
Abstract
Background
The atypical upper limb (UL) flexion pattern in children with unilateral cerebral palsy (UCP) debilitates their ability to experience natural weight bearing through arms and hands, leading to restricted mobility and reduced hand functions. The recommended therapeutic strategies to improve hand functions are not standardized, i.e., (varied protocols, treatment schedules, and frequency), though the benefits of UL weight-bearing on hand-opening and prehension skills are well-documented.
Objective
To study the efficacy of Static weight bearing (SWB) in Prone on UL with active elbow extension versus modified-constrained induced movement therapy (m-CIMT) on hand functions in children with UCP.
Methods
Randomized clinical trial. Subjects (N = 38) were randomized equally (group- 1, SWB, n = 19; and group- 2, m-CIMT, n = 19). Outcome measure- Fine Motor of PDMS-2 (FM_PDMS-2) pre-and post-interventions after 2 weeks.
Results
The percentage change (post-intervention) for the Grasping and VMI subtests in the SWB group were 37.67% and 14.11%, while for the m-CIMT group were 12.78% and 4.88%, respectively. These changes were highly significant (p 0.000).
Conclusion
Both groups, i.e., SWB and m-CIMT, showed significant differences in the percentage change post-intervention. However, the SWB group demonstrated augmented changes over the m-CIMT on both subtests of FM_PDMS-2, hence greater improvement in hand functions following SWB exercises.
Keywords
Introduction
In healthy-term infants, corticospinal fibers from each hemisphere project to each side of the spinal cord to a predominantly crossed projection in the first 2 years of life (Eyre et al., 2001). Following the initial insult (unilateral perinatal stroke), progressive maladaptive changes occur within the central nervous system (CNS) due to activity-dependent plasticity (Eyre, 2003). The corticospinal projections (from the involved hemisphere) are gradually displaced over time by uncrossed projections from the undamaged hemisphere, causing poor functional outcomes (Eyre et al., 2007).
The development of spinal cord segmental circuitry is also influenced by corticospinal tract activity. If this is disrupted during early development, the patterns of spinal cord circuitry and interneuron development become abnormal and immature, affecting M1 motor cortical mapping (Chakrabarty et al., 2009). However, therapeutic processes, i.e., early restraint of the unaffected limb along with motor training, may reverse, to some extent, the changes in spinal cord circuitry, corticospinal tract projections, and M1 motor map abnormalities, hence the improved motor outcome (Friel et al., 2012).
This consideration, in light of the International Classification of Functioning, Disability, and Health (ICF) framework, makes it possible to alter structure and function either positively or negatively through modulation of activity (Basu et al., 2015). The parents of children with unilateral cerebral palsy (UCP) identified self-care as a priority for intervention (Burgess et al., 2019). The ICF framework also aids in exploring the hand functions of children with UCP through an understanding of the inter-relationship between body structure and function, activities, and participation, thereby guiding the prevention of the diabolical cycle of deteriorating structure and function. (Basu et al., 2015).
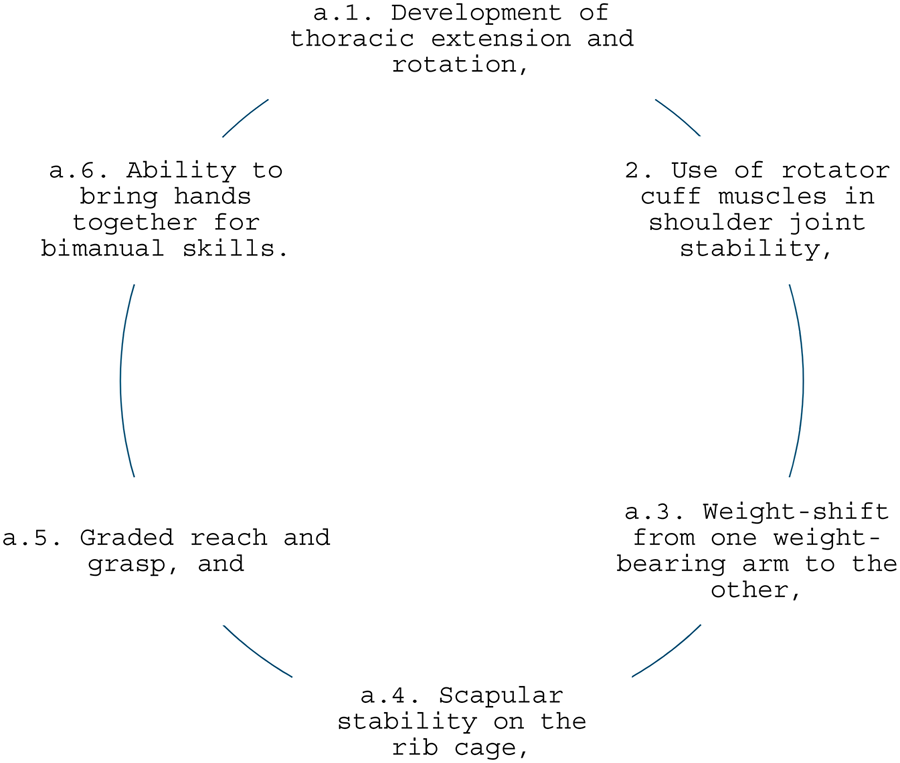
Weight-bearing and manipulative abilities are two basic functions of the upper limb (UL). The key to developing these two functions lies in the movement components of the shoulder girdle and glenohumeral joint, which is allied with the central control of flexion and extension against gravity (Irwin-Carruthers, 1982). Initially, movements of the scapula and glenohumeral joint are associated; hence, the child cannot move independently from one another to break up movement synergies. As control of the other components is established, the ability to dissociate movements of the scapula and humerus develops (Irwin-Carruthers, 1982).
Progression of UL Weight-Bearing in Typically Developing Children
The control required for weight-bearing in a typically developing baby starts at three months when the extension control moment spreads throughout the thoracic area. The thoracic extension aids in stabilizing the shoulder with scapulae in adduction (in prone on elbows) while the humerus abducts and internally rotates. At this moment, the weight is taken over by the anterior aspect of the forearm while the hand is closed. As the baby starts to push up to the extended arm, the scapula stabilizes in more adduction (Casaer, 1977; Irwin-Carruthers, 1982). Once adequate balance develops between extensor and flexor control, the child shifts weight in preparation for reaching.
In the beginning, the child attempts to stabilize the shoulder with adduction of the scapula on the weight-bearing side; until they learn to compensate with lateral flexion of the trunk on that side, the child falls to the non-weight-bearing side, which is a perfectly normal pattern (seen during early attempts to reach). However, the child cannot move their body freely over the supporting limb until they learn to stabilize the scapula adequately in abduction. With the development of this control, the child now can extend the trunk on the weight-bearing side and, as they rotate the trunk on the supporting arm, the humerus progressively becomes more abducted and externally rotated, the rotation of the forearm becomes neutral, and weight is taken along the ulnar border of the forearm and hand, allowing exploratory raking with the fingers. At this stage, this apparent dissociation is due to fixation of the distal segment rather than active isolation of movement components (Irwin-Carruthers, 1982).
The initial attempts to support the shoulder on extended elbows achieve only partial extension in the upper trunk, provided that the shoulder remains in abduction and internal rotation. The full extension is possible only when the humerus is stabilized in adduction and external rotation (dependent on the scapula being stabilized in abduction). With the increase in humeral adduction (the base of support comes in line with shoulders), the point of weight bearing on the hands moves from the ulnar side towards the base of the thenar eminence across the entire width of the palm (generating stretch on the wrist and finger flexors), and the fingers begins to extend. This causes weight transfer on an open hand with the abducted thumb (an essential component for developing the radial tripod in manipulation (Casaer, 1977; Irwin-Carruthers, 1982).
Progression of UL Dysfunctions in Children with UCP
The asymmetrical use of UL is typical in children with UCP, which may be identified from 3 months onwards (Stamer, 2000). The increased muscle contractions of the involved UL precipitate increased shoulder complex elevation with shoulder extension and internal rotation, elbow flexion, and forearm pronation with fisting of the hand. This posture of the involved UL induces lateral flexion of the spine with concavity on the involved side, elevated scapula, and substantial holding by erector spinae and latissimus dorsi. It causes the involved side of the body to do little or no weight-bearing through the UL (which is often held away from the surface) (Saussez et al., 2017).
Movement control development is also affected in non-involved UL due to deficient (Gordon et al., 2013; Saussez et al., 2017; Stamer, 2000).
Nearly all children with UCP avoid all-fours position because it requires some amount of movement control, ROM, and sensory awareness from the involved arm, hence, the unilateral use of non-involved arms in reaching and manipulation. These changes make a child with UCP extremely resistant to learning any function with the involved arm because,
non-involved arm works well enough to do many functions; hence, the child sees no reason to learn to use the involved arm, involved arm often develops impaired sensation; therefore, learning motor skills is difficult even if the child is involved mildly, and, the involved arm in a child with UCP often shows extreme sensitivity to tactile sensation (to discriminate and to protect). Even though children cannot use many sensory systems (e.g., tactile, pressure, loading, etc.) good enough to discriminate, causing them to develop extreme sensitivity in the form of protection (tactile inputs being perceived as a threat), leading them to keep the involved arm in a pull-away state, i.e., flexion posture. Hence, the involved arm is not used (Bobath & Bobath, 1984).
The excessive flexor posture affects the development of UL support, protective reactions, and ability to reach, hence, diminished hand-opening (Bobath & Bobath, 1984). Because of significant asymmetry in neuromuscular control and sensory perception, children with UCP develop abnormal perceptions of body schema, causing a shift in the sense of midline towards the non-involved side (Stamer, 2000). Altogether, these changes make the handling of children with UCP very difficult during therapy (Stamer, 2000). Thereby contributing to the deficits in UL manual dexterity, i.e., impaired skilled hand movements and precision grip abilities, hence, long-term functional impairments in hand functions during activities of daily living (Saussez et al., 2017).
Therapy Strategies Used for the Children with UCP
Treating children with UCP is often arduous because they can do several functional skills by themselves and see no reason to be interfered with. However, the impairment and disabilities in the involved arm need to be addressed intensely (Stamer, 2000). Many therapy strategies are developed to improve hand functions in children with UCP involving the repeated practice of pertinent movements, i.e., play-based, problem-solving, or goal-centered (Mastos et al., 2007) in sync with the activities of daily living, with the child as an active participant. Many of these strategies showed varying evidence of benefit (Sakzewski et al., 2014). Therapeutically, the child must be aligned to overcome the shortening on the involved side and out of rotation towards the non-involved side before beginning any UL movements. This requires weight-bearing on the arms towards the involved side by extending and rotating the thoracic spine in a prone or forward-inclined posture (Stamer, 2000). Therefore, early therapy in the prone weight-bearing position is vital to prevent contractures and functional deficits in UL.
In a study, the authors demonstrated that UL weight-bearing influenced hand-opening and prehension components in 2–7-year-old children with CP with flexor hypertonicity. They attributed these changes to the combined effect of weight-bearing and active movements and advised further studies on treatment concepts that aim to increase movement components of reach, grasp, and release in children with CP (Chakerian & Larson, 1993). In another research, recommendations were made to develop a clinical rationale for the static weight bearing (SWB) exercises through the UEs in clinical practices for children with CP because of its benefits in improving bone mineral density to reduce the susceptibility of fractures, and advocated to examine its other potential benefits in prehension skills using rigorous methodological quality over a larger sample size, in terms of functional limitations/activity and participation level (Pin, 2007).
In addition to weight-bearing, many other therapy techniques, i.e., Constraint-induced movement therapy (CIMT), neurodevelopmental therapy, and hand-arm bimanual Intensive Therapy (HABIT), are practiced in children with CP to improve UL impairments (Jayaraman & Puckree, 2010). Constraint-induced movement therapy (CIMT) is a therapy approach that restrains the non-involved arm to encourage using the involved arm. The modified CIMT (m-CIMT) is a child-friendly therapy that improves hand functions in UCP (Eliasson & Holmefur, 2015). The m-CIMT therapy includes intensive short-duration/long-duration repetitive unimanual task practice by the involved hand while constraining the non-involved hand (Sakzewski et al., 2014).
Benefits of Prone Weight-Bearing on UL
The failure to develop weight-bearing after an injury or disease interferes with the later development of manipulative abilities (Irwin-Carruthers, 1982). Processes like an early restraint of the involved limb through weight-bearing and motor training may improve the motor outcome by altering the structure and function positively or negatively through the modulation of activity (Basu et al., 2015).
The importance of weight-bearing in improving UL and hand functions/control is elaborated extensively (Chakerian & Larson, 1993; Smelt, 1989). The hypertonicity was observed to be inhibited during weight-bearing (Boehme, 1988). As a treatment principle, weight-bearing is conventionally practiced as a prerequisite before a functional activity, assuming it helps regulate muscle tone, thereby contributing to the normal development of the skilled movements of the UL and hand during sitting and standing (Brouwer & Ambury, 1994; Pearson & Williams, 1972).Though most children with CP cannot progress through all the stages of normal child development, a carefully planned treatment can help to counteract the abnormal posture and movement patterns (Bobath & Bobath, 1984).
As an outcome measure, the Quality of Upper Extremity Skills Test (QUEST) examines the quality of UE function in four domains: dissociated movement, grasp, protective extension, and weight bearing (Hoare et al., 2011). The weight-bearing domain of QUEST includes a) the weight-bearing ability to bear weight on arms in prone/4-point kneeling and b) the ability to bear weight on a fully extended right and left arm while reaching with another arm. This domain encapsulates the ICF Body Function/Structure domain (BF), which has ICF codes B7101 and B7603, and under the ICF Activity domain (ACT), which has D4452 as the ICF code (Hoare et al., 2011).
Outcome Measures for UL Evaluation in CP
To evaluate the effect of UL intervention in children with CP, the commonly used outcome measures are (Quality of Upper Extremity Skills Test [QUEST], Melbourne Assessment of Unilateral Upper Limb Function [Melbourne Assessment], and Assisting Hand Assessment [AHA], Bruininks-Oseretsky test of motor proficiency [BOTMP], Bayley scale of Infant Development [BSID], and Peabody Developmental Motor Scale-2 [PDMS-2]) (Krumlinde-Sundholm & Wagner, 2018).
The PDMS-2 is a norm-referenced, standardized test with precise scoring criteria that measures motor abilities from birth to 71 months relative to age-related typical development to identify children with delayed motor development (diagnostic/discriminative characteristic) (Wang et al., 2006). The Fine Motor of PDMS-2 (FM_PDMS-2) includes two subscales, a. grasping and b. visual motor integration (VMI), consisting of both unimanual (preferred hand) and bimanual tasks (i.e., ability to fold a paper, ability to cut a circle or a square) (Elvrum et al., 2016). The combination of the two subscales gives the fine motor composite score. (see Figure 1). The FM_PDMS-2 Test-Retest reliability (r = 0.84–0.89) and Inter-rater reliability (r = 0.94–0.99) are excellent (Van et al., 2005).

Fine Motor PDMS- 2 (FM_PDMS-2) Test Kit.
Research Question/need of the Study
Various techniques have been used to improve hand functions in children with CP. However, each one was found to have limitations, and interventions were not standardized across studies, i.e., (varied in protocol, treatment schedule, and frequency of intervention). Researchers reported the benefits of UL weight-bearing on hand-opening and prehension components and advised further studies to consider movement components of reach, grasp, and release in children with CP (Chakerian & Larson, 1993) using rigorous methodological quality (Pin, 2007). Hence, this study aimed to evaluate the efficacy of SWB in Prone on UL with active elbow extension versus m-CIMT on hand functions in children with UCP.
Methods
Study Design
This was a randomized clinical trial, and ethical approval was obtained from the Institutional Ethics Committee (IEC/KMC/MLR 11-17/224). The study followed the guidelines of the Declaration of Helsinki on the conduct of human research. The study was registered with the Clinical Trial Registry- India (CTRI), which has reference number CTRI/2018/01/011278.
Participants
A convenient sample of 38 children with UCP was recruited from the Neuro-sensory developmental unit of a tertiary hospital and was examined per the inclusion criteria (a. subjects diagnosed with UCP, b. age ranged from 2 to 5 years, and c. having Manual Ability Classification System (MACS) Level IV and V for hand functions in the involved UL) (Burgess et al., 2019). The subjects were excluded if they had h/o any medications such as barbiturates or anti-spastic drugs, received botulinum toxin injection in the involved UL within the last six months, had uncontrolled epilepsy, contractures, or fixed flexion deformity of elbow or shoulder, had visual problems or any surgical intervention of hand, using any types of UL orthosis, and children with Erb's palsy or brachial plexus injury.
Randomization
The eligible subjects’ parents were approached, and the purpose of the study was explained. They were also informed about their right to refuse or withdraw and the confidentiality of any information. Following this, written parent's assent forms were obtained. Subjects were then randomly allocated to either of the study groups, i.e., SWB Exercises (group 1) or m-CIMT (group 2), through block randomization using a concealed opaque envelope (see Figure 2).
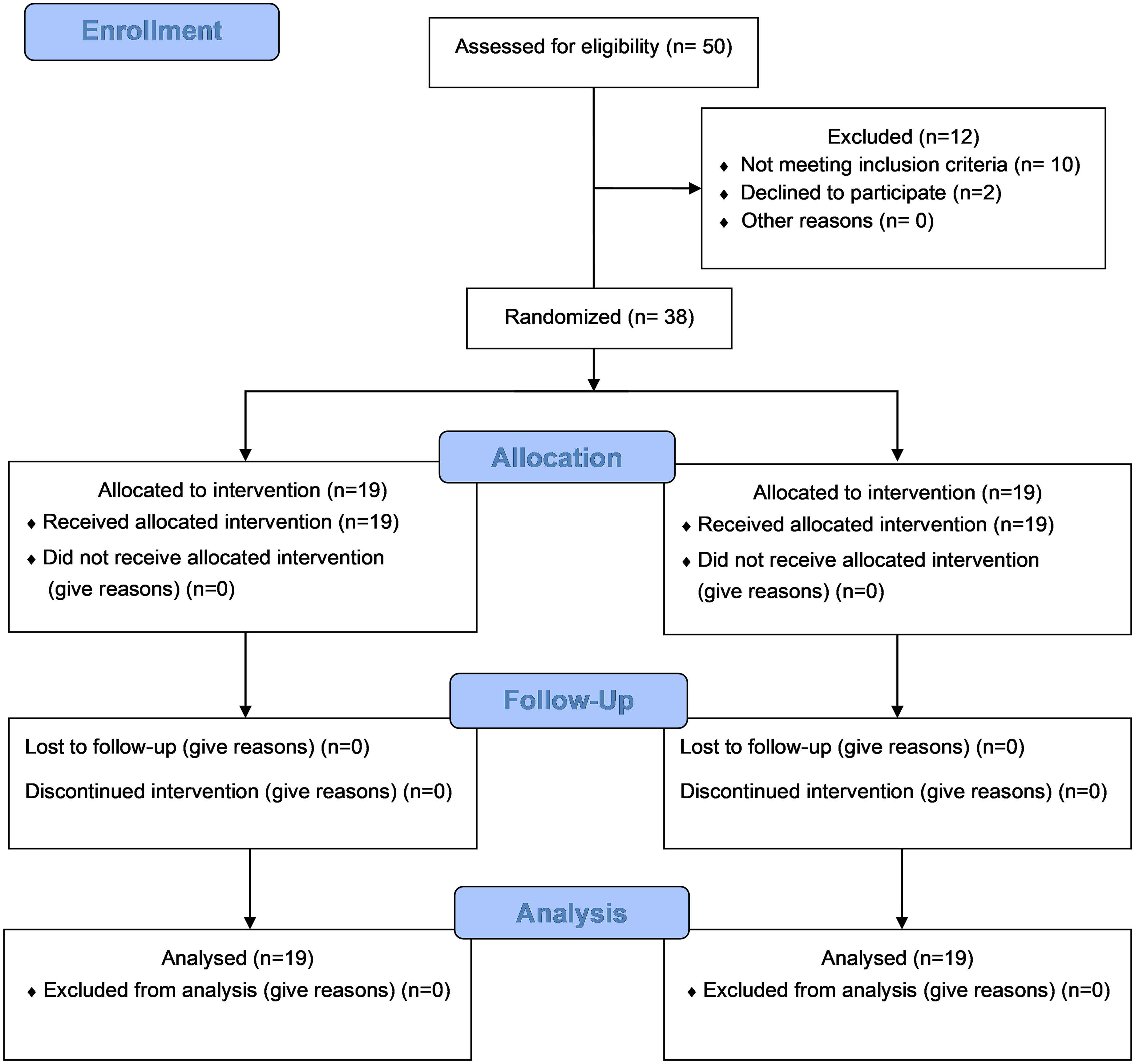
Consort Diagram.
Sample Size Estimation
The sample size was calculated using the formula:
Where, Zα = 1.96 (95% Confidence interval), Z β= 1.28,
Procedure
Interventions
Subjects in Gr 1 underwent SWB exercises [see Figure 3(A, B)] for 15 min and three sessions (with the periods of rest time based on the child's tolerance limit) for six days/week for up to 2 weeks. The exercises included prone weight-bearing for both ULs (lying prone over a bolster or Physio-roll) on forearms and hands (with an open palm and neutral trunk alignment over a wedge) and side-sitting weight-bearing (over a soft, firm cushion surface) on the involved hand only. Since children with MACS Level IV and V were only selected for this study, hence if any children were unable to maintain a full elbow extension position, the same was incorporated manually by the investigator (supporting the elbow to the limit of their initiation till they were able to maintain the same by themselves).

3A (Lateral View) & 3B (Anterior View)- SWB Therapy.
Both positions were equally distributed and implemented in alternate orders during each session by the primary investigator (1st author) at the Neuro-sensory Developmental unit of a medical college. Each position was demonstrated to the parents until they learned to perform it correctly (to be practiced at home).
Subjects in Gr 2 underwent the standard m-CIMT program (Sakzewski et al., 2014) for 45 min, equally divided into three sessions six days/week for up to 2 weeks. The non-involved hand was restrained in a restraining fabric glove till the treatment time. Tasks included are functional tasks, board games, and manipulative games.
Assessment and Instruments
The grasping subtest of FM_PDMS-2 has 26 items, while the VMI subtest includes 72 items that measure a child's ability to use his/her hands. The administration of FM_PDMS-2 requires detecting the entry point (where 75% of children in the normative sample at that age passed), basal level (the last score of 2 on three items in a row before the 1 or 0 scores), and ceiling level (when the child scores 0 on each of three items in a row) for each child before and after the intervention. The scoring criteria for each item are as follows: 2: The child performs the item according to the criteria specific for mastery; 1: The child's performance shows a clear resemblance to the item mastery criteria but does not fully meet the criteria; and, 0: The child cannot or will attempt the item, or the attempt does not show that skill is emerging. In this study, the raw scores of FM_PDMS-2 for both subtests were used to calculate changes following intervention (Elvrum et al., 2016; Wang et al., 2006).
Pre- (baseline) and post-intervention outcome measures using the FM_PDMS-2 scale were recorded by an independent evaluator who was blinded to the intervention protocol for both groups.
Data Analysis
The collected data of all 38 subjects was coded and entered in the Statistical Package for Social Science v 25.0. Descriptive statistics were used to calculate demographic characteristics and were summarised as mean and standard deviation. All variables of FM_PDMS-2 were analyzed using within-group differences in hand functions (pre- and post-intervention) and were tested for significance using the Wilcoxon signed rank test.
Results
This study examined the differences in hand function outcomes using FM_PDMS-2 following SWB exercises (Gr 1) and m-CIMT (Gr 2) in children with UCP. Thirty-eight children with UCP (N = 50 children with UCP assessed for eligibility) were recruited based on the proposed inclusion criteria with equal numbers (n = 19) in each intervention group. Gender-wise distribution was equal (50%, n = 19), and the age range was 2–5 years (mean age 4.184 ± 0.8533). Demographic details of the children with UCP are summarised in Table 1.
Descriptive Statistics of Subjects.
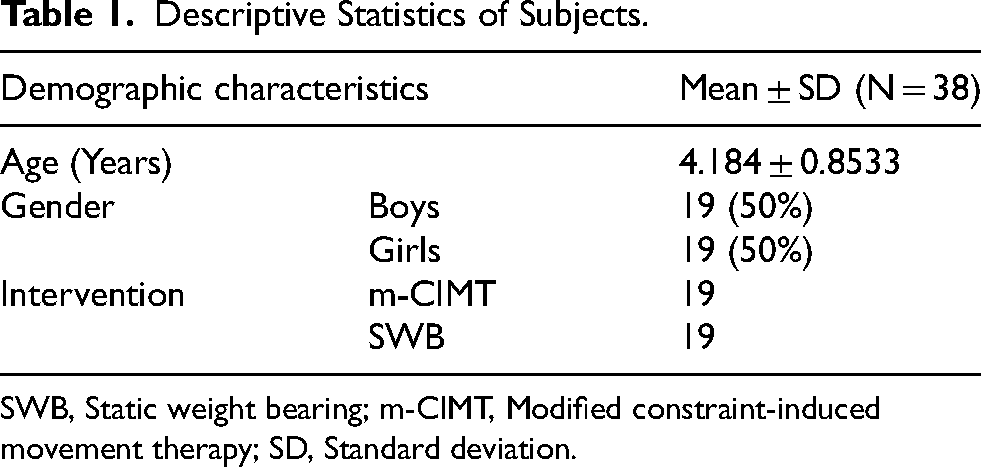
SWB, Static weight bearing; m-CIMT, Modified constraint-induced movement therapy; SD, Standard deviation.
The changes in FM_PDMS-2 subtests Pre-Post-Intervention were following:
SWB (Gr 1): The mean difference and percentage change (post-intervention) for the subtest Grasping were 12.79 and 37.67%, and for the VMI subtest were 15.89 and 14.11%, respectively. See Table 2 m-CIMT (Gr 2): The mean difference and percentage change (post-intervention) for the subtest Grasping were 5.05 and 12.78%, and for the VMI subtest were 5.80 and 4.88%, respectively. See Table 2
Changes in FM_PDMS-2 (Grasping and VMI) Subtests: Static Weight-bearing (Gr 1) and m-CIMT (Gr 2).
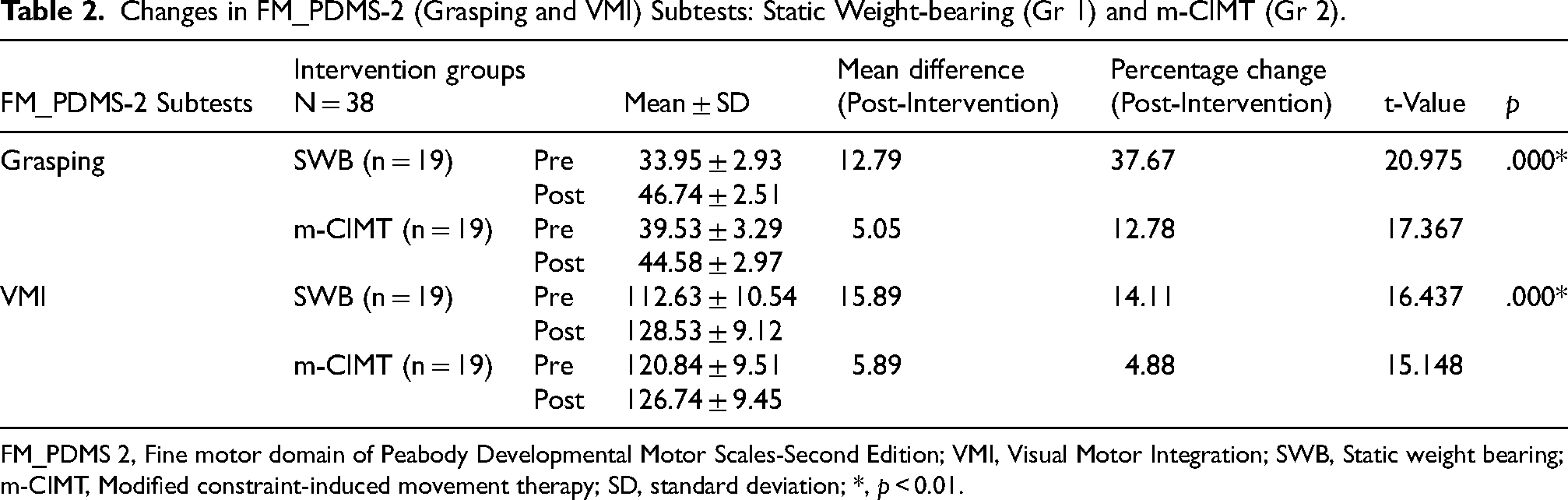
FM_PDMS 2, Fine motor domain of Peabody Developmental Motor Scales-Second Edition; VMI, Visual Motor Integration; SWB, Static weight bearing; m-CIMT, Modified constraint-induced movement therapy; SD, standard deviation; *, p < 0.01.
The post-intervention changes were greater in the Static weight-bearing (Gr 1) group compared to the m-CIMT (Gr 2) for both the subtests of FM_PDMS-2, and these were highly significant (p = 0.000).
Discussion
In children with UCP, the hand function is compromised due to spasticity and the secondary changes, i.e., reduced muscle strength, tightness/ contractures around joints, and abnormalities in bony structures. These changes lead to postural maladaptation i.e., scapular retraction/depression, shoulder internal rotation, elbow and wrist flexion, and adduction/flexion of the thumb and fingers, affecting coordination of activities between arm and hand to smoothly perform movement sequences during functional tasks (Jackman et al., 2014; Pin, 2007; Ten Berge et al., 2012).
The SWB exercises are widely used for children with CP, commonly achieved by positioning the UL in a prone with arms in extension or side sitting with support on an extended arm, i.e., weight is born directly through the hands or forearms (Pin, 2007). SWB exercises prevent tightness or contracture of soft tissues, restore the length of muscles, and reduce spasticity by inhibiting motor neuron excitability through prolonged stretch and compression on the muscle spindles, golgi tendon organs, cutaneous receptors, and joint receptors (Pin, 2007).
Therefore, the present study examined the effects of SWB exercises (N = 19) and m-CIMT (N = 19) on fine motor skills using FM_PDMS subtests in children with UCP aged 2–5 years (mean 4.184 ± 0.8533 years). The results showed positive changes in the mean differences and percentage change post-intervention for both the therapeutic strategies, i.e., SWB and m-CIMT. However, changes in fine motor skills on FM_PDMS were more significant for the SWB exercise group than for m-CIMT.
These reasons for such results are attributed to the SWB exercises that activate the dormant sensors of joint and muscle receptors, which activate the mechanoreceptors and proprioceptors on the ventral surface of the hand, inducing plastic motor changes leading to improved motor functions (van Meeteren et al., 2007). Studies have also reported that weight bearing facilitates compression on the muscle spindles, golgi tendons, and joint receptors, which helps to restore muscle length through prolonged elongation (Eliasson et al., 1992; Eliasson et al., 1995). In another study, the authors reported that weight bearing improves the musculoskeletal components and hand opening (if practiced for more than 30 therapy sessions) (Meeteren et al., 2007), which improves reach, grasp, and prehension skills (Schieber & Santello, 2004). The present study showed improved hand functions after 42 treatment sessions (15 min of 3 sessions/ day) following SWB exercises; hence, the results are in sync with the published research.
Another important finding of the present study was the considerably higher percentage change (post-intervention) for the Grasping subtest than the VMI subtest of FM_PDMS. We attribute this observation to the number of item differences between the two subtests, i.e., Grasping (26 items) and VMI (72 items). This causes early attainment of the ceiling level for the Grasping subtest of FM_PDMS.
The critical element of m-CIMT is to involve children in an active intervention i.e., play and functional activities, through the forced use of the involved extremity. In the present study, the positive changes seen following m-CIMT, small compared to the SWB, are like other studies that had reported more incredible motor changes and produced pre-planned reaching movement during unilateral tasks, leading to improved functional performance (Schieber & Santello, 2004).
In children with UCP, the hand functions and its components (e.g., muscles, joints, and bones) and other multiple limb functions (e.g., muscle strength, control of rapid coordinated movements, touch-pressure detection, and recognition of common objects and shapes) are affected (Arnould et al., 2014). These limits the ICF domain of activities, i.e., the ability to execute an essential task of daily living. The ICF formalizes the impact of CP on a child's hand functioning through its theoretical framework to categorize UL measurements at two levels (Klingels et al., 2012),
at the body function level- passive range of motion, muscle tone, strength, and sensibility, and at the activity level-
Capacity (e.g., active range of motion, fluency, accuracy, dexterity, movement speed), and Performance (e.g., spontaneous use of the affected hand during activities or play.
In the context of the above, SWB exercises might have influenced the body function level, while m-CIMT caused changes at the activity level, hence the changes seen due to either of the interventions. The weight bearing brings transformation to the passive ROM, muscle tone, strength, and sensibility, which alters the structure and function collectively, hence the enhanced improvements in hand function in children with UCP.
In the present study, both groups, i.e., SWB and m-CIMT, showed significant differences in the percentage change post-intervention. However, more improvement was seen in the SWB exercise group than in the m-CIMT. Therefore, it is justified that SWB exercises improve hand function; hence, they can be recommended as an important therapy strategy in children with UCP.
The present study investigated the hand function outcome between prone-weight bearing and m-CIMT in children with UCP, and the results support the benefits of SWB exercise; however, follow-up was not considered to know how long these effects lasted. Hence, further studies are recommended involving a homogenous sample and assessing the long-term effects of SWB and m-CIMT.
Conclusion
Both groups, i.e., SWB and m-CIMT, showed a substantial change in the Grasping and VMI subtest of FM_PDMS post-intervention. However, there was more improvement for the SWB exercise group. Thus, the findings confirm that SWB exercises bring more improvement in hand function and thus should be recommended as an important therapy strategy to enhance hand functions in children with UCP.
Footnotes
Acknowledgments
The authors are grateful to all the children and their parents and would like to thank them for their participation in this study. The authors also acknowledge the contributions of the faculty of physiotherapy at Kasturba Medical College, Mangalore, for their critical review of the study protocol at the time of study design during protocol evaluation.
ORCID iDs
Ethical Considerations
The Scientific and Institutional Ethics Committee of Kasturba Medical College, Mangalore reviewed and approved (IEC/KMC/MLR 11-17/224) the studies involving human participants. The study was registered with the Clinical Trial Registry- India (CTRI) [reference number CTRI/2018/01/011278].
Informed Consent
Written informed consent to participate in this study was provided by the participant's legal guardian/next of kin.
Author Contributions/CRediT
The role of the authors in this study is as follows:
Funding
This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicting Interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.