
Abstract
Objective
To compare outcomes of cranial vault remodeling via fronto-orbital advancement and remodeling (FOAR) versus spring cranioplasty in patients with nonsyndromic unicoronal craniosynostosis (UCS), focusing on surgical parameters and craniofacial symmetry improvements.
Design
Retrospective review comparing FOAR and spring-assisted cranioplasty outcomes using preoperative and postoperative CT data. Statistical analysis was performed using SPSS Statistics 30.0.
Setting
Institutional tertiary care center specializing in craniofacial surgery.
Patients, Participants
Nonsyndromic patients with UCS undergoing FOAR (n = 7) or spring cranioplasty (n = 11), with complete pre- and postoperative imaging and surgical data available.
Interventions
FOAR involved traditional fronto-orbital advancement and remodeling. Spring cranioplasty consisted of spring placement followed by spring removal surgery, designed to remodel cranial vault less invasively.
Main Outcome Measure(s)
Retrospective review of surgical time, estimated blood loss (EBL), packed red blood cells (PRBC) transfused, intracranial volume (ICV), facial twist (FT), skull-base twist relative to palate (SBT-P) and nasion (SBT-N), and orbital morphology symmetry.
Results
Spring cranioplasty, when considering both placement and removal, significantly reduced operative time (157.9 ± 28.6 vs 264.7 ± 48.3 min), EBL (5.5 ± 1.6 vs 26.5 ± 9.2 mL/kg), and PRBC transfusion (2 ± 4.2 vs 27.4 ± 5.9 mL/kg) compared with FOAR (P < .001). Postoperatively, patients who underwent spring cranioplasty demonstrated significant improvements in FT, SBT-P, and SBT-N (P = .003), whereas FOAR did not achieve significant changes. ICV did not differ significantly between groups. Spring cranioplasty patients demonstrated superior orbital symmetry improvement.
Conclusions
Spring cranioplasty offers a less invasive alternative to FOAR for UCS, with shorter surgery, less blood loss, and better craniofacial symmetry correction without compromising ICV expansion.
Introduction
Craniosynostosis affects approximately 1 in 1700 to 2500 births and results from premature fusion of one or more cranial sutures, which restricts growth perpendicular to the fused suture and produces compensatory growth at unaffected sutures.1,2 When a single suture is involved, the resulting cranial morphology is often predictable and diagnosis can be confirmed with CT imaging. Coronal craniosynostosis accounts for 15 to 25% of cases and may present unilaterally or bilaterally. 3 Unilateral coronal synostosis (UCS) is characterized by a combination of skull base and midfacial asymmetry, manifesting clinically as ipsilateral forehead and frontoparietal flattening, contralateral bossing, nasal root deviation, temporal fossa prominence, superior orbital rim elevation (harlequin deformity), vertical orbital dystopia, and anterior displacement of the ear and temporomandibular joint; with the nasal tip and chin deviating toward the unaffected side.1,2,4 Among the single-suture synostoses, UCS is often considered the most challenging to correct from an esthetic standpoint.5,6
The goals of surgical intervention are to achieve long-term craniofacial symmetry while supporting normal brain growth and development.2,7,8 Over time, management has evolved from strip craniectomy 9 to more extensive cranial vault remodeling procedures.2,10 The most widely performed operation for UCS is bilateral fronto-orbital advancement and remodeling (FOAR), usually undertaken between 5 and 10 months of age. 8 Timing must balance the risks of operating on young infants against the benefits of early correction for craniofacial and neurodevelopmental outcomes.1,4,11–15
Although FOAR is effective in reducing the risk of elevated intracranial pressure, its long-term esthetic results are often suboptimal.10,16,17 Immediate improvements are typical, but relapse toward preoperative morphology may occur over time, as FOAR does not directly address cranial base asymmetry. 18 Collectively, these findings underscore the limitations of FOAR in achieving lasting esthetic correction. In response, several authors have recommended intentional overcorrection at the time of FOAR surgery to counteract relapse, though this strategy remains difficult to accomplish given the constraints of the soft tissue envelope.7,17
Endoscopic-assisted craniectomy with postoperative cranial orthosis (ESC) offers a less invasive alternative, providing shorter operative times, reduced blood loss, and shorter hospital stays. 4 While traditional strip craniectomy yielded poor cosmetic results, modifications incorporating postoperative orthosis,4,19,20 or endoscopic-assisted fronto-orbital advancement, 21 improved esthetic and ophthalmologic outcomes, and in some cases surpassing FOAR.
Over the past decade, fronto-orbital distraction osteogenesis (FODO) has been increasingly applied for UCS. Unlike FOAR, FODO promotes gradual expansion, allowing new bone formation, soft tissue adaptation, and preservation of vascular supply. Comparative studies demonstrate improved long-term orbital symmetry, less temporal hollowing, and fewer residual deformities compared with FOAR.6,22,23 Distraction techniques have been shown to achieve more durable correction of skull base and orbital asymmetries, reduce postoperative strabismus, and lower perioperative morbidity, including blood loss and transfusion requirements.5,24,25
Spring cranioplasty, widely adopted for sagittal synostosis, also applies gradual distraction with lower perioperative risk. Its use in UCS, however, has been reported only in an isolated case description 26 and in a recent preliminary series. 27 These early reports demonstrated promising improvements in facial and cranial base scoliosis that were maintained at mid-term follow-up.
Despite the growing evidence supporting distraction-based methods, including improved orbital and esthetic outcomes with FODO compared to FOAR,5,24 there has been little reported directly comparing spring cranioplasty and FOAR in UCS. For the past 6 years, our group has employed spring cranioplasty in patients with UCS around 3 to 4 months of age, with encouraging early results. This report aims to compare spring cranioplasty and FOAR for correction of UCS, using CT-based volumetric and morphometric analysis evaluating intracranial volume (ICV), craniofacial symmetry, and orbital morphology.
Methods
Patients
We conducted a retrospective study of patients with non-syndromic unicoronal craniosynostosis who underwent either FOAR or spring cranioplasty between August 2014 and June 2024. The study was approved by our Institutional Review Board. FOAR patients were included if they had both preoperative CT scans and postoperative CT scans obtained at least 2 years after surgery. Spring cranioplasty patients were included if they had preoperative CT imaging, with the most recent available postoperative CT scan used for analysis.
Clinical Data and Statistical Analysis
Patient demographics and clinical data were collected from the medical record (Table 1). CT DICOM files were obtained, and pre- and postoperative ICV, facial twist (FT), skull-base twist relative to the palate (SBT-P), and skull-base twist relative to the nasion (SBT-N) were measured using Materialise (Leuven, Belgium) and the open-source software ImageJ (https://imagej.net/ij). Materialise was also used to reconstruct orbital morphology and assess symmetry. To ensure consistency across time points within the same patient, datum planes were established. For FT assessment, one plane was defined by the infraorbital rims at the bilateral zygomaticomaxillary sutures and the sella, and another by the nasion, prosthion, and sella. These planes were aligned to 0 degrees (appearing as a single line), and this orientation was used to calculate the FT angle on the affected side in ImageJ (Supplemental Material 1). For SBT-N and SBT-P, the Frankfurt Horizontal plane was established using the bilateral superior external auditory meatus and the non-affected inferior orbital rim, and this was set to the XY plane in the world coordinate system. The SBT-N angle was measured from a superior view, defined by the angle between a line from the nasion to the sella and a line from the sella to the opisthion on the affected side. The SBT-P angle was measured from the base view, defined by the angle between a line from the incisive foramen to the sella and a line from the sella to the opisthion on the affected side (Supplemental Material 2). Orbital symmetry was assessed by reconstructing orbital volumes, mirroring the unaffected orbit onto the affected orbit, and analyzing the differences.
Patient and Surgical Information.
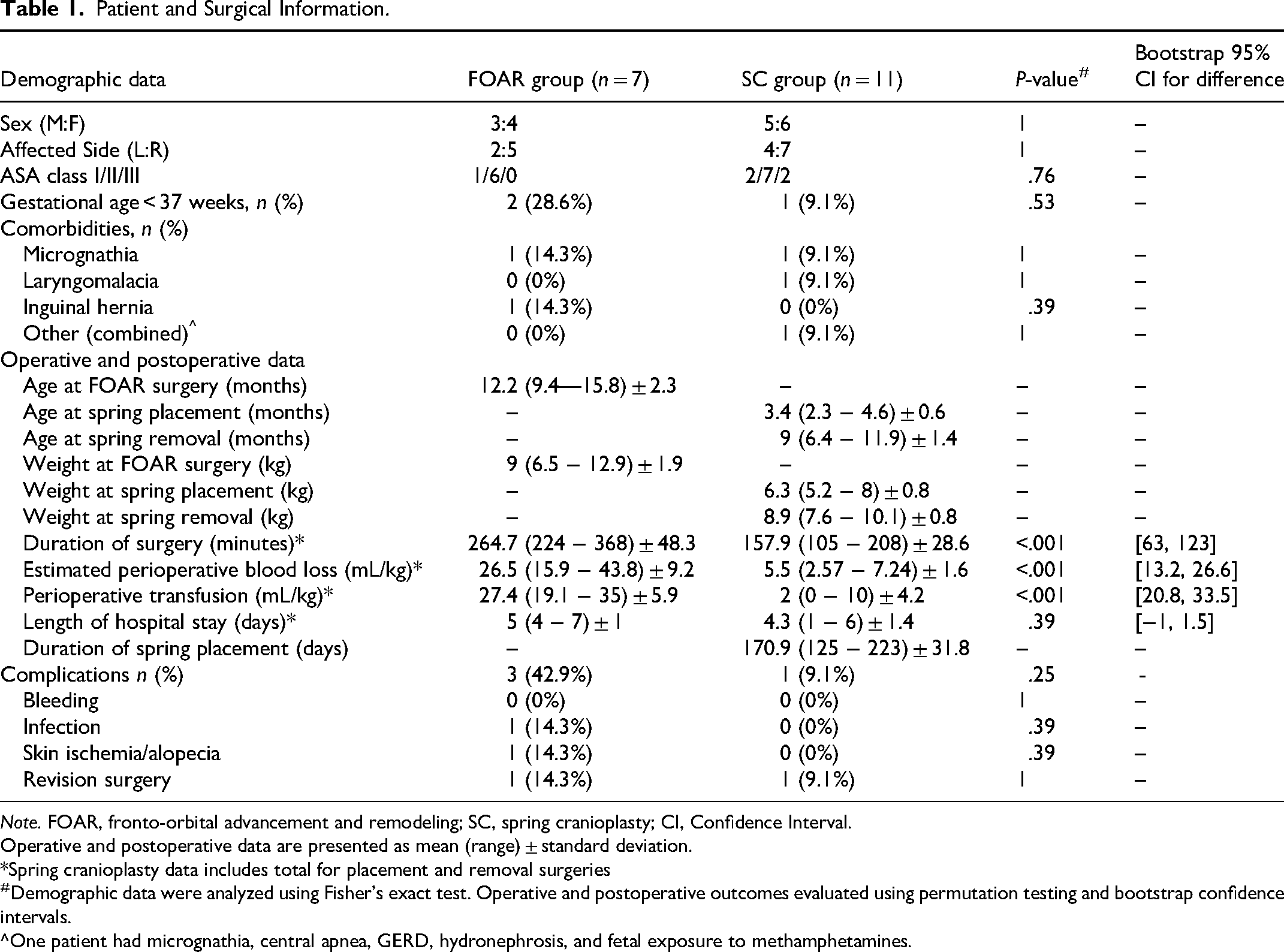
Note. FOAR, fronto-orbital advancement and remodeling; SC, spring cranioplasty; CI, Confidence Interval.
Operative and postoperative data are presented as mean (range) ± standard deviation.
*Spring cranioplasty data includes total for placement and removal surgeries
#Demographic data were analyzed using Fisher's exact test. Operative and postoperative outcomes evaluated using permutation testing and bootstrap confidence intervals.
^One patient had micrognathia, central apnea, GERD, hydronephrosis, and fetal exposure to methamphetamines.
Statistical analysis was performed using Excel Office 365 (Microsoft, Redmond, WA) and SPSS Statistics 30.0 (IBM, Armonk, NY). Demographic data were analyzed using Fisher's exact test. Due to the small, skewed sample distributions, operative and postoperative outcomes between FOAR and spring cranioplasty groups were analyzed with nonparametric methods, including permutation testing and bootstrap resampling to generate confidence intervals. Paired pre- and postoperative craniofacial measurements were assessed with 2-tailed Wilcoxon signed-rank tests. ICV was analyzed using analysis of covariance (ANCOVA) with age as a covariate to account for significant differences in age between groups.
Surgical Technique
At our institution, surgical technique is primarily determined by patient age and family preference. Patients between 3 and 4 months of age are offered spring cranioplasty as the preferred technique. Families are counseled on both surgical options, including risks, benefits, and expected postoperative course. If the parents elect to proceed with spring cranioplasty, the patient is included in the spring cohort. Patients who present after 5 months of age, or whose families decline spring cranioplasty after discussion, undergo traditional FOAR.
Frontal Orbital Advancement and Cranial Vault Remodeling
Bilateral FOAR were performed in a manner consistent with previously described techniques.19,28 Briefly, a bicoronal incision was made, followed by subgaleal dissection to approximately 1.5 cm above the superior orbital rims. Subperiosteal dissection was then carried out to expose the orbital bandeau and lateral orbits. Osteotomies were performed, after which the supraorbital bandeau and frontal bones were reshaped and fixated with absorbable plates (KLS Martin Group, Tuttlingen, Germany). Overcorrection was performed on the affected side. Autologous bone grafts were used to fill defects, and additional barrel stave osteotomies were employed as needed.
Spring Placement
Spring placement was performed according to previously described techniques. 27 Briefly, a hemicoronal incision was made, and dissection was carried out in the subgaleal plane. A suturectomy was then performed using a side-cutting bur with a footplate, extending from the anterior fontanel to the squamosal suture, with a width of approximately 5 to 10 mm. Under direct visualization, a lateral orbitotomy was performed with a matchstick bur to osteotomize the sphenoid wing and lateral orbit. Cranial springs (Osteomed, Addison, TX, or KLS Martin Group, Tuttlingen, Germany) were then placed. The number and strength of springs were determined based on bone thickness and the degree of initial suturectomy distraction at the time of placement.
Spring Removal
Cranial spring removal was performed using the previous incision. The springs were exposed and split at the midpoint to facilitate easier removal. The footplates were carefully freed from the bone and rotated out of place.
Postoperative Protocol
Patients were admitted to the ICU following FOAR or spring placement and to the surgical floor after spring removal. A low-dose craniofacial CT scan was obtained on postoperative day 2 after FOAR or spring placement. In the spring cranioplasty cohort, an additional CT scan was obtained prior to spring removal. For both FOAR and spring patients, a follow-up CT scan was obtained at a minimum of 2 years postoperatively.
Results
Patient Demographics and Clinical Data
As shown in Table 1, the FOAR group included 7 patients (3 males, 4 females) and the spring cranioplasty group included 11 patients (5 males, 6 females). There were no significant differences between groups with respect to sex distribution, affected side, ASA classification, prematurity, or comorbid conditions. When comparing FOAR with spring cranioplasty (placement and removal combined), the mean operative time was 264.7 min for FOAR and 157.9 min for spring, estimated blood loss (EBL) was 26.5 versus 5.5 mL/kg, perioperative transfusion was 27.4 versus 2 mL/kg, and hospital length of stay (HLOS) was 5.0 versus 4.3 days, respectively. The spring cranioplasty group had significantly lower operative time, EBL, and transfusion requirements (P < .001 for all), while HLOS was not significantly different between groups (P = .39).
For both groups, there were no durotomies, cerebrospinal fluid leaks, sagittal sinus injuries, or perioperative bleeding complications. In the spring cranioplasty cohort, no patients experienced spring exposure, malposition, or infection. One patient later underwent FOAR for residual deformity, which was performed at the time of planned spring removal. In the FOAR group, one patient developed a Haemophilus influenzae infection requiring surgical intervention, another required a secondary vault remodeling at age 7 for increased intracranial pressure, and a third developed postoperative skin ischemia that resulted in alopecia without tissue loss. There was no significant difference in complication rates between the 2 treatment groups (Table 2).
Craniofacial Analysis.
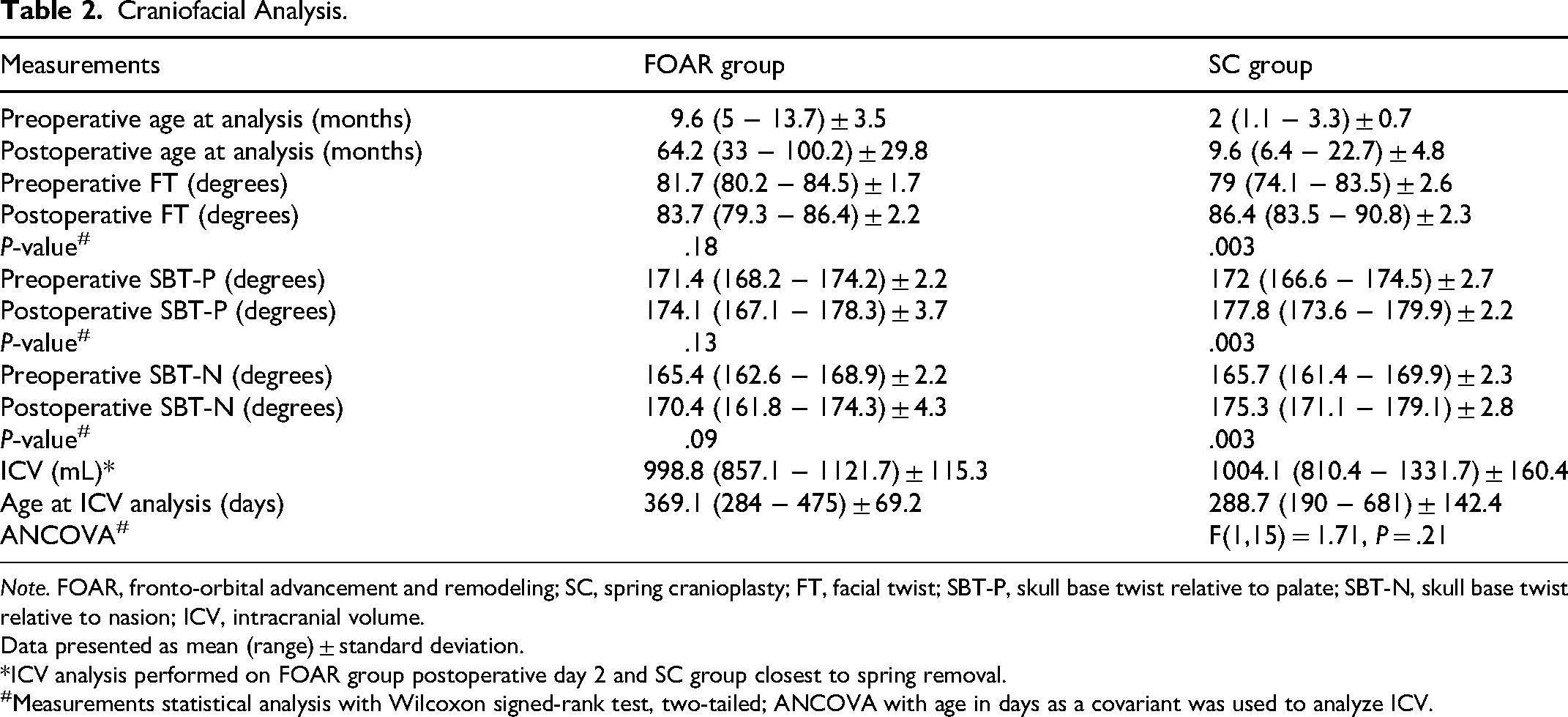
Note. FOAR, fronto-orbital advancement and remodeling; SC, spring cranioplasty; FT, facial twist; SBT-P, skull base twist relative to palate; SBT-N, skull base twist relative to nasion; ICV, intracranial volume.
Data presented as mean (range) ± standard deviation.
*ICV analysis performed on FOAR group postoperative day 2 and SC group closest to spring removal.
#Measurements statistical analysis with Wilcoxon signed-rank test, two-tailed; ANCOVA with age in days as a covariant was used to analyze ICV.
Clinical Results and Analysis
ICV and Craniofacial Morphology Analysis
ICV was analyzed using ANCOVA with age as a covariate. The FOAR group was significantly older than the spring cranioplasty group. Age was a significant predictor of ICV (F(1,15) = 13.78, P = .002), indicating that ICV increased with age, as expected. However, after adjusting for age, there was no significant effect of treatment group on ICV (F(1,15) = 1.71, P = .21).
As shown in Table 2, the mean pre- and postoperative FT angles were 81.7° and 83.7° in the FOAR group compared to 79.0° and 86.4° in the spring cranioplasty group. Improvement in FT was statistically significant after spring cranioplasty (P = .003) but not after FOAR (P = .18). Similarly, the mean pre- and postoperative SBT-P angles were 171.4° and 174.1° for FOAR versus 172.0° and 177.8° for spring cranioplasty, with significant improvement observed in the spring group (P = .003) but not in the FOAR group (P = .13). For SBT-N, the mean pre- and postoperative values were 165.4° and 170.4° for FOAR and 165.7° and 175.3° for spring cranioplasty, again demonstrating significant improvement with spring cranioplasty (P = .003) but not with FOAR (P = .09). A post hoc power analysis was conducted using α = .05 to evaluate the probability of a type II error for variables in which the null hypothesis was accepted. The resulting power values were FOAR FT = 0.609, FOAR SBT-P = 0.532, and FOAR SBT-N = 0.893. A sample size estimation revealed to achieve a power of 0.8 would require approximately 10 subjects for FOAR FT and 12 for FOAR SBT-P.
Figure 1 illustrates pre- and postoperative 3D CT reconstructions of 2 patients who underwent FOAR, showing some improvement in FT and SBT, though less pronounced than in the spring cranioplasty cohort (Figure 2). Overall, the spring cranioplasty group demonstrated greater qualitative improvements in cranial contour, orbital morphology, and symmetry.
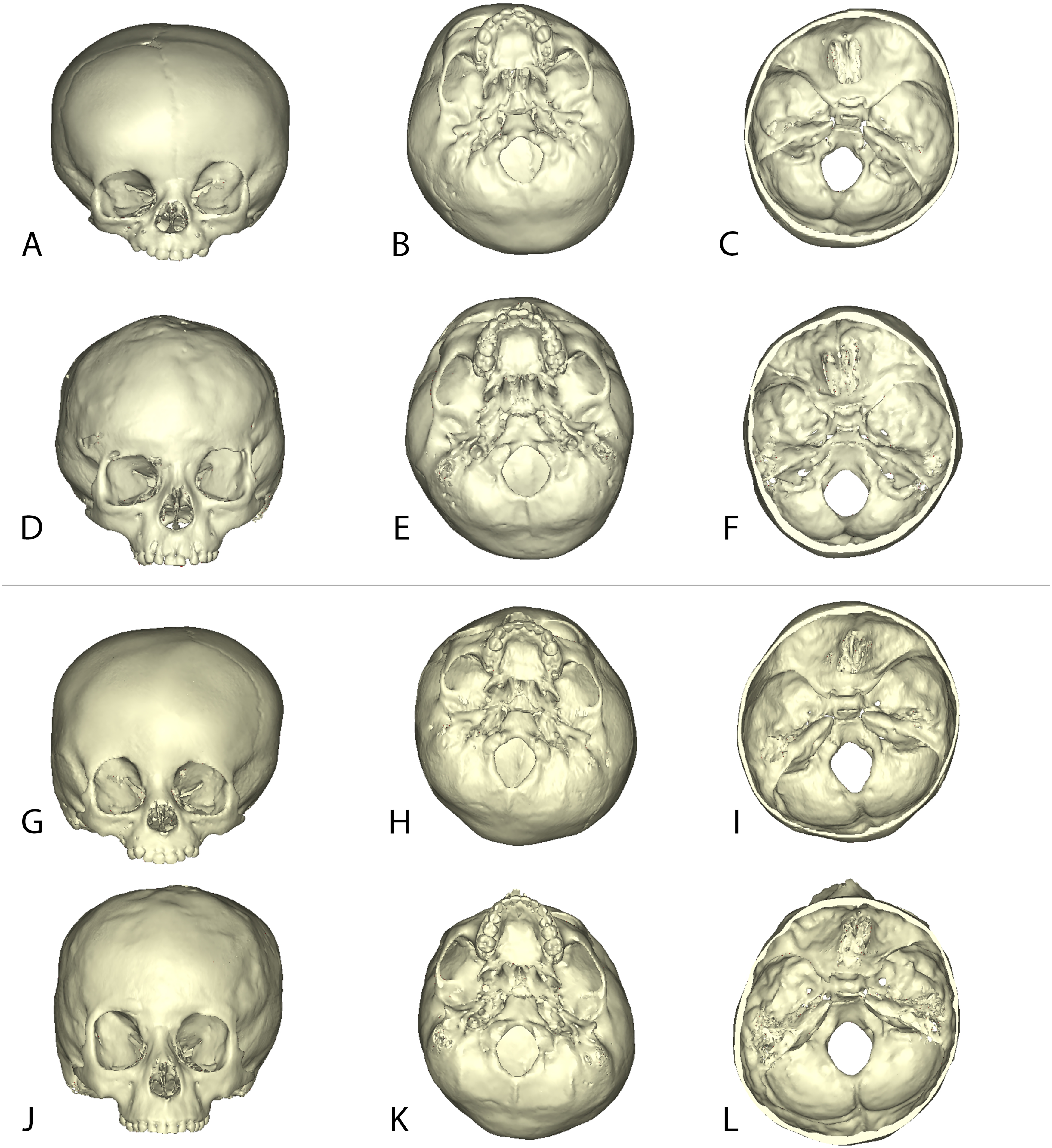
Three-Dimensional Craniofacial CT Reconstructions of 2 Patients From the FOAR Group.
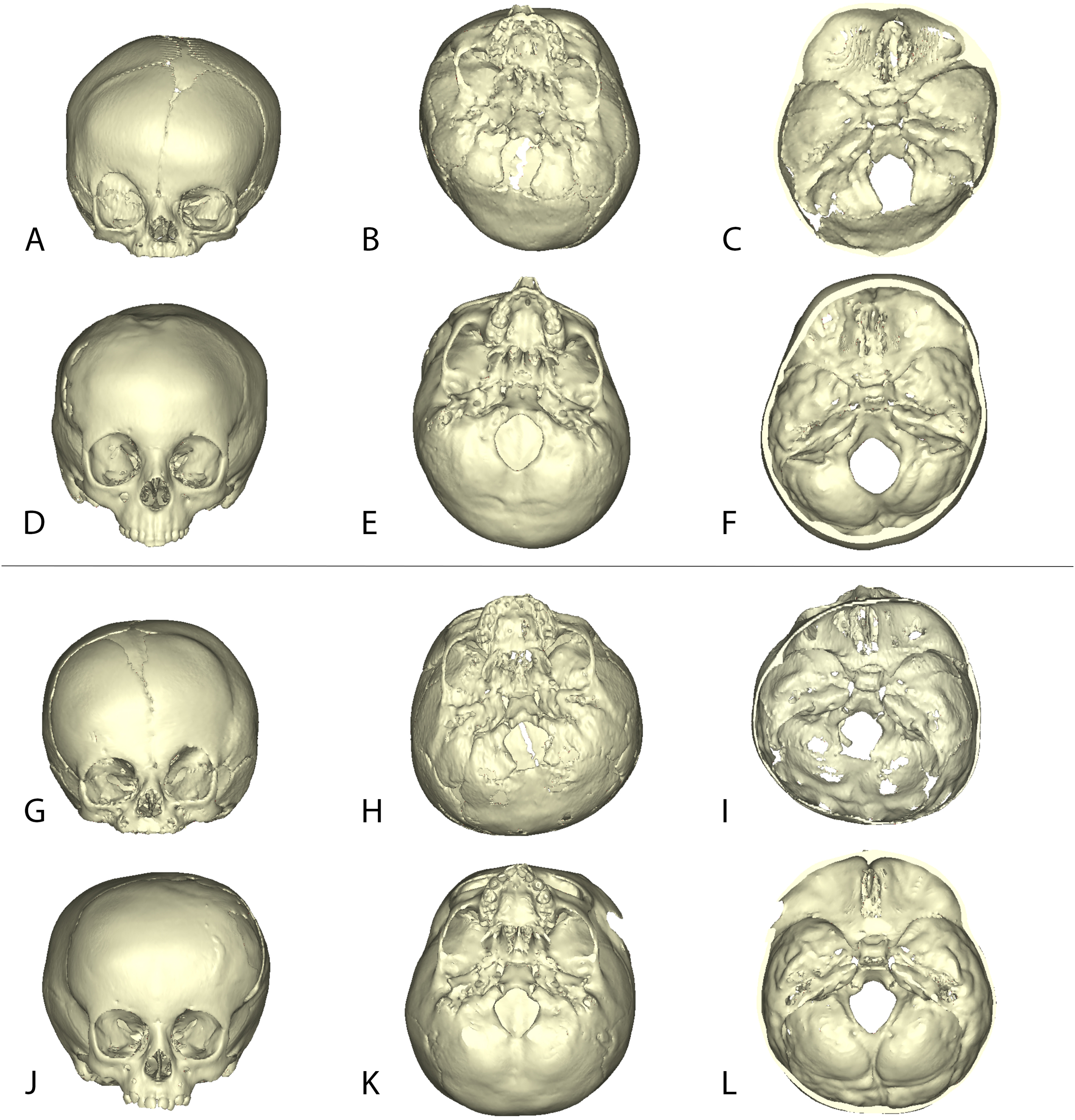
Three-Dimensional Craniofacial CT Reconstructions of 2 Patients From the Spring Cranioplasty Group.
Orbital Assessment
Figure 3 demonstrates pre- and postoperative 3D orbital reconstructions for 3 patients in the FOAR group, showing minimal change in orbital morphology. Top views and overlay heat maps reveal only minor remodeling with persistent orbital asymmetry. In contrast, Figure 4 shows the spring cranioplasty cohort, where postoperative reconstructions demonstrate clear changes in orbital morphology. Overlay heat maps indicate more substantial bony remodeling, and mirrored comparisons reveal improved orbital alignment and symmetry compared with FOAR.
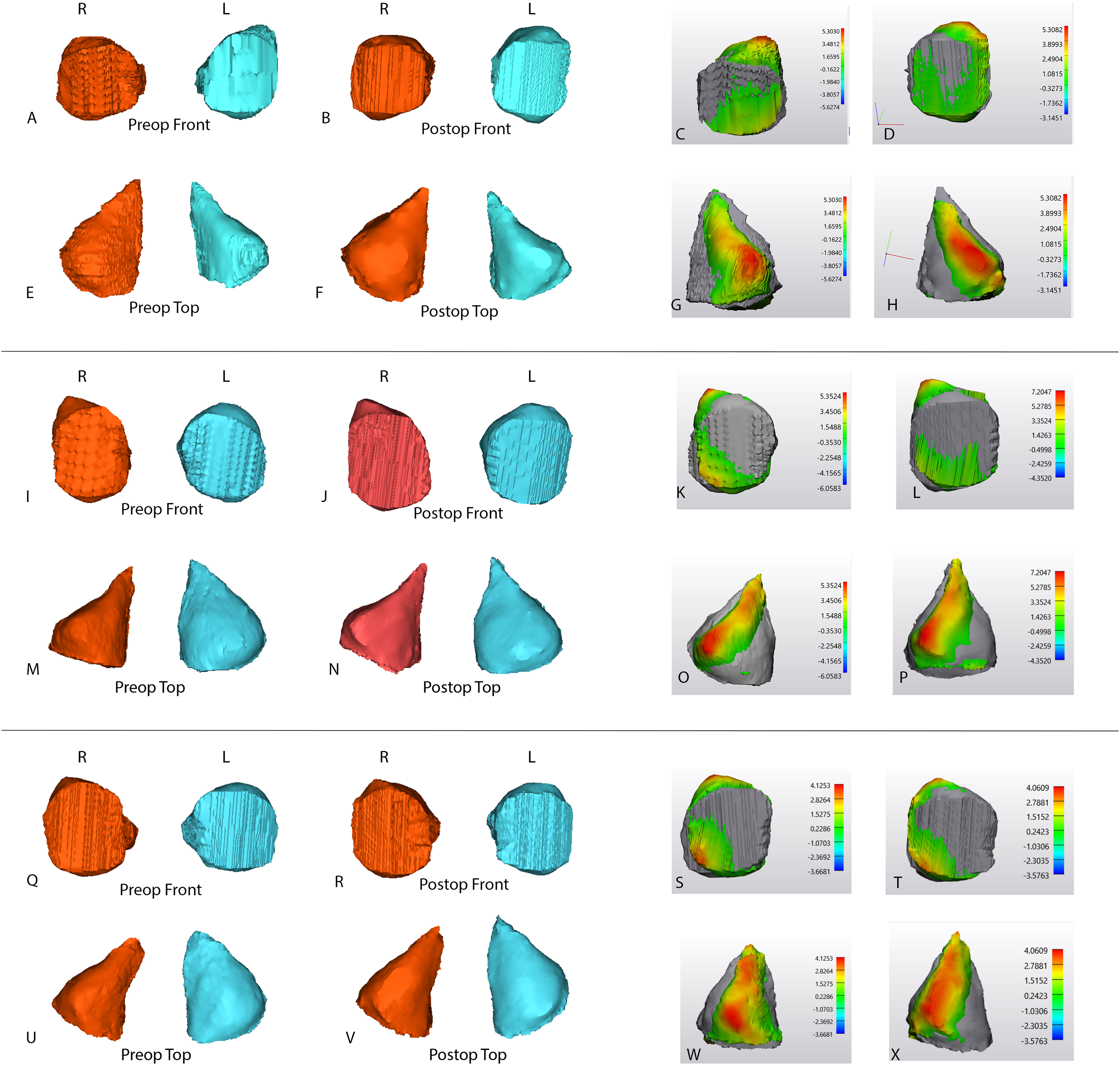
Three-Dimensional Reconstructions of Right (R) and Left (L) Orbits in Patients From the FOAR Group. Symmetry Analysis was Performed by Mirroring the Unaffected Orbit Onto the Affected Orbit (C, D, G, H, K, L, O, P, S, T, W, X).
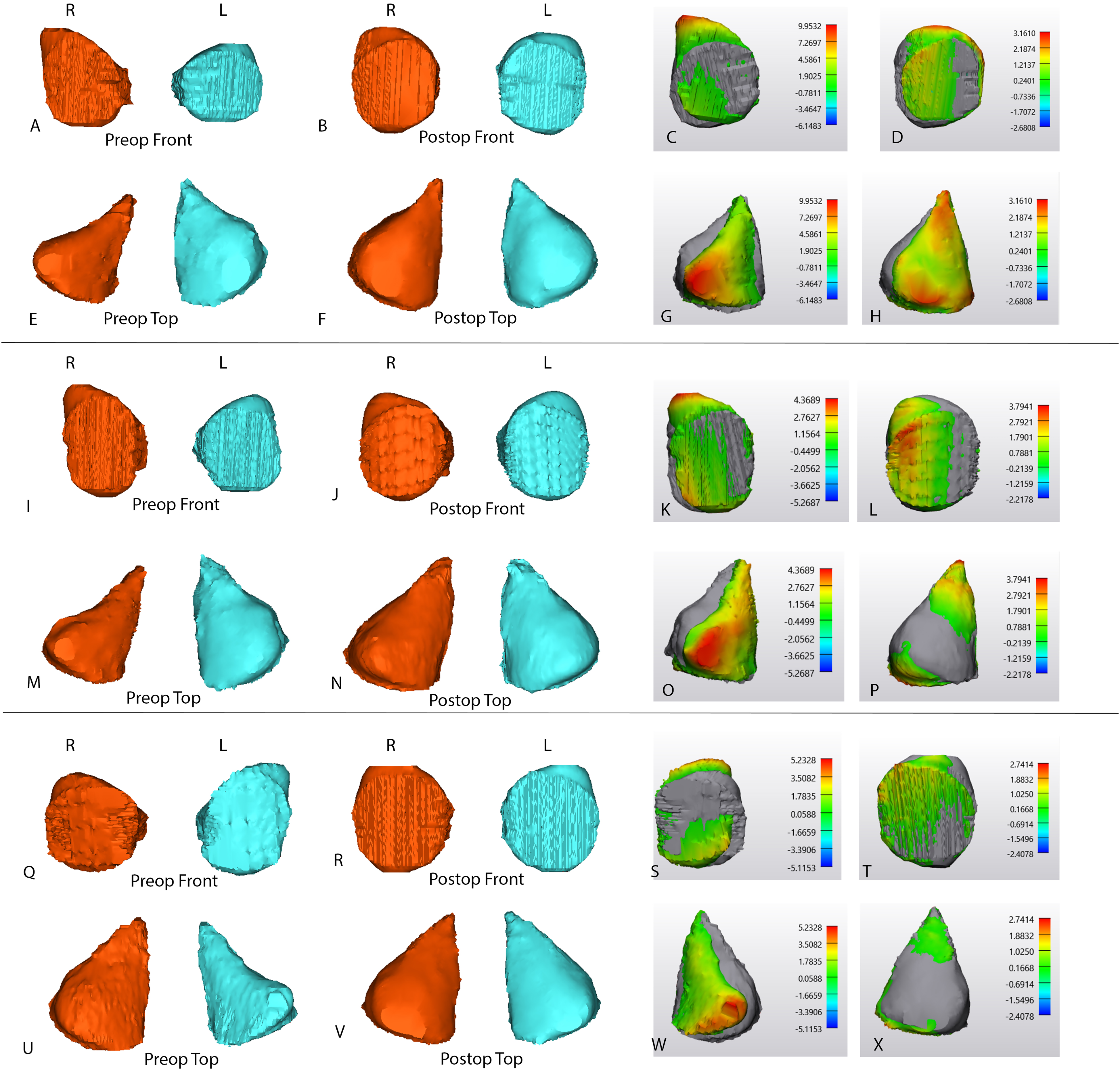
Three-Dimensional Reconstructions of Right (R) and Left (L) Orbits in Patients From the Spring Cranioplasty Group. Symmetry Analysis Was Performed by Mirroring the Unaffected Orbit Onto the Affected Orbit (C, D, G, H, K, L, O, P, S, T, W, X).
Discussion
Surgery for craniosynostosis should primarily strive to optimize brain growth and development, however the correction of the craniofacial dysmorphology is also important due to its psychosocial implications. 8 UCS poses unique challenges because of its combination of cranial base scoliosis, orbital asymmetry, and midfacial twist, which contribute to high rates of residual deformity following surgery. 6 FOAR remains the most commonly performed procedure, yet long-term studies have consistently demonstrated limitations, with relapse toward preoperative morphology and persistent deformities.5,10,17,24 Taylor et al reported that patients followed for more than 5 years after FOAR were 5 times more likely to be classified as Whitaker III or IV, reflecting persistent deformities such as supraorbital retrusion and temporal hollowing. 17 Villavisanis et al further demonstrated that FOAR patients had inferior long-term esthetic outcomes and greater orbital asymmetry compared with those treated by fronto-orbital distraction, 24 while Wu et al showed less favorable photogrammetric results after FOAR than after distraction-based approaches. 29
The disappointing long-term results with FOAR have motivated the search for alternative treatments. ESC was introduced as a less invasive option. Surgery is typically performed before 4 months of age, leveraging the pliability of the infant skull and rapid brain growth. 30 Jimenez and Barone reported that ESC, when compared to FOAR, was associated with shorter operative times, reduced blood loss, and shorter hospital stays. 4 Additionally, improved esthetic and ophthalmologic outcomes compared to FOAR has been reported when used with modifications such as postoperative orthosis,4,19,20 or endoscopic-assisted fronto-orbital advancement. 21
FODO allows for dynamic expansion and has been increasingly reported with good results for UCS. When compared to FOAR, it has been reported that there is improved long-term orbital symmetry, reduction of postoperative strabismus, less temporal hollowing, and fewer residual deformities.6,22,23 Similarly to ESC, there is lower perioperative morbidity, including blood loss and transfusion requirements.5,24,25
Spring cranioplasty is appealing because it can be performed earlier (<6 months old), taking advantage of rapid brain growth, potentially interrupting the coronal ring fusion cascade, and possibly improving neuropsychological outcomes.11,13,14,28 In addition, springs are associated with decreased operative time, blood loss, and transfusion requirements. While endoscopic surgery with cranial orthosis offers similar perioperative benefits, the use of cranial orthosis requires frequent visits, highly compliant families, and skilled orthotists, and can be associated with increased cost and prolonged treatment.4,20,21 Distraction osteogenesis also provides gradual correction with favorable long-term outcomes, but its use carries the risks of pin-site infection, scarring or alopecia, and restrictions on distraction vectors.6,24,28,31
In the present study, spring cranioplasty demonstrated several advantages over FOAR. Operative time, blood loss, and transfusion requirements were all significantly lower in the spring cohort, findings consistent with the reduced morbidity typically reported for less invasive, distraction-based techniques. Although HLOS did not differ significantly between groups, we anticipate shorter stays with spring cranioplasty as institutional experience with the procedure increases. Beyond perioperative outcomes, spring cranioplasty also produced superior morphometric results. While both groups showed some degree of postoperative improvement, only spring cranioplasty achieved statistically significant gains in FT, SBT-P, and SBT-N. These findings support the hypothesis that dynamic expansion methods may directly influence cranial base angulation, thereby promoting greater correction of facial and orbital asymmetry. In contrast, FOAR primarily involves reshaping and advancing the frontal bone and orbital bandeau without fully addressing cranial base scoliosis, which likely explains its more modest and less durable improvements. This pattern parallels outcomes reported with FODO, another dynamic expansion method, where gradual distraction yielded more reliable correction of orbital dysmorphology and cranial base asymmetry compared with FOAR.5,22–24 Collectively, these data suggest that strategies employing controlled, progressive expansion – such as springs or distraction osteogenesis – may provide a biologically favorable and mechanically more effective approach to achieving lasting craniofacial symmetry in UCS.
A post hoc power analysis revealed resulting power values of FOAR FT = 0.609, FOAR SBT-P = .532, and FOAR SBT-N = 0.893. These results indicate that the study was sufficiently powered to detect differences in SBT-N; however, analyses for FT and SBT-P were likely underpowered due to the small sample size. A sample size estimation indicated that achieving a power of 0.8 would require approximately 10 subjects for FOAR FT and 12 for FOAR SBT-P. Consequently, the acceptance of the null hypothesis for these variables is more consistent with a type II error.
ICV expansion was assessed at different time points for each group: postoperative day 2 for the FOAR cohort and the CT scan obtained closest to spring removal (typically just prior) for the spring cranioplasty cohort. Although these ages differed significantly, they represented the most comparable imaging time points available. ANCOVA was used to account for age-related differences in growth and confirmed that, after adjusting for age, there was no significant difference in ICV expansion between the FOAR and spring cranioplasty groups. This suggests that both procedures adequately support intracranial growth. Future studies will be needed to evaluate ICV expansion at standardized, long-term intervals (>5 years), though this was not possible in the present series as most spring cranioplasty patients were younger than 5 years at the time of analysis.
Qualitative and quantitative orbital reconstructions revealed marked differences between the 2 groups. In the FOAR cohort, overlay heat maps and mirrored analyses demonstrated minimal postoperative remodeling with persistent orbital asymmetry. By contrast, spring cranioplasty patients showed substantial orbital remodeling and improved symmetry, aligning with previous reports that gradual distraction more effectively corrects orbital morphology.22,25 UCS is also well known to be associated with ophthalmologic complications, including strabismus, astigmatism, and amblyopia.12,32–35 While our spring cranioplasty cohort is still too young to assess long-term ophthalmologic outcomes, the early orbital findings are encouraging and suggest a potential for improved functional as well as esthetic results.
Common criticisms of spring cranioplasty include the requirement for 2 operations (placement and removal) and the perceived unpredictability of spring performance.8,26,36 In our experience, however, the combined operative times for spring placement and removal remain significantly shorter than those for FOAR. Concerns have also been raised regarding the potential neurocognitive effects of anesthesia exposure in infants, though it remains unclear whether total anesthesia duration or the number of exposures carries greater risk. 37 Proponents of FODO argue that springs provide less reliable distraction distances. In contrast, we have observed consistent advancement when 3 or more springs are used, likely because greater force is generated and distributed more evenly along the osteotomies, which improves the predictability of outcomes. 38
This study has several limitations. First, comparisons were made between 2 treatment groups at different age ranges, which may complicate interpretation of results. Ideally, outcomes would be compared at equivalent, long-term time points (>5 years postoperatively). Although most of our spring cohort has not yet reached this milestone, one patient with long-term follow-up demonstrated similar craniofacial morphology on CT scans obtained at the time of spring removal and again at 5 years, suggesting stability over time. Second, the study is constrained by its relatively small sample size, reflecting the rarity of UCS, and by incomplete long-term follow-up. Several patients were lost to follow-up or did not undergo CT imaging beyond 2 years, limiting our ability to fully evaluate relapse. A post hoc power analysis indicated that expansion of the study cohort will be necessary to achieve adequate statistical power and reduce the likelihood of type II error. Finally, while our morphometric and volumetric analysis incorporated detailed CT-derived 2D and 3D reconstructions, more advanced geometric morphometric methods could provide an even more comprehensive assessment of craniofacial form. Future larger-scale studies with long-term, standardized imaging and incorporation of functional outcomes, including neurodevelopmental and ophthalmologic measures, will be essential to validate and extend these findings.
Conclusion
This study directly compares spring cranioplasty and FOAR for the treatment of UCS using CT-based volumetric and morphometric analysis. Like FODO, spring cranioplasty demonstrated clear perioperative advantages, including shorter operative times, reduced blood loss, and lower transfusion requirements, while providing ICV expansion comparable to FOAR. Beyond these perioperative benefits, spring cranioplasty achieved greater improvements in FT, skull base angulation, and orbital symmetry, whereas FOAR yielded only modest changes. These findings support the growing evidence that dynamic expansion techniques more effectively influence cranial base morphology and orbital alignment than traditional remodeling approaches. While the study is constrained by small sample size, variable follow-up duration, and age differences between groups, the results suggest that spring cranioplasty is a safe and effective alternative to FOAR for UCS. Larger, long-term studies with standardized morphometric and functional outcomes will be essential to confirm durability, assess neurodevelopmental and ophthalmologic effects, and clarify the role of spring cranioplasty in modern UCS management.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656251401323 - Supplemental material for Comparison of Cranial Vault Remodeling Versus Spring Cranioplasty for Nonsyndromic Unicoronal Craniosynostosis: Analysis of Outcomes
Supplemental material, sj-docx-1-cpc-10.1177_10556656251401323 for Comparison of Cranial Vault Remodeling Versus Spring Cranioplasty for Nonsyndromic Unicoronal Craniosynostosis: Analysis of Outcomes by Sarah Anne Frommer, Sebastian Kuriakose, Patrick D. Combs, Elizabeth C. Tyler-Kabara and Patrick K. Kelley in The Cleft Palate Craniofacial Journal
Footnotes
Ethical Considerations
The study was approved by the Institutional Review Board at University of Texas at Austin under IRB # STUDY00002700 on June 16, 2022.
Consent to Participate
All participants (or their legal guardians) provided written informed consent, and data was anonymized to protect confidentiality.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Share upon reasonable request
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.