
Abstract
Background
Previous research has demonstrated the relationship between vulnerability and community participation, the correlation between vulnerability and gratitude, and the role of gratitude in enhancing participation. To our knowledge, there have been no studies examining the role of gratitude in the relationship between vulnerability and community participation.
Objective
The purpose of this study was to investigate whether gratitude moderates the effect of vulnerability on community participation in individuals with multiple sclerosis (MS).
Methods
Participants were recruited from the National MS Society (N = 373). Descriptive statistics, correlation analysis, and moderation analysis were carried out.
Results
Findings demonstrated lower scores of vulnerability index were associated with increased community participation. Additionally, higher levels of gratitude were associated with increased community participation. Furthermore, gratitude influenced the effect of vulnerability index on community participation.
Conclusion
Findings supported the importance of gratitude as a viable intervention strategy to help individuals with MS to achieve positive rehabilitation goals such as community participation.
Keywords
Introduction
Multiple sclerosis (MS) is an inflammatory neurological disorder that affects approximately 2.8 million people in the world (Goldenberg, 2012; Multiple Sclerosis International Federation, 2020). MS is a chronic disease with several recognized clinical courses (Lublin et al., 2014). Its symptoms can vary widely across individuals, but more common symptoms include fatigue, bladder/bowel problems, pain, and vision changes (Lakin et al., 2021). Progression and manifestation of symptoms of MS can be unpredictable (Compston & Coles, 2008), and this unpredictability can create major challenges for individuals in their daily life and in community participation such as employment. These challenges can be due to various reasons, ranging from severe physical problems to the inability to maneuver and embarrassment in a social setting (Månsson & Lexell, 2004; Pfaller et al., 2020). Furthermore, the onset of MS often ranges between the ages of 20 and 40 years old (Pfaller et al., 2020). At this stage in the life cycle, one is highly likely to be actively participating and engaging in the community in several domains, such as employment, raising families, and social and recreational activities.
Community Participation
Community participation is recognized as a crucial quality of life component for individuals with chronic illnesses (Hemmingsson & Jonsson, 2005; Reinhardt & Stucki, 2007), and is conceptualized as being actively involved in intrinsically social activities that may take place outside or inside the home (Chang et al., 2013). According to studies on individuals with MS, there are many pertinent demographic, psychosocial and environmental predictors that are associated with reduced community participation, and these predictors include activity limitation (Pfaller et al., 2020), low educational attainment (Pfaller et al., 2020), environmental barriers (Plow et al., 2015), cognitive problems (Plow et al., 2015), disability-related stress (Lee et al., 2023), and low resilience (Lee et al., 2023). For instance, Sundar et al. (2016) showed that individuals with mobility disabilities have low community participation, including work, religious and civic activities, participation in leisure, and volunteer opportunities. Similarly, people with MS have been found to have low community participation due to depression, anxiety, pain, stress, and fatigue (Yorkston et al., 2012). Conradsson et al. (2020) also reported that people with MS who did not engage in employment by 10 years after their diagnosis had significantly reduced participation in domestic activities, walking, and daily life. Consistently, symptoms of MS restrict individuals from participating in the community and pose changes in activity participation and employment (Conradsson et al., 2018; Goverover et al., 2020).
Vulnerability Construct
Vulnerability can be conceptualized as factors that can influence an individual's likelihood of thriving (Schmidtlein et al., 2008). However, Ford et al. (2024) argue that instead of trying to define vulnerability or make it more definite and less ambiguous, one should embrace its indeterminacy and allow the concept to remain capacious. Importantly, Dunning and Durden (2013) compared four social vulnerability analysis tools and identified disability as one vulnerability factor. A study by Gartrell et al. (2018) drew upon the social determinants of health perspective to examine how factors such as social, cultural, and economic contexts influenced disability-based disadvantages. They concluded that inaccessible physical environments, inadequate social support, and institutionalized inequalities prevent people with disabilities from actively engaging in daily life, which further worsened their vulnerability. Among people of reproductive age, van der Meer et al. (2022)—in their synthesis of evidence on social determinants of vulnerability—reported that low socioeconomic attainment, lack of connection with the social environment (community participation), adverse life events, and lack of supportive social networks reduced people's ability to cope and be resilient, hence vulnerable. In sum, vulnerability can be biological, health-related, cultural, and relational (Aday, 2002; Grabovschi et al., 2013; Mechanic & Tanner, 2007). An individual could have several vulnerabilities simultaneously (Haidar et al., 2018).
For this study focusing on individuals with MS, we conceptualized vulnerability as the combination of social and cultural factors that put an individual in a disadvantaged position, which can include being a racial/ethnic minority, having less than a high school education, being unemployed, not having health insurance, and not seeing a primary care physician regularly. This broader definition of vulnerability is imperative to consider, because in the chronic disease literature these social factors are increasingly viewed as key predictors of disease initiation, progression and disability (Cockerham et al., 2017; Wallace et al., 2015). At the same time, disease and symptom progression of MS can also make individuals with MS more vulnerable. Therefore, it is important to consider the incorporation of both disability as a vulnerability factor and disability-induced vulnerabilities (i.e., challenges stemming from living with a disability that make individuals more susceptible to psychosocial difficulties).
Vulnerability factors. Ranganathan and Bhopal (2006) reported that being a minority reduces access to interventions because of a possible lack of applicability of evidence from the main population to minority populations. There is also increased morbidity among racial and ethnic minorities as compared to the majority population. Nazroo (2003) argues that the lack of representation of ethnic or racial minorities in research increases the vulnerability of ethnic/racial minorities to poor health outcomes.
Having less than a high school education is another indicator of vulnerability. Zajacova and Lawrence (2018) indicated that 57% of participants in their study without a high school education reported poorer health, as compared to only 9% of those with a college degree. Hayward et al. (2015) also reported that, in the twenty-first century, higher mortality rate was associated with adults who have a lower educational attainment.
In terms of unemployment, Herbig et al. (2013) reported that those who are long-term unemployed have a higher burden of disease. Unemployment is also found to have greater adverse effects on the mental health of vulnerable populations, such as single mothers, male manual workers, main-earner women, and manual workers without benefits (Puig-Barrachina et al., 2011). Importantly, unemployment is also high for people with disabilities as compared to people without disabilities, even after controlling for age, gender, and education (Paul and Hollederer (2023).
Not having health insurance and not seeing a primary care physician regularly are additional unique indicators of vulnerability in this study. In their study of preventive care among adults based on insurance status and usual source of care, DeVoe et al. (2003) found that adults who had not completed high school were less likely to have health insurance and a usual source of care, which resulted in poorer health outcomes. People who have a regular primary care physician are less likely to use emergency services, and—if admitted to the hospital—they tend to stay there for shorter lengths of time (McAlister et al., 2018; Swanson et al., 2022). There could be several reasons people do not have health insurance. For example, in the US, adults with poorer health were less likely to be insured because they could not afford it (Cha & Cohen, 2020). Not having health insurance also restricts a person's access to healthcare, which leads to poorer health outcomes (Michael McWilliams, 2009; Neiman et al., 2021).
Gratitude
Even though an individual with a chronic illness can have heightened vulnerability factors that could negatively affect the person's recovery, goal and/or health outcomes, there are factors that can counteract its negative effect. Sansone and Sansone (2010) defined gratitude as the appreciation of what is valuable and meaningful to a person and a general state of thankfulness and or appreciation. Gratitude has been defined as the tendency to appreciate the good and positive, and it is related to positive relationships that are both self-reported and peer-reported (Algoe et al., 2008; Emmons & McCullough, 2003; Wood et al., 2008).
Recent research has found that gratitude—a positive emotion involving the recognition that one has benefitted from the generosity of another person (McCullough et al., 2008)—plays an important role in the improved quality of life among individuals with MS (Crouch et al., 2020). Empirical evidence supports the importance of gratitude and quality of life in the general and chronic illness population (Emmons & McCullough, 2003; Wood et al., 2010). Gratitude has also been found to be related to several positive outcomes, including increased resilience to trauma through building personal, cognitive, and behavioral resources (Kashdan et al., 2006) as well as improvement of social relationships (Lambert et al., 2010).
Objective
Previous research has demonstrated the relationship of some of the constructs studied, but not in the context of individuals with MS. For instance, a systematic review demonstrated that ample studies have demonstrated the relationship between social vulnerability and community participation among aging adults (Cappelli et al., 2020). Among the general, non-disabled population, the relationship between psychological vulnerability and gratitude was demonstrated (Ilbay & Sarıçam, 2015), and the expression of gratitude can enhance participation, even in the cyberspace (Makri & Turner, 2020). However, the power of gratitude, to our knowledge, has not been analyzed to determine whether it could be beneficial for enhancing the community participation of the disability population, particularly in a disability group that is in the prime of their life for active participation in the community, including employment. Therefore, our research question was: Does gratitude moderate the effect of vulnerability on community participation in individuals with MS?
Methods
Participants
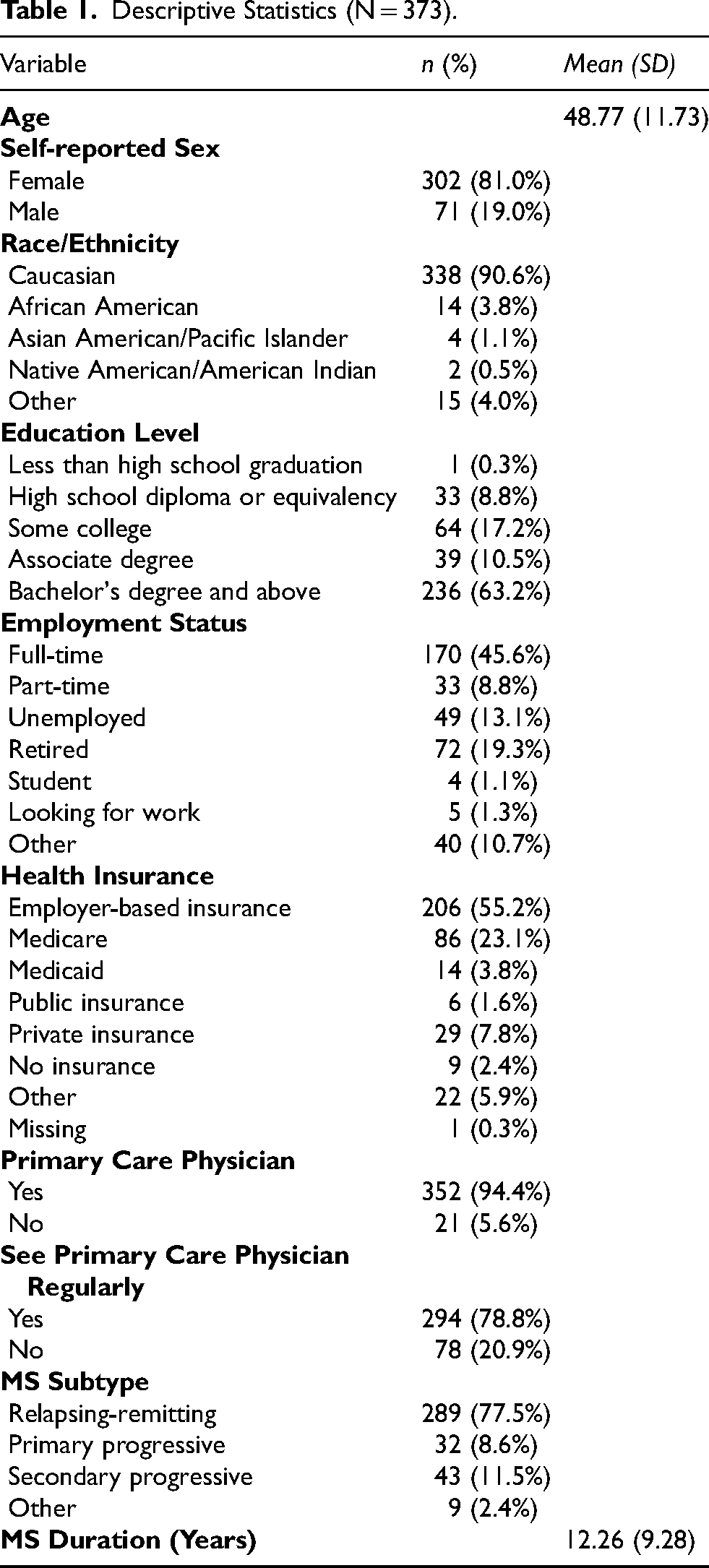
A total of 446 participants started the survey with 77 not completing the full survey, resulting in 373 participants that were included in the study. Participants’ ages ranged from 21 to 77 years old (M = 48.77; SD = 11.73). The majority identified as female (81.0%). Regarding race/ethnicity, 90.6% identified as Caucasians. In terms of education level, most participants reported having a bachelor's degree and above (63.2%). For employment status, 45.6% reported being full-time employed. Regarding health insurance, 55.2% of the participants reported having employer-based insurance, followed by Medicare (23.1%) and private insurance (7.8%). For primary care, 78.8% reported seeing their primary care physician regularly. In terms of MS characteristics, 77.5% indicated having relapsing-remitting MS (i.e., the most common MS subtype where there are episodes of symptom flare-ups followed by partial or complete recovery), and the average MS duration was 12.26 years. For detailed demographics and MS characteristics, please refer to Table 1.
Descriptive Statistics (N = 373).
Procedure
Upon the Institutional Review Board study approval, the first author contacted the National Multiple Sclerosis Society (NMSS) to advertise the study on their website and in emails to NMSS members. More specifically, the study link was disseminated via the NMSS website and direct email outreach to NMSS members. The survey was administered via Qualtrics, ensuring data security and participant anonymity. Inclusion criteria for the study participants were being at least 18 years of age and having a MS diagnosis. The advertisement consisted of a short description and the link to the study. The link further provided a consent page and pertinent information to the participants. Participants then proceeded with the survey if they agreed to move forward. The survey included sociodemographic, MS-related characteristics, and psychosocial variables. As indicated in the consent form, the first 250 participants received a $10 gift card for their participation.
Measures
Gratitude
Gratitude was assessed with a 6-item Gratitude Questionnaire-6 (GQ-6) (McCullough et al., 2002). A sample item is “I have so much in life to be thankful for.” Each item was rated on a 7-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree). Two items were reverse scored. Scores were summed and averaged. Higher scores represent higher levels of gratitude. In the current study, the Cronbach's alpha was computed to be .85 (good internal consistency).
Community Participation
Community participation was assessed with the 8-item NEURO-QOL Ability to Participate in Social Roles and Activities Short Form v1.0 (Cella et al., 2012). A sample item includes “I can keep up with my family responsibilities.” Each item was rated on a 5-point Likert scale, ranging from 1 (never) to 5 (always). Scores were summed. In the current study, Cronbach's alpha was .93 (excellent internal consistency).
Vulnerability Index
Participants’ sociodemographic characteristics were assessed, including age, race/ethnicity, education, employment, and health insurance. A vulnerability index score using various sociodemographic indicators was created based on prior literature (e.g., DeVoe et al., 2003; Nazroo, 2003; Neiman et al., 2021; Puig-Barrachina et al., 2011; Swanson et al., 2022; Zajacova & Lawrence, 2018). The vulnerability index included being a racial/ethnic minority, having less than a high school education, being unemployed, not having a health insurance, and not seeing a primary care physician regularly.
Data Analysis
All statistical analyses were conducted using the Statistical Package for Social Sciences version 28.0. Descriptive statistics were performed to demonstrate demographic and MS characteristics. Correlation analysis was carried out to examine the relationships between study variables (e.g., the strength of linear relationship between vulnerability index and gratitude). Moderation analysis was carried out following the procedures from Aiken and West (1991) and with the PROCESS macro (Hayes, 2022) and RStudio Team (2022). Moderation analysis was carried out if the moderator (i.e., gratitude) influenced the strength of the relationship between the independent variable (i.e., vulnerability index) and the dependent variable (i.e., community participation). Materials and analysis code for this study are not available. Statistical significance was set at p < .05
Results
Descriptive Statistics
Gratitude levels ranged from 2 to 7 (M = 5.82; SD = 1.10). Community participation scores ranged from 12 to 40 (M = 28.82; SD = 6.53).
Correlation Analysis
Vulnerability index was negatively correlated with gratitude (r = −.13; p < .05) and community participation (r = −.20; p < .001). Gratitude was positively associated with community participation (r = .39; p < .001).
Moderation Analysis
Moderation analysis was performed to examine if gratitude served as a moderator between the relationship of vulnerability index and community participation. The main effect for vulnerability index (B = −1.61; p < .01) was significant, suggesting that lower scores of vulnerability index were associated with increased community participation. Additionally, the main effect for gratitude (B = 2.27; p < .001) was significant, suggesting that higher levels of gratitude were associated with increased community participation. The interaction term for vulnerability index and gratitude (B = −.86; p < .05) was significant, which suggested that gratitude influenced the effect of vulnerability index on community participation. As observed in Figure 1, the effect of vulnerability index on community participation is stronger for people with higher levels of gratitude (slope = −2.55) compared to those with lower levels of gratitude (slope = −.67).
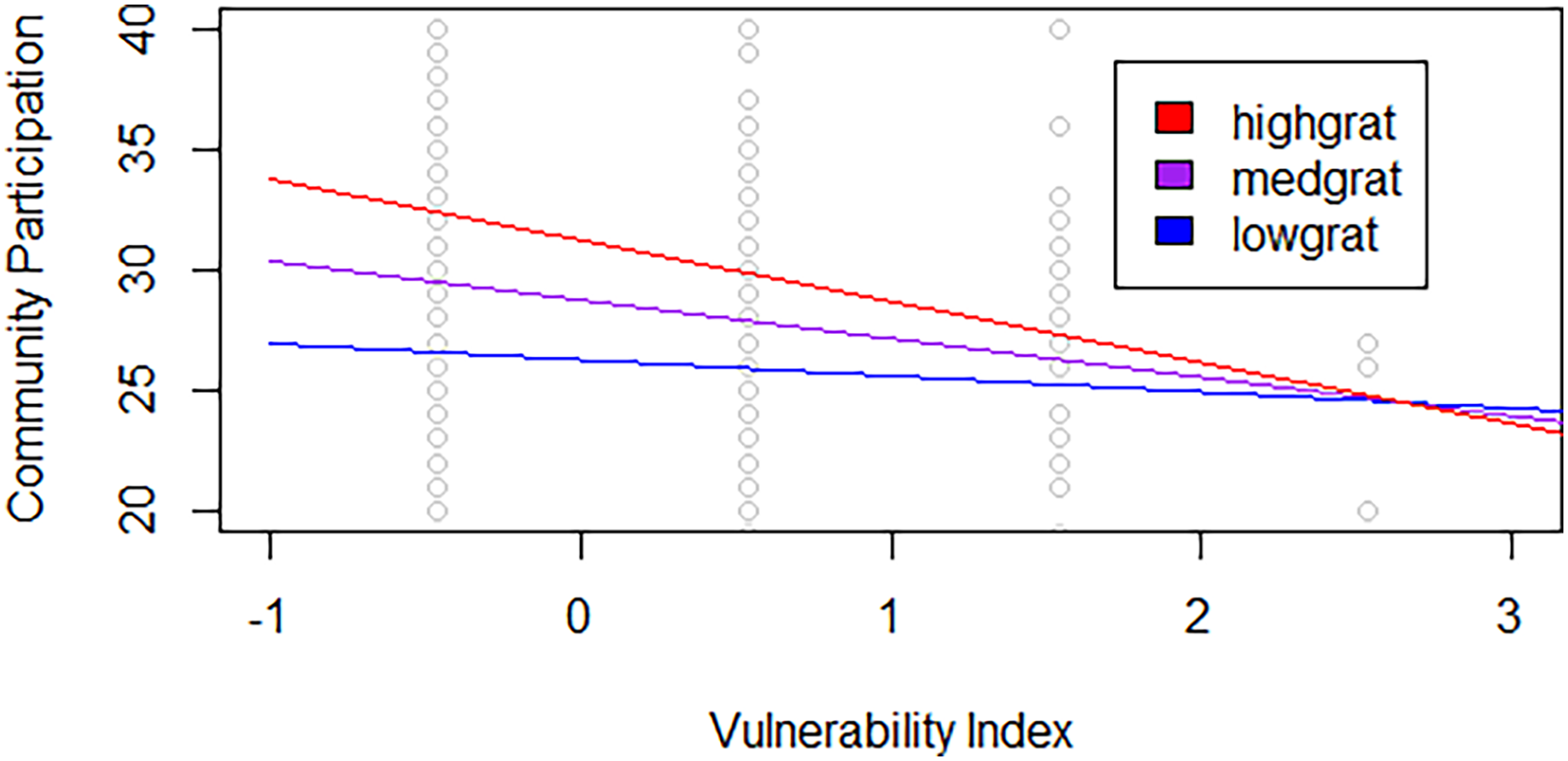
Gratitude as a Moderator between Vulnerability Index and Community Participation (N = 373).
Discussion
Study Findings
The current study investigated the moderation effect of gratitude on the relationship between vulnerability index and community participation among 373 participants with MS. Though existing studies showed relationships about impacts of MS on individuals, no previous studies directly investigated the impact of gratitude on the outcome of community participation. However, by comparing studies on gratitude (Crouch et al., 2020), we reasonably concluded our results are consistent regarding the patterns of the gratitude effects.
Specifically, results supported that vulnerability was negatively related to community participation among our MS participants. In our study, vulnerability was conceptualized as a multidimensional domain that encompasses social, cultural, and disease-related factors that put a person in a disadvantaged position, which includes race, ethnicity, education level, employment status, having health insurance, and whether one has access to a regular primary care physician to maintain healthcare services (Gartrell et al., 2018; van der Meer et al., 2022). Social and cultural factors have been shown to predict disease initiation, progression and disability (Cockerham et al., 2017; Wallace et al., 2015). Disability is considered a vulnerable factor (Dunning & Durden, 2013). MS is a highly vulnerable illness due to the variability of symptoms, progressive and unpredictable nature of prognosis (Compston & Coles, 2008), as well as the associated functional limitations such as physical (Månsson & Lexell, 2004), cognitive (Plow et al., 2015), and mental health (Yorkston et al., 2012).
Ample evidence also supported that individuals with chronic illness and disability, including those with MS, who are at a vulnerable status often have poor outcomes in their health or life goals that can be affected by the illness. For instance, due to the impact of the disease, many community and daily living activities (e.g., employment) are substantially and negatively impacted (Conradsson et al., 2018; Goverover et al., 2020). The associated symptoms of MS, including physical issues and cognitive issues, caused limited activity and thus further reduced community participation such as employment (Månsson & Lexell, 2004; Pfaller et al., 2020; Plow et al., 2015). Furthermore, studies also showed there are non-MS factors that were associated with decreased community participation among individuals with MS, including environmental barriers (Plow et al., 2015), low education (Pfaller et al., 2020), low resilience (Lee et al., 2023), and feelings of embarrassment in social settings (Månsson & Lexell, 2004).
Our participants showed a relatively low vulnerability level associated with a high level of community participation, as results showed a positive effect of gratitude. Specifically, the interaction effect demonstrated gratitude as a moderator in affecting the relationship between vulnerability and community participation. More importantly, the effect of this relationship is stronger for individuals with MS who have higher gratitude than those with a lower level of gratitude, therefore further underscoring the importance of gratitude as a buffer to motivate individuals with MS who are at a vulnerable position not to be able to engage in pursuing their personal and life goals. Although gratitude has not been used as a strategy to improve community participation for MS to the best of our knowledge, the use of gratitude to enhance other important outcomes has been well documented, including quality of life in the general and chronic illness sample (Crouch et al., 2020; Emmons & McCullough, 2003; Wood et al., 2010). Gratitude has also been used to increase resilience in trauma (Kashdan et al., 2006) and social relationships (Lambert et al., 2010). Given that individuals with MS often are at the stage of their life where many active engagements of life occur, quality of life often becomes a broader goal than health and mental health. Thus, the current study applies the concepts of gratitude which have been shown to be effective in improving quality of life in MS and applying it to the broader concept of community participation. Since employment is considered an aspect of community participation, this study highlights the role of gratitude in helping individuals with MS mitigate the adverse effects of vulnerability on employment. In other words, by promoting gratitude levels among clients with MS, that could potentially help them alleviate the negative impact of vulnerability, such as sociocultural and disease-related factors, on employment outcomes.
Strengths
The current study, to the best of our knowledge, is the first attempt to apply the concept gratitude in investigating its effect on the broader concept of community participation such as employment as a moderator among individuals with MS. Although gratitude and MS have been studied, a lot has been focused on clinical outcomes such as quality of life. Individuals with MS often are at a stage where they build their self-identity on their work, social and recreational groups. Thus, understanding the impact and how to rehabilitate this aspect of a person is imperative in the employment and social participation realm.
Limitations and Future Research Implications
While the concept of this research question is innovative, the study is not without limitations, which can further be built upon in future research. Independent replication of this study will further add to the scientific evidence. Though moderation analysis was run, no actual intervention was done. A future study on the application of a gratitude intervention with comparison group will add to the rigor of the research. Furthermore, the vulnerability factor is likely to be a potential limitation. Some of the demographics, such as race and ethnicity, types of MS, and availability of insurance, remained relatively homogenous. According to Hittle et al. (2023), the prevalence rate of people with MS across race/ethnicity are as follows: White (4 people out of 1000), Black (3 people out of 1000), people of other races (2 people out of 1000), and Hispanic/Latinx (1.5 people out of 1000). Our sample also was composed of a relatively “well adjusted” group, thus making the variability of results narrow. The narrow sample makes generalizability limited. Therefore, future studies could make additional efforts to collect data from more heterogeneous samples. For instance, we will gain a more representative group with varying vulnerability by setting inclusion criteria with a quota to ensure that we gather data from those who have lower educational attainment, are unemployed, and have lower income.
Clinical Implications
There are several important clinical implications based on the results of this study that are worth noting. First, the most important implication is acknowledging the importance of gratitude as a strategy to enhance outcomes when working with individuals with MS. Though the specific result from this study supports that gratitude enhances community integration, which encompasses many aspects such as work, social, and recreational domains, other studies also support that gratitude is beneficial for other outcomes such as quality of life and resilience. Professionals, therefore, must keep in mind its value, and should promote and implement (if appropriate) or refer individuals with MS who they work with. For instance, incorporating a gratitude list (i.e., making a list of things to be grateful for on a regular basis) has been demonstrated to improve worker's well-being (Komase et al., 2021). Rehabilitation professionals can encourage clients with MS in creating a gratitude list regularly as this exercise can be implemented easily in daily life, including at their workplace. Second, understanding vulnerability is important for individuals with MS. In this study, we broaden vulnerability to include sociocultural as well as disability-related factors. Thus, professionals must be aware of the many facets of vulnerability factors that individuals may face that could affect their community participation outcomes (including employment), which not only include demographic variables but also disability-specific variables. Previous research demonstrated that sociodemographic aspects (e.g., educational attainment, ethnicity) have been linked to work-related quality of life (Coura et al., 2017). For example, when working with clients with MS to acquire and sustain employment, rehabilitation professionals should take vulnerability factors into consideration as they can influence their employment prospects.
Conclusion
This study examined the moderating effect of gratitude on the relationship between vulnerability index—which includes demographic and disability-related factors—and community participation among 373 individuals with MS. Our result supported that low vulnerability is related to high community participation, and high gratitude is related to high community participation. More importantly, the effect of vulnerability on community participation was stronger for those with higher levels of gratitude than for those with lower levels, thus supporting the importance of gratitude as a viable intervention strategy to help individuals achieve positive goals such as community participation. Thus, gratitude should be considered as a practice and/or strategy when working with individuals with MS, as it can help them with their respective goals in engaging in the community (e.g., employment) and can improve understanding of how their disability as well as other unique social/cultural factors may play a vulnerable role in affecting them.
Footnotes
Acknowledgements
None to report.
Ethical Considerations
The study was reviewed and approved by the University of Wisconsin-Madison Institutional Review Board as an exemption study (#2019-1262).
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Funding
Support for this research was provided by the University of Wisconsin–Madison, Office of the Vice Chancellor for Research and Graduate Education with funding from the Wisconsin Alumni Research Foundation.
Declaration of Conflicting Interests
One of the authors, Beatrice Lee, is an editorial board member of the Journal of Vocational Rehabilitation.