
Abstract
Male osteoporosis is underappreciated. Little is known about men’s knowledge of osteoporosis and how much men are at risk. This study surveyed men’s knowledge of osteoporosis and their risk factors with reference to women in the primary care setting in Macau, China. A convenience sample of 302 men and 635 women aged 18 to 90 years completed questionnaires comprising the Osteoporosis Knowledge Assessment Tool and the One-Minute Osteoporosis Risk Test. Their risks of osteoporosis were assessed with the Osteoporosis Self-Assessment Screening Test. Men and women, who were aged 55 years or below, had similarly limited knowledge of osteoporosis. People aged above 55 years had significantly less knowledge; men had less knowledge than women only in this age-group. If questions specific to women or menopause were excluded, men had similar knowledge as women. A higher proportion of men than women had risk factors as more men consumed alcohol or smoked tobacco. Similar proportions of men and women reported a loss of 1 inch in body height after age 40. After age 55, 29.2% men were at medium to high risk of osteoporosis. This study concludes that health education and primary prevention of osteoporosis should be promoted to men starting in middle-age.
Introduction
Osteoporosis is not rare or trivial in men. The lifetime risk of nontraumatic fracture for a 60-year-old man was found to be about 25% (Nguyen, Eisman, Kelly, & Sambrook, 1996). Osteoporotic fractures lead to higher morbidity and mortality in men than in women (Endo, Aharonoff, Zuckerman, Egol, & Koval, 2005; Kannegaard, van der Mark, Eiken, & Abrahamsen, 2010). This is an important issue in public health and its prevention needs the public’s awareness. Such awareness is however inadequate even in the medical literature. A systematic review in 2011 identified only 13 published articles studying older men’s knowledge of osteoporosis, all reporting limited knowledge (Gaines & Marx, 2011). Even men with fractures were only 55% correct in a knowledge test (Wilson et al., 2011).
Previous studies consistently reported that men had less knowledge of osteoporosis than women (Doheny, Sedlak, Estok, & Zeller, 2007; Juby & Davis, 2001). Most knowledge assessment tools were however primarily focused on women’s risk factors rather than specifically for men (Gaines et al., 2011). It is uncertain if the types of questions would affect the assessment result. Moreover, specific areas of deficiency in men’s knowledge are more informative than the overall generalized result. That 32.6% of men got the correct answers in a test is less useful than that 35.8% were correct on the benefit of exercise in preventing osteoporosis (Lee & Lai, 2006). To facilitate opportunistic prevention and patient education of osteoporosis in the time-constrained primary care, more information on patients’ specific deficiencies in knowledge and behavior is required.
An individual’s bone mass reaches the peak usually around age 30 years and declines thereafter. Of the limited studies on men’s knowledge of osteoporosis, very few recruited younger subjects or the age distribution of the sample was not specified (Ali, Shonk, & El-Sayed, 2009; Tung & Lee, 2006). Risk factors of osteoporosis could have been present but neglected for decades before fractures occur. Young men’s knowledge and risk factors of osteoporosis are particularly underresearched.
This study surveyed the knowledge and risk factors of osteoporosis in primary care patients over the full age range of adulthood. To better understand men’s knowledge and risk factors of osteoporosis, this study compared the male and female recruits. The aim was to contribute information for future patient education and prevention of male osteoporosis.
Method
This study recruited consecutive patients, aged 18 years or above, attending adult clinics at two primary care health centers from mid-July to mid-September 2011 in Macau city, China. The two centers served about 53% of the Macau population. A research assistant and a nurse assistant explained the aim of the study to the patients in the waiting rooms. They distributed the questionnaires to the patients who gave verbal consent to participate in the study. Help was given to those who had difficulties with the questions. Illiterate patients were excluded. In addition to basic information such as the patient’s age and gender, the questionnaire consisted of the Osteoporosis Knowledge Assessment Tool (OKAT) and the One-Minute Osteoporosis Risk Test. The body mass index was taken by the nurse/research assistant at the side-room. The study population was divided into three age-groups: Group A (below 35 years), Group B (35-55 years), and Group C (above 55 years).
The OKAT was chosen to assess the recruits’ knowledge of osteoporosis as it was (a) a validated tool with good internal consistency (Cronbach’s alpha of .69), (b) designed to include the younger age-group of 25 to 44 years, and (c) suitable for self-administration by the respondents (Winzenberg, Oldenburg, Frendin, & Jones, 2003). It had been used by other studies on bone health (Long, Thiny, Sandler, & Gangarosa, 2010; Ryder, Kessler, Jones, & Shorr, 2007). OKAT consists of 20 questions of which six are gender-specific (e.g., Question 18 on bone loss after menopause). The answers are in the form of “Yes/No/Don’t Know.” A score of +1 was given to each correct answer and 0 otherwise. It was translated into Chinese for this study. The Chinese version was presented to a group of family practice trainees and tutors for comments and then tested in a pilot study by the author (WCP) with face-to-face interviews of 406 conveniently sampled patients. Cronbach’s alpha for the Chinese version was .742.
The One-Minute Osteoporosis Risk Test, with 19 questions, was designed by the International Osteoporosis Foundation for the public awareness of the presence of risk factors of osteoporosis (International Osteoporosis Foundation, 2011). Although it is not designed to assess an individual’s absolute risk, it includes the questions in the FRAX® (WHO Fracture Risk Assessment Tool) and has official multilanguage translations. The Chinese version was used in this study. In this test, three questions are specific to women and one to men. So the possible maximum number of risk factors is 18 for women and 16 for men.
To assess the osteoporosis risk of the recruits, this study used the Osteoporosis Self-Assessment Screening Tool (OST). It was designed by a study of women in eight Asian countries (Koh et al., 2001). OST derives an index (an integer) from the equation of (body weight − age) * 0.2. It was validated in Asian men (Kung, Ho, Ross, & Reginster, 2005; Li-Yu, Llamado, & Torralba, 2005), African Americans (Sinnott, Kukreja, & Barengolts, 2006), and American Whites (Adler, Tran, & Petkov, 2003; Skedros, Sybrowsky, & Stoddard, 2007). It identified men with diminished bone mineral density with a sensitivity of 83% to 90% and specificity of 64% to 66% (Adler et al., 2003; Kung et al., 2005; Li-Yu et al., 2005; Skedros et al., 2007). This study adopted the Asian indexes (OST for Asians or OSTA) of −1 to −4 as medium risk and that of less than −4 as high risk (Li-Yu et al., 2005; Saetung, Ongphiphadhanakul, & Rajatanavin, 2008).
Statistical Methods
The data analysis was done with the R statistical packages. A study of Chinese older men reported that about 33.0% answered correctly a knowledge test on osteoporosis (Lee & Lai, 2006), and another study of Chinese women reported that 58% women had heard of osteoporosis (Saw et al., 2003). With the assumptions that the recruits would have similar proportions and that the female/male ratio of the study population would be 1.5, the estimated sample size for men was 58 for the null hypothesis (no difference between the proportions) at α = .05 and power = .80. The data collection for this study continued till the number of male recruits of all three age-groups exceeded 60.
This study used the t test and ANOVA to compare the knowledge scores and the Wilcoxon rank-sum test to compare the risk indexes between men and women. For the risk factors, as the possible maximum number was 18 for women but 16 for men, the two-sample proportion test was used to test the null hypothesis that there was no difference between the two genders. In essence, this test used 18 and 16 as the denominators to compare the probabilities of risk factors in women and men, respectively, and the test-statistic was a chi-squared value. Linear regression was used to detect any association between the knowledge score and the risk factors. For all statistical tests, p < .05 was taken as statistically significant.
The study was approved by the Health Bureau, Government of Macau Special Administrative Region, China.
Results
Recruited Population
Of 1,097 people approached, 937 questionnaires with valid data were returned and analyzed. The overall response rate was 85.4%; 77.4% for men and 89.8% for women (χ2 = 30.923, p < .001). Of the 937 recruits, 302 were men (32.2%) and 635 women. The age range was 18 to 90 years (mean 48.3 ± 16.1) for men and 18 to 86 years (mean 45.7 ± 14.5) for women. The distribution in different age-groups is shown in Table 1.
Distribution of Age, Knowledge Scores, and Risk Factors Among Respondents of Different Age-Groups.
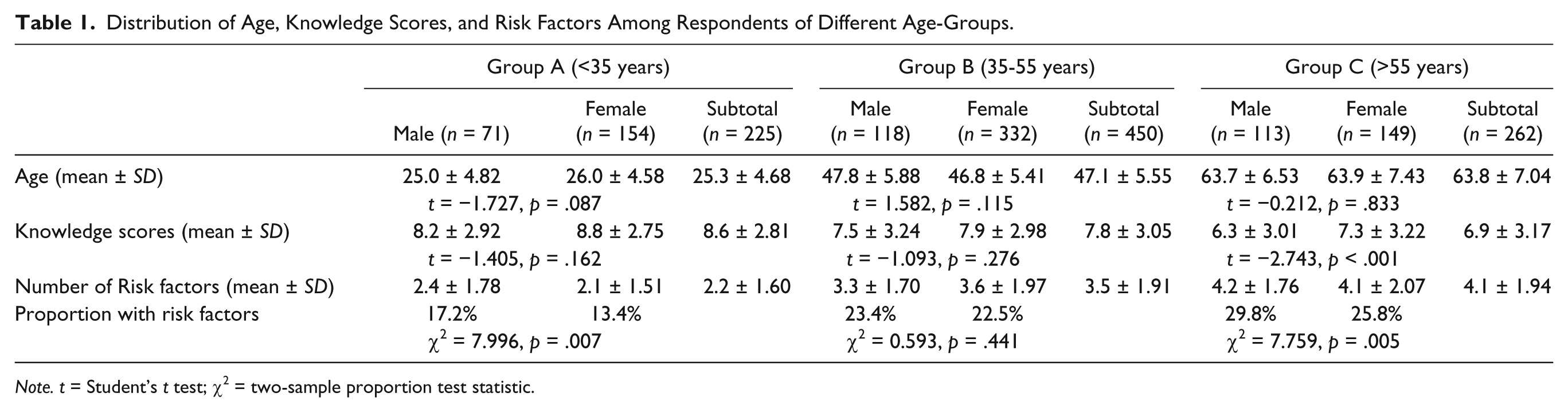
Note. t = Student’s t test; χ2 = two-sample proportion test statistic.
Knowledge
The knowledge scores were normally distributed (Shapiro–Wilk test W = 0.984, p < .001). The mean score of all the respondents was 7.69 ± 3.09 out of the maximum of 20 (i.e., 38.5% were correct); 7.18 ± 3.16 (35.9%) for men and 7.94 ± 3.02 (39.7%) for women. The mean score decreased from 8.6 to 7.3 as the age advanced (Table 1). Men older than 55 years had significantly less knowledge than the younger groups (ANOVA F = 19.503, p < .001). In all age-groups, the women scored higher than the men in knowledge. However this difference was statistically significant only in the group aged >55 years in which men scored significantly less than women (t = −2.743, p < .001).
The male respondents scored significantly lower than the females in the questions about the incidence of osteoporosis or fracture (Questions 4, 8, 9; Table 2), bone loss after menopause (Question 18), and calcium supplement (Question 15). Of all the men, 92.4% considered it easy to know their risk of osteoporosis, 84.1% agreed that osteoporosis usually caused symptoms before fracture, and 82.8% considered two glasses of milk adequate for the daily calcium intake.
Frequency of Correct Answers to the Knowledge Questions by Gender Groups.

The percentage of respondents within their gender group who chose the correct answers.
If the gender-specific questions (4, 6, 8, 9, 18 19; Table 2) were excluded, men’s total score (5.1 ± 2.26) was similar to women’s (5.3 ± 2.24, t = −1.353, p = .177), even in the older age-group (4.5 ± 2.36 vs. 5.0 ± 2.31, respectively, t = 1.298, p = .196).
Risk Factors
The number of risk factors of osteoporosis in each respondent ranged from 0 to 11. For the whole sample, the mean number of risk factors was 3.4 ± 1.97 and median 3.0; 3.4 ± 1.87 (out of 16) for men and 3.4 ± 2.03 (out of 18) for women. Overall, significantly more men had risk factors than women (two-sample proportion test χ2 = 14.107, p < .001). The 35 to 55 years group was different from the other groups as similar proportions of men and women had risk factors (Table 1).
A much larger proportion of men smoked cigarettes or consumed alcohol. If these two risk factors were excluded, the mean number of risk factors was 2.85 ± 1.68 for men and 3.28 ± 2.00 for women (two-sample proportion test χ2 = 0.021, p = .884).
Men were significantly more likely to have 30 minutes of physical activity per day (Table 3). There were 195 men and 422 women aged 40 years or above. Of these, 31 men and 100 women reported the loss of 1 inch or more of body height after age 40 (χ2 = 2.866, p = .090).
Frequency of “Yes” Answers to the One-Minute Osteoporosis Risk Test by Gender Groups.
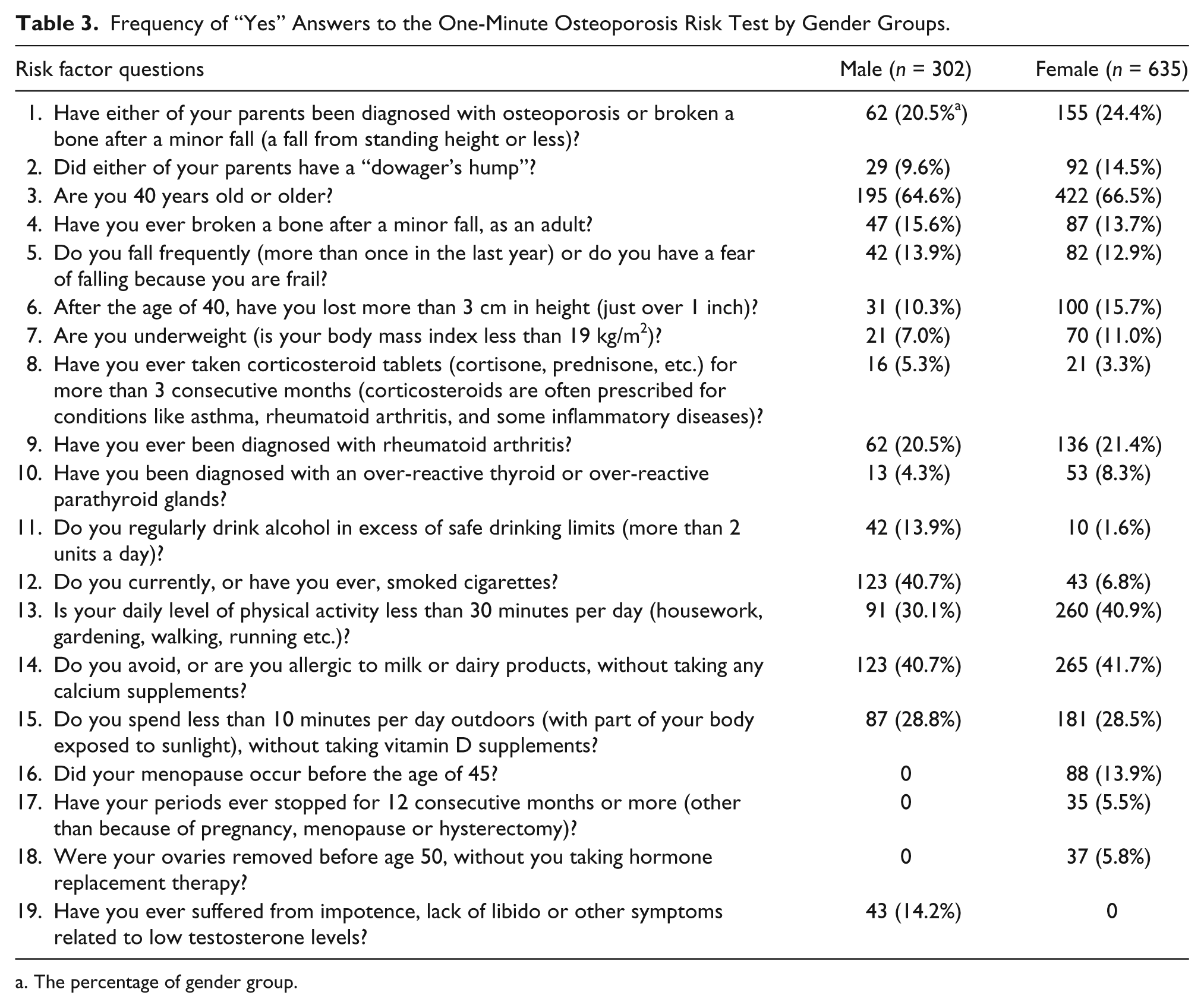
The percentage of gender group.
Knowledge and Risk Factors
For the whole sample, there was no significant association between the score of knowledge and the number of risk factors, either for men (r = 0.091, p = .116) or women (r = 0.022, p = .576). However, for women aged >55 years there was marginally significant correlation between knowledge score and the number of risk factors (r = 0.165, p = .045). For either men or women, there was no significant association between the knowledge score and the presence of individual risk factors.
Estimated Risk
Before age 55 years, the OST indexes were high for either gender (Table 4). For the respondents aged >55 years, women were significantly at higher risk than men (mean risk index −1.42 ± 2.28 vs. 0.31 ± 2.37, Wilcoxon test W = 11245, p < .001). But 29.2% of men aged >55 years were at medium or high risk.
Distribution of OSTA Scores Among Respondents of Different Age Groups.

Discussion
This study recruited 302 men and 635 women aged 18 to 86 years attending two large outpatient clinics, with various reasons of encounter, for their knowledge and risk of osteoporosis. Before age 55 years, men’s score of the knowledge test (OKAT) was similar to women’s. After this age, women had significantly better knowledge than men. If the questions related to gender difference like menopause were excluded from OKAT, men achieved similar scores as women. The One-Minute Osteoporosis Risk Test reported the same mean of 3.4 factors for men (out of the possible maximum of 16) and for women (out of the possible maximum 18). Higher proportion of men than women had risk factors because higher proportion of men than women smoked tobacco or consumed alcohol. There was no association between knowledge and the number (or presence) of risk factors in either gender. Of men aged >55 years, 29.2% had an OST risk index ≤−1.0, suggesting moderate or high risk of osteoporosis and the need for further investigation of bone mass density.
The respondents in this study had limited knowledge of osteoporosis (38.5% correct in the OKAT), a result comparable with the studies in other places like the United States (Gaines et al., 2011; Shawa, Favela, & Diaz, 2011) or Hong Kong (Lee & Lai, 2006). Unlike other studies, this study reported better knowledge in the younger respondents, and men in the younger age-groups had similar knowledge as women. But it was uncertain if age was a confounder as this study did not ask for education levels. Women in the older age-group had better knowledge than men probably because they perceived more risk from the disease or they had been the main target for health education of osteoporosis. Another probable explanation could be the questionnaire bias. The OKAT was “developed with a primary focus on risk factors related to women’s health issues (e.g., the effect of menopause on bone health),” so much so that a specific tool for the assessment of men’s knowledge of osteoporosis was proposed (Gaines et al., 2011; Gaines & Marx, 2011). With the exception of the question on calcium supplement, the recruited women in this study were more likely than men to be correct in the knowledge test only on the gender-related questions (Table 2). This study however cannot give a firm verdict. Taking away the female-specific questions affected only the performance by the respondents aged above 55 years, the relatively knowledgeable younger men and women were not affected. The feasibility of a separate assessment tool for men needs further research. A potential bias from this study was the significantly lower response rate from men (77.4%) than women (89.8%). It was uncertain if the men who chose to respond were more knowledgeable. Nonetheless, the high response rate from men indicated that the majority had been recruited and that the potential bias would be small.
The results of this study indicate that future education in male osteoporosis needs to emphasize the knowledge that (a) men are not immune to osteoporosis but would encounter it at a relatively later age than women, (b) osteoporosis is a silent disease before the occurrence of fracture, and (c) men themselves can do a lot to prevent osteoporosis by appropriate physical exercise and diet.
The One-Minute Risk Test identified few risk factors (the median of 3 for both genders). It must be emphasized that this test is not for the assessment of the risk of osteoporosis, but rather to help people become aware of their own risk factors. For this purpose, its usefulness in this study’s population is doubtful. Half of the respondents had three risk factors and might perceive a false security. However, the test gave some important information: few respondents had adequate exposure to sunlight or physical exercise, and men started to lose body height after the age of 40 years (not statistically different from women). The latter information is particularly important though a subjective one. It suggests that male osteoporosis might start in middle age. This study also reported that more men than women had risk factors of osteoporosis except the age-group of 35 to 55 years. However, no explanation could be identified for the similar proportions of affected men and women aged 35 to 55 years.
In spite of the low scores for the One-Minute Risk Test, this study’s respondents began to have medium to high risk of osteoporosis after age 55 years as reported by the OST. In this age-group, 65.8% of women and 29.2% men were at such risks. The OST might appear crude as it includes only body weight and age for assessing the risk. Nevertheless, it is an inexpensive and simple clinical prediction rule in the office setting to select people for further screening, especially in places where dual-emission X-ray absorptiometry is not readily accessible for population screening. Although this study had not asked the recruits for any previous tests of bone mass density, it was very likely that most of the men had never had such tests. The data support the need for preventive measures for a large number of men after middle age.
Limitations
This study recruited a consecutive convenience sample of patients in primary care. The strength of this study was the inclusion of the whole range of adult age. But further study is required to validate whether the findings were applicable to the general population. There were two possible sampling biases. First, men were less likely than women to consult doctors. Compared with the general population, male patients in health centers might be more conscientious about health, have received more information about bone health, and have more lifestyle risk factors. Second, we did not exclude patients with proven osteoporosis or previous bone mass density investigations. Given that previous investigations could be associated with better knowledge (Winzenberg, Oldenburg, Frendin, De Wit, & Jones, 2005), this might contribute to the better knowledge in women aged >55 years as they were more likely than men to have had these investigations.
Another limitation is that this study did not include the patients’ income, education level, and current illnesses. As osteoporosis is predominantly an age- and gender-related disease, this study confined the variables to age and gender only. The association between other factors and men’s knowledge of osteoporosis requires further study.
This study translated the OKAT into Chinese and this version had not been formally validated. The question “There are no effective treatments for osteoporosis available in the United States” was not modified to suggest the unavailability of treatment even in technically advanced countries. Our respondents’ knowledge score was congruent with the results of other studies, suggesting that this OKAT version could be applied to our local population.
Conclusion
Men, like women, had limited knowledge of osteoporosis. Significant difference in knowledge of osteoporosis between men and women was reported in the over 55 years age-group. Men in this age-group had little knowledge of osteoporosis although a large proportion was at medium or high risk. Whether men need a specific osteoporosis knowledge assessment tool remains controversial. But more education and preventive measures are surely required for men starting from middle age.
Footnotes
Acknowledgements
We are grateful for the research and nurse assistants for data collection. We thank Dr. Chau-Sha Kwok of the Fai Chi Kei Health Centre and Dr. Ping-Wan Li of Hac Sha Wan Health Centre for their assistance in this research. We also thank Dr. K. F. Lam of the Department of Statistics and Actuarial Science, the University of Hong Kong, for his comments on the statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.