
Abstract
This study sought to determine the feasibility and clinical value of using a novel mobile application (app) to record the muscle/physical activity (PA) of caregivers. In all, 23 caregivers were enrolled and they were trained to use the app and a wearable device that automatically recorded their care activities and PA/burden. Data were collected for 42 days. Muscle activity was measured for 3 weeks during maximum voluntary isometric contraction (MVIC) and PA. Approximately 80% of the caregivers agreed that they conveniently used the wearable device through the mobile app. The most active %MVIC was noted for the back muscles during feeding assistance. As regard subjective pain evaluation, back pain was the most prevalent and pain level in the left knee was the highest. Incorporating mobile apps with wearable devices to record every activity of the caregivers may be feasible and can provide valuable clinical data for optimizing their pain management.
Introduction
Care for older adults and people who require assistance because of their inability to perform activities of daily living (ADL) independently has expanded from family- and community-based assistance to the public social system and market-based assistance. In a rapidly aging society (older adults 7% in 2000 but 14% in 2017, and expected as 20% in 2026), the demand for care is increasing because of changes in the family structure and expansion of social assistance (Cha et al, 2015). Herewith, caregivers (69.3% aged ≥50 years) can take only brief breaks and, therefore, overwork when moving, lifting, transporting, and/or changing the positions of care recipients—increasing the risk of work-related musculoskeletal injuries (Kwon et al., 2013, Park et al., 2009). As such, novel approaches/technologies should be developed to provide not only high-quality care to patients, but also to reduce the physical burden of the caregivers.
Recently, various education-based smartphone application (app) programs that connect wirelessly to the Internet have gained popularity (Garg et al., 2016; Hewitt et al., 2020; Nicholl et al., 2017; Petrozzi et al., 2019). However, studies have rarely focused on developing apps for the prevention of musculoskeletal injuries among caregivers. On the other hand, such apps might facilitate efficient physical activity (PA) management and exercise-related education dissemination—minimizing the risk of musculoskeletal disorders in caregivers. Yet, they have excellent accessibility and convenience via mobile devices (e.g., smartphones).
Accordingly, the purpose of this study was twofold; first we aimed to develop (and explore the feasibility of) a mobile app that could assess simple/relevant data as regard the PA of caregivers. Second, we aimed to examine their subjective work-related musculoskeletal symptoms in correlation/addition to the data provided by the app.
Methods
Participants
In this prospective study, the convenience sampling method was used to include caregivers based on the following criteria: caregivers working ≥4 days per week, having no difficulty in communication, having ability to understand questions, and having no history of musculoskeletal disorder before working as caregivers. All volunteered to participate after having understood the study purpose. Caregivers with central nervous system disorders, peripheral neuropathy, neuromuscular disorders, history of brain/spinal or other types of surgery, joint contracture, hypersensitivity to surface electrodes, dementia, cognitive dysfunction, alcohol or drug abuse, inability to communicate in Korean language were excluded.
The caregivers who had attended at one long-term nursing care facility for older adults and at two residential homes for people with severe disabilities were screened according to the inclusion/exclusion criteria. Those who met the inclusion criteria were given a brief explanation of the study as well as a participant information sheet that they could keep and refer to. The consent form was distributed to the willing caregivers.
This study was approved by the Research Ethics Committee of the relevant institute and conducted in accordance with the ethical principles of the Declaration of Helsinki. Written informed consent was obtained from all participants.
App for Caregivers
An Android-based mobile app that could record and assess data regarding care activities was installed in a 10-inch tablet PC (provided to all 23 participants). It was designed to allow full daily self-monitoring of care activities and physical burden, and automatically record PA through a wireless surface electromyogram (EMG) device (Delsys Trigno Wireless EMG System, Delsys Inc., Boston, MA, USA) and a smart band (Mi Band 1A, Xiaomi Inc., Beijing, China), which were synchronized with the app (Figure 1). It functioned as the gateway to transmit data collected by the EMG sensors (regarding muscle activity [MA] with maximal voluntary isometric contraction [MVIC]) and smart band (regarding PA—in terms of the number of daily steps, walking distance, calories, etc.) to a platform. To normalize the EMG signals from the upper trapezius, biceps brachii, and erector spinae muscles, manual muscle examination was performed to measure MVIC (Figure 1). A data communication chip was inserted into the tablet PC to facilitate network connection (Internet) for data transmission (Figure 1). The mean values (mV) of the data obtained from the upper trapezius, biceps brachii, and elector spinae muscles using the EMG device were divided by MVIC and normalized %MVIC values were determined. Data analyses were performed using the normalized values (%MVIC).
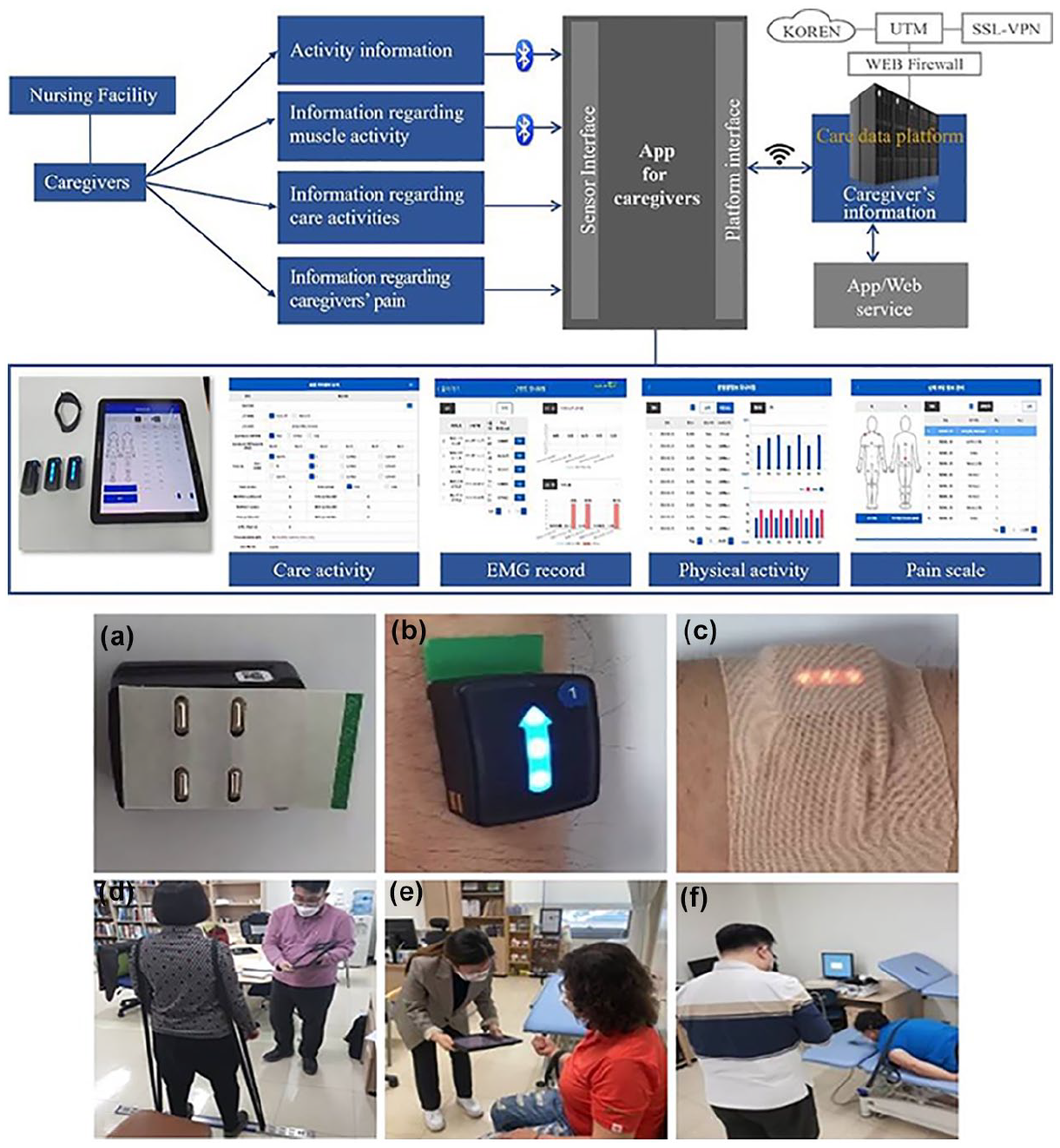
(Upper figure) Flowchart showing the study plan for caregivers’ data collection and evaluation using the app): (a) Preparing a sensor and placing a gel patch, (b) attaching the sensor on the body, (c) applying elastic tapes to fix the sensor, (d) MVIC of the trapezius muscle (shoulder), (e) MVIC of the biceps brachii muscle (arm), (f) MVIC of the erector spinae muscle (back).
To evaluate the usage of the tool by the participants, all actions were automatically logged by the device for further analysis. Moreover, the participants were asked to fill in a tailored technology acceptance questionnaire at the end of the study. Caregivers used the app during the study period for 6 weeks to document information on physical burden due to care activities.
Data entered into the app were transmitted/stored in the Care Service platform within the 00 information technology (IT) network. The platform was implemented in the IT system within a closed network environment of the 00. Security management was performed based on the unified threat management approach (a system in which individual network security functions are integrated) as well as a system requiring access to secure sockets layer virtual private network (Figure 1).
Outcome Measures
MA in caregivers
To assess MA, a commercial Internet of Things–based EMG device (Delsys Trigno Wireless EMG System, Delsys Inc., Boston, MA, USA) was used (Lugones-Sanchez et al., 2022). This system was integrated with EMG sensors and 6-axis sensors to measure body movement and was connected to the app (Figure 1). Changes in MA before and after app use were analyzed at the workplace. EMG data were collected on three times during the study period: Day 1, Day 21 (Days 0–21), and Day 42 (Days 22–42). To collect data, the EMG sensors were attached to three body areas (upper trapezius, biceps brachii, and erector spinae muscles). Data were collected based on the type of care activity. The collected data were analyzed using an EMG software (EMG-works Analysis-Delsys, Boston, MA, USA) with a sampling rate of 1 kHz. To eliminate noise, a 20-Hz low-pass filter and a 500-Hz high-pass filter were used. Muscle signals were treated as the root of the mean square.
The surface EMG sensor on the upper trapezius muscle was attached at half line between the C7 spinous process and acromion lateral border. Pertaining to the upper trapezius, manual resistance with a custom made stabilizer with a rope was applied to the arm while the shoulder was elevated in the standing position. Furthermore, the surface EMG sensor on the biceps brachii muscle was attached at mid-arm level. MVIC strength of the biceps brachii was assessed at 90° elbow flexion on a bench customized with a rope, and the sensor for the erector spinae muscle was attached laterally to the L1/L2 spinous process. Participants were restrained across the lower legs and requested to wear a chest harness to resist trunk extension in prone position on the table for us to measure the MVIC value of their erector spinae. Strong verbal encouragement and visual feedback by a physiatrist blinded to the participants were provided to request the participants “elevate, pull, and extend as hard and fast as possible.” Each participant performed three 5-second MVICs with a 60-second rest between attempts for each shoulder, arm, and back. Values obtained in the middle 3 seconds were used for data analysis. The PA of the caregivers during the study period was measured using the wearable smart band connected to the app. Data were analyzed based on the performed activities.
Caregivers’ response of satisfaction questionnaire
A satisfaction questionnaire was used to evaluate the degree of inconvenience caused by smart bands and EMG sensors worn during care activities; the questionnaire was scored based on a 5-point Likert scale as follows: strongly disagree (1), disagree (2), neutral (3), agree (4), and strongly agree (5). It is used to evaluate a system’s usability in a relatively quick and reliable fashion (Kosar et al., 2022). The satisfaction parameter had six statements as follows: the smart band was inconvenient to use during care activity, EMG device was inconvenient to use during care activity, app was inconvenient to use during care activity, tablet PC was convenient as a medium for app use, and app could be used more efficiently with a smartphone than with a tablet PC. The parameters were analyzed by calculating the average value of each statement in the satisfaction parameter.
To identify the physical burden on the musculoskeletal system (during assisting with transfer, reposition, feeding, and toileting) of caregivers, the following data were collected each day: personal characteristics, the level of physical difficulty experienced by the care recipients such as ADL state score (1: independent patients [total score = 0], 2: patients with minimal need for assistance [total score ≤ 25%), 3: patients with moderate need for assistance [total score between 26% and 50%], 4: patients with maximum need for assistance [total score between 51% and 75%] and 5: patients with total need for assistance [total score > 75%]; Rodakowski et al., 2012), duration/frequency of care activities, pain scale (visual analog scale [VAS]), MA, and PA (e.g., the number of steps).
Caregivers’ subjective perception of pain level
To examine the subjective perception of musculoskeletal symptoms due to care activities, pain in six body areas (neck, shoulder, arm/elbow, hand/wrist, back, and leg) was assessed using a VAS, with a pain scale ranging between 0 and 10 points. The participants were instructed to rate pain (i.e., aching, throbbing, stiffness, burning sensation, insensitivity, and shooting) in each of the body areas. They recorded data (frequency/duration) on each of the four types of care activities (transfer, reposition, toileting, and feeding). After 3 weeks of using the app until the last day of this study, participants assessed the recorded their activity.
Statistical Analysis
The sample size was calculated based on a previous study (Shebib et at., 2019) and taking into account the pain scale. At a significance level of 0.05 and a statistical power of 95%, the calculated total number of participants was 20. Considering a 10% dropout rate, the final number of participants was set to 23. Mean values were compared using the Mann–Whitney U tests. A generalized linear model was used to compare daily PA and EMG device–obtained data. A repeated-measures two-factor analysis of variance was performed in addition to multiple comparisons in case of a statistically significant difference. Pearson coefficients were used for correlation analyses. Statistical analysis was performed using the IBM SPSS software package for Windows (version 19.0, Chicago, IL, USA). Statistical significance was set at p < .05.
Results
Participant Characteristics
This study enrolled a total of 23 female participants (mean age, 55.17 ± 4.59 years; mean height, 159.87 ± 4.42 cm; and mean weight, 61.39 ± 8.24 kg). Only four participants (17.4%) were aged 41–50 years, 13 participants (56.5%) were aged 50–60 years, and six participants (26.1%) were aged >60 years. Majority of care recipients (90%) were not independent and many required assistance for feeding. The caregivers worked the night shift for 20% of their work days.
Among the four types of care activities, toileting accounted for the highest volume of work per day (duration: 114.92 minutes; frequency: 28.58). Regarding the average daily PA during work hours, the number of steps based on the work type was 126,443 (working on week days), 10,243 (working in the afternoons), and 7,078 (working at nights). Therefore, the activity level was the highest on weekdays, followed by afternoons and nights.
Muscle Activity
Shoulder muscles were the most active during assistance during reposition (mean %MVIC, 51.70), followed by toileting (mean %MVIC, 47.81), transfer (mean %MVIC, 45.40), and feeding (mean %MVIC, 44.30) after 3 weeks of app use. In contrast, arm muscles were the most active during assistance with transfer (mean %MVIC, 24.13), followed by reposition (mean %MVIC, 20.61), toileting (mean %MVIC, 15.17), and feeding (mean %MVIC, 11.48) after 3 weeks of app use. Back muscles were the most active during assistance with feeding (mean %MVIC, 63.91), followed by transfer (mean %MVIC, 63.35), reposition (mean %MVIC, 47.25), and toileting (mean %MVIC, 47.04) after 3 weeks of app use. No significant differences were noted in MVIC before and after the study.
App-Related Survey Outcomes
All 23 caregivers responded to the questionnaire, and the results revealed the level of inconvenience experienced by the participants when using the smart band (score, 1.83 ± 0.98), EMG device (score, 2.43 ± 0.95), and the app (score, 2.26 ± 1.10). The average score regarding the suitability of using the tablet PC as a medium for the app was 3.57 ± 1.04. Furthermore, the respondents reported that smartphones would be a better choice than tablet PCs for this app (average score, 4.13 ± 1.01).
Pain Level
The prevalent type of pain reported by caregivers was experienced in the back (n, 1235 times), followed by the right wrist (n, 958), right shoulder (n, 653), left wrist (n, 584), and left shoulder (n, 467). The highest subjective perception of pain was in the left knee (3.09), followed by the right knee (2.97), left ankle (2.92), and back (2.87). Subjective perception of the pain level in all types of care activities correlated negatively with the ADL status of the care recipients (correlation coefficients; transfer: −.067, reposition: −.043, toileting: −.098, feeding: −.031), indicating that higher pain level reflected lower ADL (Table 1). Pain correlated positively with “assistance with bathing” (frequency/duration) (correlation coefficients; frequency: .210, duration: .229) and “assistance with going out” (correlation coefficient; frequency: .265; Table 1).
Correlation Coefficients Between Care Activities and Subjective Pain Assessment.
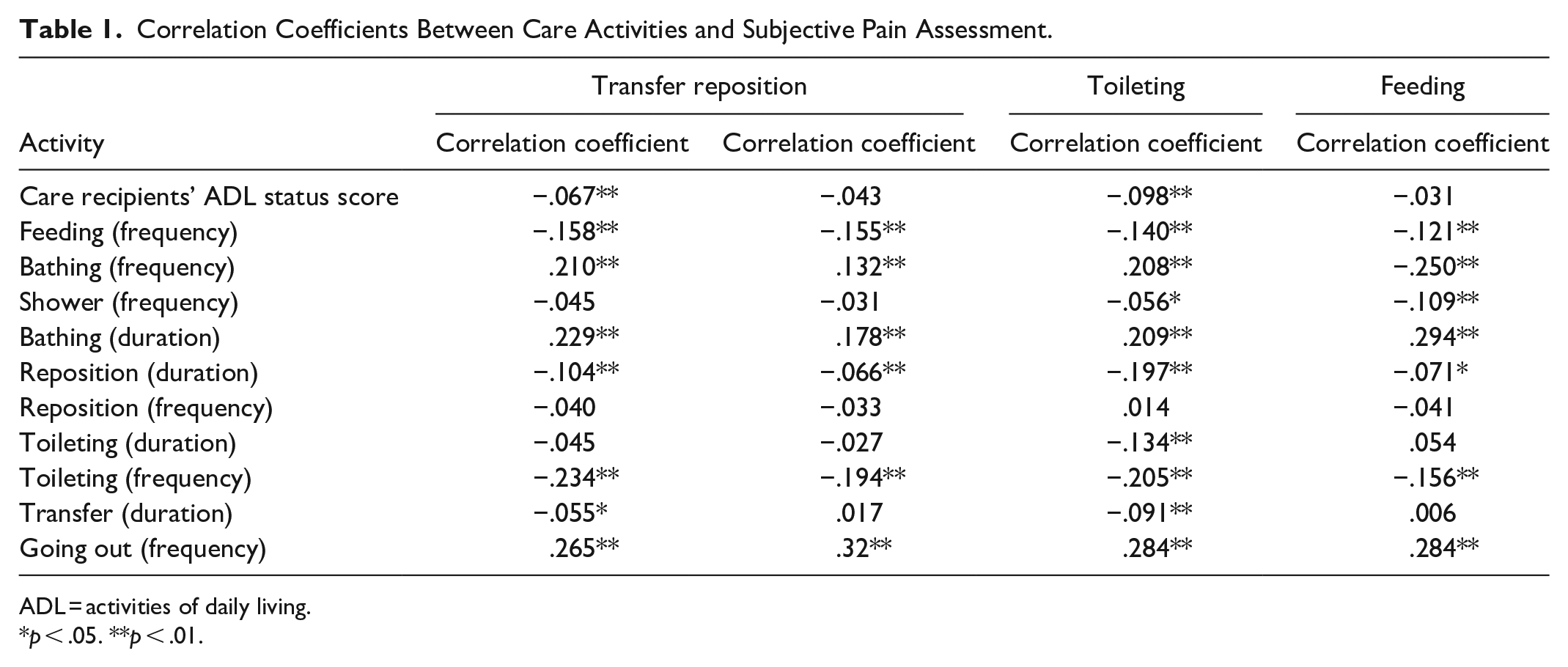
ADL = activities of daily living.
p < .05. **p < .01.
Discussion
Our findings suggest the feasibility of a novel mobile app connected to a wearable device for recording data on care activities, levels of pain, MA and PA during care activities in caregivers. To our best knowledge, this is the first study to develop a comprehensive app that can efficiently/effectively track the activities of caregivers.
In our study, the questionnaire survey showed that approximately 80% of caregivers agreed that both the EMG device and smart band could be used conveniently with the app. The primary reason for the remaining 20% of negative reviews was the inconvenience of wearing these devices. In addition, smartphones were preferred to tablet PCs. Therefore, in the future, it plans to develop a built-in device PA and MA measurement using smartphone as the medium.
Several previous studies have attempted to introduce mobile activity recognition (Joe et al., 2013; Loh et al., 2018), and various medical experiments have been performed for collecting activity data from physicians, nurses, and patients. However, there are few mobile apps for caregivers to record data regarding their care activities. Therefore, this new/mobile app may be a useful and an accurate method of assessing physical burden in caregivers and efficiently aiding caregivers to plan/develop strategies of reducing physical burden during care-related activities.
Our findings revealed that the low back was the most commonly reported site of musculoskeletal discomfort and had the highest %MVIC. This finding is consistent with that of a previous study that characterized the burden and musculoskeletal discomfort in informal caregivers caring for adults with chronic physical disabilities (Darragh et al., 2015).
In this study, subjective perception of pain levels in all four types of care activities correlated negatively with the ADL status of the care recipients, indicating that higher pain levels resulted in lower ADL status scores. It is, therefore, high physical burden reported by the caregivers is not surprising. A previous study identified the level of care as a significant predictor of caregiver injury (Darragh et al., 2015). Caregivers reported peak pain severity in the left knee, which reached a VAS score of 3.09. The median pain severity (6 weeks) was below the VAS score of 3 for several body sites. In contrast, a previous study demonstrated that the pain level ranged between VAS scores of 3 and 5, perhaps because of the fact that informal caregivers’ injuries may be associated with caregiving tasks, and yet not many caregivers received training on how to perform these tasks efficiently or safely (Darragh et al., 2015). Therefore, professional caregivers may experience relatively lower pain levels than informal caregivers.
In addition, pain correlated positively with “assistance with bathing” (frequency/duration) and “assistance with going out” (frequency). Therefore, ADL status of the care recipients, assistance with bathing (frequency/duration), and assistance with going out (frequency) were risk factors that can increase the physical burden on their musculoskeletal system in this study.
In this study, quantitative assessment was performed using an EMG device and a smart band; qualitative assessment was performed via a questionnaire survey conducted among the caregivers.
Our study has some limitations. First, our sample size was relatively small, thus further validation through large-scale studies is required. Second, the experiments were performed in a relatively short period. Thus, further studies are warranted to assess the long-term benefits of using this mobile app. Third, the sample was comprised predominantly of caregivers of long-term nursing care facility for older adults and residential homes for people with severe disabilities, and there was a lack of inclusion of other clinical settings.
In conclusion, this study indicated the feasibility of incorporating mobile apps with wearable devices to record MA, pain level, and PA in caregivers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Translational Research program for Care robots funded by the Ministry of Health & Welfare, Republic of Korea [grant number HK19C0017].
Ethics Statement
This study was approved by the Daegu Catholic University Research Ethics Committee (approval no. MDCR-20-013) and conducted in accordance with the ethical principles of the Declaration of Helsinki. Informed consent was obtained from all subjects involved in the study.