
Abstract
Objectives: This study sought to explore feasibility, acceptability, and preliminary effects of aerobic training (AT), mindfulness training (MT), or both (MT + AT) on cognitive function in older individuals at risk of dementia. Method: Participants were randomized to AT, MT, both, or usual care (UC). Z-scores of attention, verbal fluency, and episodic memory for non-demented adults (ZAVEN) were computed at baseline, end of treatment (EOT), and 6 months since baseline. Results: Of the 36 enrolled participants (12 M, 24 F, mean age = 70.1 years), 97% were retained in the study at 6 months. At EOT, MT had higher ZAVEN scores than UC (b = .43, P =.03) and AT (b = .26, P = .10), while no differences were seen with MT + AT. A similar pattern was observed at a 6 month follow-up (all P values = .10). Discussion: MT may improve cognitive function in older individuals at risk of dementia. These preliminary findings need to be confirmed in a fully powered RCT.
Introduction
Because of population aging, the prevalence of dementia is increasing worldwide and no effective pharmacological treatment is currently available to delay or treat this condition. One-third of cases of dementia are attributable to modifiable risk factors such as cognitive and physical inactivity, diabetes, hypertension, obesity, smoking, and depression. 1 Since improvements in risk factors could prevent up to 3 million dementia cases worldwide, 2 increasing attention has been dedicated to the development of preventive interventions targeting multiple lifestyle factors simultaneously. 3
Despite the evidence that both physical 4 and cognitively stimulating5-8 activity may prevent cognitive decline or the development of dementia, only a limited number of studies have focused on the effect of interventions combining cognitive and physical activity. Results have been somewhat encouraging, with a small study reporting that combined aerobic and cognitive training could lead to larger effects than either alone 9 and another suggesting that such combined approaches may increase brain plasticity, 10 while a large 2 × 2 factorial RCT of cognitive training and aerobic activity found no differences in cognitive function between active interventions and controls, but used a very active comparator. 11
Mindfulness training (MT), a form of cognitive training designed to cultivate purposeful and non-judgmental attention to the moment-to-moment experience of mental events and physical sensations 12 has shown promising effects on various cognitive domains in older adults with and without cognitive impairment. A recent systematic review and meta-analysis has shown that mind–body interventions (including mindfulness) improved cognitive function in older adults with cognitive impairment, but the studies were limited by the small sample size, the heterogeneity of outcome measures, the lack of an active control condition and a short follow-up duration. 13
Taken together, this evidence suggests a potential benefit of MT on cognitive function; however, to date, there is limited information on the feasibility, acceptability, and the possible effects of MT (alone or combined with exercise training) on cognitive function in older adults.
Thus, in preparation for a future large efficacy study, we were interested in (a) determining the feasibility and acceptability of MT, exercise training, and their combination among older adults at risk for dementia (primary outcomes) and (b) exploring the possible effects of these interventions on cognitive function (secondary outcome).
Method
A detailed description of the methods for this study has been published elsewhere. 14 Briefly, this single-site randomized controlled trial (RCT) was conducted in the Providence, RI area. Providncem Prthe. Participants were recruited over 3 distinct recruitment cycles between April 2016 and May 2018.
Study Population. Participants were recruited from the community using flyers placed in public venues, advertisements in local newspapers, and online resources. Interested individuals contacted the study staff using a dedicated phone number included in all recruitment materials. Inclusion criteria included age ≥ 55, being physically inactive (i.e., not meeting American Heart Association recommendations of ≥ 150 minutes of moderate or ≥ 75 minutes of vigorous physical activity weekly, 15 determined via 7-day physical activity recall questionnaire), 16 reporting at least 2 risk factors for dementia (i.e., in addition to physical inactivity, cognitive inactivity, diabetes, hypertension, obesity, smoking, and depression), 1 self-reported cognitive complaints, and fluency in English. We screened participants for self-reported cognitive complaints by using a single question “do you feel that your memory or thinking skills have gotten worse recently?” If participants answered “yes,” they were deemed to be eligible.
Exclusion criteria were inability/unwillingness to provide informed consent; contraindications to physical activity, blood pressure > 200/110 at the screening visit, severe depressive symptoms (i.e., scores ≥ 14 on the depression subscale of the Hospital Anxiety and Depression Scale (HADS), 17 a history of psychosis, severe cognitive impairment (Mini Mental State Examination (MMSE) scores < 27), 18 hospitalization in the previous 6 weeks, ongoing mind–body practice (≥ once a month).
Participants received a US$40 gift card for completing each study visit. All participants provided full informed consent, and the study protocol was approved by the institutional review board at our institution. The study was registered at Clinicaltrials.gov (NCT03289546).
Procedures
After providing informed consent and confirmation of eligibility, participants completed baseline assessments. Using a 2 × 2 factorial design, participants were then randomized to aerobic training (AT) alone, MT alone, both AT and MT, or neither (usual care (UC)). The randomization schedule was generated in “R” (cran.us.r-project.org) and was based on a permuted block randomization scheme with small (size 2–4), random-sized blocks. Study investigators and personnel involved in data analysis were masked to participants’ allocation. The mindfulness instructors were aware that participants received MT, but they were masked to their AT status (i.e., whether they also received AT). The research assistant was not masked, but all study assessments were independently completed by the participants using an electronic interface with no involvement of the study staff.
Interventions
MT sessions were held at the Miriam Hospital Centers for Behavioral and Preventive Medicine and followed the curriculum of the mindfulness-based stress reduction (MBSR) program 12 with 3 notable exceptions: sessions lasted 2 hours (vs. the usual 2.5 hours), there was no intensive all-day class, and yoga exercises were omitted to avoid confounding effects of yoga exercise on cognitive function. Participants first attended an orientation session during which they were introduced to the purpose, content, and schedule of the intervention, followed by a 2-hour MT session once a week for 8 weeks. The curriculum included (1) training in awareness of sensations (“body scan”), a technique based on the cultivation of attention to bodily sensations that normally go unnoticed; (2) training in the awareness of the sensations of breathing; (3) training in directing the attention to simple activities of daily life and in recognizing when the attention is no longer focused on a specific object of attention; and (4) “open awareness,” a practice in which participants are instructed to just notice events (physical sensations, sounds, thoughts, and emotions) arising from moment to moment and cultivate an attitude of openness and acceptance. In addition, participants practiced mindfulness exercises for 30 minutes daily on their own with the guidance of a digitally recorded, standardized, guided mindfulness practice provided in different formats (CD or MP3 file) depending on the participant’s preference; MP3 files were uploaded onto the patient’s smartphone. Sessions were led by a certified MT instructor with > 5 years’ teaching experience.
AT participants attended 3 exercise sessions/week for 12 weeks (held at a local YMCA and supervised by the research assistant). The curriculum included a 10-minute warm-up, followed by 40 minutes of aerobic exercise (walking on a treadmill), and a 10-minute cool down. Participants were instructed to maintain their heart rate at 65–75% of the age-predicted max heart rate using a heart rate monitor provided to each participant at study inception or to exercise at an intensity of 12–13 in the Borg scale of the rate of perceived exertion. 19 The Physical Activity Readiness questionnaire 20 was administered prior to each session to identify symptoms (e.g., chest pain, dizziness, and injury) that contraindicated participation in exercise training.
MT + AT participants attended 2 AT sessions and 1 MT session/week for 8 weeks, followed by 3 AT classes per week for 4 additional weeks. The MT intervention in the MT + AT group was identical in content, number of sessions, and individual MT practice to that delivered in the MT alone condition.
UC participants received a free YMCA voucher and a copy of the MT practice recording at study completion. All participants continued the medications prescribed by their healthcare provider.
Study Assessments
Assessments were performed at baseline, end of treatment (EOT), and 6 months post-baseline.
Primary Outcomes: Feasibility and Acceptability
Metrics of feasibility included retention and attendance, with pre-determined retention and attendance rates of ≥ 80% and ≥70%, respectively, indicating good study feasibility. For MT and MT + AT, individual mindfulness practice at home was tracked using a self-report diary; completion of ≥70% of exercises indicated good feasibility. Acceptability was assessed using a program satisfaction survey (ratings ranged from 1—“not at all” to 5—“very much”) which was completed at EOT.
Secondary Outcome: Cognitive Function
At the baseline, EOT, and 6-month visits participants independently completed a neuropsychological battery using a tablet device to measure attention (Digit Symbol Substitution Test [DSST]), executive function (F-A-S Verbal Fluency Test [FAS]), and episodic memory (International Shopping List Test [ISLT]) available at www.cogstate.com. Each test took 3 to 5 minutes to complete and all participants underwent a practice trial prior to the administration of cognitive assessments. Scores from these 3 cognitive domains were used to calculate a single composite score (
Descriptive Variables
Information on socio-demographic characteristics (age, sex, race/ethnicity, and education) was collected using validated self-report forms. Information on medical history was abstracted from electronic medical records. Depressive symptoms were assessed with the 7-item depression subscale of the HADS (normal values ≤ 7). 17
Statistical Analysis
Analyses were performed according to the intention to treat approach. Retention, attendance, and acceptability scores at EOT and 6 months were calculated separately for each condition and compared using t-test, ANOVA, or chi-squared tests as appropriate. It should be noted that none of these measures (retention, attendance, or acceptability) had missing data, and thus, these are appropriate methods for comparing conditions. The ZAVEN score was calculated by converting DSST, FAS, and ISL scores to standardized z-scores (i.e., by subtracting the baseline group mean μ from score X and dividing it by the group baseline standard deviation (X−μ/σ), and then averaging the standardized z-scores).
Mixed effects longitudinal models were used to estimate effects on the ZAVEN composite score, controlling for baseline ZAVEN values. Models included a random intercept to adjust for repeated measures of the outcome over time within participant. Time was entered as a categorical variable to allow for comparisons of mean outcomes between time period. A single model allowed for all pairwise comparisons between groups with the goal of estimating effect sizes and corresponding confidence intervals.
Results
Three participants’ cohorts were recruited between April 2016 and May 2018. Overall, 159 participants were screened; 87 (54.7%) were eligible; 43 (49.4%) consented to participate in the study; and 37 (23.3% of all screened) were randomized to AT (n = 10), MT (n = 10), MT + AT (n = 10), or usual care (n = 7). One participant withdrew from the study immediately after randomization and was not included in the analysis (Figure 1—Consort diagram). Baseline participants’ characteristics are shown in Table 1. Participants were 70.1 (SD = 6.8) years of age on average, 67% were female, and 89% reported at least some college-level education. Over half of the study sample had a history of hypertension and high cholesterol, a third had a history of depression, and all were physically inactive per study’s inclusion criteria. Baseline MMSE scores were normal across all groups. CONSORT diagram. Baseline Demographic Characteristics by Intervention Group. Values are means (SD) for continuous variables and n (%) for categorical variables; participants had the option of selecting more than 1 race. AT, aerobic training; HADS, Hospital Anxiety and Depression Scale; MMSE, Mini Mental State Examination; MT, mindfulness training; MT + AT, Mindfulness training + aerobic training; UC, usual care.

Primary Outcomes: Feasibility and Acceptability
Participant’s Satisfaction Ratings.

Values are means (SD). All satisfaction ratings range from 1 = not satisfied to 5 very satisfied.
AT, aerobic training; MT, mindfulness training; MT + AT, Mindfulness training + aerobic training.
Secondary Outcome: Cognitive Function
Mean Unadjusted Cognitive Scores by Intervention Group.
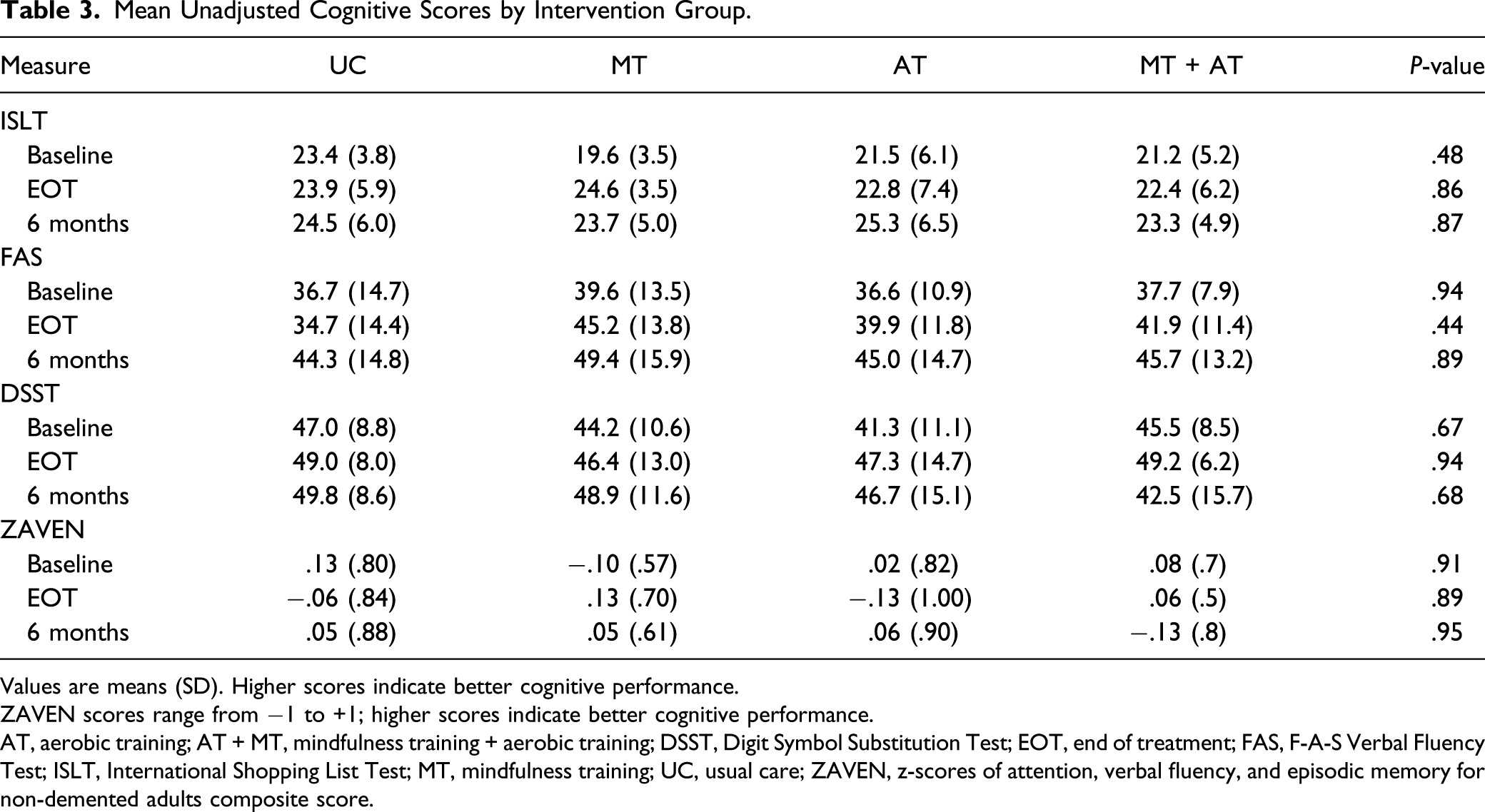
Values are means (SD). Higher scores indicate better cognitive performance.
ZAVEN scores range from −1 to +1; higher scores indicate better cognitive performance.
AT, aerobic training; AT + MT, mindfulness training + aerobic training; DSST, Digit Symbol Substitution Test; EOT, end of treatment; FAS, F-A-S Verbal Fluency Test; ISLT, International Shopping List Test; MT, mindfulness training; UC, usual care; ZAVEN, z-scores of attention, verbal fluency, and episodic memory for non-demented adults composite score.
To examine potential cohort effects, models were also analyzed separately within each of the 3 study cohorts; results were consistent with the overall findings.
Discussion
Overall, this pilot study met pre-defined criteria for feasibility for overall study retention as well as for MT session attendance and individual mindfulness practice completion. Exercise session attendance in the AT group was below the feasibility threshold and was further reduced in the combined MT + AT group. Participants reported moderate-to-high satisfaction with the structure and components of the interventions and perceived them as beneficial.
Our 97% retention rate at intervention completion compares favorably with that of both exercise-based rehabilitation and standard MT such as the mindfulness-based stress reduction program (both around 50%). 23 AT session attendance was sub-optimal in both AT and MT + AT, but overall enjoyment as well as ratings for specific AT components (including number of classes) were satisfactory. Because time commitment is a known barrier to the attendance of exercise-based rehabilitation programs, this could have been a similar barrier to attendance in our study; alternatively, unforeseen personal factors did not allow participants to join classes.24,25
While this feasibility study was designed to provide preliminary estimates of effect and was not powered to detect differences in cognitive outcomes, we found preliminary evidence of a possible effect of MT on cognitive function, compared to AT and UC, that was maintained at follow-up. Our preliminary results do not suggest a synergistic effect of exercise and MT. This finding was somewhat surprising because we expected to observe the greatest improvements in cognitive function in the group combining mindfulness and aerobic exercise training. A possible explanation is that, while we ensured that aerobic exercise during the AT sessions reached moderate levels of exercise intensity, participants did not attend a sufficient number of AT sessions, as shown by the sub-optimal attendance reported in both the AT and AT + MT groups. In addition, intervention duration may be a factor. A recent meta-analysis suggests that a longer intervention duration (i.e., 6–12 months) is needed to demonstrate effects of physical activity on cognitive function. 4 Future studies should consider a longer duration of the AT and more accessible forms of aerobic exercise (e.g., neighborhood walking), especially considering recent findings that light aerobic exercise increases brain volume. 26
To our knowledge, there is only 1 (ongoing) study exploring effects of MT and AT on cognitive function, 27 and thus, the literature does not offer many insights. A 2 × 2 RCT of cognitive training and aerobic activity found no differences between groups, but used a very active control condition, 11 while a small RCT suggested that combined aerobic and cognitive training could lead to larger effects than either intervention alone. 9 Evidence from an fMRI imaging study indicated that such combined approaches may increase brain plasticity. 10
Strengths of this study include the rigorous design, rigorous assessments of cognitive function, and the use of standardized interventions. There are also important limitations, including restricting enrollment to English-speaking individuals and the low representation of minorities. Further, because this study had a small sample size and was not powered to detect effects on cognitive function, results need to be interpreted with caution. 28 In addition, we cannot exclude that the greater training volume per se, with the associated additional attention received by the instructors, might have affected cognitive outcomes. If this were the case, we should see greater effects in the arms with greater training volume, that is, in the AT and the MT + AT group. Instead, there were no additional benefits in the AT and the MT + AT conditions, and attendance actually declined with a higher training volume. In a future, larger study, a generic health education condition could be used to control for the attention received from the instructors. Despite these important limitations, these preliminary findings constitute a promising line of investigation that deserves to be pursued in a fully powered trial.
In sum, the MT, AT, and MT + AT interventions demonstrated overall good general feasibility in older adults at-risk for dementia; yet, added incentives or a different type of exercise intervention may be needed to increase attendance to AT and a longer intervention may be needed to improve effects of AT on cognitive measures. These preliminary estimates provide proof-of-concept evidence that MT may improve cognitive function in individual at risk of dementia that need to be confirmed in a larger RCT. Showing that MT (alone or combined with exercise) improves cognitive function in older individuals at risk of dementia could have a significant impact on the prevention of dementia and age-related cognitive decline.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by a grant from the Norman Prince Neurosciences Institute to Drs. Salmoirago-Blotcher and Snyder and by a grant from the Center for Mindfulness at Brown University to Dr. Salmoirago-Blotcher. The funding agencies were not involved in the study design; in the collection, analysis and interpretation of data; in the writing of this report; and in the decision to submit this article for publication.