
Abstract
Exercise is significantly beneficial for patients with osteoporosis. However, physiological and psychological factors such as pain and kinesiophobia prevent patients from participating in exercise. Therefore, it is important to understand how these patients perceive participation in exercise. This qualitative study was conducted in China using conventional content analysis. Using a purposeful sampling method, 17 patients with primary osteoporosis were recruited. Data were collected through a semi-structured interview and managed using ATLAS.ti 21. Nine generic categories were developed from 26 subcategories and two main categories were identified: Barriers and facilitators, support systems, network resources, positive emotions, and reactions were the facilitators for exercise in this study. In addition, mindful exercise was positively viewed by the patients. Inefficient awareness, weak support systems, and burdens were identified as barriers. To improve compliance in clinical practice, targeted exercise protocols should be developed for patients based on these perceptions.
Introduction
Primary osteoporosis is the most common form of osteoporosis that occurs as a result of the natural aging process (Abdolalipour et al., 2021). It is a pathological condition in which bone loses strength and quality as bone mass volume decreases, leading to the thinning and weakening of bones and prone to fracture (Paolucci et al., 2016). In addition, osteoporosis-related skeletal changes, skeletal deformities, muscle structure strains, and axial posture deformities (kyphosis) can lead to chronic back pain (Abdolalipour et al., 2021), even in the absence of fractures (Vellucci et al., 2018). Furthermore, patients with chronic pain or a history of fractures often experience psychological reactions such as reluctance or fear of movement (kinesiophobia), which is an excessive, irrational fear of physical activity or movement due to the increased sensitivity to pain or fear of renewed fractures (Alexiou et al., 2018).
Exercise is recommended by many international guidelines and expert consensus as a nonpharmacological and complementary treatment for patients with osteoporosis (Brooke-Wavell et al., 2022; Gregson et al., 2022). However, pain and kinesiophobia have been found to be the factors that discourage patients from participating in the exercise (Bäck et al., 2020; Casiano et al., 2022). Therefore, mindful exercises are recommended for these patients with pain because of their gentle and slow movements and combination of mindfulness elements, which are also effective for psychological symptoms (Chinese Association of Rehabilitation Medicine, 2019; Ravari et al., 2021). Mindful exercise is a multimodal low-intensity exercise that involves coordinated body motions, regular breathing, and focuses on the mind–body interactions. The classic exercise methods in China include Tai Chi, Ba Duan Jin, Wu Qin Xi, and Yi Jin Jing, meanwhile, in the West region implies Yoga and Pilates techniques (Peng et al., 2021; Wu et al., 2019).
A previous randomized controlled trial (RCT) has shown that mindful exercise (Pilates) was effective in relieving pain and psychological symptoms in patients with primary osteoporosis (Oksuz & Unal, 2017). However, the experiences and feelings related to exercising in these patients remain to be explored. A systematic review reported that few RCTs identified facilitators and barriers to exercise participation or adherence (Rodrigues et al., 2017). Therefore, it is important to understand and consider the perceptions of patients with primary osteoporosis, particularly those with pain and kinesiophobia, when developing an appropriate exercise program. Therefore, this study aimed to explore the perceptions of patients with primary osteoporosis who participated in exercise experience or not, and also aimed to identify facilitators and barriers to participation in exercise. The findings of this study could serve as a guide for future development of exercise programs or interventions.
Materials and Methods
Design
A descriptive qualitative study was conducted using in-depth, semi-structured face-to-face interviews with a conventional content analysis approach. The reporting of this study is in accordance with the Standards for Reporting Qualitative Research (SRQR) guideline.
Participants
Patients were recruited using a purposive sampling method from the pain department of a traditional Chinese medicine hospital in Kunming, China, between June and October 2022. Inclusion criteria were as follows: (i) has been diagnosed with primary osteoporosis, which was made by the patients’ physician based on World Health Organization (WHO) diagnostic criteria (NIH Consensus Development Panel, 2001); (ii) aged 18 years old and above; (iii) with mild to moderate back pain (measured by Numerical Rating Scale, with a score from 1 to 6) for more than 3 months; (iv) experiencing kinesiophobia (scores above 26 according to the Chinese version of the Tampa scale of kinesiophobia-11 (TSK-11) (Cai et al., 2019); and (v) have good communication and language skills. The exclusion criteria were patients currently or recently (within the past 3 months) suffering from fractures, tumors, and other serious comorbidities. Patients undergoing other psychotherapy or taking psychotropic medications were also excluded in this study. The data saturation method was used to achieve the required sample size.
Interview Guide
Using the fear avoidance model as a conceptual framework (Leeuw et al., 2007), an interview guide was developed with input from literature reviews and expert group discussions. The guide was reviewed by a panel of six experts in nursing, mindful exercise, physical therapy, and orthopedics and piloted on two participants who had characteristics similar to the actual sample. The feedback from the preliminary interview and experts was used to revise the guide (Figure 1).
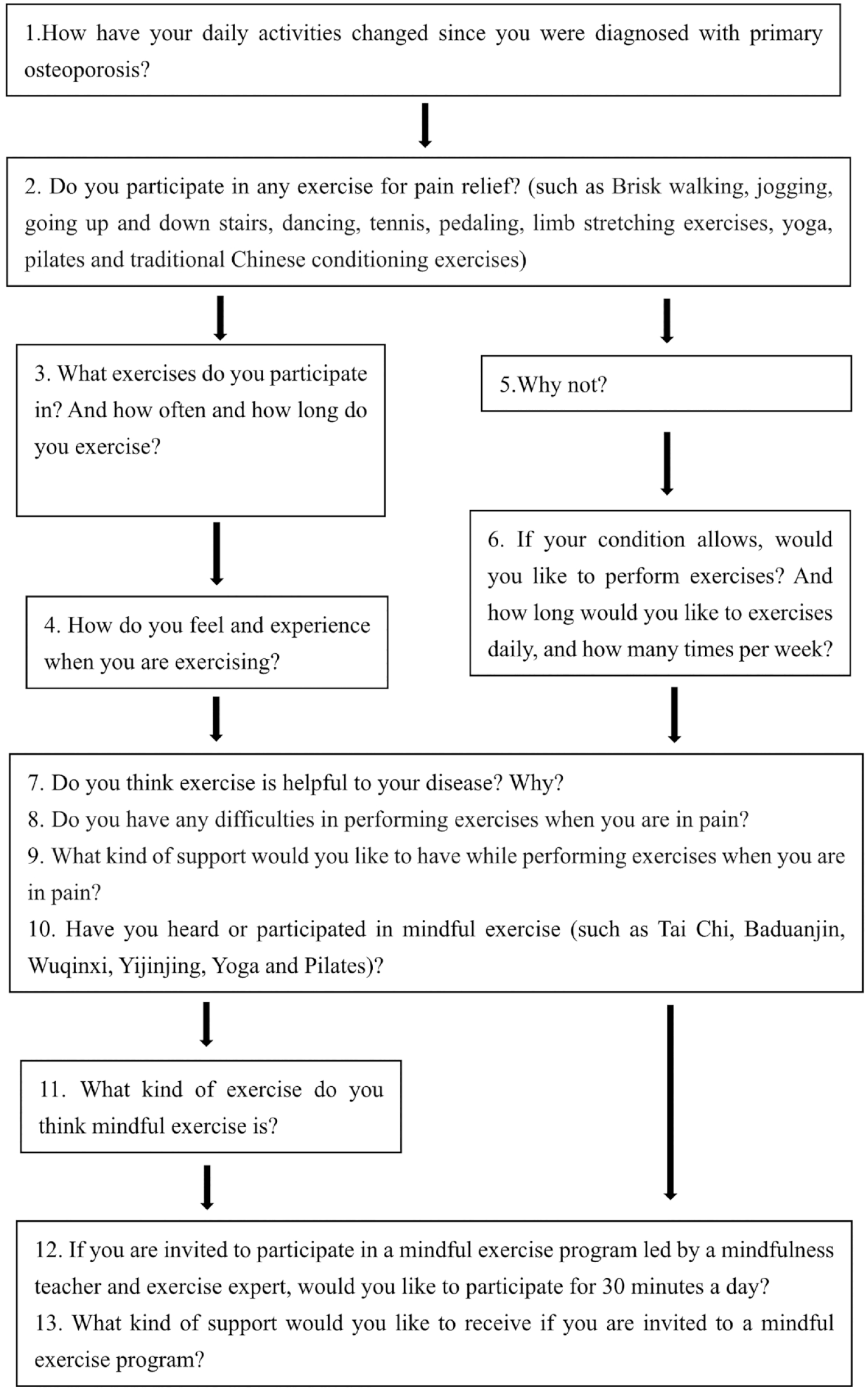
Interview guide.
Data Collection
Data were collected through a semi-structured interview from June 10 to October 27, 2022 after receiving ethical approval from the Institutional Review Board. The interviews were scheduled between days 2 and 5 after the patient’s admission to the hospital. Prior to the interview, eligible participants were briefly introduced to the content and purpose of the study, and kinesiophobia scores were assessed using the TSK-11. Patients with a score of 26 and above were included in the study and written informed consent was obtained.
The one-on-one interview was conducted in a closed atmosphere, either in a doctor’s office or in a rehabilitation room. The closed-door method was adapted to ensure a quiet environment free from external disturbances and allow for effective conversations between the researchers and participants. The interview sessions were video and audio recorded with the patients’ consent using the main researcher’s smartphone, which was protected by a password known only to the researcher. The researcher moderated the interview session with questions and conversations that avoided directions and cues. A semi-structured interview guide and probing questions were used. Each session lasted 45 to 60 minutes to gather sufficient information from each participant. Each patient was interviewed only once.
Data Analysis
The qualitative data were managed and coded by ATLAS.ti 21 using conventional content analysis because there is little literature supporting and providing information on this topic (Hsieh & Shannon, 2005). The results of this analysis are often presented in easy-to-understand language that is closer to the data itself since codes and categories were developed from textual data (Elo & Kyngäs, 2008).
Transcription of the audio recordings into texts was done within 24 hours by a trained transcriber; meanwhile, video recordings of the movements, facial expressions, and emotional changes in the participants were transcribed and marked in the texts. The texts were then read repeatedly and checked against the recordings to ensure their accuracy. First, preliminary codes were condensed by the main researcher and derived based on the meaningful sentences or phrases selected after a comprehensive and in-depth reading of the transcripts. Next, preliminary codes with similar themes were grouped into clusters to form subcategories and further classified into categories. Corresponding excerpts from the data were found for the codes to document the movements, facial expressions, and emotional changes of the participants in comparable positions. A double check of the findings with the interview encodings and transcripts was conducted by another researcher who is an expert in qualitative research. Discussions and debriefings were held with the research team and two supervisors experienced in qualitative research until a final consensus was reached. In addition, descriptive analyses of quantitative demographic data were performed using SPSS software for Windows 27.0.
Trustworthiness
The qualitative research (SRQR) checklist (O’Brien et al., 2014) was used to report the consolidated criteria followed by research methods and findings. Emoji notes, field notes, and self-reflective notes connected researchers with data. Group discussions between experts and researchers were used to code, and summarize categories and subcategories to ensure dependability. Review by peer or expert verification and participant verification of findings were methods to ensure credibility (Ansari et al., 2021). Therefore, the generated main category, generic category, subcategory, and representative statements were shared and discussed with selected participants, two external and two internal experts, respectively, to support the credibility, and confirmability of the findings. For transferability, the findings of this study (experiences, perceptions, and needs of the patients) could serve as a guide for the clinical implementation of exercise programs in the future.
Ethical Considerations
Patients who met the inclusion criteria were approached on the first day of their hospital stay and informed about the details of the study. Patients were also given adequate time to consider whether to participate in the study, as the interviews were conducted on days 2 to 5 of the hospitalization. They have been informed that they may withdraw from the study at any time and would not be discriminated against or face retaliation for their participation or nonparticipation, nor their status in the study affect the medical services provided to them. Data collection procedures were carried out in accordance with the Declaration of Helsinki, with maintenance of confidentiality and anonymity. Recruitment and interview sessions only commenced after ethical approval from the study setting and written consent from the participants, as well as permission to use the Chinese version of the TSK-11 scale, were obtained.
Results
The sociodemographic and clinical characteristics of the participants are presented in Table 1. Of the 17 total patients, 7 were males and 10 were females aged 48 to 87 years (median age 67, and interquartile range [IQR]: 58–72.5). Pain duration was from 1.5 to 16.5 years and the pain level score of NRS ranged from 1 to 6. TSK-11 scores of all 17 patients ranged from a minimum of 27 to a maximum of 41, with a median score of 33 and an IQR of 29.5 to 37.5.
Participants’ Demographic and Clinical Characteristics (N = 17).
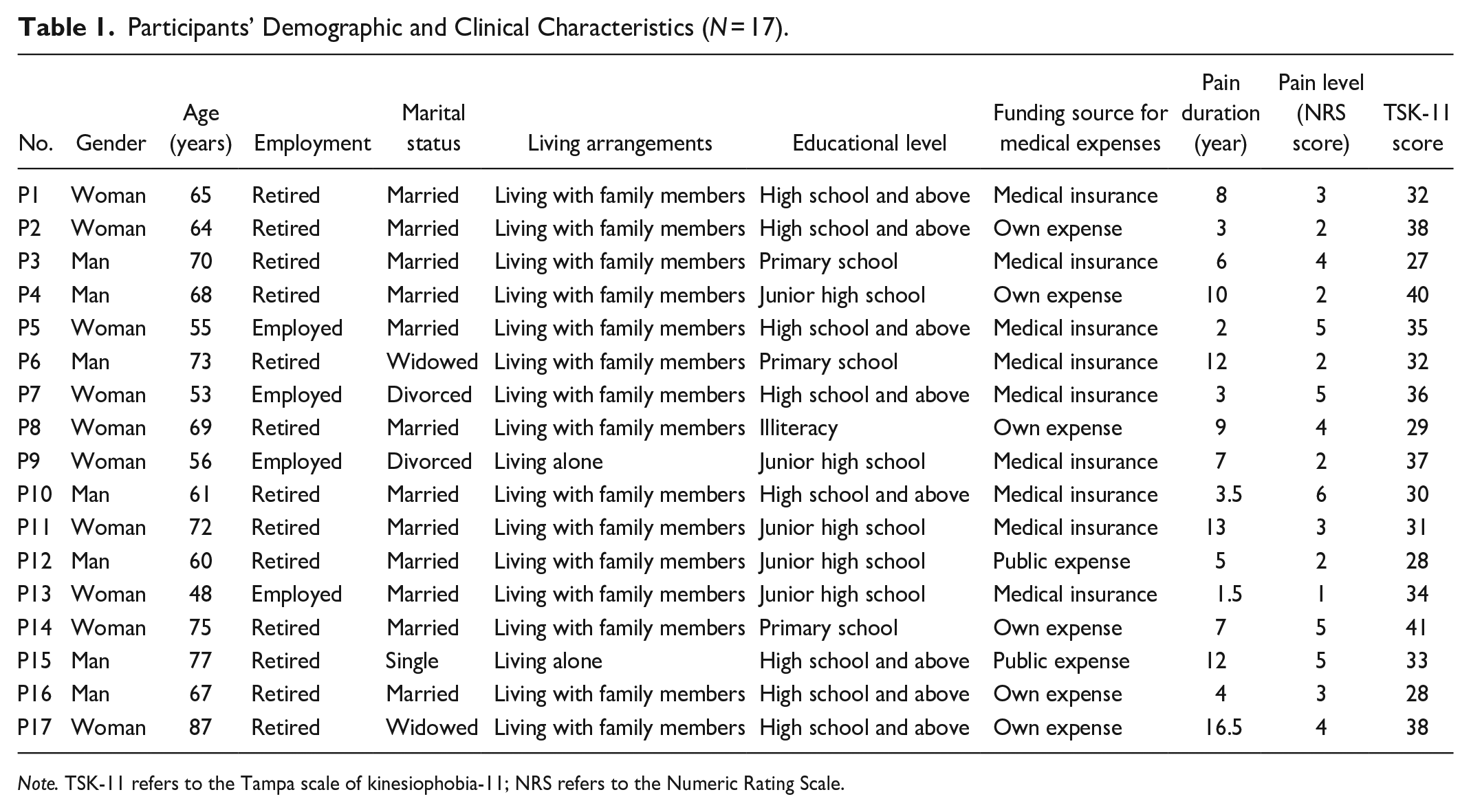
Note. TSK-11 refers to the Tampa scale of kinesiophobia-11; NRS refers to the Numeric Rating Scale.
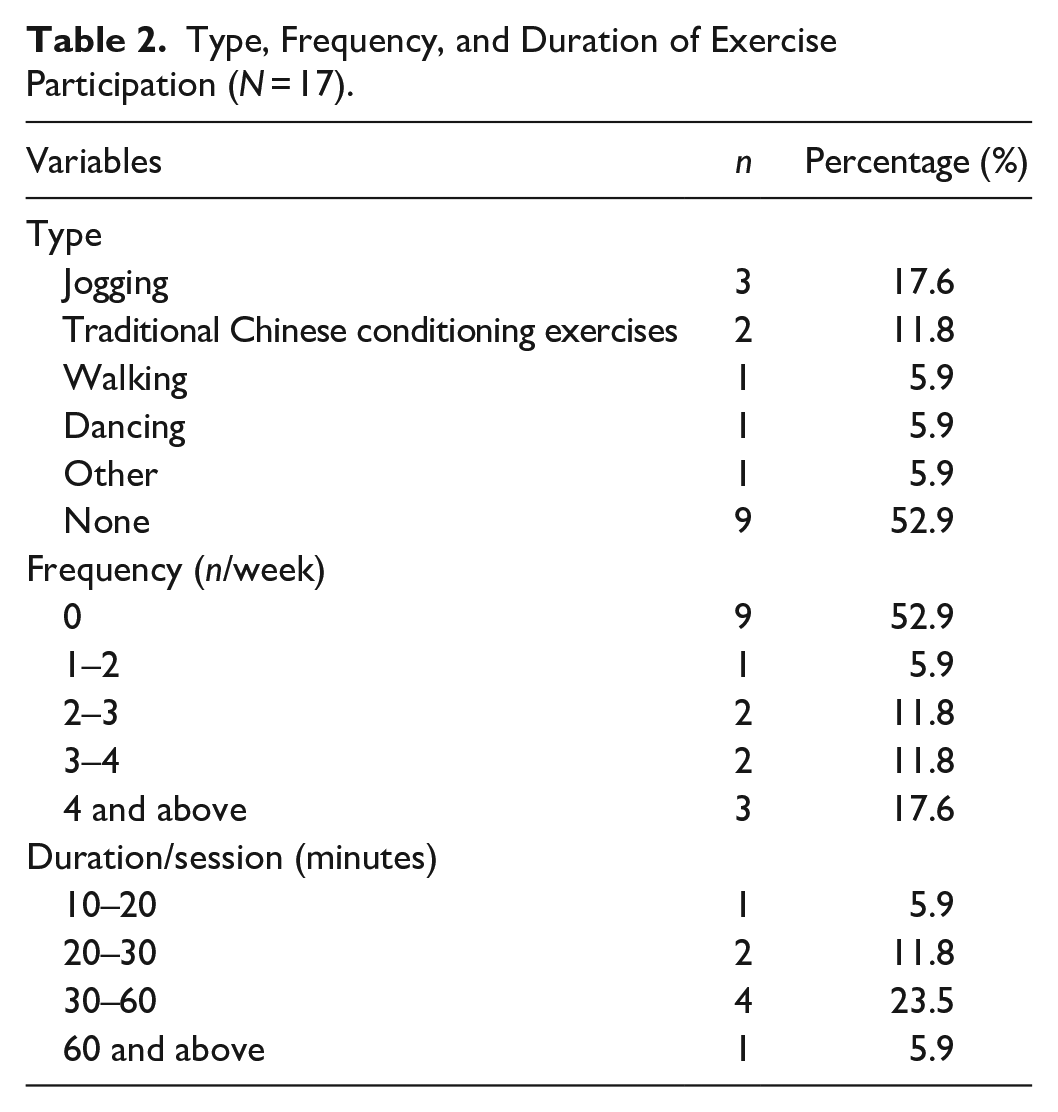
Subsequently, patterns of participation in the exercise were summarized. Eight patients had tried various types of exercises prior to their hospitalization. They chose their favorite exercise program from the internet, newspapers, or a TV show. They received no guidance from healthcare or sports professionals in performing the exercise. Most of these exercises were relatively mild, such as walking, jogging, and dancing, and two of them had regularly participated in mindful exercise (Tai Chi and Ba Duan Jin). Details on the type, frequency, and duration of the exercises are shown in Table 2. Among them, jogging was selected most frequently. Their exercise frequency was mostly more than four times a week, and the duration of each exercise was 30 to 60 minutes.
Type, Frequency, and Duration of Exercise Participation (N = 17).
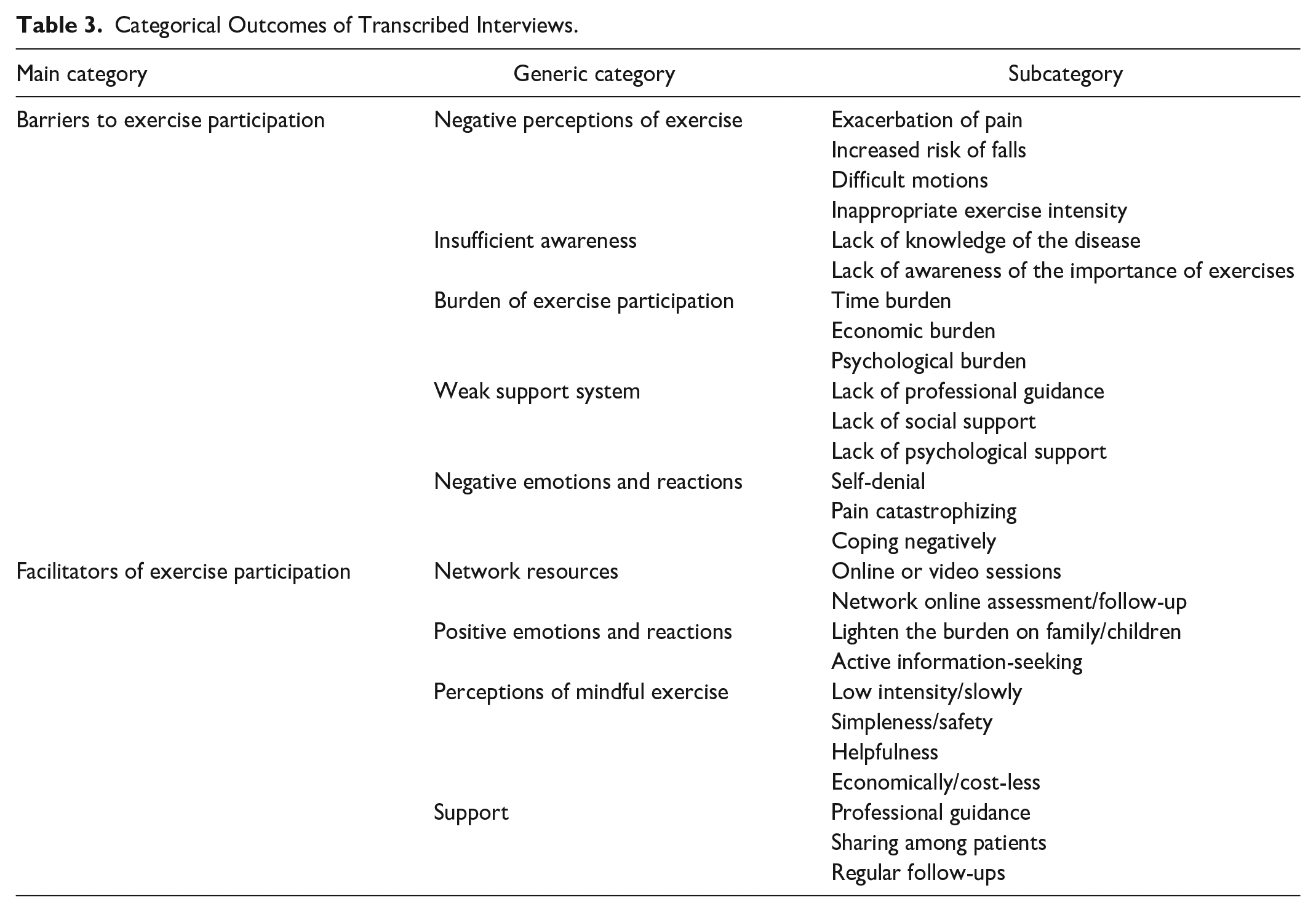
A total of 178 preliminary codes were grouped into 26 subcategories. Subsequently, nine generic categories were developed from the 26 subcategories and two main categories were then identified in the data (Table 3): barriers and facilitators of exercise participation. Among the barriers categories, the following generic categories were identified: negative perceptions of exercise, insufficient awareness, weak support system, burden, and negative emotions and reactions. Meanwhile, network resources, positive emotions and reactions, perceptions of mindful exercise, and support were grouped into facilitator categories.
Categorical Outcomes of Transcribed Interviews.
Barriers to Exercise Participation
There were five generic categories under this main category.
Negative perceptions of exercise
Most participants had negative experiences with exercise. As a result, many participants questioned or disputed the effectiveness of exercise and feared that exercise could lead to disease complications: It was said on the internet that walking backwards was good for brain function. You see, last year I fell because of walking backwards and finally broken my left leg (Sigh).(P2) When I was first hospitalized, the doctor advised me to do some kind of bridge exercise. Although it was difficult for me, I persisted for a few days, but it didn’t work at all. Instead, it got worse. I didn’t want to do it anymore; it was too painful (Shake his head). (P12)
Insufficient awareness
More than half of the respondents in this study have never exercised to relieve pain. Two main subcategories were identified: lack of knowledge about the disease and awareness of the importance of exercise. The interview sessions revealed that most participants did not have a full understanding of osteoporosis and how it causes back pain. In addition, participants feared that the exercise would make their pain worse or lead to more serious complications, such as fractures because they did not practice the right exercises. As a result, patients lacked motivation and poorly accepted the exercise. Four of the participants in this study declined to engage in any form of exercise in the future. Three participants are cited below: Why exercise? In my current situation, lying down is the best. (P3) Exercise may increase the risk of fractures, right? For example, fall during exercise. I think I’d better not exercise or reduce exercise. (P16) What does exercise do? the most important thing is to relieve the pain for me (Angry). (P4)
Burden of exercise participation
The findings mainly summarized two kinds of burdens: internal and external burdens. Of which, external burdens included time and money, while the internal burden was psychological. Psychological burden is noted when the patients have an emotional fear that they would be a burden to their family and also when they worry their family members would be affected as they are required to care for and support patients during medical treatments. In all, 16 participants reported experiencing this kind of psychological burden, while 6 participants in this study experienced the economic and time burden due to their condition. Below are sample responses: I have been in pain for more than 10 years, repeatedly, I can’t even turn over when the pain starts, I can’t move by myself, and need help from others, causing a lot of trouble for my children (sigh). (P8) I don’t have time to come to the hospital for rehabilitation. My home is far away. (P13)
Weak support system
In all, 11 respondents stated that having professional medical support encourages them to exercise, while the lack of such support was one of the reasons for their kinesiophobia. Patients were more dependent on support from a doctor or therapist prior to exercise, while nine patients experienced anxiety when exercising without physician guidance: The doctor always told me verbally what to do, which was too abstract, and I was worried that I would exacerbate my disease by exercising too much. (P9) The doctor asked me to find some pictures and videos on the Internet to follow, but there are too many, who knows which is right and which is wrong. (P8)
Three respondents were aware of their own psychological problems and would like professional psychological support.
My sleep quality and mood have been very bad since I got sick. I hope a professional psychiatrist can help me. (P5) No one wants to hear how I feel, I’m in pain, not only physically, but also psychologically. (P13)
Some of the patients suffered from back pain due to primary osteoporosis for a long period of time without an effective cure. Therefore, they stressed the need for proper understanding, help, and support from family members. One of the patients stated: My children are all working in another city. There are only me and my wife at home. My wife has many chronic diseases. She needs someone to take care of her. How could she take care of me? (Shake his head). (P15)
Negative emotions and reactions
A total of three negative emotions and reactions were extracted, consisting of self-denial, pain catastrophizing, and coping negatively. Pain catastrophizing is defined as “an experience of actual or expected exaggerated negative mindset in the experience of pain.” This behavior belongs to poor cognitive and emotional coping mechanisms.
Many of the patients showed self-loathing and depreciation due to the adverse effects of experiencing long-term pain, causing patients to change their perceptions and consciousness toward many aspects of life, including exercise. Eight participants in this group described their self-denial, for example: It’s so difficult to get up and move around every time, let alone participate in exercise, it’s useless when getting older (Sigh). (P17)
In all, 11 participants in this group thought their pain was horrible and could not be eliminated. The keywords expressed by these participants included “life rather than death,” “unbearable/breakdown,” “worried/fearful,” and “disability/use-less.” I just want to lie down every day now, it hurts after sitting for a long time. (P16) The pain was really unbearable, and a score of 10 was not enough (NRS). Don’t know how to reduce this pain. (P8)
Long-term fear of pain causes patients to also adopt negative coping strategies for disease treatment, including a tendency to avoid and resist various rehabilitation training. There were nine participants with obvious “escape psychology,” which was defined as coping negatively. Below are some of their interview excerpts: After getting sick, I think about how to relieve the pain every day, don’t want to care about anything else (Frowning). (P1) I used to travel a lot with friends and family, but now I don’t want to go anywhere, can’t go anywhere (Sighing). (P5)
Facilitators of Exercise Participation
Four generic categories were extracted and classified as facilitators participating in the exercise.
Network resources
Some respondents indicated that the availability of online exercise guides would save time and reduce transportation costs. In addition, it would be better if there were online follow-ups, which could correct the wrong exercise methods and update the exercise program according to the physical conditions of the individual. One respondent explained: Professional online sessions or videos will motivate me to participate in exercise after discharge. (P5)
Positive emotions and reactions
About half of the patients responded positively to exercise if it facilitates recovery from illness. As long as it has a positive effect on the rehabilitation of the disease, they were willing to try whether it is pharmacological or nonpharmacological therapy. Three patients said that they often learned some knowledge about osteoporosis online, especially those related to exercise or mindful exercise.
If exercise is helpfulness, I am willing to participate every day to strengthen my bones. Get well soon can reduce the burden on the family and not cause trouble to my children. (P5) I learned Tai Chi from the internet (Smile). (P15)
Perceptions of mindful exercise
Although only two of the respondents have previous regular experience in mindful exercise, but almost all have heard of mindful exercise, especially Tai Chi and Ba Duan Jin. Some perceptions of mindful exercise were extracted, such as “low-intensity/slowly,” “simpleness/safety,” “helpfulness,” and “economically/cost-less.” I am willing to participate in such simple and safe sports as Ba Duan Jin. (P10)
Most of them were also receptive toward a duration of 30 minutes of practice per day.
I’m retired and I have nothing to do every afternoon, so it’s nice to spend 30 minutes exercising (Smile). (P2)
Support
Although most respondents were willing to participate in a mindful exercise program, professional guidance, and support from others were their main concerns: Professional guidance is important not only during hospitalization but also after discharge. (P3) I have done mindful exercises before. I know personal feelings and experiences are important, who do I share my feelings with after I leave the hospital? (P5)
Considering the positive effects of mindful exercise program toward relieving pain, some patients hope to have regular follow-ups: With regular follow-ups, I’ll be able to see how it works, so I’ll be more confident doing it. (P4)
Discussion
Exercise plays a crucial role in maintaining skeletal health (Tong et al., 2019). Previous studies have shown that exercise or physical training can improve bone mass (Kemmler et al., 2020), bone composition (Goolsby & Boniquit, 2017), and bone calcium content (Al Dahamsheh et al., 2019) with less adverse reactions. Exercise has become increasingly popular in many countries and is recommended in osteoporosis prevention and treatment guidelines (Gregson et al., 2022; Makras et al., 2019). Over the past decade, numerous studies have emerged of mindful exercise as an intervention in patients with primary osteoporosis. Researchers have applied Yoga, Pilates, Tai Chi, and Ba Duan Jin to patients with osteoporosis and have obtained various results. Although many studies have reported the effectiveness of pain relief (Oksuz & Unal, 2017; Sun et al., 2021), there were still negative results reported by researchers (Grahn Kronhed et al., 2020). Exercising the wrong way could cause adverse consequences (Sluka et al., 2018). This study found that participation in exercise was perceived as poor or unsatisfactory, which is a similar outcome to a previous study (Rodrigues et al., 2017).
It was also discovered that patients obtained exercise-related knowledge and information from the internet, newspapers, relatives, or friends, but to a lesser extent from professional doctors or nurses. This may have resulted in patients performing exercises inappropriately. Notably, the lack of good post-exercise experience led these patients to question or dispute the effectiveness of the exercise.
In addition, the frequency and duration of the respondents’ exercising routine varied tremendously, with some exercising very frequently while others very occasionally. The frequency and duration of exercise regimes (minimum 3 sessions/week/year) were critical for patients with osteoporosis (Zitzmann et al., 2022). Exercise experts and professional healthcare workers should thus formulate reasonable exercise frequencies and durations for those patients.
Moreover, the interviews found that patients with kinesiophobia had insufficient awareness of the disease and chronic pain. This may be related to inadequate disease management and health education (Ansari et al., 2021). Patients’ fear of exercise and lack of participation in social activities that involve exercising have led to poor adherence to doctor’s treatment recommendations. Therefore, it is recommended that healthcare professionals pay specific attention to patients’ complaints, conduct kinesiophobia screening before discharge, and educate patients in detail about the causes, treatment, and prognosis of osteoporosis. These measures would help patients actively overcome the adverse effects of kinesiophobia and improve patient compliance in participating in the exercise.
It has also found that psychological, economic, and time pressures are barriers to participation in exercise activities. Some respondents indicated that they experienced psychological distress because they caused problems for their families. These patients may need psychological support. However, psychotherapies have often been neglected (Burns et al., 2018; Vidal et al., 2019), including among patients in China (Liu et al., 2019). Therefore, finding a viable, convenient, and cost-effective way to alleviate psychological problems while reducing the economic burden is crucial.
The support system of participants in this study was reported to be relatively weak, with a lack of professional, psychological, and family support. Patients mentioned that their doctor’s exercise recommendations were vague, with unclear instructions on duration, frequency, and method. Therefore, some participants experienced increased pain due to incorrect exercise methods (Sinaki, 2013). It is believed that there was a lack of clear education, possibly due to a shortage of personnel, time, and space (Ansari et al., 2021; Gao et al., 2020).
In terms of psychological support, many respondents indicated that the psychological problems caused by their disease were serious. Some had suicidal thoughts and wanted psychological support and counseling. Psychological distress was also influenced by kinesiophobia and family misunderstanding (Berthelot et al., 2019). Patients relied heavily on the support and help of family members to complete certain exercise routines and perform daily activities. Therefore, it is recommended that medical staff expand and improve professional guidance for family members caring for these patients with pain and kinesiophobia, and help foster empathy.
This study found that pain is one of the key factors affecting exercise, consistent with previous studies (Borisovskaya et al., 2020). Pain not only directly affects exercise but also leads to negative emotions (self-denial) and reactions (negative coping), which indirectly affect patient movement (Attali et al., 2023). Therefore, in addition to disease treatment and pain control, the mental health of patients with chronic pain and kinesiophobia also needs special attention (Hemmati et al., 2021).
Nonetheless, it was encouraging to find that most participants were still willing to participate in mindful exercise programs with professional guidance, as this exercise is considered slow, safe, easy, and economical. In China, the vast majority of exercise specialists and healthcare professionals recommend Tai Chi, Ba Duan Jin, or Wu Qin Xi for these patients with pain, which are also recommended in the Chinese osteoporosis guidelines (Chinese Association of Rehabilitation Medicine, 2019). It is noteworthy to consider that existing mindful exercises consist of some routine movements that are too difficult for these patients. Therefore, future research should focus on an appropriate mindful exercise program.
In addition to professional guidance, regular follow-up, and patient-to-patient sharing facilitated participation in exercises. However, it was found that healthcare professionals provided guidance during the hospitalization and there was little follow-up care (Fan et al., 2021). Therefore, online video face-to-face follow-up and online courses can be a new model for future implementation because of their convenience and time-saving, but age and generational limitations should be considered (Zhao et al., 2021). In addition, patient-to-patient sharing could facilitate the diffusion of positive emotions and reactions (Finlay et al., 2022), which have also been found to be facilitators of exercise participation.
Limitation
There are some limitations in this study. First, the interview data were collected only from patients with primary osteoporosis, who experienced mild to moderate chronic back pain. However, patients without pain may have a more positive perception toward exercise. While those with severe pain may have more negative perceptions, but most of these patients refused to be interviewed because of excessive pain. Second, most of the respondents have no previous experience with mindful exercise, which may lead to one-sided or incomplete perceptions of mindful exercise. In addition, all participants were recruited from a traditional Chinese medicine hospital and were likely to have strong beliefs in some kind of mindful exercise (such as Tai Chi, Ba Duan Jin). It may therefore be necessary to include patients with no and severe pain in further studies or to apply more stringent sample selection.
Conclusions and Application
This is one of the few studies that has reported on patients with primary osteoporosis’ perceptions and expectations of exercise. Pain and kinesiophobia experienced by patients with primary osteoporosis led to anxiety and avoidance of exercise and daily activities, which, in turn, led to psychological problems. This study used qualitative research methods to gain an in-depth understanding of the patients’ perceptions of participation in exercise. It is recommended that nursing and healthcare professionals should pay attention to patient’s inner feelings and needs to improve compliance with exercise participation. At the same time, the patient’s social support system and psychological problems need improved approaches to help patients actively embrace exercise therapy. In addition, combining mindfulness with exercises may be an appropriate way to encourage participation, but professional guidance and regular follow-up are needed to ensure compliance and safe practice.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The ethical committee of the First Affiliated Hospital of Yunnan University of Traditional Chinese Medicine. The approval number is XW[2022](004).