
Abstract
Background
Foot-drop impacts negatively on ability to walk and quality of life. Evidence indicates that there are benefits and drawbacks to commonly used orthotic devices: ankle foot orthoses (AFOs) and functional electrical stimulation (FES). Further exploration is needed of the foot-up brace and newly-developed ‘footwear for foot-drop.’
Objective
This study explored users’ perspectives on four devices that support foot-drop.
Method
Secondary analysis was conducted of semi-structured qualitative interview data (n = 18) collected during a prototyping process relating to new ‘footwear for foot-drop.’ Interpretative Phenomenological Analysis explored people’s experiences of different orthotic devices. Participants (Female n = 12; Male n = 6) had foot-drop due to multiple sclerosis (MS) (n = 14), Guillain-Barre syndrome (n = 1), cerebral palsy (n = 1), chronic stroke (n = 1) or post spinal surgery (n = 1).
Results
Positive and negative experiences were reported for the functionality and design features of each device. Decision-making about device use was affected by foot-drop severity, personal preferences and context of use. Ease of use, comfort and appearance of devices were valued by participants.
Conclusions
Enhanced insights into different device options will support more informed, person-centred decision-making for device-users and prescribers. This may reduce device abandonment, improving experiences and outcomes. Study findings support the need for further research into the foot-up brace and ‘footwear for foot-drop.’
Keywords
Introduction
Foot-drop describes a symptom of different health conditions where people find it difficult to ensure that their toes clear the ground when walking. This makes walking more effortful, both physically and mentally. People need more concentration and energy to use strategies like lifting their hips and knees up further and/or swinging their affected leg out to avoid tripping.1,2 Fear of falling can lead to avoidance of physical activity and becoming less able to take part in social and working roles, reducing health and wellbeing.1,2
In studies of people attending foot-drop clinics, it is most commonly caused by nerve damage in the lower back and legs. People also develop foot-drop due to neurological conditions, including stroke, multiple sclerosis, cerebral palsy and motor neurone disease.3–5 Overall prevalence of foot-drop is not known, 3 although approximately 20% of people with stroke develop it. 6 More research is needed into how many people have foot-drop more generally, and why. Due to its negative impacts and chronic nature, orthotic devices are often prescribed to people with foot-drop.
Frequently prescribed orthotic devices include ankle foot orthoses (AFOs) and functional electrical stimulation (FES), with the former being the most available option in the UK National Health Service.2,7 There are different AFO designs available, some of which are rigid and restrict movement at the ankle, while others are hinged or dynamic and permit some movement.8,9 FES consists of applying electrodes to the common peroneal nerve that stimulate the tibialis anterior muscle to generate ankle dorsi-flexion at the right point in the gait cycle. 2 Both devices have been shown to improve gait and reduce the risk of falls. 7
Regarding the effectiveness of both devices to support foot-drop, previous quantitative studies have shown that they improve temporal and spatial parameters for mobility such as increasing gait speed and reducing the risk of falls.10,11 Qualitative studies have shown that both devices appear to provide similar benefits for improving gait, increasing independence and social participation, reducing the risk of falls and in turn, potentially improving quality of life for individuals living with foot-drop.2,10 Despite these advantages, analysis also highlighted drawbacks with the use of these devices. 2 Users report devices to be cumbersome, restrictive, difficult to apply or conceal, and limiting some activities. 2 These findings are congruent with the results shown by a recent systematic review and meta-synthesis of qualitative studies, 1 further highlighting limitations with regard to the aesthetic, comfort, ease of use and psychosocial implications of wearing devices to support foot-drop.
Further devices have been developed in response to this need, including the foot-up brace, 12 which involves anchor points inserted into the upper of the shoe and attached to the ankle that are joined by a strap that provides support for the tibialis anterior muscle. There is currently a lack of research into this device. More recently, ‘footwear for foot-drop’ 12 has been developed, which incorporates support for the tibialis anterior muscle through elastic straps that cross diagonally across the upper of the shoe, anchored within the footwear at the ankle and distal section of the sole. Research evaluation of this prototype device is underway. 13
It is important to understand user perspectives regarding such devices and influences on their choices. There is a risk that people stop using devices which do not sufficiently meet their needs, with both safety and cost implications. People who need to use an orthotic device will be safer and less likely to fall if they do so, with implications for their wellbeing and for health service costs due to reduced fall rates and device wastage, as well as greater physical activity participation.14–16 In response, this study aimed to explore user experiences of AFOs, FES, foot-up braces and ‘footwear for foot-drop.’
Methodology
Secondary data analysis was used to address the study aims, using qualitative data collected during a device prototyping process. A favourable ethical opinion was provided by the Queen Margaret University Ethics Committee [17/2/2021]. During the development of the prototype ‘footwear for foot-drop,’ 18 semi-structured qualitative interviews were conducted. These interviews were designed with the aim of exploring people’s experiences of foot-drop and its impacts on their lives, devices they have used and their views on these devices (including the novel ‘footwear for footdrop’) and the aspects of a device that they view to be most important. A Constructivist Phenomenological approach was taken in this secondary analysis, seeking to explore perceptions and lived experiences in participants’ own words, with recognition of the co-construction of insights through the interactive data collection and analysis processes. 17 It is important to convey the context of this process to enable the reader to decide whether findings are transferable to their context and understand trustworthiness of the analysis.
Data were collected by CB who had no relationship with any of the participants prior to the study. The primary research team members (CB, DS, KJ, GW) have been actively involved in research into all the devices mentioned and are invested in exploring the best devices for different people and purposes, rather than solely exploring the novel device. Due to the fact that the primary research team are involved in the development of ‘footwear for foot-drop,’ an additional team conducted the secondary data analysis with supervision (CK, NB, NC, SH). They were students in physiotherapy with insights into the health conditions experienced by participants, but no vested interest in the performance of different devices. The secondary data analysis team were supported to understand the nature of the study and received supervision throughout the data analysis process from two team members with expertise in qualitative analysis (CB, KJ). This supervision focused on the process rather than influencing the findings, supporting rigour. Data were fully anonymised before they were made accessible for secondary analysis.
Original study inclusion and exclusion criteria.
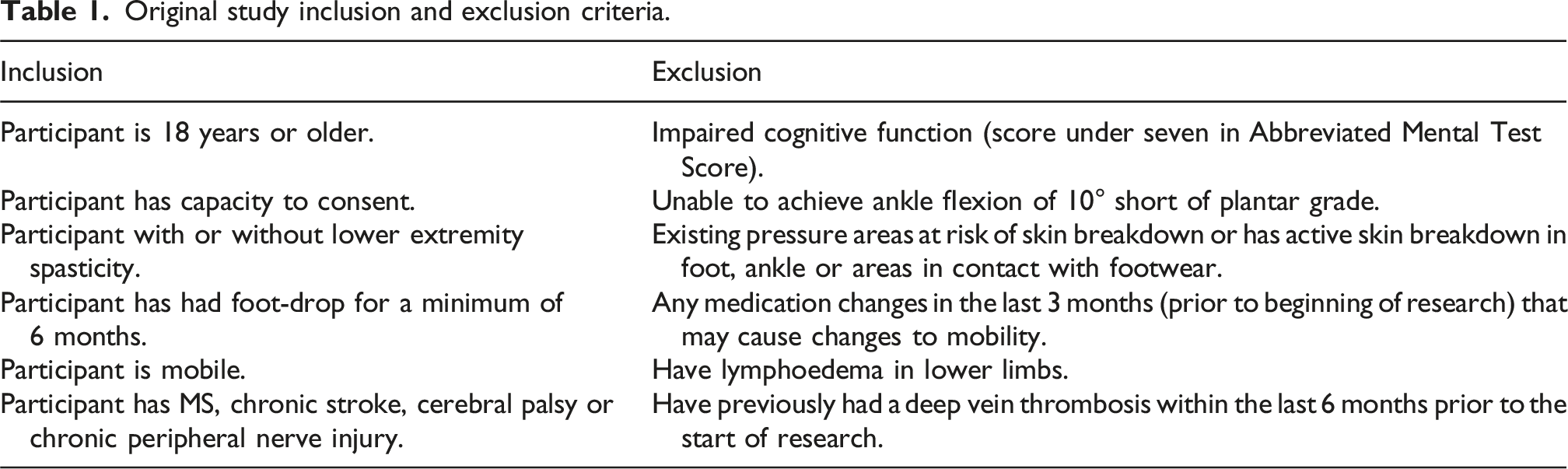
Interviews made flexible use of a semi-structured topic guide (see Supplemental File A), ensuring that participants were able to lead the conversation and unexpected insights could emerge. Questions related to the study aims listed above, ensuring insights about how people’s lives were affected by their foot-drop, how they made use of and made decisions about orthotic devices, and what they found most important when thinking about whether or not to use an orthotic device. Participants discussed only the devices they had previously used, and all had worn the novel ‘footwear for foot-drop’ for at least 1 week prior to undertaking interviews. All interviews were audio-recorded, transcribed, anonymised and stored securely for analysis.
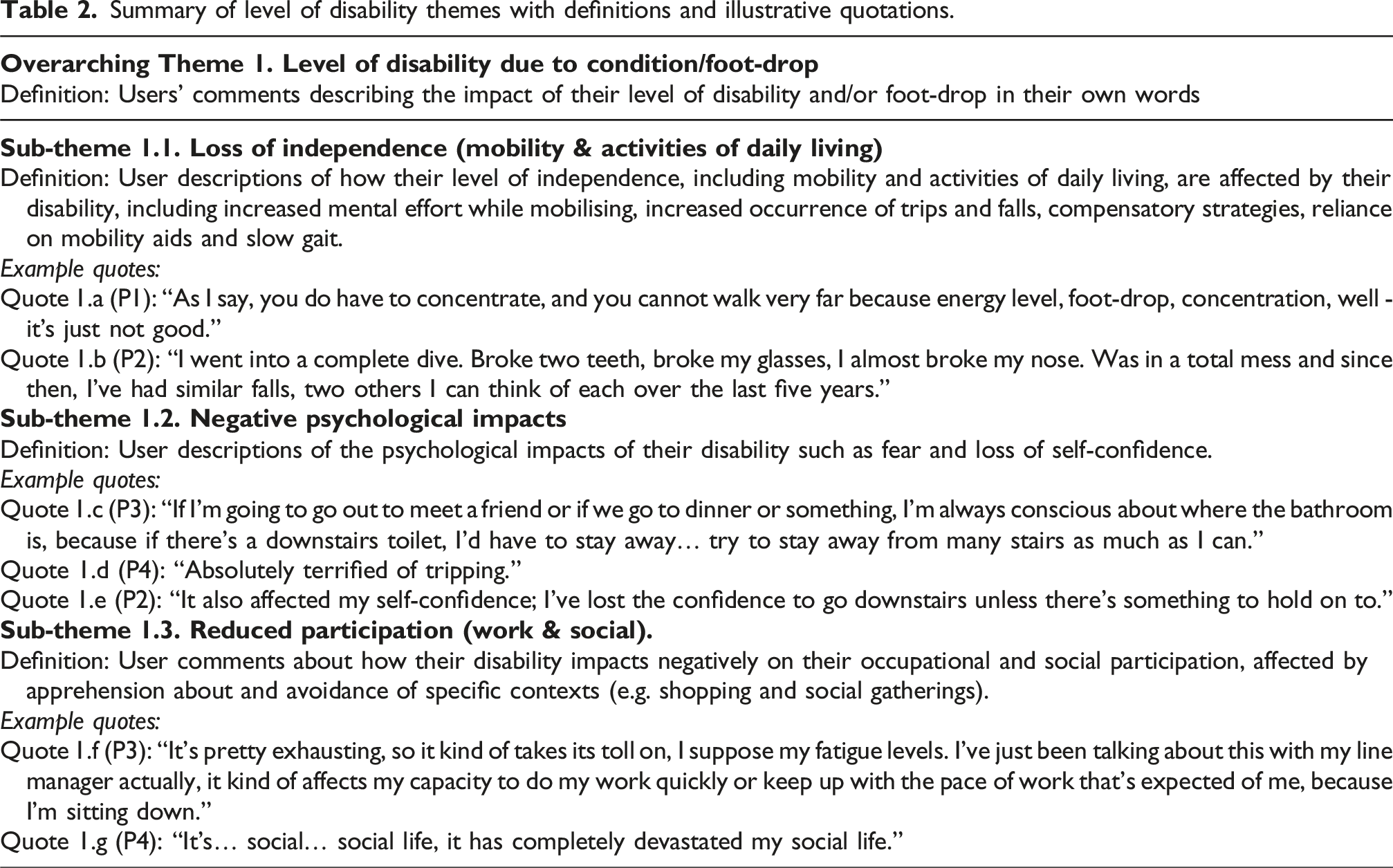
Interpretative phenomenological analysis (IPA) was used to enable rich insights into the experiences and perceptions of participants. It involves a double hermeneutic process where the researcher attempts to formulate an understanding of how participants make sense of a phenomenon. 18 Preconceptions are noted and set aside to enable an inductive approach to exploring the data and subsequently generating insights. 19 Training in this process was provided by an experienced researcher (CB). Case-by-case analysis and cross-case analysis were conducted, starting with in-depth reading of two transcripts by all four analysts and exploratory note taking. Through discussion, the team grouped statements with similar meaning to develop draft themes and sub-themes. These were given a label and definition. To illustrate this process: when asked about how foot-drop affected the person, one participant responded “It also affected my self-confidence; I’ve lost the confidence to go downstairs unless there’s something to hold onto.” This influenced formation of a sub-theme called ‘Negative psychological impacts’ and other such comments were then coded to this sub-theme. At the next stage, relevant sub-themes were grouped that all addressed a person’s level of disability due to foot-drop and/or the condition causing their foot-drop, forming an overarching theme. Themes and sub-themes were primarily descriptive, focusing on ways that people made sense of their experience. A further, more interpretative layer of analysis identified linkages between these themes and sub-themes, for example, regarding influences of the severity of a person’s disability on choices relating to device use. As analysis progressed, the team found it useful to use terminology from the International Classification on Functioning Disability and Health (ICF) framework where appropriate. 20 Additional themes were identified regarding device-specific themes such as design features and functionality.
The remaining transcripts were individually analysed with cross-checking of analysis between team members, and the theme table refined through team discussion. This final table of themes, sub-themes and their definitions was then used to repeat the analysis of each transcript, leading to a final table of themes with definitions and all supporting data (see Supplemental File B to provide access to underlying data without compromising participant privacy).
Results
Eighteen people consented to participate and completed interviews (Females n = 12; Males n = 6). Their mean age was 58 years (range of 34–76 years). The reasons provided for participants’ foot-drop were Multiple Sclerosis (MS) (n = 14), the peripheral nerve condition: Guillain-Barré syndrome (n = 1), Cerebral Palsy (n = 1), Chronic Stroke (n = 1) or post spinal surgery nerve injury (n = 1). More people had unilateral foot-drop (n = 14) and four people had bilateral foot-drop. All participants had utilised the ‘footwear for foot-drop’ due to the context of data collection, while 14 had also used AFOs previously, 16 had used the foot-up brace and 12 had used FES. Interviews lasted 34 min on average, ranging from 20 to 58 min.
Three overarching themes emerged: 1. level of disability due to condition/foot-drop; 2. Device comparison (positive aspects); and 3. Device comparison (negative aspects). The interplay of factors which influence device use was then explored.
Theme 1. Level of disability due to condition/foot-drop
Summary of level of disability themes with definitions and illustrative quotations.
Theme 2. Device comparison (positive aspects)
Summary of positive aspects of devices (design features and functionality) with definitions and illustrative quotations.
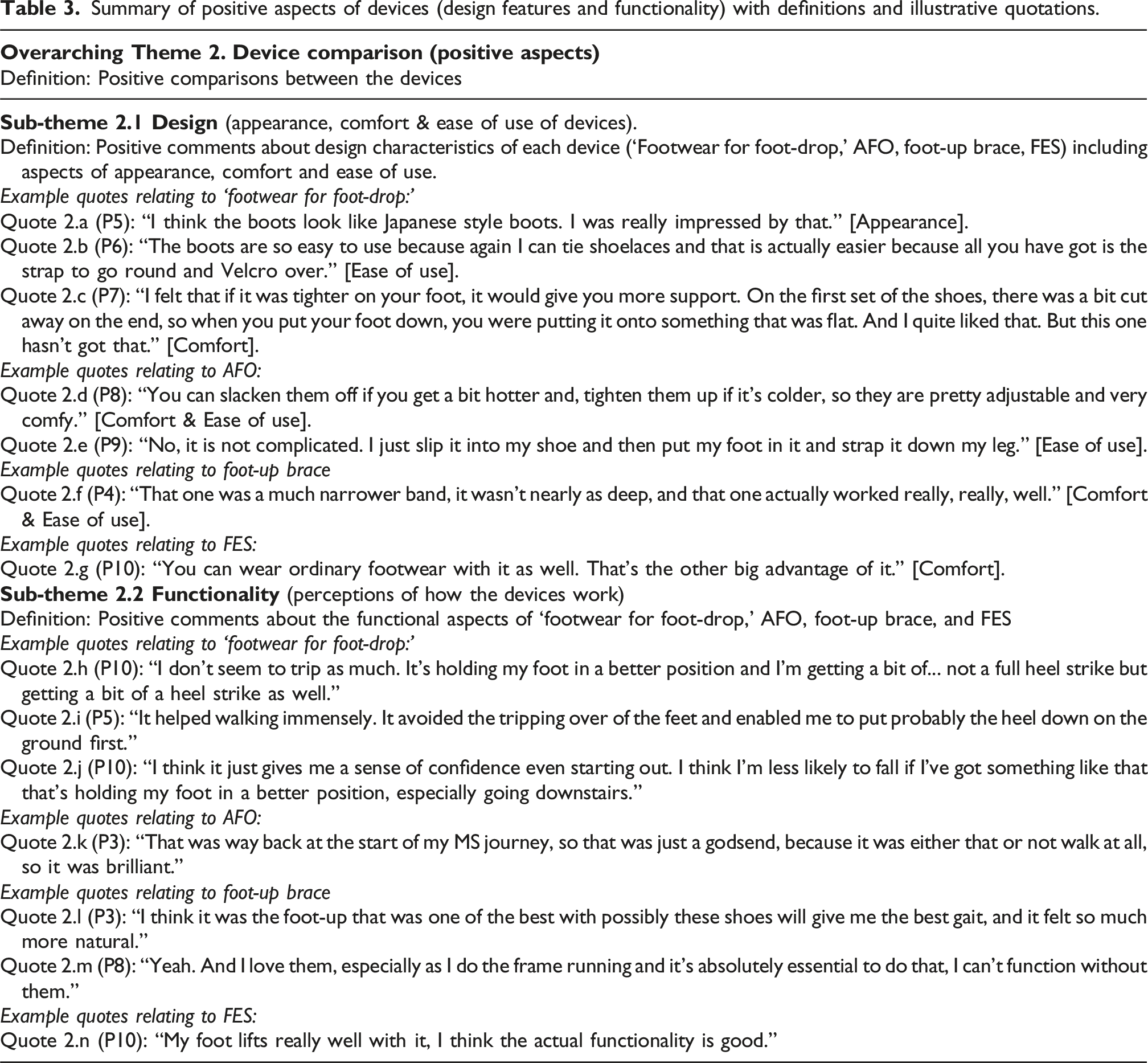
Regarding the functionality of devices, multiple benefits were reported by participants, including positive impacts on mobility, independence, performing functional tasks, reducing the risk and fear of falls and increasing confidence and social participation (Table 3: quotes 2.h; 2.i; 2.j; 2.k; 2.l; 2.m; 2.n). The ‘footwear for foot-drop’ was highlighted as increasing confidence and reducing fear and risk of falls when performing functional tasks such as descending stairs or mobilising (quotes 2.h; 2.i; 2.j). The foot-up brace was described as facilitating social participation in sporting activities (quote 2.m). There were more reports of the ‘footwear for foot-drop’ (quotes 2.h; 2.i; 2.j) and AFO (quote 2.k) being psychologically beneficial, in contrast to the foot-up brace and FES.
Theme 3. Device comparison (negative aspects)
Summary of negative aspects of devices (design features and functionality) with definitions and illustrative quotations.
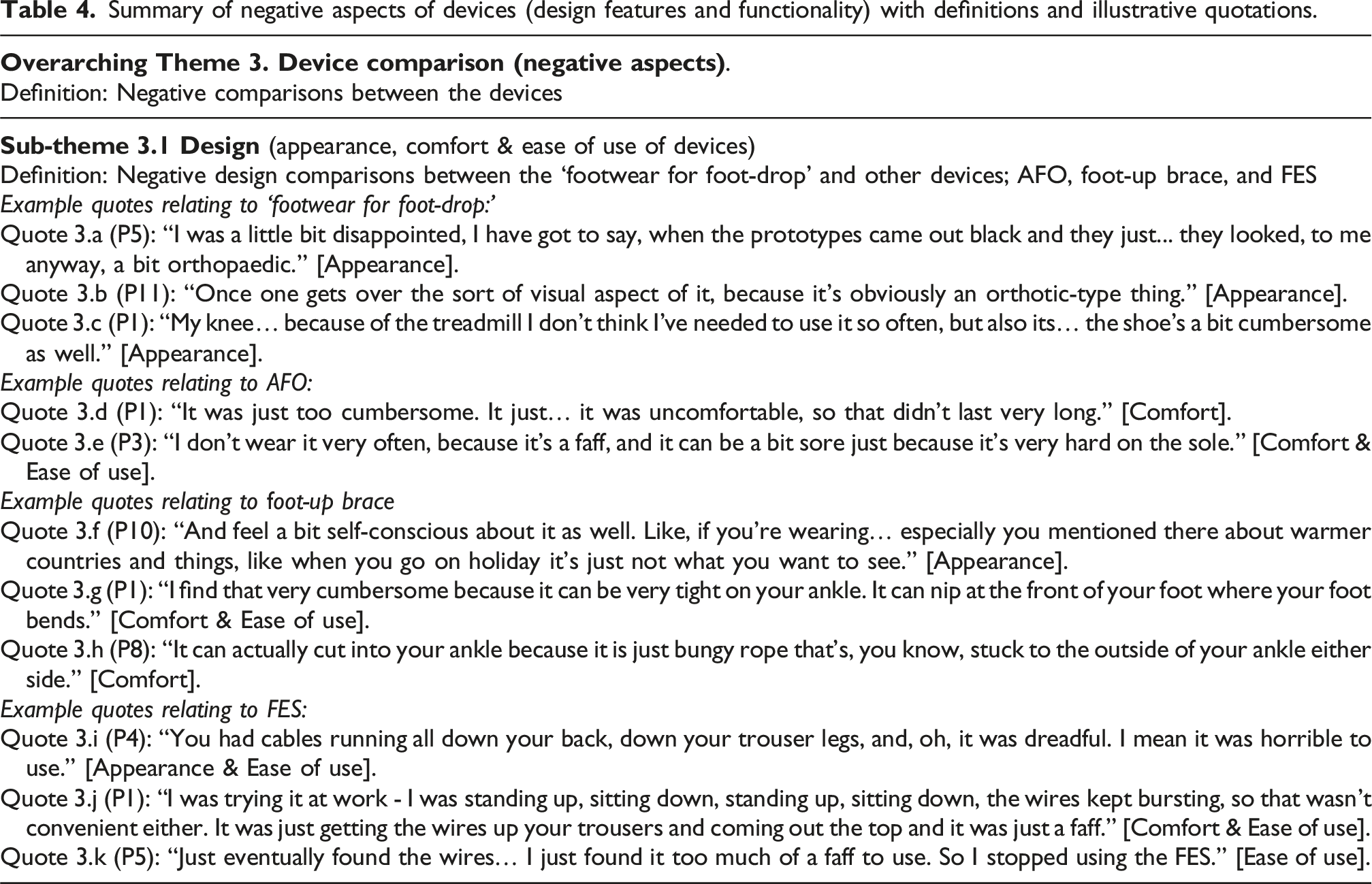
Regarding functionality of devices, numerous negative aspects of device utilisation were reported by participants, including limitations on independence and participation and negative psychological experiences (Table 4: quotes 3.l; 3.m; 3.n; 3.o; 3.p; 3.q). AFOs were criticised for restricting ankle range of motion, limiting independence and participation and causing emotional stress (quotes 3.m; 3.n). The foot-up brace was described as posing a barrier to independence, including when driving (quote 3.o). The ‘footwear for foot-drop’ was found to be uncomfortable by some, with impacts on mobility (quote 3.l).
Interplay between factors which influence device use
Participants’ explanations of their views and experiences enabled interpretation of ways in which themes and sub-themes interlinked. Figure 1 illustrates an interplay between influences on device use, including intrinsic factors that related to level of disability and severity of foot-drop, and extrinsic factors that related to aspects of the device such as appearance, ease of use, comfort and functionality. Illustration of Interplay between intrinsic and extrinsic influences on device use.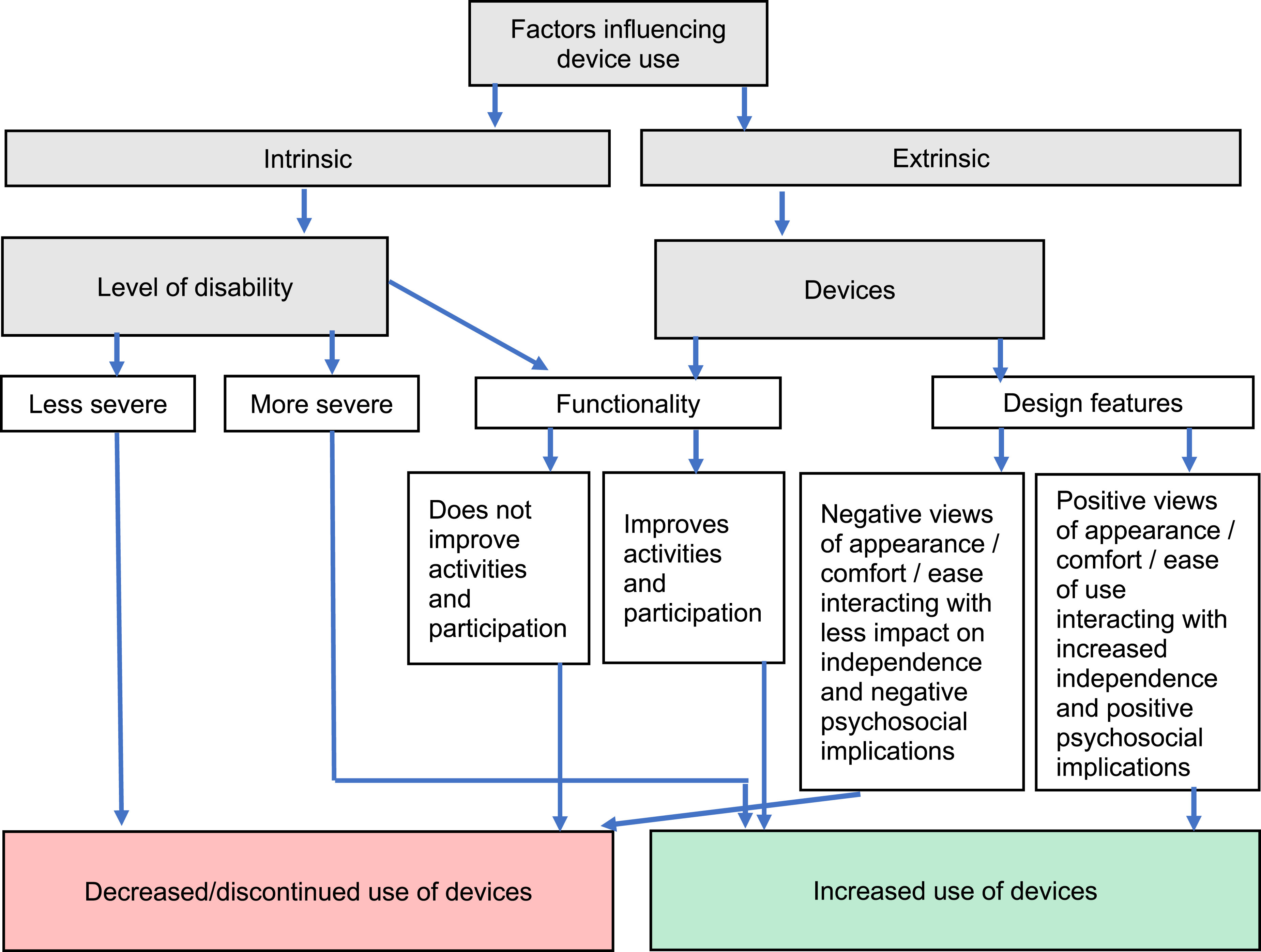
Regarding the interaction between level of disability and devices, Participant 1 (Table 4: quote 3.c) explained that having less severity of foot-drop reduced their dependence on devices and their functionality. Participant 3 described how their more severe mobility difficulties meant they relied on the functionality of a device (AFO) greatly: “that [AFO] was just a godsend, because it was either that or not walk at all, so it was brilliant (AFO)” (Table 3: quote 2.k).
Illustrating interactions between design features and psychosocial implications of device use, Participant 10 explained that the appearance of a device (AFO) influenced their self-image when socialising: “And feel a bit self-conscious about it as well… when you go on holiday it’s just not what you want to see” (Table 4: quote 3.f). For some people this may reduce the likelihood of using the device. Participant 3 explained that they stopped using an AFO due to negative experiences regarding ease of use and comfort (Table 4: quote 3.e, P3). Interaction between device comfort and independence was found for the foot-up brace, with Participant 12 explaining that they didn’t like to use this device for driving as a result (Table 4: quote 3.o).
Interactions between intrinsic and extrinsic factors may also influence use of devices, with severity of disability impacting on how much people are willing to tolerate their drawbacks.
Discussion
This study aimed to explore user experiences of AFOs, FES, the foot-up brace and ‘footwear for foot-drop.’ Analysis of participants’ responses led to the identification of two emergent concepts. These concepts were: “Design features” which encapsulates appearance, comfort and ease of use of devices, and “Functionality” which includes how devices impact on people’s activities, participation and psychological well-being.
It is important to note that all devices had positive impacts on individuals in this study, reflecting positive perceptions of their functionality. Participants described negative impacts of foot-drop such as fear of falls, fatigue and loss of confidence. FES and AFOs supported greater mobility, independence and participation, aligning with findings of previous studies.1,2,10,18–23 Functional benefits of the foot-up brace and ‘footwear for foot-drop’ included improved gait, reduced risk of falls and increased confidence. These are novel findings and support further research and development focusing on these devices.
Focusing on design features, participants reported both positive and negative experiences of AFOs and FES. On balance, more negative comments were reported, such as AFOs and FES being cumbersome, unattractive, restrictive, uncomfortable and having poor ease of use. This may reflect the participants as people who were willing to try a new device, potentially due to some dissatisfaction with others that they had tried. People who were finding their existing device appropriate may not have decided to take part in the prototyping process for the ‘footwear for foot-drop.’ The critical comments do, however, align with those in previous qualitative studies,1,2,24 one of which found that difficulties concealing AFOs could pose limitations for the use of the device during social participation. 2 Similarly, a participant in the current study explained that the appearance of AFOs made them self-conscious when socialising (quote 3.f, P10) (Table 4). It seems evident that the appearance of devices may have psychosocial significance for those with foot-drop and other physical disabilities.
The use of assistive technology and fear of stigmatisation have long been established as posing psychosocial difficulties for people living with physical disabilities.25–27 People may experience discrimination or feel excluded from society as a result of their impairment or condition. 27 This can negatively impact on self-esteem and psychological well-being, as shown in a qualitative study interviewing 14 individuals living with acquired chronic and complex neurological conditions. 26 This is not always the case, however, as one qualitative study 28 found that positive integration of a physical condition or impairment into one’s sense of identity is possible. They found this among participants who used FES to help them adjust to life with foot-drop, showing that devices can play an important part in a person’s adjustment to disability. This is likely to be affected by a person’s acceptance of a device; which is likely to be influenced by personal preferences in relation to its design features. 2
The interplay between intrinsic and extrinsic influences on decision-making about device use (Figure 1) suggested that design features are key. For example, two participants (Table 4: quotes 3.e; 3.k) explained that they stopped using or reduced their use of AFOs and FES because they were not easy to use. In one study, 28 experiences of people who used FES for foot-drop were analysed to develop a similar model of the relationships between influences on device use. They suggested that decision-making is multi-faceted, with numerous considerations, including personal autonomy, relationship with the device and positive or negative experiences of the device. Some people may prioritise ease of use, while others may place a high priority on the appearance of the device. 27 Assistive devices may possess negative symbolism for the person, who may feel that they draw attention to their disability and expose them to stigmatisation. The person may, as a result, stop using the device. 27 In the case of foot-drop, this is likely to leave them open to greater risk of trips, falls, and injury. Clearly a person’s preferences are key to ongoing usage and related function and safety.
The study findings raise the importance of person-centred practice, highlighting that what is meaningful and matters most to patients should be at the centre of treatment. 29 In this context, providing device alternatives with varying design features is important to help avoid fear of stigmatisation and device abandonment. Further research into the potential for the foot-up brace and ‘footwear for foot-drop’ as options is warranted, as there were more positive perceptions of the design features of these devices (Table 3). It would be valuable for prescribers to educate themselves on the advantages and disadvantages of devices and use this information in conversations with people during the prescription process. There is a risk that people are provided with the device that is most readily available, rather than one that is most appropriate for the individual’s impairment or circumstances. Availability may be more influenced by awareness of the provider, and/or cost of the device. It would be valuable to create a decision-aid that supports providers. This should address functionality by considering the range of manifestations of foot-drop (e.g. with or without spasticity) and give guidance about who might benefit from each device. Alongside functionality, however, any decision aid should also incorporate flexibility and acceptance regarding social and psychological influences on people’s device choices. This would support more person-centred practice, which is more likely to lead to prescription of a device which suits the needs of individuals and which they continue to use.
When considering applying the results of this study, it is important to be aware of the potential for bias and the measures taken to manage this. The primary research team has interest in all the devices explored in the study but is invested in developing novel ‘footwear for foot-drop’ as an option for people with foot-drop. In order to manage the potential bias, they involved a secondary research team, however, they had less experience of qualitative research. Supervision of the steps in analysis was provided to increase their skills 30 without influencing the findings, supporting analytical autonomy. The analysis team took measures to increase consistency in their development of themes and use of these themes to analyse each transcript.
Conclusion
Exploration of users’ experiences in the use of various devices to support foot-drop highlighted that individuals require different options. Their decisions regarding which device to use are affected by the severity of their foot-drop, personal preferences and context of use. Having options for device use will support person-centred practice, as different devices possess various advantages and disadvantages which will be prioritised differently by each person. All devices were reported to improve gait, independence and participation. Further research is required to examine the functionality and design features of the foot-up brace and ‘footwear for foot-drop’ as less researched and novel devices to support foot-drop.
Supplemental material
Supplemental Material - Devices for foot-drop: Qualitative exploration of functional electrical stimulation, ankle-foot orthoses, foot-up braces, and footwear for foot-drop
Supplemental Material for Devices for foot-drop: Qualitative exploration of functional electrical stimulation, ankle-foot orthoses, foot-up braces, and footwear for foot-drop by Cathy Bulley, Christopher Kelly, Niamh Buchan, Niall Cowie, Sarah Hellicar, Kavi Jagadamma, Derek Santos, and Gillian Wilson in Technology and Disability.
Supplemental material
Supplemental Material - Devices for foot-drop: Qualitative exploration of functional electrical stimulation, ankle-foot orthoses, foot-up braces, and footwear for foot-drop
Supplemental Material for Devices for foot-drop: Qualitative exploration of functional electrical stimulation, ankle-foot orthoses, foot-up braces, and footwear for foot-drop by Cathy Bulley, Christopher Kelly, Niamh Buchan, Niall Cowie, Sarah Hellicar, Kavi Jagadamma, Derek Santos, and Gillian Wilson in Technology and Disability.
Footnotes
Acknowledgements
We gratefully acknowledge the support of all study participants.
ORCID iDs
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki and a favourable ethical opinion was provided by the Queen Margaret University Ethics Committee [17/2/2021]. Written informed consent was provided by all participants.
Author contributions
Conception: Cathy Bulley, Kavi C Jagadamma, Derek Santos, Gillian Wilson; Data collection: Cathy Bulley; Data analysis and interpretation: Christopher James Kelly, Niamh Buchan, Niall Cowie, Sara Hellicar, with method supported by Cathy Bulley; Preparation of the manuscript: Cathy Bulley, Christopher James Kelly, Niamh Buchan, Niall Cowie, Sara Hellicar; Revision by all.
Funding
The secondary analysis did not receive funding; while the original data was partially supported by a Queen Margaret University Innovation Fellowship.
Declaration of conflicting interests
Four authors (CB, KJ, DS, GW) are founding directors of the Health Design Collective, a spin-out social enterprise company that has developed innovative ‘footwear for foot-drop.’ This is one of the devices explored in this article and further researchers were involved to ensure analysis was unbiased.
Data Availability Statement
All themed data are provided in Supplemental File 1. Ethical approval did not allow the authors to upload full interview transcripts due to risk of loss of anonymity due to combined data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.