
Abstract
Rationale
Assistive technologies play a vital role in palliative care by addressing physical, emotional, and social needs. Despite their growing relevance, a comprehensive understanding of their purposes, the methodologies used to study them, and the populations they serve remain limited.
Objective
This scoping review aimed to explore the purposes of assistive technologies in palliative care, examine the methodologies employed in their study, and identify the target populations they serve.
Methods
A systematic search was conducted in five databases: PubMed, ScienceDirect, CINAHL, Web of Science, and IEEE Xplore. The search terms focused on “assistive technology” and “palliative care,” and were restricted to original research published between 2000 and 2024. Studies were screened using predefined inclusion and exclusion criteria, and data were extracted from the selected publications to address the research questions.
Analysis
The review identified 12 relevant publications. Assistive technologies were found to address diverse purposes, including symptom management, monitoring, communication, and psychosocial support. Methodological approaches varied widely, encompassing qualitative, quantitative, and mixed-methods designs. Target populations included older adults, individuals with neurodegenerative diseases, cancer patients, and young individuals with rare conditions, with applications across diverse care settings and palliative care stages. However, the limited number of publications suggests potential knowledge gaps, highlighting the need for broader search strategies and increased recognition of assistive technologies in palliative care research.
Introduction
Assistive technology (AT) is defined as a wide range of tools and devices that are designed to enhance the functional capabilities of individuals with disabilities or special needs, thereby promoting independence and improving quality of life. 1 In the context of healthcare, particularly in palliative care, a crucial role is played by AT in supporting patients by facilitating communication, managing symptoms, and enhancing overall well-being.2,3
Palliative care is characterized as a specialized area of healthcare that focuses on providing relief from the symptoms and stress of serious illness, with the primary goal of improving the quality of life for both patients and their families. 4 The World Health Organization defines palliative care as an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other physical, psychosocial, and spiritual problems. 5 This holistic approach is supported by various sources, which emphasize the importance of addressing not only the physical aspects of care but also the emotional, social, and spiritual needs of patients.6,7
It has been indicated by research that effective palliative care involves a multidisciplinary team that collaborates to address the complex needs of patients, which often includes the integration of technology to enhance care delivery.8,9 The incorporation of assistive technologies is believed to facilitate better communication among healthcare providers and patients, optimize symptom management, and ultimately improve patient satisfaction and outcomes.
AT has the potential to play a significant role in palliative care practices by addressing various needs of patients and supporting caregivers. The initial motivation for this scoping review was to examine whether the term “assistive technology” is widely recognized and commonly explored within the field of palliative care, providing insight into its prominence and relevance in academic and clinical discourse. The review was subsequently conducted to systematically explore how AT is utilized in this context and to provide an overview of its integration into palliative care. It seeks to identify the diverse applications of AT, outline its potential benefits for patients and families, and examine opportunities for enhancing its use in palliative care settings.
Method
In the initial phase of the review, a protocol was developed to guide the process. The protocol was designed to define the rationale, research questions, and planned methods, ensuring a systematic and transparent approach. By preparing the protocol prior to the commencement of the review, adherence to a structured methodology was facilitated, minimizing bias and enhancing reproducibility. This approach aligns with the scoping study framework proposed by Arksey and O’Malley, 10 which emphasizes methodological rigor and transparency in the planning and execution of scoping reviews.
To identify potential gaps in the use of assistive technology within the domain of palliative care, the following research questions were developed. These questions are aligned with the What-Who-How approach, while recognizing the inherent complexities in comprehensively addressing all relevant dimensions: (1) What are the purposes of assistive technologies in palliative care? (2) How were the studies on assistive technologies in palliative care conducted? (3) Who were the target groups for assistive technology interventions in palliative care?
The literature search was conducted using the databases PubMed, ScienceDirect, CINAHL, Web of Science, and IEEE Xplore. A consistent core search strategy was applied across all databases, with adaptations made to align with the specific Boolean syntax requirements of each platform (e.g., use of AND and OR operators). The search terms required references to “assistive technology” (without alternatives) and “palliative care,” which included alternative phrases to capture a broader scope, namely, “hospice care,” “end-of-life care,” “supportive care,” “terminal care,” and “dying patients.”
Where possible, database settings were configured to: Limit the search time frame to publications between 2000 and 2024. Restrict results to original research articles, excluding review papers and non-research literature.
The detailed search terms, including the full list of alternative phrases for “palliative care,” are provided in the appendix. This systematic approach ensured comprehensive coverage while maintaining consistency across databases.
The identified studies from the systematic literature search were screened based on predefined inclusion and exclusion criteria to ensure relevance and quality. These criteria were applied to refine the results and focus on studies addressing assistive technologies in palliative care, as outlined below.
Inclusion criteria
• The paper contains any of the valid combination of the defined search terms. • The paper was published between 2000 and 2024. • The study involves original research, including randomized controlled trials, observational studies, qualitative or quantitative studies, or mixed-methods research.
Exclusion criteria
• The paper discusses drugs. • The paper focuses on the effect, development, or use of pharmaceutical drugs. • The paper is a review article, guideline, commentary, or policy document. • The paper is a conference proceeding (excluded to prevent double counting with related full journal publications). • The full text of the paper is not accessible. • The paper is not written in English.
To support a structured and transparent screening process and to help minimize potential bias, three reviewers (Reviewers A, B, and C) were involved at different stages of the scoping review. Following the application of inclusion and exclusion criteria, the literature search results were processed and analyzed using a structured and systematic approach. The search results were exported as citation files and imported in a reference manager software. Duplicates were identified and removed by Reviewer A. To ensure compatibility and accessibility for all reviewers, the cleaned list of citations was exported to two separate spreadsheets. In their respective copies, Reviewers A and B independently screened the titles and abstracts based on the predefined inclusion and exclusion criteria.
In cases where the categorization by Reviewers A and B differed, Reviewer C acted as an adjudicator to resolve disagreements. For the publications that passed this initial screening, the full-text papers were independently analyzed by Reviewers A and B to confirm eligibility. During this stage, data were extracted from each publication, including: • Name and Year of Paper • Publication Year • Geographic Region • Type of Publication • Study Design • Focus of the Study • Outcomes Measured • Demographics (Age Groups and Gender) • Clinical Conditions • Care Settings • Palliative Care Stage • Purpose of Technology • Type of Technology • Stage of Development • Usability and Customization
Any conflicting categorizations during the full-text analysis were again resolved by Reviewer C.
Results
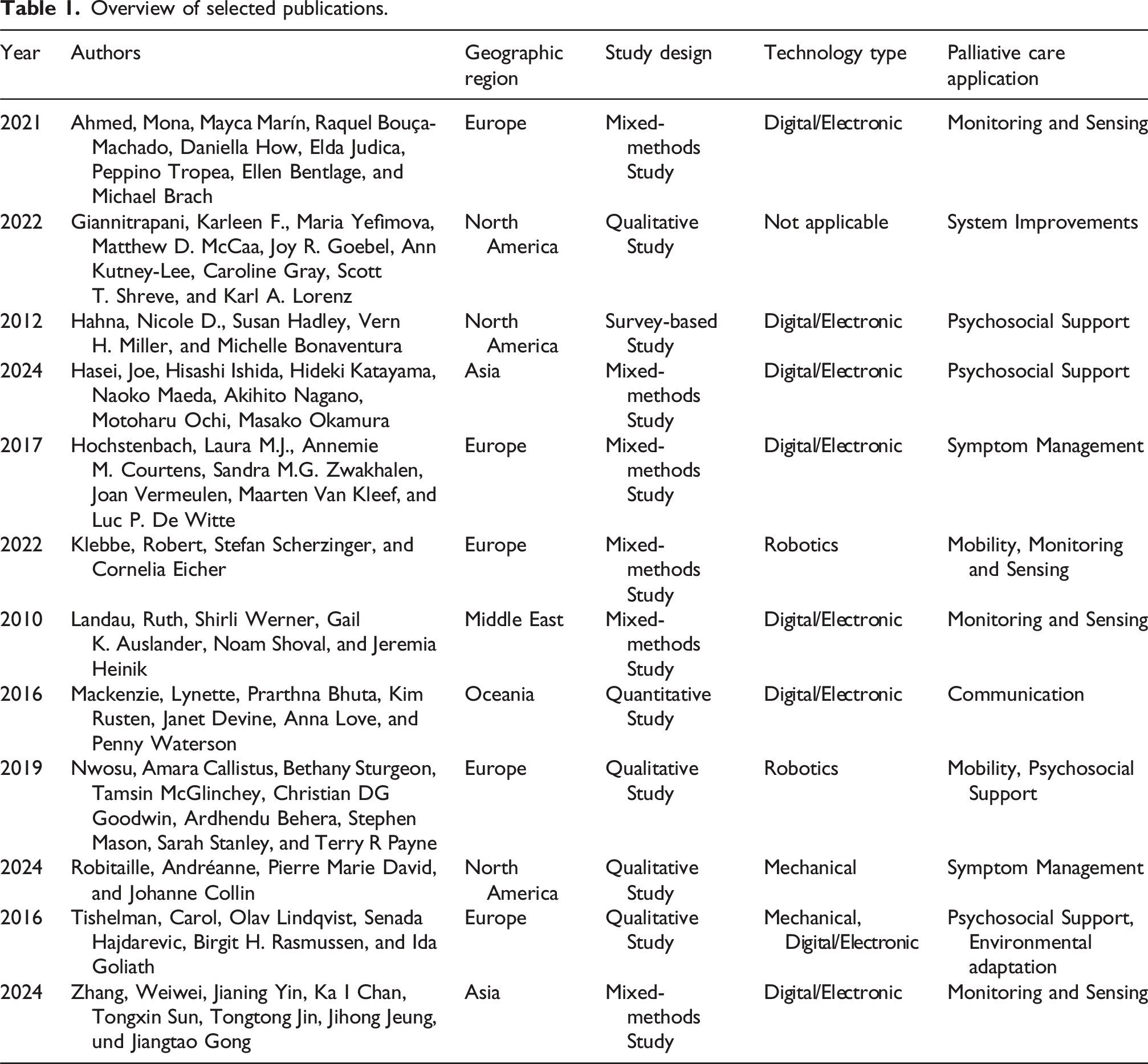
The database search yielded a total of 256 results (ScienceDirect: 203, IEEE Xplore: 0, PubMed: 7, CINAHL: 38, Web of Science: 8). After duplicates were removed, 247 unique records remained and were screened by the reviewers. This screening process resulted in 24 publications being selected for full-text analysis. Following the consolidation of the full-text review, 12 publications were included in the final analysis.11–22
The publication years vary between 2010 and 2024. See Figure 1 and Table 1. Flowchart to illustrating the study selection. Overview of selected publications.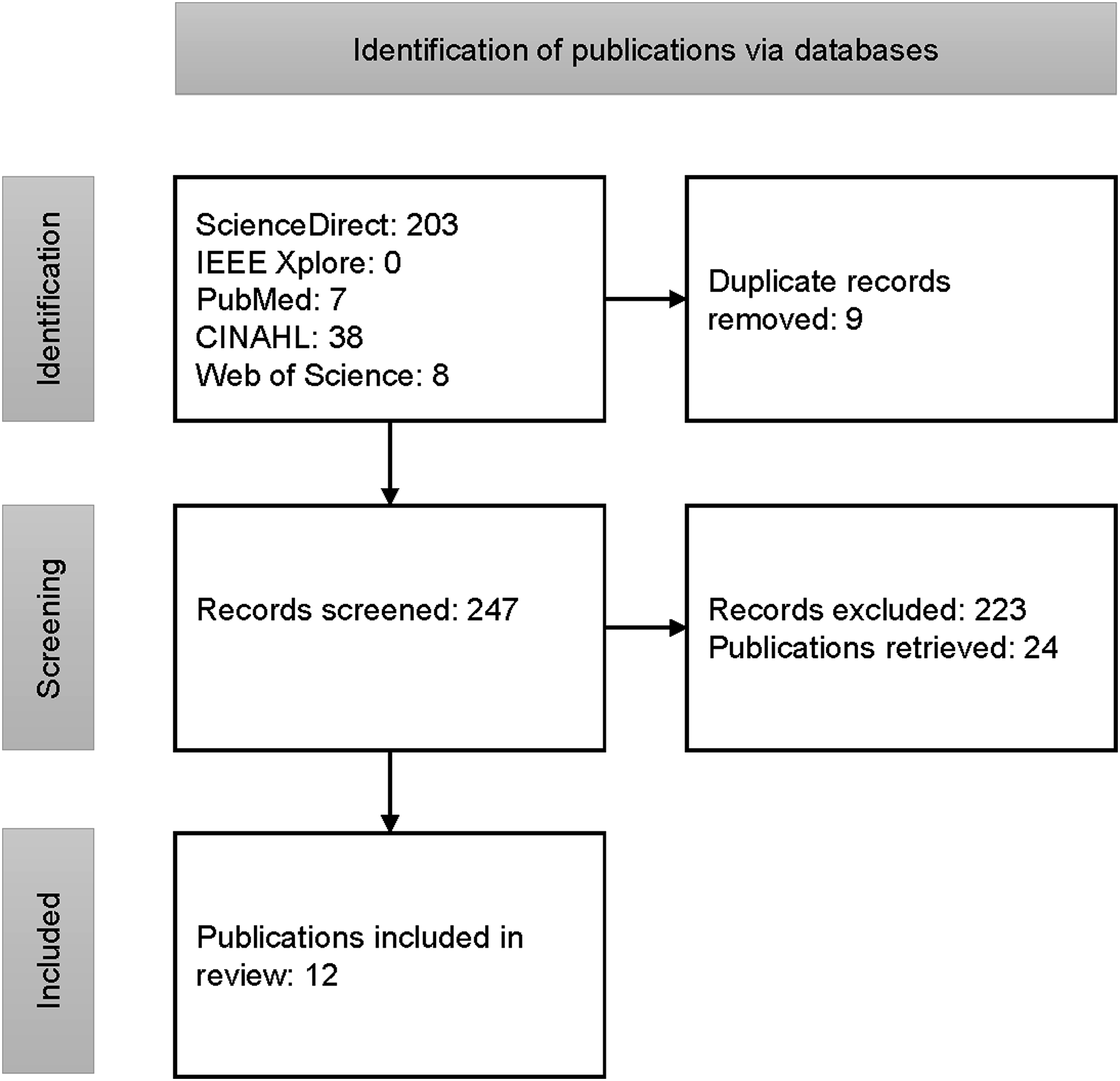
In the following, the three questions defined in the method section are addressed.
What are the purposes of assistive technologies in palliative care?
Publications reveal a variety of ways in which assistive technologies address the needs of palliative care. These technologies serve purposes ranging from symptom management and monitoring to psychosocial support and communication, with specific examples provided by the analyzed studies.
Assistive technologies are frequently used to manage symptoms and improve patient comfort. For instance, Robitaille et al. 20 describe the use of elastomeric infusion pumps to manage respiratory distress during pandemics, ensuring dignity in end-of-life care. Similarly, Hochstenbach et al. 15 highlight an eHealth system designed for cancer pain self-management, showcasing its utility in alleviating symptoms and empowering patients.
Monitoring technologies play a crucial role in ensuring patient safety, autonomy, and care quality. Zhang et al. 22 describe privacy-oriented fall detection cameras, designed to enhance safety while addressing concerns about patient privacy in home-based care. Klebbe et al. 16 focus on customized robotic systems for ALS patients, demonstrating their ability to enhance autonomy and provide essential physical support. Ahmed et al. 11 contribute further by presenting an integrated care platform for patients with neurodegenerative diseases, aimed at improving care coordination and usability.
Psychosocial support is another critical function of assistive technologies in palliative care. Hasei et al. 14 illustrate how the metaverse can provide emotional support and reduce anxiety for young patients with rare cancers, showing the innovative potential of virtual environments. Tishelman et al. 21 explore how photographic elicitation can be used to enhance well-being, identity, and social integration for end-of-life patients. Giannitrapani et al., 12 for example, focus on family narratives to identify areas for quality improvement in end-of-life care practices. Music therapy technologies, as discussed by Hahna et al., 13 also demonstrate their role in providing emotional support in hospital-based care.
Communication is a key area where assistive technologies make a significant impact. Mackenzie et al. 18 emphasize the importance of telehealth and “Augmentative and alternative communication” (AAC) tools for patients with motor neuron disease, enabling effective communication and improving access to care. Beyond individual applications, assistive technologies also contribute to broader system-level enhancements.
How were the studies on assistive technologies in palliative care conducted?
The publications analyzed provide insights into how studies on assistive technologies in palliative care have been conducted. These studies employ diverse methodologies, reflecting the complexity and multidimensional nature of the field.
Many studies utilize qualitative approaches to explore nuanced patient and caregiver experiences. For example, Robitaille et al. 20 conduct a qualitative study using interviews with healthcare practitioners, researchers, and managers to investigate the use of elastomeric infusion pumps for respiratory distress management in pandemic settings. Similarly, Hochstenbach et al. 15 employ qualitative methods to develop and evaluate an eHealth system for cancer pain self-management, with a focus on patient symptom relief and self-management strategies. In total, 6 studies were based on the qualitative approach.12,14,15,19–21
Mixed-methods designs are also prevalent,11,16,22 combining qualitative and quantitative approaches to provide comprehensive insights. Zhang et al. 22 use a mixed-methods approach, including surveys, interviews, and co-design workshops, to examine privacy concerns and usability feedback related to fall detection cameras for older adults. Klebbe et al. 16 adopt a mixed-methods design to evaluate customized robotic systems for amyotrophic lateral sclerosis (ALS) patients, gathering data on autonomy and usability feedback through observational studies and patient feedback.
Quantitative design was applied once in a study requiring measurable outcomes. Mackenzie et al. 18 conduct a quantitative study to assess the effectiveness of telehealth and AAC tools for patients with motor neuron disease, focusing on communication access and usability.
Additional context about study execution reveals, for example, that Tishelman et al. 21 employ an innovative approach using photographic elicitation to explore environmental adaptations and well-being among end-of-life patients, effectively integrating research tools as part of the intervention. In contrast, Nwosu et al. 19 provide a structured analysis of assistive and robotic technologies in palliative care through a qualitative SWOT (Strengths, Weaknesses, Opportunities, Threats) framework, highlighting the heterogeneity in existing studies.
The measured outcomes varied widely and often reflected the aims of the studies. Some studies focused on patient outcomes, such as symptom relief, emotional support, and autonomy (e.g., References 14, 16), while others targeted system-level outcomes, such as quality improvement and care coordination (e.g., References 11, 16). Additionally, studies like Landau et al. 17 emphasize caregiver outcomes, exploring decision-making processes and ethical considerations associated with tracking technologies for dementia patients.
Who were the target groups for assistive technology interventions in palliative care?
The studies encompass a wide range of populations, reflecting the diverse applications of assistive technologies in this field. Assistive technologies are often designed for older adults (age > 50 years), who are represented in 6 studies.11,15–17,21,22 For example, Zhang et al. 22 focus on individuals aged 55 to 94, with a mean age of 67.8 years, addressing privacy concerns and usability of fall detection cameras. Similarly, Landau et al. 17 target older adults with dementia, with a study population aged 60–87 years (mean age of 72.2 years), highlighting the use of tracking technologies in community settings. Gender representation varied across studies; for instance, Zhang et al. 22 report 134 male and 255 female participants, while Klebbe et al. 16 had a predominance of male participants (73%) in their study on robotic systems for ALS patients.
In terms of clinical conditions, neurodegenerative diseases were a frequent focus, with specific attention to conditions such as ALS and dementia. For example, Klebbe et al. 16 explore robotic systems tailored for ALS patients, while Landau et al. 17 examine ethical implications of tracking technologies for dementia care. Other studies targeted broader clinical populations, such as cancer patients. Hochstenbach et al. 15 developed an eHealth system for cancer pain management, while Hasei et al. 14 address the needs of young patients with rare cancers.
The settings of these interventions were diverse, ranging from home-based care to hospital and community settings. Home-based care was emphasized in 4 studies.15,16,18,22 Hospital-based care was highlighted in 2 studies12,13 while Hasei et al. 14 focus on the use of virtual environments, and retirement homes, residential care, community settings were discussed in References [11,17,19–21].
Regarding the palliative care stage, all studies addressed advanced illness or end-of-life care.
Discussion
This scoping review shows the diverse roles of assistive technologies in palliative care, such as symptom management, monitoring, emotional support, communication, and systemic improvements. Encompassing digital devices, robotics, and mechanical aids, these technologies address the complex needs of patients and caregivers, contributing to improved care delivery, outcomes, and well-being in palliative settings.
Furthermore, the review highlights diverse methodologies in assistive technology research for palliative care, including qualitative, quantitative, and mixed-methods designs. These approaches are tailored to explore user experiences, evaluate system integration, or measure impacts, emphasizing the need to align research designs with the field’s complex challenges and goals.
Assistive technology interventions in palliative care serve diverse groups, including older adults, individuals with neurodegenerative diseases, cancer patients, and those with rare conditions. Implemented across various settings—home care, hospitals, hospices, and community facilities—they address stages from advanced illness to end-of-life care, demonstrating their adaptability and importance in comprehensive care.
Considering the number of results in ScienceDirect for the search term “assistive technology” (i.e., over 1,000,000) and approximately 119,000 results for “palliative care,” the identification of only 12 publications for this review may appear small in comparison. However, this outcome aligns with related reviews, such as the scoping review by Tan et al. 23 on digital technologies in palliative care, which analyzed 24 publications after the screening process. The smaller number of publications on assistive technologies compared to digital technologies in palliative care likely reflects the broader scope and more frequent use of “digital technologies” in research. In contrast, “assistive systems” is narrower and less consistently applied, limiting its visibility in searches.
What sets this scoping review apart is the deliberate decision to use “assistive technology” as a search term without further specification regarding the type of technology or the field of application. This approach was based on the understanding that assistive technology functions as an umbrella term encompassing a wide range of technologies applicable within the palliative care domain. By intentionally avoiding narrower or predefined categorizations, this review aimed to capture the full breadth of potentially relevant literature.
Within the extensive body of literature, two key factors may explain the relatively small number of publications explicitly addressing assistive technology in palliative care. First, some publications on assistive products may not explicitly use the label “assistive technology,” making them less visible in targeted searches. Second, assistive technologies with cross-domain utility are often not documented specifically within the context of palliative care, even when they are relevant to it. These factors highlight potential gaps in terminology and domain-specific reporting that could contribute to the observed scarcity of publications on this topic.
The relative scarcity of publications explicitly using the term “assistive technology” raises the question of whether the term itself lacks sufficient prominence or recognition in the academic and clinical discourse surrounding palliative care. This observation highlights a potential knowledge gap, suggesting the need for initiatives to promote the term and its relevance more widely. Such measures could include targeted educational efforts, integration into professional guidelines, and greater emphasis on the term in research and policy documents. Addressing this gap would not only enhance the visibility of assistive technology but also foster its acceptance and integration across diverse domains, including palliative care.
Building on the insights of this review, several directions for future research and analysis emerge. Future reviews may benefit from a stronger focus on the scientific rigor of included studies, with particular attention to study design, quality, and the use of randomized controlled trials to evaluate the effectiveness of assistive technologies in palliative care. Comparative studies across different healthcare systems and cultural contexts may offer valuable perspectives on the varying patterns of adoption and integration. Further exploration of implementation barriers—such as affordability, accessibility, and resistance from healthcare professionals—would contribute to a more comprehensive understanding of the conditions under which assistive technologies are successfully adopted. Ethical considerations, including concerns related to privacy, algorithmic bias, and patient autonomy, warrant closer examination, particularly considering the increasing use of AI-based and monitoring technologies. A comparative analysis with broader digital health interventions may also help to contextualize assistive technologies within the evolving landscape of technological innovation in palliative care. Lastly, refining the thematic categorization of technologies could enhance conceptual clarity and reduce overlap between categories. To support these research directions, future studies should consider expanding the search strategy beyond the term “assistive technology” to include related concepts and specific technological applications, thereby enabling a more comprehensive and representative synthesis of the literature.
Conclusion
This scoping review highlights the multifaceted role of assistive technologies in palliative care, encompassing purposes such as symptom management, monitoring, emotional support, communication, and systemic improvements. The studies reviewed demonstrate the diversity of methodologies employed, including qualitative, quantitative, and mixed-methods designs, tailored to explore user experiences, evaluate system integration, and measure outcomes. Additionally, the target populations are broad, ranging from older adults and individuals with neurodegenerative diseases to cancer patients and those with rare conditions, with applications across various care settings and palliative care stages.
Despite the significant contributions of assistive technologies, the relatively small number of publications explicitly addressing their role in palliative care points to notable gaps. These gaps may stem from inconsistent use of the term “assistive technology” in literature and the underrepresentation of technologies with cross-domain applications in palliative care research. Expanding search strategies and promoting the recognition of assistive technologies in academic and clinical contexts are essential steps to bridge these gaps and foster a more comprehensive understanding of their potential in palliative care.
Footnotes
Ethical considerations
This study is a scoping review of the literature and did not involve human participants or animals. Therefore, ethical approval was not required.
Author contributions
CONCEPTION: Martin Biallas, Aliaksei Andrushevich. PERFORMANCE OF WORK: Martin Biallas, Aliaksei Andrushevich, Clemens Nieke, Martin Morandell, Lorenzo Desideri. INTERPRETATION OR ANALYSIS OF DATA: Martin Biallas, Aliaksei Andrushevich, Clemens Nieke, Martin Morandell, Lorenzo Desideri, Evert-Jan Hoogerwerf, Andrew Paice. PREPARATION OF THE MANUSCRIPT: Martin Biallas, Aliaksei Andrushevich, Clemens Nieke, Martin Morandell, Lorenzo Desideri, Evert-Jan Hoogerwerf, Andrew Paice. REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Martin Biallas, Aliaksei Andrushevich, Clemens Nieke, Martin Morandell, Lorenzo Desideri, Evert-Jan Hoogerwerf, Andrew Paice. SUPERVISION: Evert-Jan Hoogerwerf, Andrew Paice.
Funding
The authors disclosed receipt of the financial support from Lucerne University of Applied Sciences and Arts for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article