetrator. From the participants, anger as a defense against underlying and unconscious processes became evident, where on various occasions, the participants’ anger was often displaced, and they would project their self-hatred and punishment through physical and verbal aggression directed toward others: I would be angry at everyone, I would not care what people would do like; it affected me because I was fighting with people now, you see. But I was fortunate because I never fought with people like physically; we would fight verbally, words, and stuff, then I would, I would plot with some other people to fight with them… that's how it affected my life. I used to have a lot of enemies right in prison. Even the officials used to say, “this, this, this boy, yes, this one is disrespectful.” (Participant 4)
Even if someone takes a paper, it's mine you see, and since it's mine, maybe he is just pulling my leg… he is making a joke, okay, alright. I don’t take it as a joke, No! I take it personal, because I just had that thought, you see, and now it's like there is a demon that possesses me that “Hey you, do this, again” you see… It was as though it was becoming a habit that if I harm someone, you see, okay, and then that thought would come that “I killed my stepmother; actually it's whatever, uh, it's like I don’t have, I don’t have, I am nothing in life.” (Participant 6)
I would swear at the teachers. I started taking out my problems on others, I was always involved in fights, I was now a violent person. (Participant 7)
Furthermore, the idea that suicidal behavior, including suicidal wishes and fantasies are a common practice among individuals who have killed or caused serious injury to others (Glover, 1988; Litz et al., 2009; MacNair, 2001) was evident in this study as participants reported suicidal thoughts, attempts, and self-harming behavior. The participants used suicidality to escape from their trauma and the reality of having killed or caused serious harm to others. Participants 3 and 8 reported: They once found me attempting to hang myself; I had tied a rope, I had already told myself that “I am hanging myself. They will find me dead in the morning”, but I was interrupted by a police officer. (Participant 3)
I have actually thought of it; I have thought of committing suicide. (Participant 8)
In explaining what he does to make himself feel better, Participant 9 reported self-harming or punishment as a way in which he releases painful emotions and material: Like I would get into the shower and lock myself in, hit the walls with my fists. I am releasing everything that is burdening me, my sister, and I would feel a bit better. Maybe at night, midnight around 1, 2, I would open cold water in the shower, slam my head, like [pause] I deal with my consequences in various ways.
Similarly, substance abuse for the participants offers a temporary escape from their reality. Below are extracts from the participants who used or continue to use substances to escape their trauma: I continued using drugs because the moment I realised this thing it, it was eating me up, you see, it was only better when I was under the influence. (Participant 5)
To lessen some of the things that were tormenting me, I ended up smoking and drinking a lot. (Participant 7)
I have been suffering from trauma for the longest time, even outside, like I was traumatised, but outside I would drink beer, smoke drugs, and then I would forget…it helped a lot, I don’t want to lie. It helped me a lot. (Participant 9)
Although these behaviors are self-destructive and reckless, they serve the psychological function of assisting participants in temporarily escaping and evading their trauma. To further achieve this, they engage in various avoidant behaviors, which are discussed in the next theme.
Avoidance and Significant Behavioural Changes
The individual's innate desire to avoid any reminders of their actions and distance oneself from the horror of having murdered is a common symptom of perpetrator trauma (MacNair, 2001). According to McGlothlin (2020), avoidance, as employed in perpetrator trauma, is a strategy used to evade the memories of the original trauma. This was evident in the participants’ responses as they engaged in various avoidant behaviors to counteract the psychic sufferings that emanated from their actions. They reported engaging in various avoidant behaviors ranging from isolating and withdrawing themselves from others to avoiding the conversations around the offense(s), the environment where they committed their offense(s), the victims, or anyone who knows about the offenses. By avoiding conversations around one's offense, the participants reported: I don’t involve myself in such topics… if they are talking about it in a way that they are loud and stuff, I find something, I read maybe, I can read a book or do something…or I just listen to music volume up, just, just to avoid. (Participant 4)
I actually don’t like talking about it, and I don’t like to be in places where there are a lot of people you see, mam, because that's where someone will bring it up, so I avoid such things. (Participant 5)
Some of the participants expressed that they will not be going back to the environments where the offenses were committed: That's why I even told my mother that I don’t want to go back to Soweto. (Participant 9)
Participant 8, who was convicted of killing his cousins, reported on his need to avoid seeing his grandmother, who was the victims’ caregiver: There was another day where my mom, uh, she told me that my grandma [pause], uh, she would love to see me. And I told her this right away, that I don’t, I don’t, I don’t want to see her…I think it's because of what I have done or it's because it would remind me, like it would take me back to the day because whenever I see her, I would be reminded of her house, I would be reminded of her kids, I would be reminded of everything that, that happened there… I don’t want to see her… I don’t want to see her.
This participant, along with other participants, uses avoidance as a defense against painful memories of their actions. Not seeing their victims or people who know about their offenses and not returning to the environments where their offense(s) were committed is a means to avoid any reminders of what they have done and as an attempt to distance themselves from their actions. These avoidant behaviors can be seen as efforts to repress the unconscious memories, feelings, and thoughts that provoke anxiety in the participants.
Avoidant behaviors and perhaps the increased level of aggression and the significant symptoms associated with the effects of having committed murder and causing serious harm to others might account for the significant behavioral changes that accompany the individuals. According to Litz et al. (2009), significant behavioral changes follow the perpetration of violence, and these changes are characterized by, but not limited to, defiance and loss of spirituality and religion (in previously spiritual and religious people), and this was also evident in the participants’ contributions. The participants experienced a significant change in their behaviors, where previous behaviors were abandoned, and the effects of their offenses preoccupied them. To elaborate on this, participants 2, 5, and 7 reported: I was playing drums in church; there was a time where I gave up on playing drums in church. (Participant 2)
I changed…I have now turned into something else…I also felt like you see, a monster at home. (Participant 5)
Now even the teachers were complaining that I sleep during classes, I would swear at the teachers, I started taking out my problems on others, and I was always involved in fights. I was now a violent person. (Participant 7)
It is evident in this theme that the participants experienced a wide range of symptoms that were associated with their offense(s) and victim(s) as well as experienced significant behavioral changes.
Discussion
The primary aim of this study was to explore perpetrator trauma among juvenile offenders incarcerated for violent offenses. The participants narrated their general experiences of having committed murder or causing serious harm to others which was accompanied by psychological, emotional, social, cultural, and moral consequences. This closely mirrors the experiences of combat veterans, perpetrators of holocausts, genocides, and apartheid, including many others who had to deal with the aftermath of having broken and violated social norms, contracts, and their personal, familial, and societal moral borders. The findings also support the notion that perpetrator trauma is an experience that is not only limited to individuals who murdered in their line of duty but transcends to various other individuals, including offenders. This supports the works of Gray et al. (2003), Harry and Resnick (1986), and Ternes et al. (2020), who argued that offenders might experience post-traumatic stress reactions from their own violent offenses. The population in this study experienced various symptoms associated with their offenses and victims. They also experienced both emotional and moral torments for going against the legal, moral, societal, cultural, spiritual, and familial set of rules, with the act of murdering or causing serious harm to others representing what McGlothlin (2020, p. 106) referred to as an “immutable transgression of a radical experiential threshold that, once crossed, cannot be re-traversed.” Dire consequences accompany this immutable transgression. For some participants, it affects their integrity and identity when the offense is internalized, during which they feel as though they have become their offenses. This supports the works of Anderson (2018), McGlothlin (2020), and Roldán-Sevillano (2021), who argued that such perpetration-based events are known to destroy societal ties and leads to an existential divide between society and the perpetrator, which complicates the perpetrators’ ability to see themselves outside of their offenses. Thus their offenses becoming part of their personal identity. In addition, they experience various symptoms that corroborate perpetrator trauma symptomatology literature where they constantly and persistently relive their offenses through flashbacks, nightmares, memories, and thoughts about their offenses and victims, as well as experiencing psychogenic amnesia and positive psychotic symptoms in the form of auditory hallucinations, and a constant state of paranoia, and rarely, visual hallucinations (Chung et al., 2016; Evans et al., 2009; Glover, 1985; Grossman, 1995; Harry & Resnick, 1986; Karam, 2019; MacNair, 1999, 2001, 2008, 2015; McGlothlin, 2020; Mohamed, 2015; Roldán-Sevillano, 2021; Ternes et al., 2020). Furthermore, the realization that they caused such serious harm, as well as disrupted and potentially destroyed the lives of others with their actions, brings intense feelings of guilt, shame, regret, self-devaluation and condemnation, sadness, and hopelessness characterizing their lives with a constant negative emotional state (Jinkerson, 2016; Litz et al., 2009; MacNair, 1999, 2001, 2008; Roldán-Sevillano, 2021), which according to Grossman (1995) will preoccupy them for the rest of their lives. They also engage in various reckless and self-destructive behaviors such as aggression and violent outbursts and engage in suicidal behaviors, and use substances as a numbing tool to escape their trauma (Glover, 1985; MacNair, 1999, 2001; Maguen et al., 2010; Roldán-Sevillano, 2021). To further escape and evade their trauma, they engage in various avoidant behaviors such as avoiding conversations around the offense(s), avoiding people who know about the offense(s), avoiding places where the offenses took place, and they avoid seeing or talking about their victims (McGlothlin, 2020). This lack of acknowledgement of the victim or even denial of the offense might be seen as a lack of empathy or remorse for the victim. However, this is a means to evade the burden of their offenses and the accompanying moral impacts. The lasting impact of perpetrating such violent and serious offenses is associated with significant behavioral changes that are observable by others. These significant behavioral changes follow their commission of the violent offenses during which the effects of the offenses preoccupy them. Roldán-Sevillano (2021) argued that changes in interpersonal relations characterized by withdrawal and self-isolation are largely provoked by the perpetrators’ underlying feelings of shame and guilt. Similarly, Litz et al. (2009) argued for the potential outcomes of perpetration-based events, which are largely characterized by severe behavioral changes such as interpersonal difficulties, domestic violence, further criminal behavior, and a loss of spirituality and religion.
Limitations and Recommendations
The major limitation of this study is the relatively small sample size, particularly in a field where minimal is known. The small sample size makes it difficult to make hypotheses about perpetrator trauma among juvenile offenders as the findings of this study are only limited to the participants of this study. Secondly, perpetrator trauma studies in South Africa and globally among juvenile offenders are very limited. Therefore, there were limited conceptual models to choose from in terms of conceptualizing the study and locating it within a specific theoretical framework. Thus, the researcher had to rely on conceptual models based on veterans who murdered in their line of duty and not juvenile offenders or offenders generally. Furthermore, the limited empirical studies on perpetrator trauma also led to the authors developing a screening questionnaire to help in the recruitment process, as there were no other realistic ways in which the participants could have been recruited due to a lack of valid and reliable questionnaires that are specific to perpetrator trauma. Moreover, only participants who reported symptoms of perpetrator trauma on the questionnaire were selected.
Although this study has contributed to the understanding of perpetrator trauma among juvenile offenders, it would be beneficial to explore perpetrator trauma among various offenders including female, child, and adult offenders to compare how perpetrator trauma might differ among these populations and to get a clearer and more descriptive picture of perpetrator trauma among offenders. It might also be beneficial to explore the relationship between type of offense and the type and severity of symptoms experienced as well as possible resiliency factors in offenders who committed similar offenses, however, do not experience perpetrator trauma. Secondly, perpetrator trauma is often neglected and overlooked as it is not an officially recognized and diagnosable disorder. Therefore, it would be of great benefit for offenders if a perpetrator trauma questionnaire (measurement scale) was to be developed. This questionnaire could be used in correctional settings to assist in identifying offenders suffering from perpetrator trauma for successful treatment and management before release or reintegration into society. There is also a need for perpetrator trauma studies that focus on developing conceptualization and treatment models.
Conclusion
In previous years, the existence of perpetrator trauma has been confronted with major protest and contest, with many arguing that perpetrators or offenders murder or commit serious and violent offenses callously and gleefully without any psychological repercussions. However, it was evident in this study that committing murder or causing serious harm to others is associated with psychological consequences not only for the victim and the victims’ families but also for the offenders. These offenders are confronted by various psychiatric and psychological symptoms associated with the offense(s) and the victim(s). These symptoms affect their daily functioning and tend to cause significant behavioral changes that have deleterious consequences on them and the society at large. This is because, without treatment or effective rehabilitation, these traumatized individuals might engage in repetition compulsion, a central feature of trauma, where traumatized individuals unconsciously relive, re-enact, or re-act their traumatic events or find themselves in situations where the event is likely to happen. Therefore, an untreated or unresolved perpetrator trauma might translate into repeated cycles of violence, chronic offending, and recidivism.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.