
Abstract
Purpose
Physiotherapy (PT) is an essential part of care for improving function and increasing community participation in children with cerebral palsy (CP). Combining animal-assisted intervention (AAI) with PT (AA-PT) offers a unique approach, potentially boosting motivation and participation in ambulatory children with CP. This case series piloted AA-PT integrating a rehabilitation dog for children with CP, to enhance walking and balance training.
Methods
Four ambulatory children with CP (7–16 y.o.a, GMFCS I-II, 3 girls, 1 boy) participated in an 8-week individualized AA-PT intervention. Assessments at baseline (0 weeks), pre-intervention (8 weeks), post-intervention (16 weeks), and follow-up (24 weeks) included Kids Mini BESTest, timed up and go (TUG), dual task cost (DTC), and spatiotemporal parameters. The AA-PT included weekly 60-min sessions integrating a rehabilitation dog in walking and balance training. Visual analog scales (VAS) assessed perceived comfort, safety, enjoyment, and confidence while walking with and without the rehabilitation dog.
Results
Individual-responder analysis showed improvements in Kids Mini BESTest scores, reduced DTC, and increased walking speed for all. Children reported higher enjoyment, confidence, safety, and comfort when walking with the rehabilitation dog.
Conclusion
AA-PT integrating a rehabilitation dog may enhance balance, dual-task cost, walking speed, and confidence in ambulatory children with CP.
Keywords
Introduction
Cerebral palsy (CP) is a permanent neurological condition, acquired in utero, at birth or in infancy, and primarily impacts movement and posture, which leads to delays in gross motor function (Rosenbaum et al., 2007). Physiotherapy (PT) can help to address gross motor function, such as walking and balance ability, motor impairments such as spasticity and weakness, and secondary complications such as contractures (Aisen et al., 2011; Odding et al., 2006). Ultimately, PT aims to increase quality of life while promoting participation and independence in functional and community activities (Aisen et al., 2011; Novak et al., 2020). Further, neurorehabilitation principles recommend repetitive, high-intensity training of relevant tasks in purposeful environments to ensure motor learning and transferability of skills for functional improvements (Maier et al., 2019). Dosage and practice required to achieve a meaningful level of learning necessitates high levels of motivation and engagement from client, especially children. This poses a challenge to pediatric physiotherapists to balance the need for high repetitions of task-specific practice, and the importance of making therapy appealing so that children will actively engage in training. Interventions for walking and standing balance for children with CP are extremely diverse with no consensus on which are most effective (Moreau et al., 2016; Novak et al., 2020; Qian et al., 2022). The development of evidence-based walking and balance interventions targeting participation in age-appropriate activities through enjoyment and motivation are needed.
Animal-assisted PT interventions (AA-PT) are an innovative approach that may enhance walking and balance training. Rehabilitation dogs are specialized service mobility dogs trained to work alongside rehabilitation professionals in therapeutic contexts to provide support during interventions. This support can be similar to a portable gait aid (e.g., walker) or a stationary support (e.g., parallel bar). A study by Rondeau et al. (2010) demonstrated that a walking retraining intervention supported by a rehabilitation dog improved walking speed and walking patterns for individuals post-stroke (Rondeau et al., 2010). Service dogs have been shown to also improve emotional and psychological wellbeing for children living with disabilities, and therapy dogs have been shown to reduce fear and pain when patients are in medical environments (Elmacı & Cevizci, 2015; Yap et al., 2017). Integrating a rehabilitation dog into walking and balance training for children with CP has yet to be explored. This case-series piloted an 8-week, individualized AA-PT where children with CP worked with a rehabilitation dog as part of their balance and walking training. The effects on postural control, dual-task cost, spatiotemporal parameters of walking, and perceived confidence, comfort, and safety of walking were evaluated.
Methods
This was a prospective, consecutive case series exploring an individualized 8-week AA-PT for standing balance and walking training working with a rehabilitation dog. Four participants with CP were evaluated across four time points over 24 weeks: baseline at 0 weeks (BL), pre-intervention at 8-weeks (PRE), post-intervention at 16 weeks (POST), and follow up at 24 weeks (FU).
The rehabilitation dog (Loki) was trained by the Fondation Mira (Montréal, QC). At the time of the intervention, Loki was a 3.5-year-old Labrador-Bernese Mountain Dog cross, weighing approximately 39 kg and standing 20 inches tall (at the shoulder). A harness with a rigid handle of different heights was fit to each participant following standard practice for fitting gait aids (Figure 1) (Palisano et al., 2016). A physiotherapist with pediatric and neurorehabilitation experience was trained by the Fondation Mira (Montréal, QC) as the service dog handler and worked alongside Loki for each session to deliver the intervention. Loki's welfare was a primary factor in ensuring effective treatment at each session. A protocol was developed and strictly followed by a veterinarian specializing in Veterinary Sports Medicine and Rehabilitation (author R.P.) to ensure that Loki was closely monitored and performing at his best.
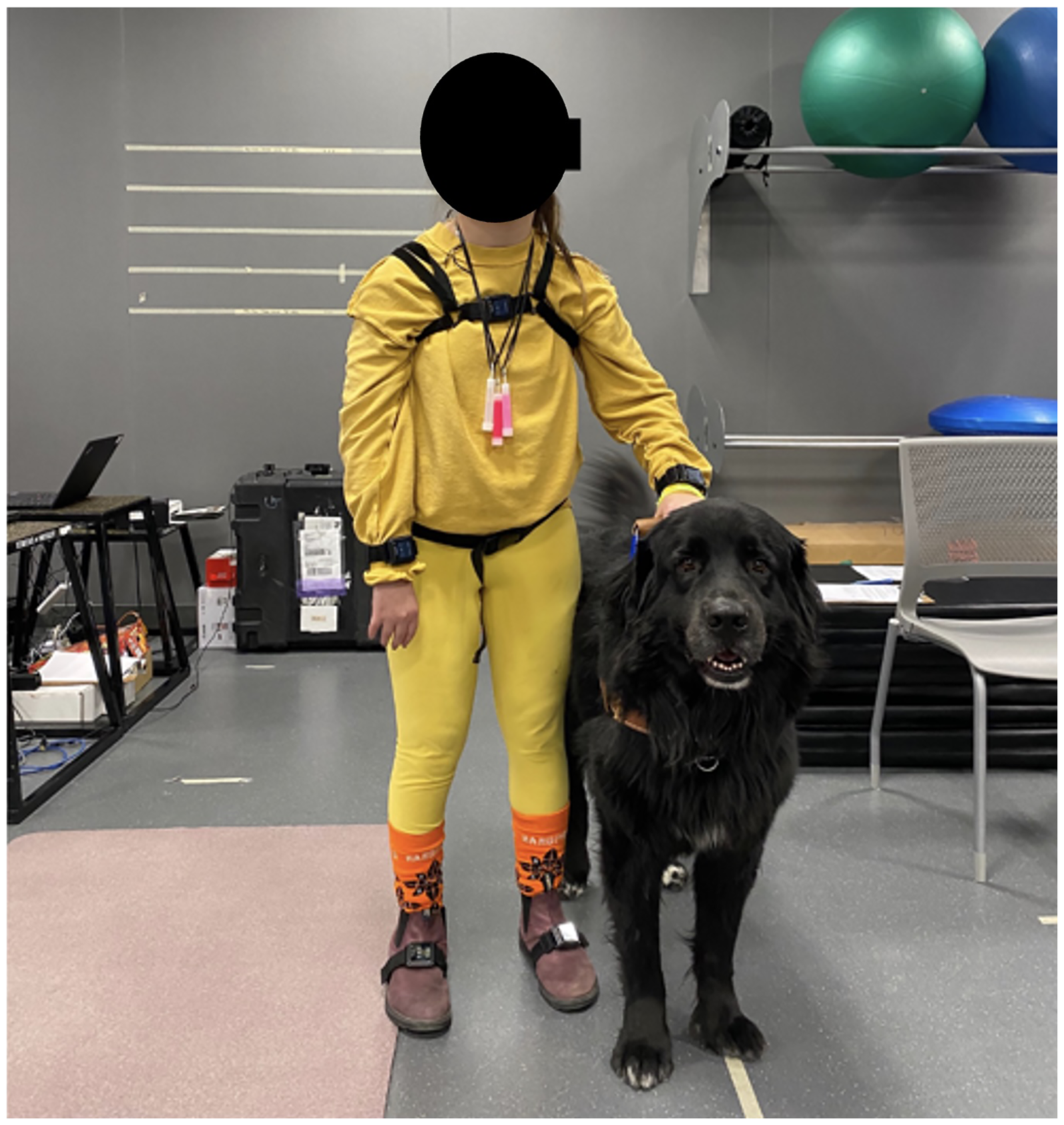
The rehabilitation dog, Loki, with a participant during a research assessment.
Loki's training provided him the skills to respond appropriately to changes in walking, sudden losses of balance and to act as a stable support surface during various dynamic and static rehabilitation activities. Loki's position changed frequently throughout the data collection and intervention sessions. When walking, Loki walked alongside the participant, similar to a gait aid. When working on balance activities he could be positioned in front or to the side to provide more (bilateral) or less support (unilateral) (see Intervention section). This study was approved by the institutional human and animal research ethics boards at the University of Saskatchewan, Canada. Each participant and their family and/or guardian reviewed and provided informed consent for the research assessments and PT intervention.
Participant Recruitment
Recruitment of participants was completed through a local pediatric outpatient clinic. Inclusion criteria for participation were a diagnosis of CP, age 7–18 years, a gross motor classification (GMFCS) of I or II, goal of improving walking and/or postural control ability, currently ambulating in community with or without assistive devices, able to follow verbal instructions independently and give verbal instructions to the rehabilitation dog. Exclusion criteria for participation in the intervention were: medically advised to not participate in exercise programming, unable to commit to weekly intervention of 8-weeks, uncontrolled seizure disorders, fear or allergy to dogs, and typical gait aid that required bilateral use of arms for weightbearing.
Outcome Measures
At BL, participants and their families self-reported demographics. Clinical outcome measures included Timed Up and Go (TUG), Timed Up and Go with a cognitive task (TUG-COG) and the Kids Mini BESTest (Dewar et al., 2019; Dewar, Claus, Tucker, Ware et al., 2017; Horak et al., 2009). TUG and TUG-COG were collected at all four time points. Scores for the TUG and TUG-COG were used to evaluate changes in dual tasking ability and dual task cost. The TUG is a reliable and responsive measure for measuring balance, anticipatory postural control and functional mobility (Carey et al., 2016; Williams et al., 2005). Minimal Detectable Change (MDC) values in the TUG test of 1.40 (GMFCS I) and 2.87 s (GMFCS II) and a Minimal Clinically Important Difference (MCID) (effect size 0.8) of 0.36 s (GMFCS I) and 0.87 s (GMFCS II) are reported for children with CP (Carey et al., 2016). Using TUG and TUG-COG scores, dual-task cost (DTC) as described by Kelly et al. (2010) and Carcreff et al.(2019) was also calculated at each time point. DTC has been shown to be an important aspect of gait performance in children with CP and can successfully be used to determine the effects of a cognitive task on walking ability (Carcreff et al., 2019). The Kids Mini BESTest was collected at BL, PRE, and POST and measures certain aspects of postural control (anticipatory and reactive postural control, sensory orientation, and dynamic balance during walking.), as described by the Systems Framework for Postural Control (Dewar, Claus, Tucker, Ware et al., 2017; Horak, 2006; Horak et al., 2009). The Kids Mini BESTest has a maximum score of 28, with a higher score meaning better performance and the MDC is reported as a minimum of 3 points overall (Dewar et al., 2019; Dewar, Claus, Tucker, Ware et al., 2017).
At each timepoint, participants completed a spatiotemporal analysis of their walking while using their typical assistive devices (e.g., AFOs) by walking on a 10-meter instrumented walkway (GAITRite ®; CIR Systems, Inc., NJ, USA). Footwear (e.g., indoor running shoes), walking aids and equipment (e.g., AFOs) were kept consistent for each assessment and during the intervention. They completed six walking trials at their self-selected speed (Johnson et al., 2020; Mohamed & Appling, 2020); three without and three with Loki. To account for changes in speed due to gait initiation and termination, participants were asked to start and stop at target lines placed one metre from each edge of the mat (Johnson et al., 2020; Wang et al., 2012).
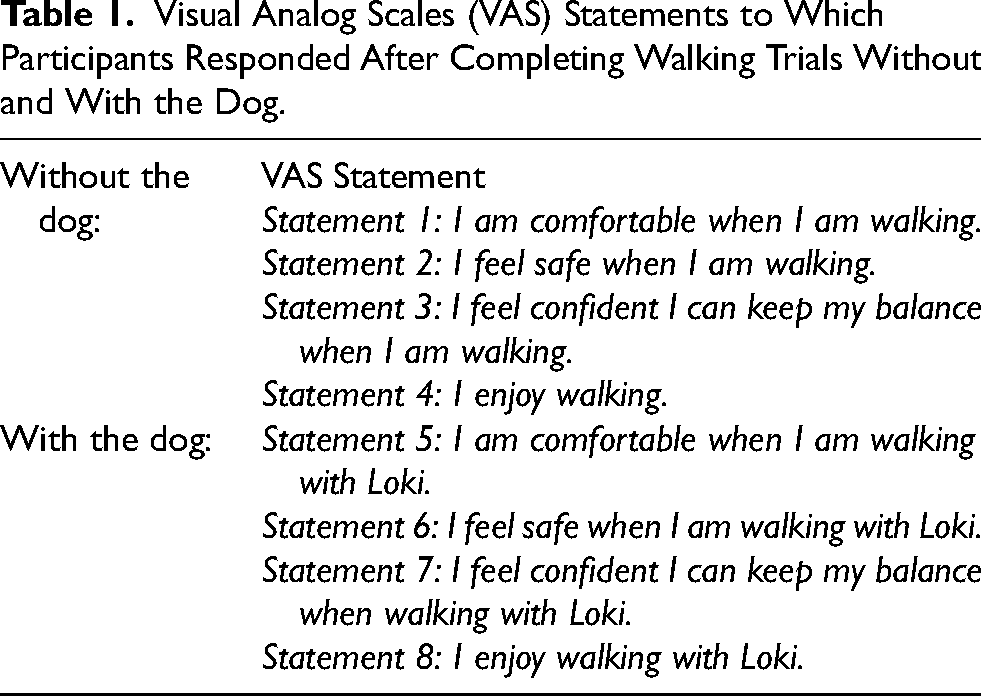
Visual Analog Scales (VAS) captured participant confidence, comfort, safety, and overall enjoyment at all time points. Participants completed VAS (Table 1) after walking without and then after walking with Loki by marking along a 10 cm line. Distance from the far left indicated agreement of each statement with 0 cm aligned with a rating of “Not at all”, and 10 cm on the far right indicating a rating of “Completely”. Measurements were converted to a percentage (e.g., 5 cm was converted to 50%).
Visual Analog Scales (VAS) Statements to Which Participants Responded After Completing Walking Trials Without and With the Dog.
Intervention
Each child participated in an individualized 8-week AA-PT for walking and postural control ability assisted by the rehabilitation dog, Loki. Participants completed an initial PT assessment to guide intervention planning. The intervention was guided by the principles of the Task-Oriented Approach (Shumway-Cook et al., 2022) and Systems Framework for Postural Control (SFPC) (Horak, 2006) and individualized to address the goals and priorities identified by the child and their family. Children attended in-person, once per week for training. Training sessions were divided into three parts: alignment and static postural control, walking strategy, and real-world walking (see Table 2).
Intervention Goals, Outline, and Systems Framework for Postural Control (SFPC)
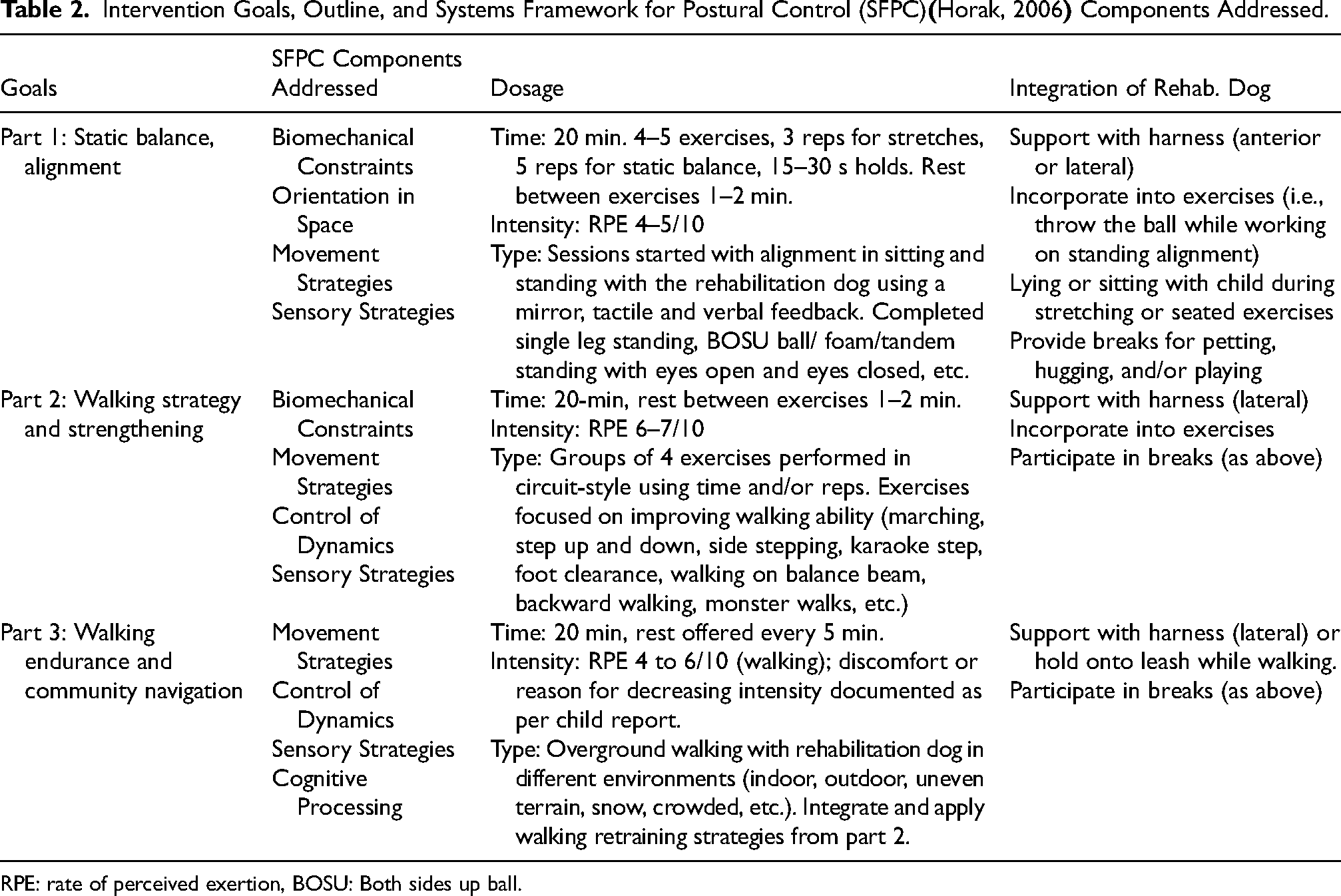
RPE: rate of perceived exertion, BOSU: Both sides up ball.
The intervention was guided by each participant to provide ownership and decision-making over their time in the intervention and to encourage participation and engagement (Holt et al., 2020; Jackman et al., 2022). Real-world practice incorporated retraining activities in community settings (indoor and outdoor) across various terrains, using stairs, and navigating crowds. Intensity was guided by the participant's subjective report and the rate of perceived exertion scale (RPE) on a 10-point scale (Fragala-Pinkham et al., 2015). Rest breaks of up to 5 min were incorporated after each part of the intervention and were also provided if the participant voiced fatigue and/or other symptoms (e.g., pain).
Loki was integrated into each component (Figure 2) as a stability support or mobility aid (e.g., holding the harness while walking), or reward (e.g., sit-to-stand training with dog cuddle). Participants could choose to walk with Loki as active recovery, with planned rest breaks dedicated to interacting with Loki. Children consented to not participate in other PT programming during the 8-weeks but did continue in their typical hobbies, sports, or other registered activities. There were no changes made to any of their assistive devices or typical home programming during the intervention.

Images of children participating in AA-PT with Loki the rehabilitation dog.
Data Analysis
Descriptive statistics including means and standard deviations (SD) were calculated for a person-based analysis. Participants were classified as having made an improvement, a deterioration, or no change when walking with Loki (with dog: WD) and without Loki (no dog: ND) based on a change equal to or greater than the MDC or MCID (if available), or a percentage change of more than 10% between time points (Mayo et al., 2014). As children with CP are known to present with diverse impairments that may vary from one time to another due to natural changes and compensations, the BL period of eight weeks was used as a control period. The eight-week FU period was used to see if any changes following the intervention were maintained. The BL and FU periods were used as part of the individual responder analysis to compare changes during these periods and compare them to the 10% threshold. MCID for cadence and walking speed for children living with CP were used to determine if significant changes occurred between each time point and when walking with or without Loki (Johnson et al., 2020). MCID values for a medium effect size were used as follows; Cadence as 5.90% (GMFCS I) and 7.60% (GMFCS II) of normal, and walking speed as 8.70% (GMFCS I) and 6.80% (GMFCS II) of normal. Normal values were calculated as the mean baseline value without Loki for each participant. GAITRite® analysis software was used to obtain spatiotemporal footfall data with first and last steps removed from each trial. Step length, percentage time spent in double support (%timeDS), percentage time spent in swing (%timeSw), percentage time spent in stance (%timeSt), walking speed, and cadence were summarized for analysis. Data were analyzed within separate limbs defined as more affected (MA) and less affected (LA) limbs as reported by the participant and confirmed by the physiotherapist assessor. For VAS Scales, a difference of more than 1 cm (or 10%) (Powell et al., 2001) was used as a significant improvement or deterioration.
Results
Demographics and Case Specific Information
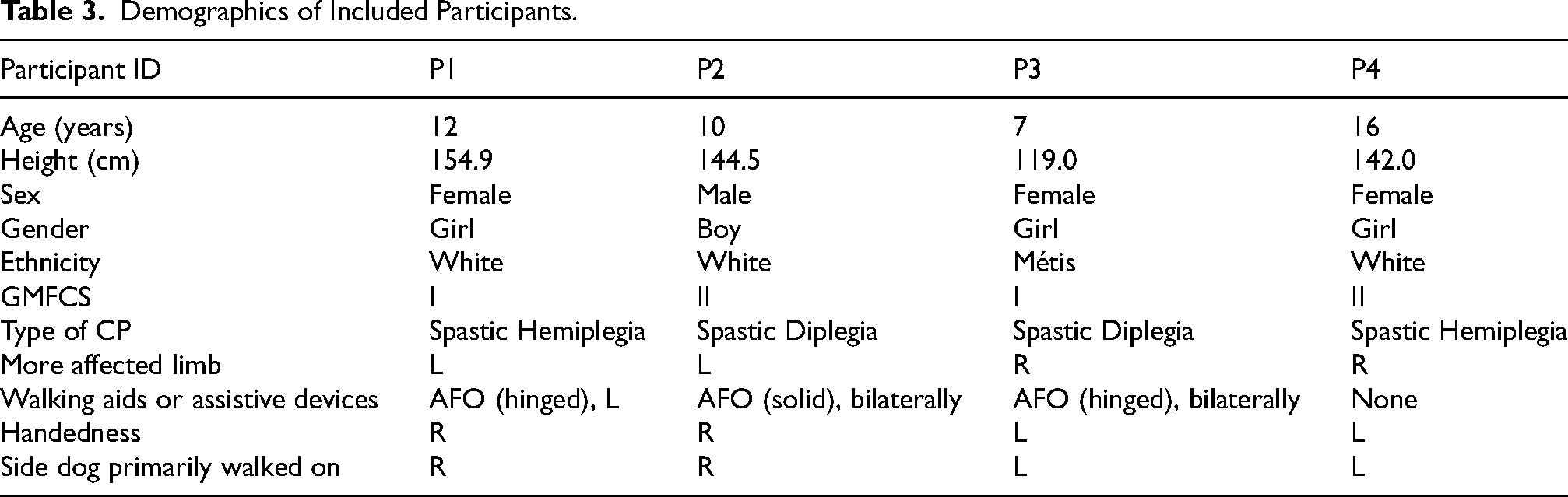
Four ambulatory (GMFCS I-II) children living with CP (P1, P2, P3 and P4), ages 7–16 years old, three identifying as girls and one identifying as a boy participated (Table 3). All participants completed each of the four research assessments and participated in all weekly training sessions of the 8-week intervention. There were no adverse events reported or observed throughout the entire 24-weeks. Priorities identified by all four participants and their families at PRE assessment centered on improving walking endurance, walking ability in peer-group activities, lower extremity strength, and better balance in day-to-day activities.
Demographics of Included Participants.
Mean TUG and TUG-COG times and DTC are described in Table 4 and Figure 3.
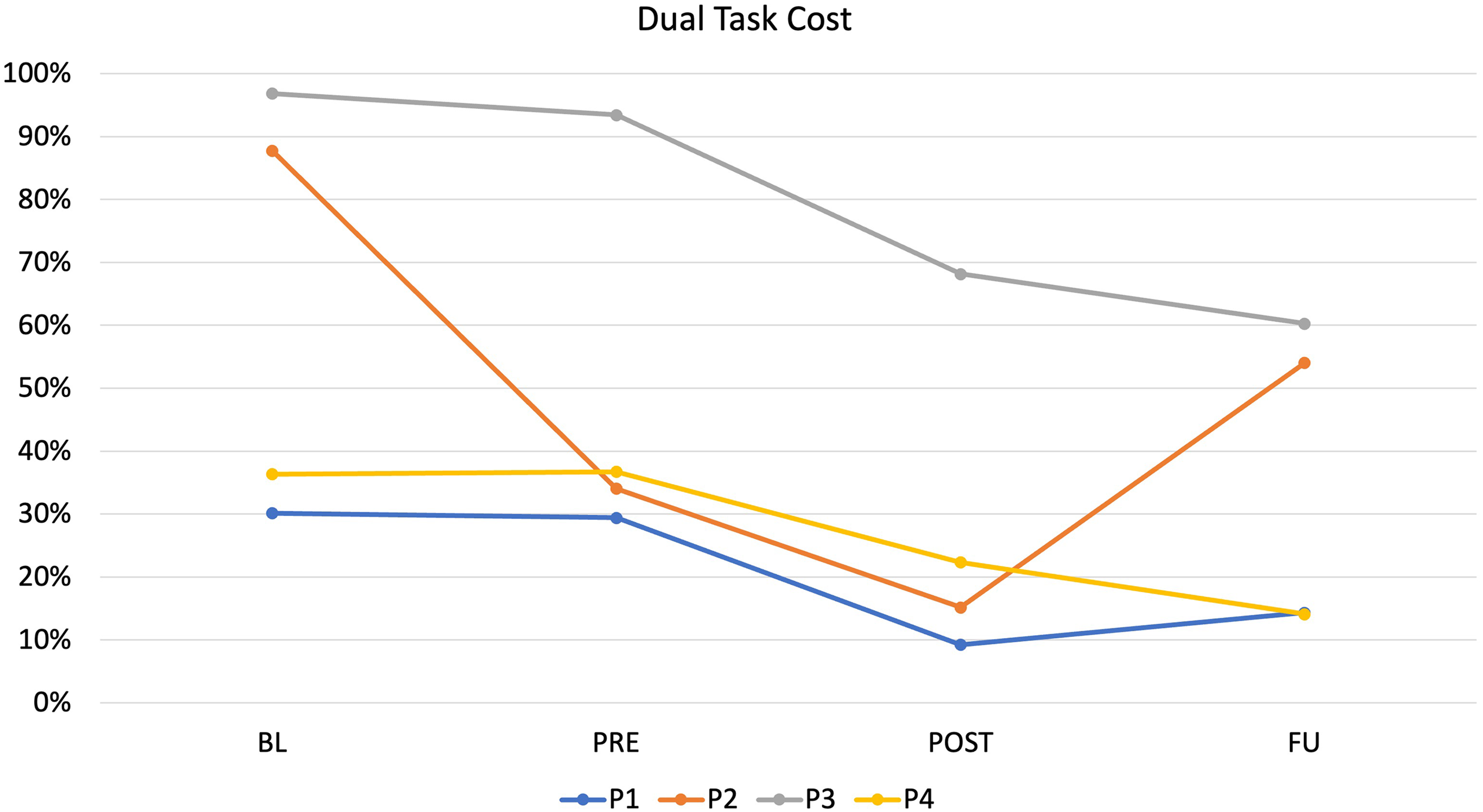
Change in Dual task cost (DTC) at each time point (Baseline (BL), Pre-intervention (PRE), Post intervention (POST), and Follow-up (FU) for each participant.
Timed Up and Go (TUG) and TUG Combined with a Cognitive Task (TUG.CT) Scores, Percentage Change and Dual Task Cost per Participant and for Each Timepoint (Baseline (BL), Pre-Intervention (PRE), Post Intervention (POST), and Follow up (FU)).
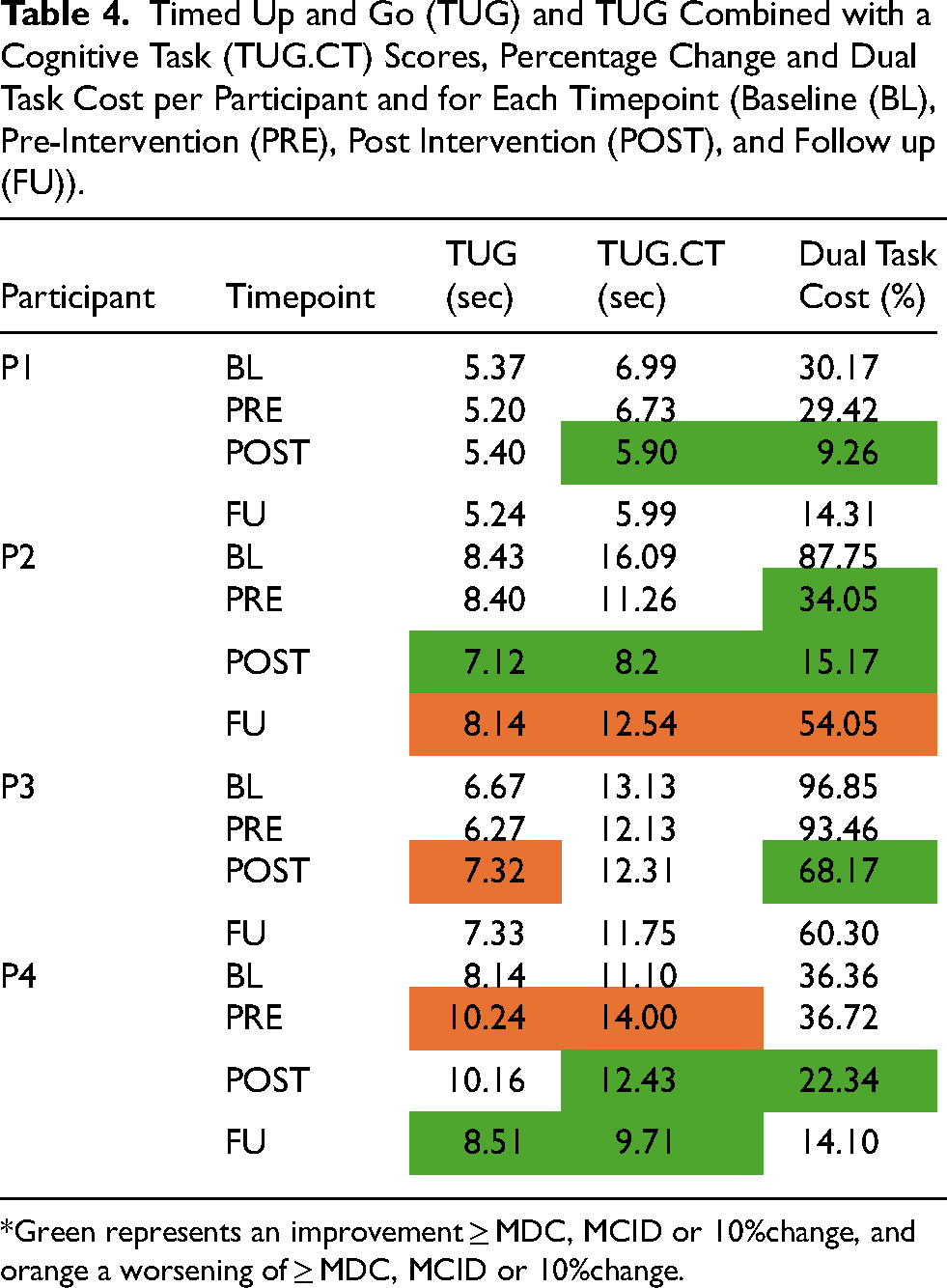
*Green represents an improvement ≥ MDC, MCID or 10%change, and orange a worsening of ≥ MDC, MCID or 10%change.
Participant 1
TUG times showed no change across all timepoints (<MDC and MCID). TUG-COG decreased by 0.83 s from PRE to POST (improvement >10% threshold). This improvement was maintained with a 1.53% change from POST to FU assessments and reflects a 20% reduction (>10% threshold) in DTC between PRE and POST.
Participant 2
Between BL and PRE assessments, there were minimal changes in TUG time for P2 (<MDC and MCID). Between PRE and POST assessments, there was an improvement of −1.28 s (>MCID for TUG). Their TUG-COG times showed a decrease of 2.85 s (>10% threshold) and a 53.70% decrease in DTC between BL and PRE. Following the intervention, P2 had an improvement in TUG-COG time of −3.06 s (> 10% threshold). The DTC was 18.88% less at the POST assessment compared to PRE. At FU there was an increase in TUG-COG time of 4.34 s (> 10% threshold) which represented a 38.88% increase in DTC.
Participant 3
P3 showed a decrease in TUG time from BL to PRE of 0.50 s (> MCID). Between PRE and POST, TUG time increased by 1.05 s (>MCID). Their TUG-COG time reduced by 1 s (>MCID) and the DTC was reduced by 3.39% between the BL and PRE assessments. TUG-COG time increased between the PRE and POST assessments by 0.2 s (<MCID) but DTC reduced by 25.29%. At FU, TUG-COG decreased by 0.56 s (>MCID) and DTC reduced by 7.87% compared to POST.
Participant 4
P4 TUG time changes did not meet the MCID between BL and PRE or PRE and POST assessments. Their FU TUG time reduced by 1.4 s (>MCID) compared to POST. TUG-COG time increased by 2.9 s between BL and PRE assessment (>10% threshold); however, DTC was almost identical between both time points. Following the intervention (POST), there was a decrease in the TUG-COG time of 3.57 s (> 10% threshold). DTC was reduced by 14.37% when comparing the PRE and POST assessment scores. At FU, DTC was 14.10%, which was the lowest of all four assessment time points.
The Kids Mini BESTest
Kids Mini BESTest scores are described in Figure 4 for BL, PRE and POST timepoints. There were no changes of more than one point between the BL and PRE assessments for any of the participants. From PRE to POST assessments, each participant increased their score by 4–5 points.
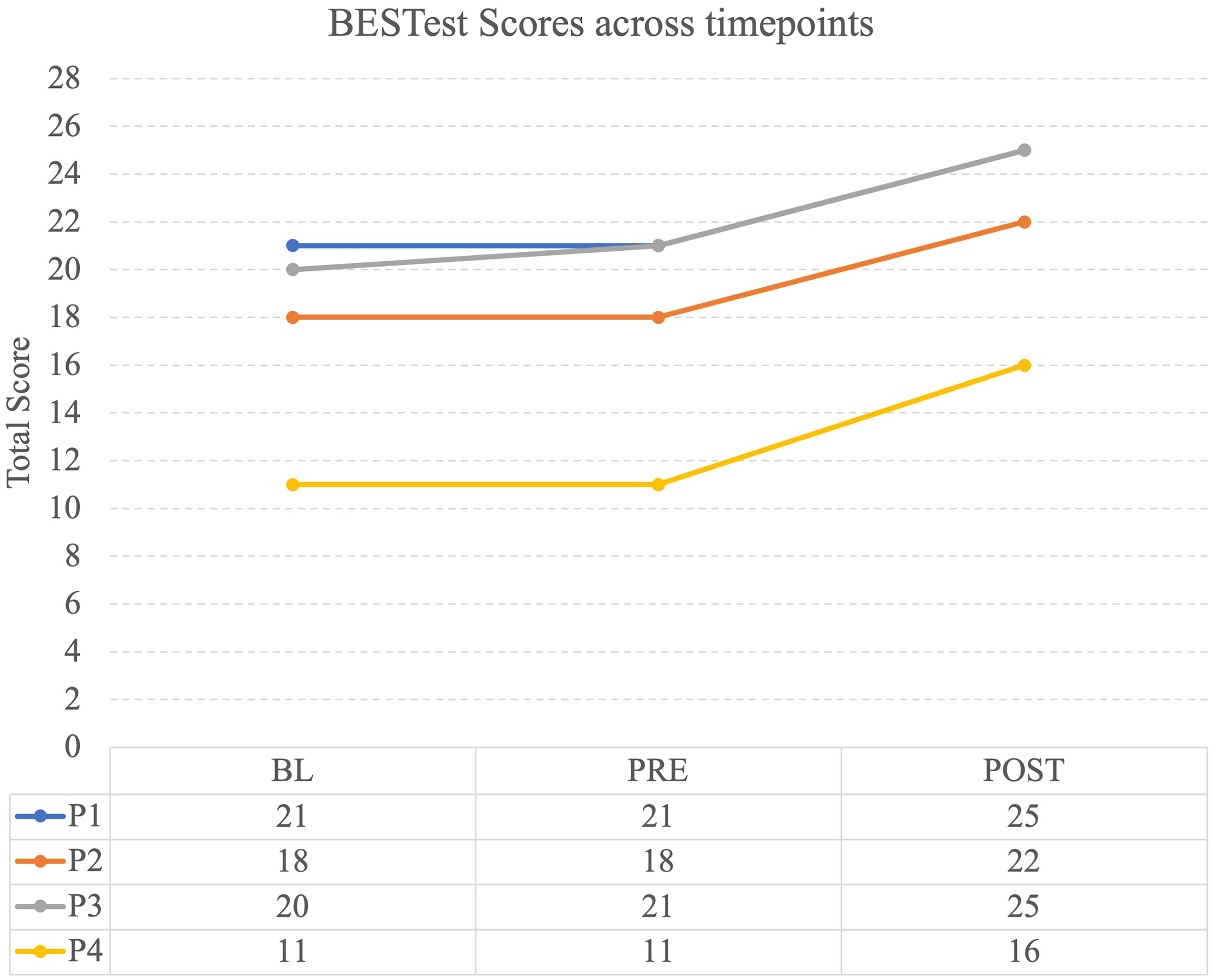
Total scores of the Kids Mini BESTest for each participant at baseline (BL), preintervention (PRE), and postintervention (POST).
Spatiotemporal Parameters
All spatiotemporal parameters were highly variable across time points and participants with and without Loki for both the less affected and more affected limbs. Means and SDs for each spatiotemporal parameter (step length, %timeDS, %timeSw, %timeSt, velocity, and cadence) are available in supplementary material 1. Percentage change for each participant's step length and %timeDS between BL to PRE, PRE to POST, and POST to FU are reported in Table 5, and in Table 6 for walking speed and cadence. Any improvements that are beyond the 10% threshold are highlighted in green and any decline beyond the 10% threshold is highlighted in orange. Percentage change for %timeSt and %timeSw are available in supplementary material 1; there were no changes beyond the 10% threshold at any time point for any participant for %timeSt and %timeSw, except for a decrease in %timeSw for P3 of 13.10% when walking with Loki at FU compared to POST.
Percentage Change (%change) for Step Length and Percentage Time Double Support (%timeDS) Between Baseline (BL) and Preintervention (PRE) Assessments, PRE and Postintervention (POST) Assessments and Between POST and Follow Up (FU) Assessments When Walking with the Dog (WD) and Without the Dog (ND) for Each Limb (More Affected (MA) and Less Affected (LA)).
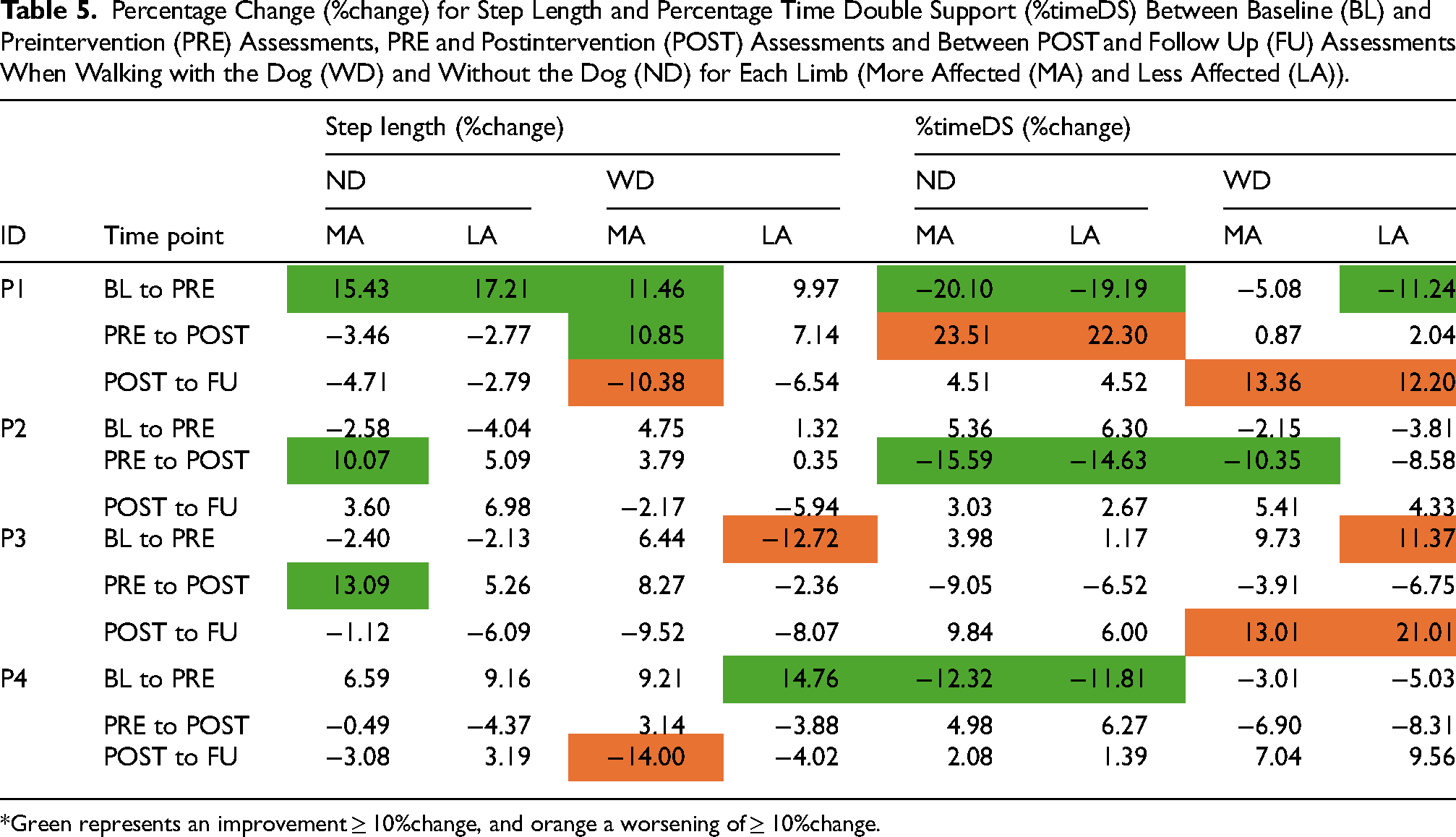
*Green represents an improvement ≥ 10%change, and orange a worsening of ≥ 10%change.
Minimal Clinically Important Difference (MCID) Between Baseline (BL) and Preintervention (PRE) Assessments, PRE and Postintervention (POST) Assessments and Between POST and Follow Up (FU) Assessments for Walking Speed and Cadence.
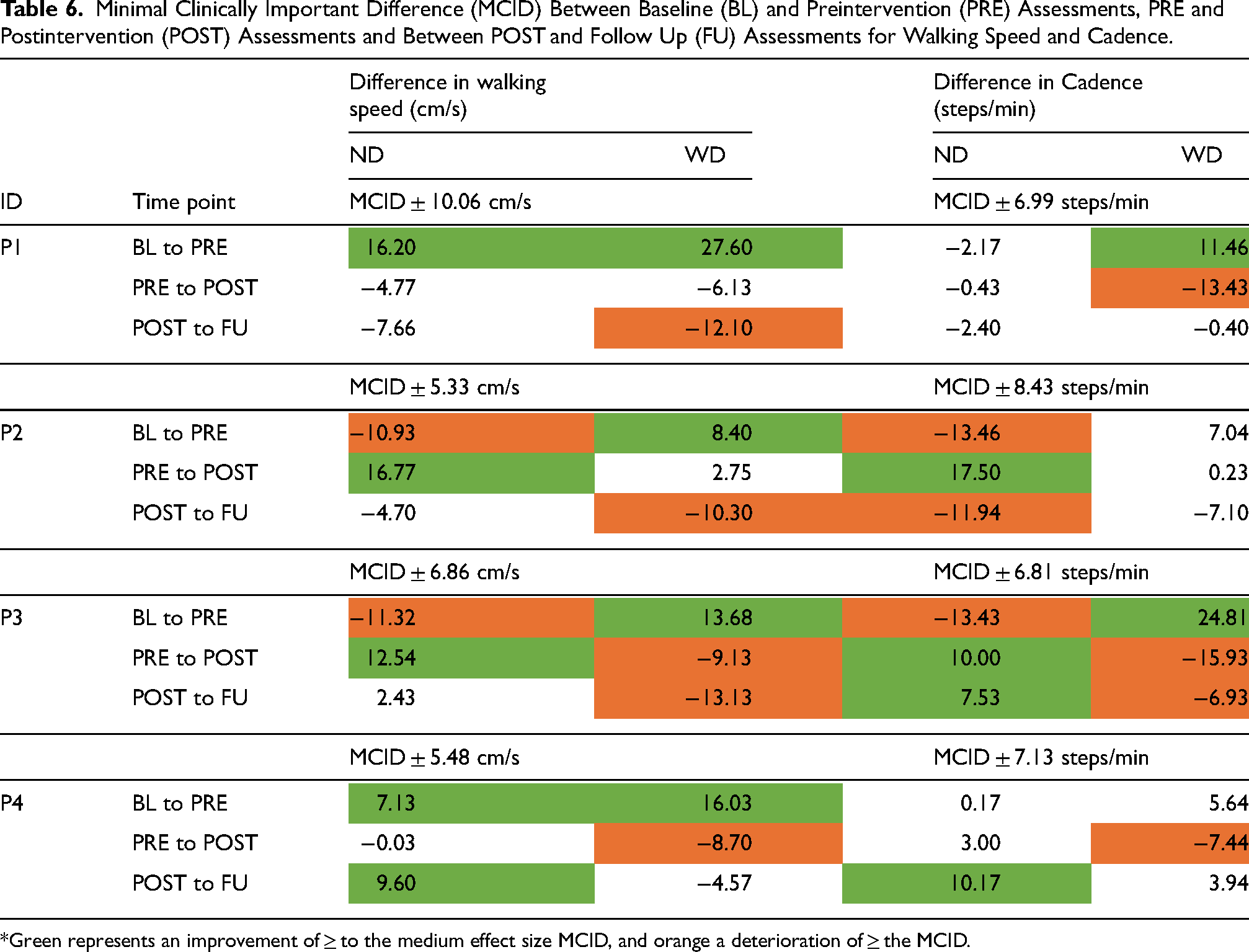
*Green represents an improvement of ≥ to the medium effect size MCID, and orange a deterioration of ≥ the MCID.
Participant 1
Step length improved (MA side only) when walking with Loki from BL to PRE, PRE to POST, and POST-FU. Step length also improved from BL to PRE when walking without Loki. Relative time spent in DS improved from BL to PRE walking with (MA side only) and without Loki, worsened when walking without Loki PRE to POST, and worsened when walking with Loki between POST to FU. Walking speed improved BL to PRE with and without Loki, and worsened walking with Loki from POST to FU. Cadence improved walking without Loki from BL to PRE and worsened walking with Loki PRE to POST.
Participant 2
For Participant 2, step length improved (MA side only) between PRE and POST when walking without Loki. There were improvements in %timeDS from BL to PRE when walking with (MA side only) and without Loki, and again from PRE to POST when walking with Loki (MA side only). For Participant 2, walking speed improved when walking with Loki and worsened without Loki between BL and PRE, improved without Loki between PRE and POST, and worsened with Loki between POST and FU. Cadence worsened when walking without Loki between BL and PRE, PRE and POST, and POST and FU.
Participant 3
Step length improved (MA side only) for Participant 3 when walking without Loki between PRE and POST. The relative time spent in DS worsened between BL and PRE (LA side only) and POST to FU. Between BL and PRE, walking speed worsened without Loki and improved with Loki while the reverse change was seen PRE to POST: walking speed improved without Loki and worsened with Loki. From POST to FU, walking speed worsened when walking with Loki. Cadence improved when walking with Loki and worsened when walking without Loki between BL and PRE, with opposite changes (worsening with Loki and improving with Loki) between PRE and POST, and POST and FU.
Participant 4
For Participant 4, step length worsened (MA side only) when walking with Loki between BL and PRE. There was an improvement in %timeDS between BL and PRE when walking without Loki. Walking speed improved walking with and without Loki between BL and PRE, worsened walking with Loki between PRE and POST, and improved walking without Loki between POST and FU. Finally, cadence worsened between PRE and POST when walking with Loki and improved between POST and FU when walking without Loki.
Walking Speed and Cadence
Means and SD for each participant at each timepoint for walking speed and cadence are available in Supplementary Material 1. At BL, PRE and POST assessments, all participants walked more quickly with Loki than without. At BL and PRE assessment, cadence increased for all participants when walking with Loki. P1 had an increase (>MCID) in speed both when walking with Loki and without and cadence when walking with Loki at the PRE assessment (Table 5). At POST, their cadence decreased (>MCID) when walking with Loki. At FU, there was a decrease in walking speed (>MCID) when walking with Loki. As is described in Table 5, P2 and P3 both had an increase in speed with Loki (>MCID) at the PRE assessment compared to BL. At the POST assessment, when walking without Loki, P2 and P3 both had improvements in their walking speed and cadence that greatly surpassed the MCID compared to the PRE assessment; this was maintained at FU. When walking without Loki, P3 had a decrease in speed and cadence (>MCID) at POST and FU assessments. P4 had an increase in speed (>MCID) both with and without Loki at PRE assessment compared to the BL; the speed increase was more than double when walking with Loki compared to walking without (Table 5). Following the intervention, P4 had a decrease in speed and cadence (>MCID) when walking with Loki.
Visual Analog Scales
VAS scores are visually represented for each participant are available in Supplementary Material 2. P1 marked the extreme end of each VAS scale (i.e., 100%) for each statement at each time point; there were no changes in any of their VAS scores throughout the 24 weeks. P2 reported a significant improvement in comfort, safety and, enjoyment when walking with Loki compared to ND at each assessment time point. At POST, P2 had an improvement of 61% in perceived confidence to maintain their balance while walking without Loki and an improvement of 39% in perceived walking safety without Loki. P3 reported a decrease of 35% in perceived confidence in balance ability while walking without Loki at the POST assessment but an increase of 41% when walking with Loki. P4 had an increase of 76% in perceived safety between the BL and PRE assessments and an increase of 11% between POST and FU when walking without Loki. Following the intervention, perceived enjoyment of walking increased by 11%.
Discussion
This is the first study to assess the impacts of integrating a rehabilitation dog for walking and balance training in children with CP. Each child had an improvement in their postural control and in DTC following the intervention. Changes in spatiotemporal parameters of walking were highly variable across participants with no consistent pattern identified. Dog-assisted therapies have been shown to improve psychological and emotional health through decreased stress, anxiety, and fear in health settings (Elmacı & Cevizci, 2015; Muñoz Lasa et al., 2015; Yap et al., 2017). Our study similarly showed an increase in comfort and confidence when walking with vs. without the dog.
In our study, all participants had an improvement in their TUG-COG scores and in DTC following the intervention with Loki. To walk with Loki, one must use tactile and verbal cues for speed and direction while also attending to the environment and their own physical abilities both in static and dynamic movements. Working with Loki required both manual and cognitive efforts and provided opportunities to train postural control and walking with increased cognitive load (dual task). Increased DTC has been shown to reduce walking performance and postural control ability through decreased walking speed and decreased stability in walking (Palluel et al., 2019; Roostaei et al., 2021). This decreased walking ability directly impacts overall function of children with CP in their community environments and decreases their participation in age-appropriate activities (Palluel et al., 2019; Roostaei et al., 2021). By improving DTC through training in salient environments, with appropriate progression of complex dual tasking, we may improve motor integration and attentional capacity (Bianchini et al., 2022). Improved dual-tasking may lead to improvement in walking function and participation in peer-group activities as there is less attentional demand for the control of walking and more ability to respond and attend to the environment (Shumway-Cook et al., 2022).
Each participant increased their Kids Mini BESTest score beyond the MCID from PRE to POST and showed improvement across each domain of postural control as measured by this test. Deficits in postural control for children with CP are well documented and considered a multifactorial process that includes the ability to orient the body in space and to maintain equilibrium within that orientation (Dewar, Claus, Tucker & Johnston, 2017; Horak, 2006; Novak, 2014; Novak et al., 2020; Shumway-Cook et al., 2022; Woollacott & Shumway-Cook, 2005). Improvement of postural control seen in this study may be attributed to the use of the SFPC (Horak, 2006) across each part of the intervention. By integrating Loki into the intervention, cognitive processing and reactive postural control were challenged more directly. The intervention was individualized at each session and children had an opportunity to practice and reinforce the strategies practiced in the research space into salient environments. Loki responded well to frequent and continuous verbal and tactile cueing from the child, which demanded significant attentional focus and decision-making related to the surrounding environment (e.g., navigating a crowd). Both the child and Loki needed to have capacity to be responsive to one another while navigating complex environments. The harness itself was not perfectly rigid or stable on Loki and this inherent rotational movement could have created a sense of instability as the child walked. Loki also had an ability to react or choose to move unexpectedly requiring a subsequent appropriate reaction from the child, further challenging their anticipatory and reactive postural control. The improvement seen in our study on the Kids Mini BESTest ranged from 4–5 points. This is comparable to research by Jha et al. (2021) that compared a 6-week PT intervention for balance combined with virtual reality gaming vs. PT intervention only. Both groups showed a significant improvement with a mean change on the Kids Mini BESTest of 8.7 points for intervention and 5.8 points for control group (Jha et al., 2021).
Following the intervention, all participants had changes to their spatiotemporal walking parameters. Although these changes were not consistent across participants, there were some important differences observed. All participants demonstrated changes in their spatiotemporal parameters between BL and PRE; this captures the variability typically seen in this population and may allow for better understanding of changes following the intervention (Brændvik et al., 2019; Brégou Bourgeois et al., 2014). All four participants spent more time in double support than what is considered typical prior to the intervention (Jacqueline Perry, 2010). Increased time spent in double support in children with CP is described as a strategy to improve stability while walking (Abel & Damiano, 1996; Carcreff et al., 2020; Davids et al., 2019). Following the intervention, the percentage time spent in double support decreased and step length increased for 3 of the 4 participants (P2, P3 and P4), both when walking with and without Loki. Decreased time spent in double support is also connected with improved walking speed which was also observed in these three participants (Carcreff et al., 2020; Davids et al., 2019; Moreau et al., 2016). This adjustment may indicate improved dynamic postural control as the participant is better able to control periods of time spent in single leg support which may in turn improve advancement through more time spent in the swing phase (Abel & Damiano, 1996).
Walking speeds and cadences increased for all participants when walking with Loki post-intervention. At baseline (BL) without the dog, all walked slower than the range reported for typically developing
Similar to the Rondeau et al. study (Rondeau et al., 2010) working with a rehabilitation dog with adults post-stroke, an improvement in walking speed was observed in our study, where children's speed increased when walking with Loki but also following the intervention when walking without Loki. It is suggested that a rehabilitation dog assists in navigating complex environments and is easily integrated into any setting safely (Darekar A et al., 2008; Rondeau, 2008; Rondeau et al., 2010). Rondeau et al. (2010) suggest that the use of walking training with a rehabilitation dog highlights the utility of the task-oriented approach in walking retraining and that a rehabilitation dog is easier to use than a typical gait aid due to its ability to walk independently of the person.
All participants reported increased or high levels of self-perceived enjoyment and safety while walking, confidence in balance ability and comfort when walking with the dog compared to walking without. Children practiced components of walking training in a variety of indoor and outdoor settings with Loki, while the PT observed and provided verbal cueing as needed. Practicing walking training in community can be limited if safety is a concern from the perspective of the treating PT or the child themselves. Providing external support in the form of Loki, that the child could manage independently, increased self-perceived confidence, safety, comfort, and enjoyment, and may have led to the improved walking ability in these community settings. Providing opportunities to explore their environment safely with chances for variability or error in meaningful ways may have provided increased confidence in walking abilities which then translate to day-to-day life. It has been previously reported that dynamic balance ability is perceived as a primary limitation of walking ability by children with CP and their caregivers. (Nelson & Boyer, 2021) Our study shows that the addition of a rehabilitation dog to walking training improves perceived confidence in balance ability which could directly improve walking function. This improved sense of confidence, safety and comfort may motivate patients to engage in walking activities more. As previously mentioned, to improve walking ability and function, a task-oriented or goal-oriented approach that centers on high intensity and high frequency has been shown to be useful in walking training (Maier et al., 2019; Peri et al., 2017; Salem & Godwin, 2009). The improvement in participant perceived comfort, safety, confidence, and enjoyment when walking with Loki also translated to walking without the dog following the intervention, particularly for perceived safety. This finding suggests that the AA-PT encouraged participants to try new skills in and out of session (i.e., in community) due to these perceived benefits which supports improved translation of intervention-based to community-based gains.
Limitations
This case series was a first study to explore an AA-PT and generalizability of our findings may be limited across all children with CP. Future research is warranted and needed to better understand who might benefit most from integrating a rehabilitation dog into balance and walking training. Also, the use of the Kids Mini BESTest limits applicability of results to children who can complete standing and walking tasks as assessed by this measure. Further investigation of integration of a rehabilitation dog with children who are non-ambulatory and into typical PT settings would be valuable in evaluating the effectiveness of AA-PT. Rehabilitation dogs, and service animals in general, are living beings that are collaborating in the work and interventions being carried out. Loki had his own needs – although infrequent, Loki required breaks due to heat or fatigue and could be distracted by sudden changes in the environment. Loki also demonstrated behaviors such as slowing his walking pace, looking back to the handler and leaning towards the participant when he needed a rest break. This poses challenges in ensuring consistency and evaluation across timepoints for factors such as engagement, walking speed, motivation, and wellbeing of both the dog and participant. Service dogs like Loki are also trained to be highly attuned to the emotional responses and physical changes of the people they work with; it is entirely possible that Loki demonstrated his own need for rest breaks when he sensed that the individuals he was working with also needed a rest. It is possible that these experiences of responding to Loki and supporting his own needs mimic a more realistic lived experience for the child also. AA-PT interventions require flexibility and responsiveness not just to the children, but to the dog as well. Practical considerations—such as participant allergies, occasional distraction, or the need for a familiar handler—also shaped how and where sessions could occur. Ultimately, ensuring Loki's well-being and autonomy remained central, which sometimes meant adapting our plans in real time. Organizations and individuals that can train service dogs like Loki are limited; accessing specialized service dogs can be extremely challenging for both individuals and health care providers. Feasibility indicators such as cost, handler training, care and support for the dog, as well as operational supports for implementing this type of AA-PT should be evaluated. Future work on preparing service dogs for rehabilitation and the ongoing demands of working with children with a physical disability, and factors to ensure the dog's welfare and ongoing readiness for work will be an essential component of integrating rehabilitation dogs into PT interventions. Evaluating the experiences and willingness of health care providers to collaborate in this type of intervention would lend a broader understanding of how to best implement this type of intervention in current health care settings. Finally, broader qualitative exploration of the psychosocial impacts for children and their families of this type of AA-PT is merited and would deepen and expand understanding.
Conclusion
This is the first study to evaluate integrating a rehabilitation dog into walking and postural control training in children living with CP and offers promising initial insights into this type of AA-PT intervention. Following an 8-week individualized AA-PT with a rehabilitation dog, children with CP improved their postural control and dual-tasking ability. Ongoing evaluation of AA-PT is merited to broaden applicability in pediatrics and other rehabilitation settings.
Implications for Rehabilitation
First study to evaluate the integration of a rehabilitation dog into walking and balance training for children living with CP. Integrating a rehabilitation dog into walking and balance training for children with CP increases the cognitive and dual task demands of postural control training Training with a rehabilitation dog only once per week for 8 weeks improved postural control and walking confidence.
Supplemental Material
sj-docx-1-nre-10.1177_10538135251353467 - Supplemental material for An Animal-Assisted Physiotherapy Intervention with a Rehabilitation Dog for Walking and Balance Training: A Case Series of Children Living with Cerebral Palsy
Supplemental material, sj-docx-1-nre-10.1177_10538135251353467 for An Animal-Assisted Physiotherapy Intervention with a Rehabilitation Dog for Walking and Balance Training: A Case Series of Children Living with Cerebral Palsy by Valerie Caron, Alison Oates, Romany Pinto, Joel L Lanovaz, Colleen A Dell, Sarah Oosman and Sarah J Donkers in NeuroRehabilitation
Supplemental Material
sj-docx-2-nre-10.1177_10538135251353467 - Supplemental material for An Animal-Assisted Physiotherapy Intervention with a Rehabilitation Dog for Walking and Balance Training: A Case Series of Children Living with Cerebral Palsy
Supplemental material, sj-docx-2-nre-10.1177_10538135251353467 for An Animal-Assisted Physiotherapy Intervention with a Rehabilitation Dog for Walking and Balance Training: A Case Series of Children Living with Cerebral Palsy by Valerie Caron, Alison Oates, Romany Pinto, Joel L Lanovaz, Colleen A Dell, Sarah Oosman and Sarah J Donkers in NeuroRehabilitation
Footnotes
Acknowledgements
This research was conducted on Treaty 6 and Treaty 4 Territories and the Homeland of the Métis. We acknowledge and thank the First Peoples of this land and reaffirm our commitment to respectful relationships with one another. We would like to thank the children and their families who committed to and invested their time in this project. We are grateful to the Fondation Mira (Montréal, QC) for training Loki and supporting our research team throughout the study. Thank you to Jodi Walkner and Erin McCormick for their support in recruitment for this case series. We would also like to acknowledge Dr. Elizabeth Condliffe and Dr. Gary Linassi for their input on this work.
Thank you to all the members of our extended team for their immense contributions, particularly Loki, who always put his whole heart and self into bringing joy to everyone he met.
Ethical Considerations
This study was approved by the University of Saskatchewan's Human Biomedical Research Ethics Board (REB-Bio#1091) and the Animal Research Ethics Boards (AUP# 20190049).
Consent to Participate
Each participant and their family and/or guardian reviewed and provided informed consent for the research assessments and PT intervention.
Consent for Publication
Each participant and their family and/or guardian consented to images/media being captured during the data collection process and intervention and for these images to be shared in published materials.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was provided by a Saskatchewan Health Research Foundation Collaborative Innovation Development Grant; the Branch Out Neurological Foundation Graduate Scholarship; the Saskatchewan Center for Patient Oriented Research PhD Scholarship; and the College of Medicine, Health Sciences Program at the University of Saskatchewan.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on reasonable request from the corresponding author, VC. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.