
Abstract
Background:
Preoperative management of Graves’ disease (GD) typically includes antithyroid drugs, β-blockers, and short-term iodine. However, intensified therapy may result in excessive elevation of thyroid-stimulating hormone (TSH). Whether a TSH threshold (≥10.0 μIU/mL) can determine greater operative difficulty in such patients is unclear. Therefore, we assessed this association in patients with GD who underwent total thyroidectomy.
Methods:
This retrospective cohort study included consecutive patients with GD who underwent total thyroidectomy at a single center between 2009 and 2022 (n = 1516). The primary analysis comprised a complete case-cohort design (n = 1407; TSH ≥ 10.0 group, n = 48; TSH < 10.0 group, n = 1359). Primary outcomes included intraoperative blood loss, enlargement ratio (ER; estimated preoperative thyroid weight/preadmission thyroid weight), and operative time. Secondary outcomes were perioperative complications and resected thyroid weight. Multivariable linear or logistic regression included prespecified covariates. Rare events were modeled using Firth’s penalized logistic regression. For temporal context, we compared preadmission and preoperative TSH levels. Preoperative TSH was modeled as four clinically defined categories based on the institutional reference range to address heterogeneity within the TSH < 10.0 μIU/mL category.
Results:
Of 1407 patients, 48 (3.4%) had preoperative TSH ≥ 10.0 μIU/mL. Unadjusted analyses indicated that the TSH ≥ 10.0 group had greater blood loss (median, 52 mL vs. 34 mL; p < 0.001), higher ERs (1.137 vs. 1.029), longer operative times (129 minutes vs. 112 minutes), and heavier resected thyroids (131.8 g vs. 97.0 g). Adjusted models indicated that TSH ≥ 10.0 was independently associated with greater blood loss (β = 53.03 mL; p < 0.001) and higher ERs (β = 0.12; p = 0.002). Dichotomized analyses indicated that TSH ≥ 10.0 increased the odds of ER ≥ 1.1 (adjusted odds ratio [aOR] 2.60; p = 0.004) and operative times ≥ 120 minutes (aOR: 2.29; p = 0.018). Preadmission TSH ≥ 10.0 μIU/mL was more common in the TSH ≥ 10.0 group (20.8% vs. 3.2%), indicating earlier elevation.
Conclusions:
Preoperative TSH ≥ 10.0 μIU/mL was independently associated with greater blood loss and higher ERs in patients with GD who underwent total thyroidectomy. Avoiding iatrogenic hypothyroidism and marked TSH elevation during preoperative preparation may improve operative conditions.
Keywords
Introduction
Graves’ disease (GD) is an autoimmune thyroid disorder characterized by diffuse goiter and thyrotoxicosis. Total thyroidectomy is a definitive option when antithyroid drugs are ineffective or poorly tolerated, rapid disease control is necessary, or patients and clinicians prefer surgery.1,2 Although contemporary series have reported low permanent complication rates, thyroidectomy for GD is often technically demanding because of thyroid hypervascularity, friability, and interval gland enlargement. Reassessments of safety and efficacy have resulted in the increased use of total thyroidectomy as initial treatment for patients with antithyroid drug intolerance/contraindications, large or compressive goiter, or suspected thyroid malignancy, as well as for those who prefer surgery for definitive therapy. 3
Preoperative preparation aims to optimize thyroid function and the operative field and commonly includes the use of antithyroid drugs and, in some cases, potassium iodide (KI).1,2 Iodide can acutely suppress thyroid hormone synthesis, 4 reduce thyroid blood flow, and induce sclerosis-like changes, potentially reducing intraoperative blood loss and technical difficulty. However, evidence of the utility of KI is mixed, and practices vary across institutions.5–7
Although the goal of preparation is euthyroidism, overtreatment during titration may cause iatrogenic hypothyroidism, resulting in elevated thyroid-stimulating hormone (TSH) levels (“TSH overshoot”). Elevated preoperative TSH is often accompanied by interval gland enlargement and increased hemorrhagic operative fields despite standard preparation.
TSH, which is also known as thyrotropin, promotes follicular cell proliferation and activates angiogenic pathways within the thyroid,8,9 including upregulation of vascular endothelial growth factor, which increases intrathyroidal vascularity.10–12 These mechanisms provide a biological explanation linking elevated preoperative TSH with hemorrhagic, enlarged, and less navigable operative fields.
We examined the widely recognized threshold of TSH ≥ 10.0 μIU/mL, which is commonly used as a pragmatic and clinically communicable marker of significant hypothyroidism. 1 Although overt hypothyroidism is strictly defined by elevated TSH with low FT4, the relationship between preoperative TSH levels and operative difficulty in GD—particularly intraoperative blood loss and interval thyroid enlargement—has not been rigorously evaluated using this clinically actionable threshold. We hypothesized that markedly elevated preoperative TSH (≥10.0 μIU/mL) increases operative difficulty, specifically intraoperative blood loss and interval thyroid enlargement, through thyroidal angiogenesis and interstitial edema.
Materials and Methods
The primary objective of this large single-center cohort study was to evaluate whether a preoperative TSH threshold ≥10.0 μIU/mL is independently associated with greater operative difficulty during total thyroidectomy for GD as measured by intraoperative blood loss, ER, and operative time. The secondary objective was to assess whether preoperative KI exposure is independently associated with the primary outcomes after adjustment for prespecified covariates. Secondary analyses included clinically important safety outcomes such as reoperation for postoperative hematoma, permanent vocal cord paralysis, and permanent hypoparathyroidism.
The Ethics Committee of Kuma Hospital approved this study (20250612-3), which was conducted in accordance with the Declaration of Helsinki (2013 revision). Informed consent was waived with opt-out procedures and anonymized data handling.
This retrospective cohort study included consecutive patients with GD who underwent total thyroidectomy at a single center between January 2009 and December 2022 (Fig. 1). GD was diagnosed by board-certified specialists based on biochemical thyrotoxicosis with positive thyrotropin receptor antibody (TRAb) and/or increased radionuclide uptake supported by typical clinical and Doppler ultrasonographic findings such as diffuse goiter, orbitopathy, and increased thyroid blood flow. To exclude destructive thyroiditis and other etiologies, atypical cases were adjudicated during multidisciplinary conferences. Although a prior study of this cohort examined postoperative TRAb trajectories, 13 it addressed distinct objectives.
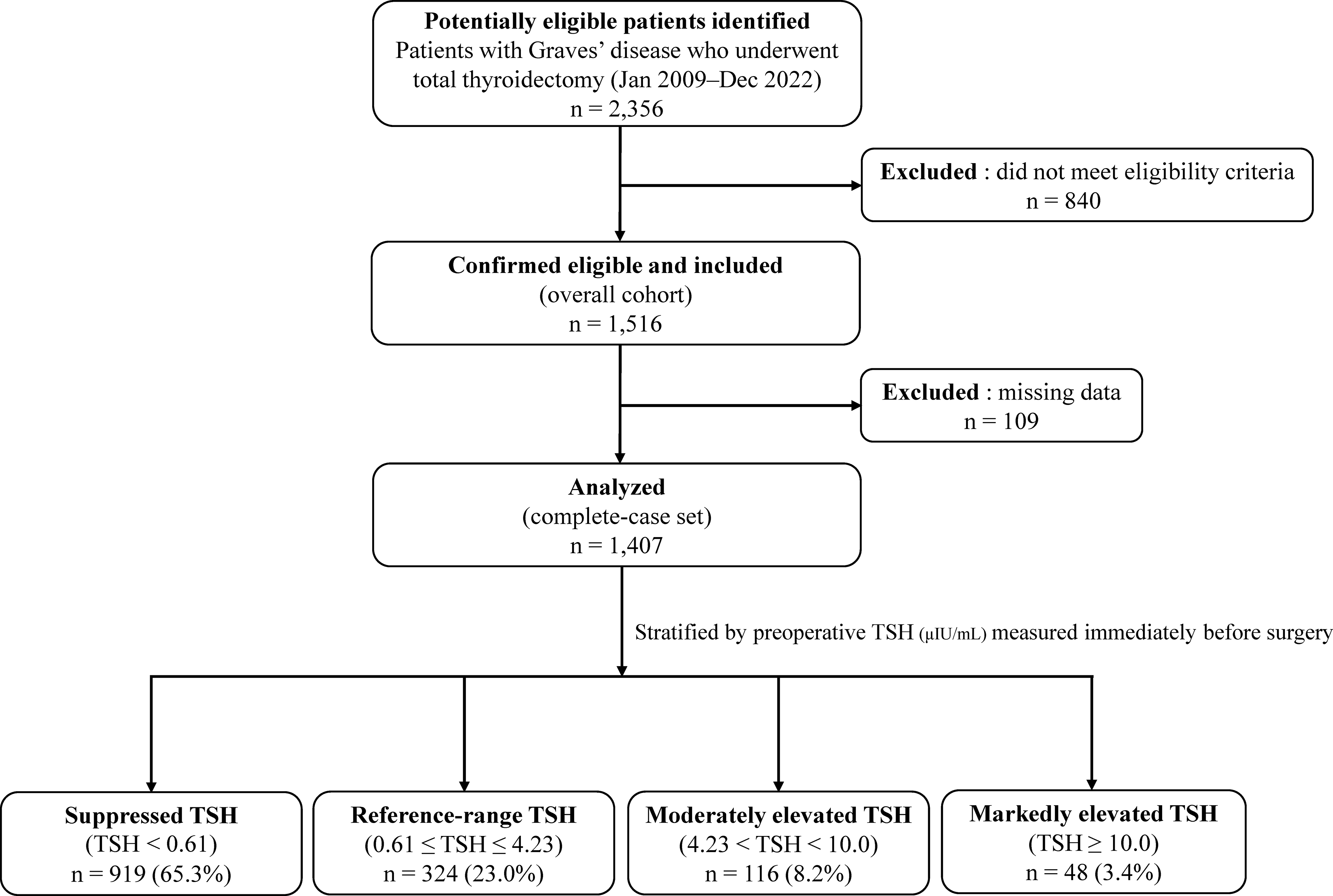
Study flow and analytic cohorts. Of 2356 patients with Graves’ disease who underwent total thyroidectomy between January 2009 and December 2022, 840 were excluded. To avoid double counting, each patient was assigned one primary reason for exclusion: <12 months of postoperative follow-up at our institution (n = 589), concomitant thyroid cancer (n = 159), reoperation (n = 47), concomitant hyperparathyroidism (n = 35), or prior radioiodine therapy (n = 10). Therefore, 1516 patients comprised the overall cohort. For prespecified analyses, 109 patients with missing data were excluded, yielding a complete case-cohort of 1407. The complete case-cohort was stratified by TSH measured immediately before surgery: <0.61 μIU/mL (n = 919; 65.3%); 0.61–4.23 μIU/mL (n = 324; 23.0%); 4.23 to < 10.0 μIU/mL (n = 116, 8.2%); and ≥ 10.0 μIU/mL (n = 48; 3.4%). GD, Graves’ disease; TSH, thyroid-stimulating hormone.
Thyroid function assays transitioned in January 2019; therefore, institutional validation supported pooling of TSH and free triiodothyronine (FT3) results across the study period (Supplementary Fig. S1). TSH values below the lower limit of quantification (0.005 μIU/mL) were set to 0.005 μIU/mL. TRAb levels (M22) were measured using a third-generation ECLIA (Roche, Indianapolis, IN, USA) and truncated at 400 IU/L when the values were above the upper reportable limit after dilution. The institutional reference range for free thyroxine (FT4) was 0.9–1.7 ng/dL. Among patients with preoperative TSH ≥ 10.0 μIU/mL, overt hypothyroidism and subclinical hypothyroidism were defined as FT4 < 0.9 ng/dL and FT4 within the reference range, respectively.
In the primary analysis, preoperative TSH was treated as a binary exposure using the prespecified threshold of ≥10.0 μIU/mL as a practical proxy for sustained high TSH exposure. To address heterogeneity within the TSH <10.0 μIU/mL category and align with the institutional reference range (0.61–4.23 μIU/mL), we modeled TSH as the following four categories: <0.61, 0.61–4.23 (reference), 4.23 to <10.0, and ≥10.0 μIU/mL. These categories were used in adjusted multivariable models for continuous and binary outcomes. The prespecified contrast of interest was ≥10.0 μIU/mL category.
Preoperative endocrine therapy was individualized by the treating endocrinologists and adjusted based on the preoperative results of serial thyroid function tests and assessments. Antithyroid drugs (methimazole or propylthiouracil) were titrated for biochemical control. KI was often introduced in the late preoperative period. Glucocorticoids were used occasionally as adjunctive therapy when control remained difficult. Thyroid function was monitored regularly during outpatient management (at least every 3 months). Preoperative KI initiated within 1 month, levothyroxine (LT4) coadministration, and glucocorticoid use were considered binary variables.
Preoperative thyroid weights were estimated using ultrasonography and the following ellipsoid formula with an institutional calibration constant (0.70) and derived from comparisons between ultrasound estimates and resected specimen weights:

Preadmission and preoperative measurements were obtained. The ER was defined using the following equation to capture clinically relevant interval changes based on preadmission parameters:

All comparisons and multivariable analyses used a complete case-cohort approach (listwise deletion). Imputation was not performed. The analytic cohort comprised 1407 patients (TSH ≥ 10.0 μIU/mL group, n = 48; TSH <10.0 μIU/mL group, n = 1359) with available preoperative thyroid function test results (TSH, FT3, FT4), TRAb values, prespecified clinical covariates, and operative/perioperative data.
Prespecified dichotomies were male sex, aged ≥40 years, body mass index (BMI) ≥25 kg/m2, resected thyroid weight ≥100 g, TRAb ≥100 IU/L, FT3 ≥4.0 pg/mL, KI initiated within 1 month, blood loss ≥200 mL, ER ≥1.1, and operative time ≥120 minutes. The surgeon category (trainee <5 years vs. staff ≥5 years) was included as a covariate. Cutoff values were prespecified. An ER ≥1.1 was considered pragmatic, and KI exposure was binary because the dose and duration were unavailable.
Outcomes
Primary outcomes were intraoperative blood loss, ER, and operative time. For dichotomous analyses, ER ≥1.1 was used as a pragmatic prespecified threshold to enhance clinical interpretability and align with the observed distribution. Secondary outcomes were resected thyroid weight and perioperative complications such as permanent vocal cord paralysis (defined as no recovery based on laryngoscopy results within 12 months) and permanent hypoparathyroidism (defined as the continued need for active vitamin D or calcium supplementation to maintain normocalcemia >12 months postoperatively).
Statistical analysis
Continuous variables were compared using Mann–Whitney U (two groups) or Kruskal–Wallis (four TSH categories) tests. Categorical variables were assessed using χ2 or Fisher’s exact tests. Continuous variables are reported as the median (interquartile range [IQR]) unless otherwise specified.
All multivariable analyses used complete case-cohort data (listwise deletion; no imputation). Multivariable linear regression was used for continuous outcomes (blood loss, ER, and operative time). Logistic regression was used for prespecified dichotomies and adjusted for prespecified covariates (male sex, aged ≥40 years, BMI ≥25 kg/m2, resected thyroid weight ≥100 g, TRAb ≥100 IU/L, FT3 ≥4.0 pg/mL, KI ≤1 month, and surgeon category [trainee vs. staff]).
To continuously model TSH, we fitted adjusted linear models with restricted cubic splines for log-TSH for each primary outcome and plotted adjusted means (95% confidence intervals [CIs]) with reference lines at the institutional lower limit of normal (0.61 μIU/mL), upper limit of normal (4.23 μIU/mL), and 10.0 μIU/mL. Exploratory receiver-operating characteristic analyses compared prespecified and clinically plausible thresholds (TSH levels ≥7.0, ≥8.0, and ≥10.0 μIU/mL) for ER ≥1.1 to assess robustness rather than define an optimal cutoff value.
Rare outcomes including permanent vocal cord paralysis, permanent hypoparathyroidism, and reoperation for hematoma were modeled using Firth’s bias-reduced logistic regression. These results are reported as adjusted odds ratios (aORs) and 95% CIs; p values were determined based on Wald tests. The overall association of categorical TSH (degrees of freedom = 3) was evaluated using a penalized likelihood ratio test. 16 In prespecified models with TSH ≥10.0 μIU/mL as the dependent variable (including KI ≤1 month), FT3 ≥4.0 pg/mL was excluded because of complete separation.
For supportive dichotomized analyses, operative time ≥ 120 minutes, blood loss ≥ 200 mL, and ER ≥ 1.1 were prespecified based on prior literature and cohort distributions.17–19 In the complete case-cohort set, these corresponded to the upper 36.2% (63.8th percentile), 11.2% (88.8th percentile), and 35.4% (64.6th percentile) of patients, respectively. The primary analysis continuously modeled outcomes. We assessed residual diagnostics, applied HC3 standard errors when necessary, checked multicollinearity (variance inflation factor <5) and influence (Cook’s distance >4/n), and used two-sided p < 0.05. Analyses were conducted using StatFlex version 7.0 (Artec, Osaka, Japan) and R version 4.5.1 (R Core Team 2025; R Foundation for Statistical Computing, Vienna, Austria) with the logistf package (version 1.26.1).
Results
Baseline characteristics of the overall cohort (n = 1516) are summarized in Table 1.
Clinical Characteristics and Surgical Data of Patients Undergoing Total Thyroidectomy for Graves’ Disease (Overall Cohort, n = 1516)
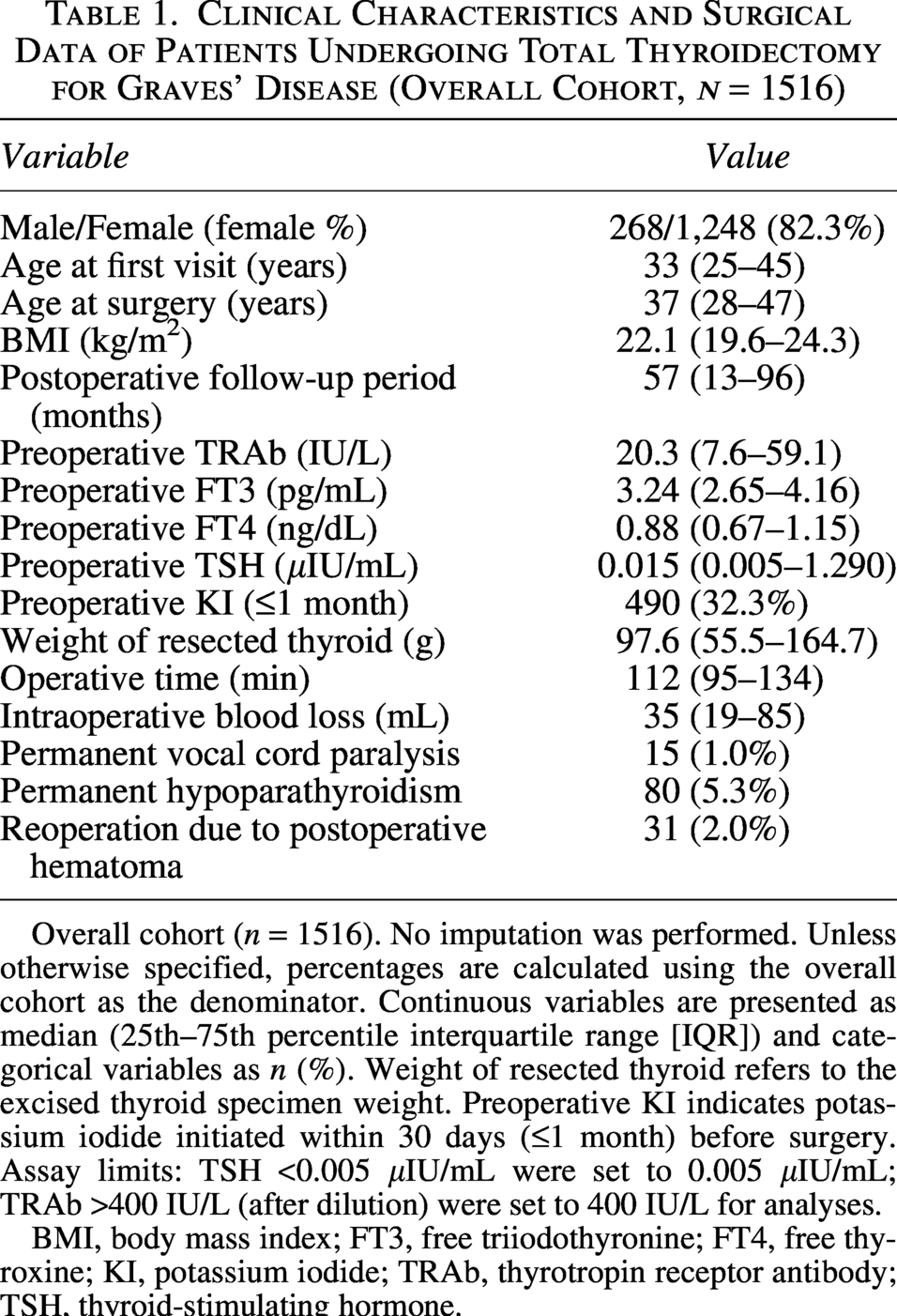
Overall cohort (n = 1516). No imputation was performed. Unless otherwise specified, percentages are calculated using the overall cohort as the denominator. Continuous variables are presented as median (25th–75th percentile interquartile range [IQR]) and categorical variables as n (%). Weight of resected thyroid refers to the excised thyroid specimen weight. Preoperative KI indicates potassium iodide initiated within 30 days (≤1 month) before surgery. Assay limits: TSH <0.005 μIU/mL were set to 0.005 μIU/mL; TRAb >400 IU/L (after dilution) were set to 400 IU/L for analyses.
BMI, body mass index; FT3, free triiodothyronine; FT4, free thyroxine; KI, potassium iodide; TRAb, thyrotropin receptor antibody; TSH, thyroid-stimulating hormone.
Analyses comprised a complete case-cohort design. For adjusted categorical analyses, patients were also stratified into four preoperative TSH categories based on the institutional reference range.
Preadmission TSH was higher in the TSH ≥10.0 group than in the TSH <10.0 group (median: 2.25 vs. 0.006 μIU/mL; p < 0.001) (Table 2). Additionally, preadmission TSH ≥10.0 μIU/mL was more frequent in the TSH ≥10.0 group than in the TSH <10.0 group (20.8% vs. 3.2%). Among patients with preoperative TSH ≥10.0 μIU/mL, most (45/48; 93.8%) had overt hypothyroidism (FT4 below the lower limit of normal), and only a few (3/48; 6.3%) had FT4 within the reference range.
Comparison of Clinical and Surgical Characteristics Between Patients With Preoperative TSH ≥10.0 μIU/mL and Those With TSH <10.0 μIU/mL
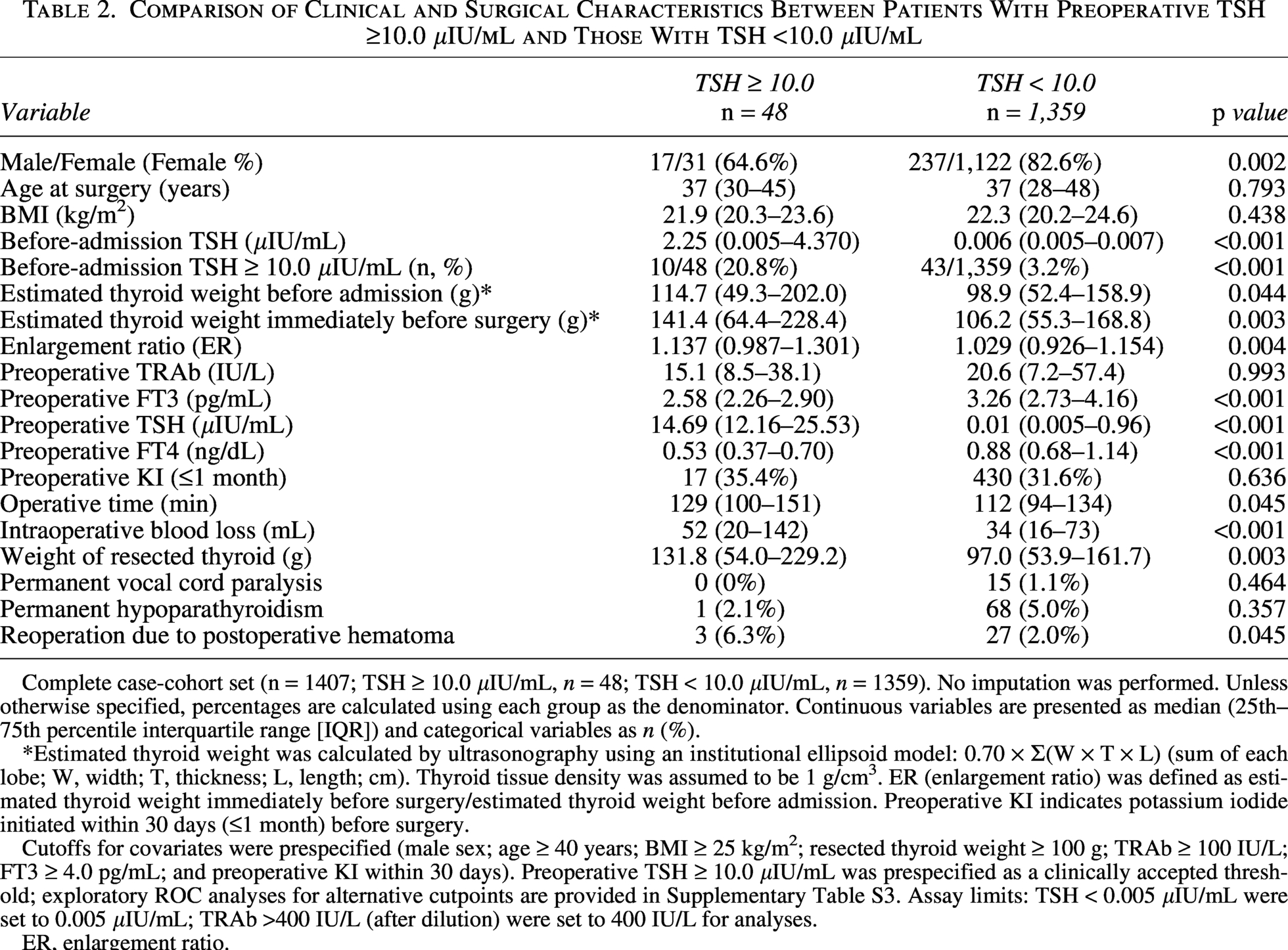
Complete case-cohort set (n = 1407; TSH ≥ 10.0 μIU/mL, n = 48; TSH < 10.0 μIU/mL, n = 1359). No imputation was performed. Unless otherwise specified, percentages are calculated using each group as the denominator. Continuous variables are presented as median (25th–75th percentile interquartile range [IQR]) and categorical variables as n (%).
*Estimated thyroid weight was calculated by ultrasonography using an institutional ellipsoid model: 0.70 × Σ(W × T × L) (sum of each lobe; W, width; T, thickness; L, length; cm). Thyroid tissue density was assumed to be 1 g/cm³. ER (enlargement ratio) was defined as estimated thyroid weight immediately before surgery/estimated thyroid weight before admission. Preoperative KI indicates potassium iodide initiated within 30 days (≤1 month) before surgery.
Cutoffs for covariates were prespecified (male sex; age ≥ 40 years; BMI ≥ 25 kg/m²; resected thyroid weight ≥ 100 g; TRAb ≥ 100 IU/L; FT3 ≥ 4.0 pg/mL; and preoperative KI within 30 days). Preoperative TSH ≥ 10.0 μIU/mL was prespecified as a clinically accepted threshold; exploratory ROC analyses for alternative cutpoints are provided in Supplementary Table S3. Assay limits: TSH < 0.005 μIU/mL were set to 0.005 μIU/mL; TRAb >400 IU/L (after dilution) were set to 400 IU/L for analyses.
ER, enlargement ratio.
To clarify the timing of the preadmission assessment, the median interval between the last preadmission blood test and the preoperative test was 19 days (IQR: 13–29; range: 1–91) for 1407 patients. When stratified into four TSH categories (<0.61, 0.61–4.23, 4.23 to <10.0, and ≥10.0 μIU/mL), the corresponding median intervals were 17 days (IQR: 12–28; range: 1–90), 24 days (IQR: 17–32; range: 1–91), 19 days (IQR: 14–31; range: 4–86), and 18 days (IQR: 13–32; range: 5–71), respectively. A significant difference was observed among groups (Kruskal–Wallis test, p < 0.001). This timing indicated that preadmission outpatient thyroid function monitoring was generally performed within a clinically acceptable timeframe. Among 1407 patients, 372 (26.4%) received LT4 co-administration during antithyroid drug treatment, and the frequency increased across TSH categories (20.7%, 37.1%, 39.1%, and 47.9%, respectively; p < 0.001). Preoperative glucocorticoids were administered to 51 (3.6%) of 1,407 patients and also differed across TSH categories (5.0%, 0.4%, 0.9%, and 2.1% for TSH < 0.61, 0.61–4.23, 4.23 to <10.0, and ≥10.0 μIU/mL, respectively; p = 0.002).
Compared with the TSH <10.0 μIU/mL group, the TSH ≥10.0 μIU/mL group had higher ERs (p = 0.004), longer operative times (p = 0.045), greater blood loss (p < 0.001), and heavier resected thyroid weights (p = 0.003). The TSH ≥ 10.0 μIU/mL group also included fewer female patients (p = 0.002) and more cases of reoperation for postoperative hematoma (3/48 vs. 27/1359; p = 0.045). No significant differences in permanent vocal cord paralysis or permanent hypoparathyroidism were observed (Table 2). Box plots for ER and blood loss are shown in Supplementary Figure S2.
After adjustment (Table 3), categorical TSH (reference: 0.61–4.23 μIU/mL) indicated that TSH ≥ 10.0 μIU/mL was independently associated with greater blood loss (β = 58.31 mL; 95% CI: 28.11–88.52; p < 0.001) and higher ERs (β = 0.14; 95% CI: 0.06–0.22; p < 0.001), but not with operative time (β = 7.49 minutes; p = 0.121). Intermediate TSH strata were not significant for blood loss or ER (Table 3 and Fig. 2). Restricted cubic spline analyses further illustrated these associations across the TSH spectrum (Fig. 3). Preoperative KI initiated within 1 month was not independently associated with blood loss, ER, or operative time (Table 3).
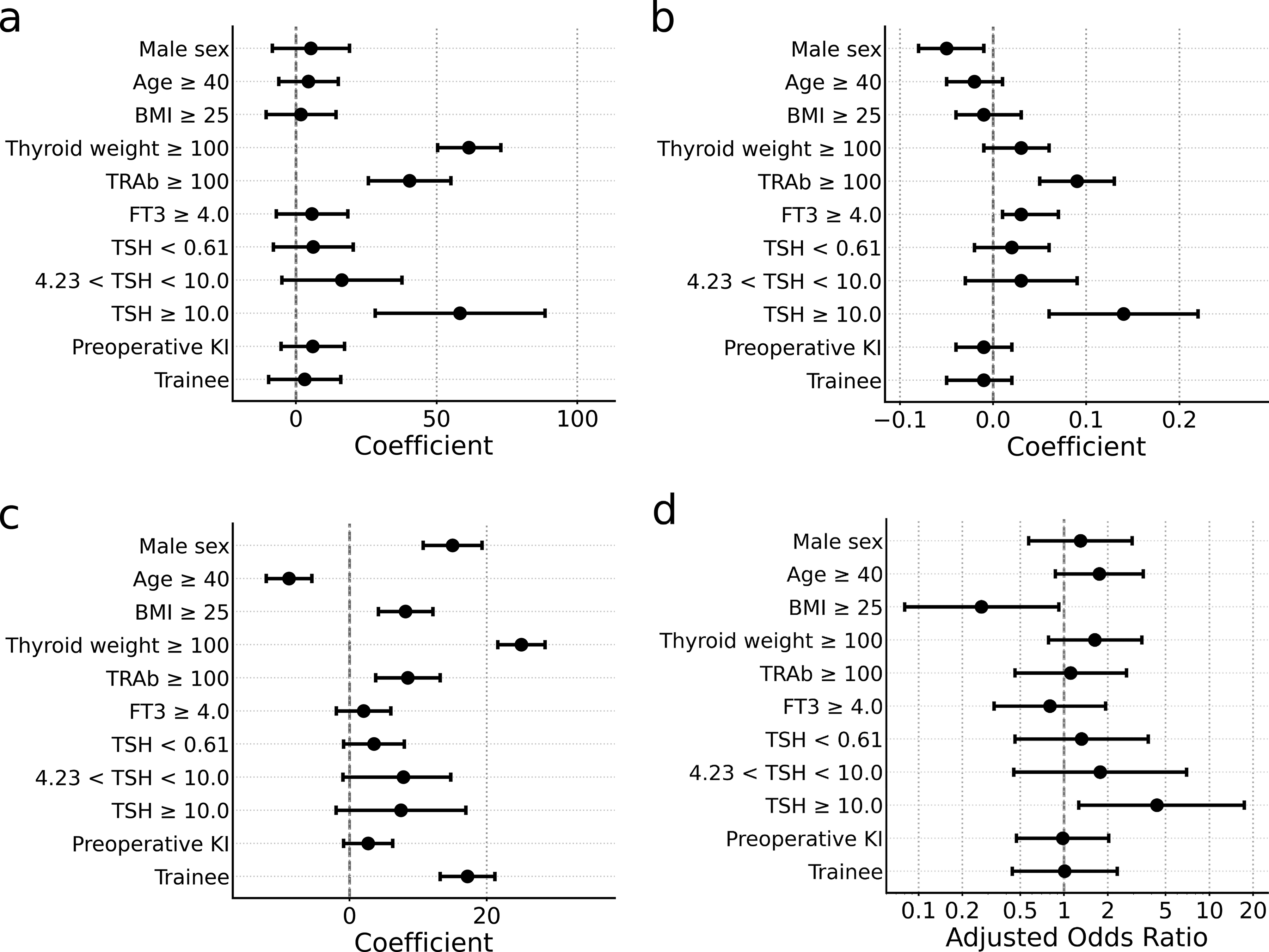
Coefficient plots from prespecified multivariable models in the complete case-cohort set (n = 1407). Adjusted β coefficients (95% CIs) from linear regression for
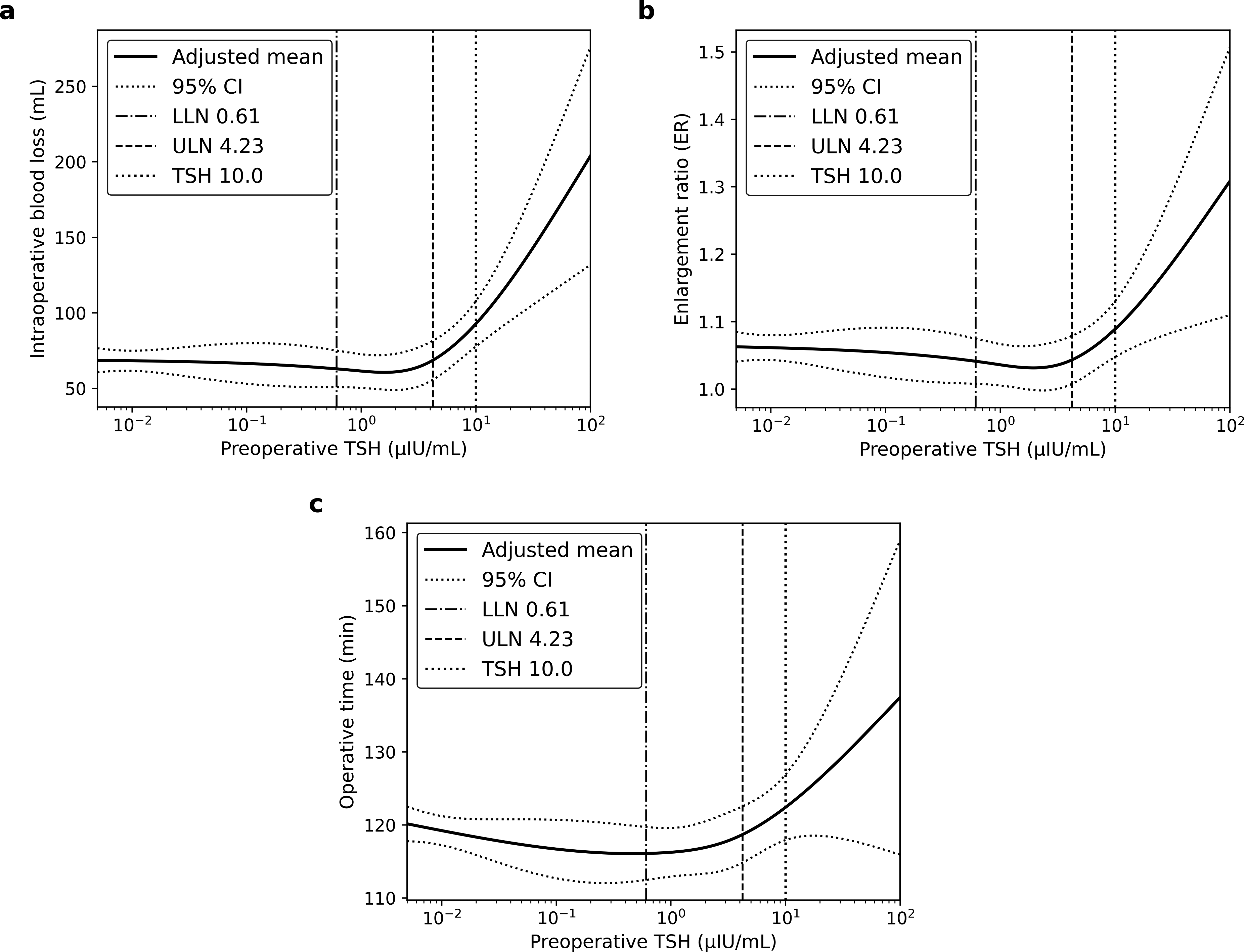
Adjusted restricted cubic spline curves illustrate the relationship between preoperative TSH and
Multivariable Linear Regression Analysis of Preoperative TSH Categories and Continuous Surgical Outcomes
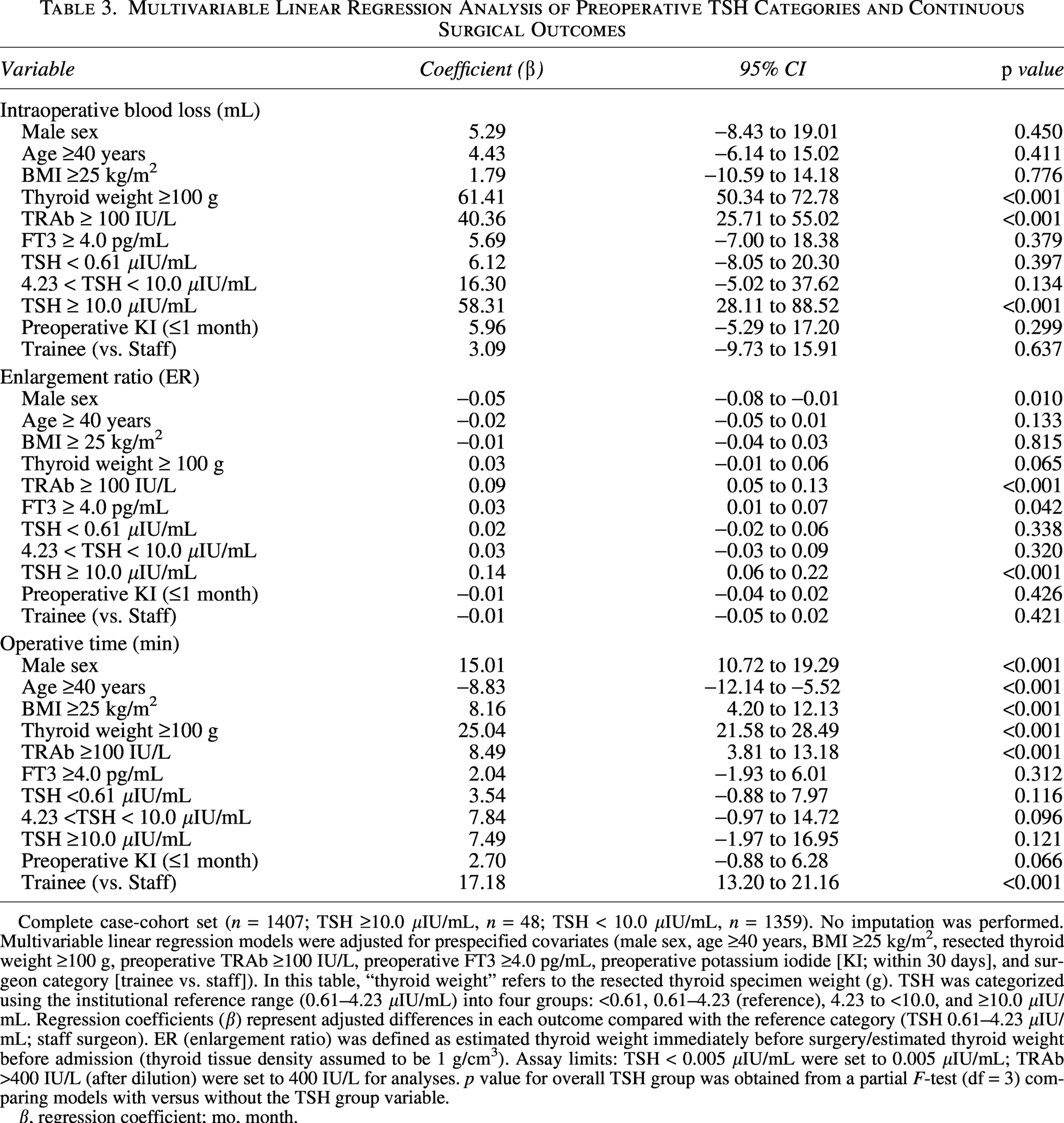
Complete case-cohort set (n = 1407; TSH ≥10.0 μIU/mL, n = 48; TSH < 10.0 μIU/mL, n = 1359). No imputation was performed. Multivariable linear regression models were adjusted for prespecified covariates (male sex, age ≥40 years, BMI ≥25 kg/m², resected thyroid weight ≥100 g, preoperative TRAb ≥100 IU/L, preoperative FT3 ≥4.0 pg/mL, preoperative potassium iodide [KI; within 30 days], and surgeon category [trainee vs. staff]). In this table, “thyroid weight” refers to the resected thyroid specimen weight (g). TSH was categorized using the institutional reference range (0.61–4.23 μIU/mL) into four groups: <0.61, 0.61–4.23 (reference), 4.23 to <10.0, and ≥10.0 μIU/mL. Regression coefficients (β) represent adjusted differences in each outcome compared with the reference category (TSH 0.61–4.23 μIU/mL; staff surgeon). ER (enlargement ratio) was defined as estimated thyroid weight immediately before surgery/estimated thyroid weight before admission (thyroid tissue density assumed to be 1 g/cm³). Assay limits: TSH < 0.005 μIU/mL were set to 0.005 μIU/mL; TRAb >400 IU/L (after dilution) were set to 400 IU/L for analyses. p value for overall TSH group was obtained from a partial F-test (df = 3) comparing models with versus without the TSH group variable.
β, regression coefficient; mo, month.
In multivariable logistic models, preoperative TSH ≥10.0 μIU/mL was independently associated with ER ≥1.1 (aOR: 2.60; 95% CI: 1.37–4.97; p = 0.004), blood loss ≥200 mL (aOR: 5.18; 95% CI: 1.77–15.19; p = 0.002), and operative time ≥ 120 minutes (aOR: 2.29; 95% CI: 1.16–4.54; p = 0.018) (Supplementary Table S1). In rare event models, TSH ≥ 10.0 μIU/mL was also associated with reoperation for postoperative hematoma (aOR: 4.35; 95% CI: 1.26–17.37; p = 0.043) (Table 4). TSH ≥10.0 μIU/mL was not associated with permanent vocal cord paralysis or permanent hypoparathyroidism. Resected thyroid weight ≥100 g predicted permanent hypoparathyroidism (aOR: 1.80; 95% CI: 1.08–3.00; p = 0.024) and TRAb ≥100 IU/L predicted permanent vocal cord paralysis (aOR: 2.82; 95% CI: 1.04–7.64; p = 0.041) (Table 4).
Multivariable Analysis of Preoperative TSH Categories and Binary Surgical Outcomes Using Firth’s Bias-Reduced Logistic Regression
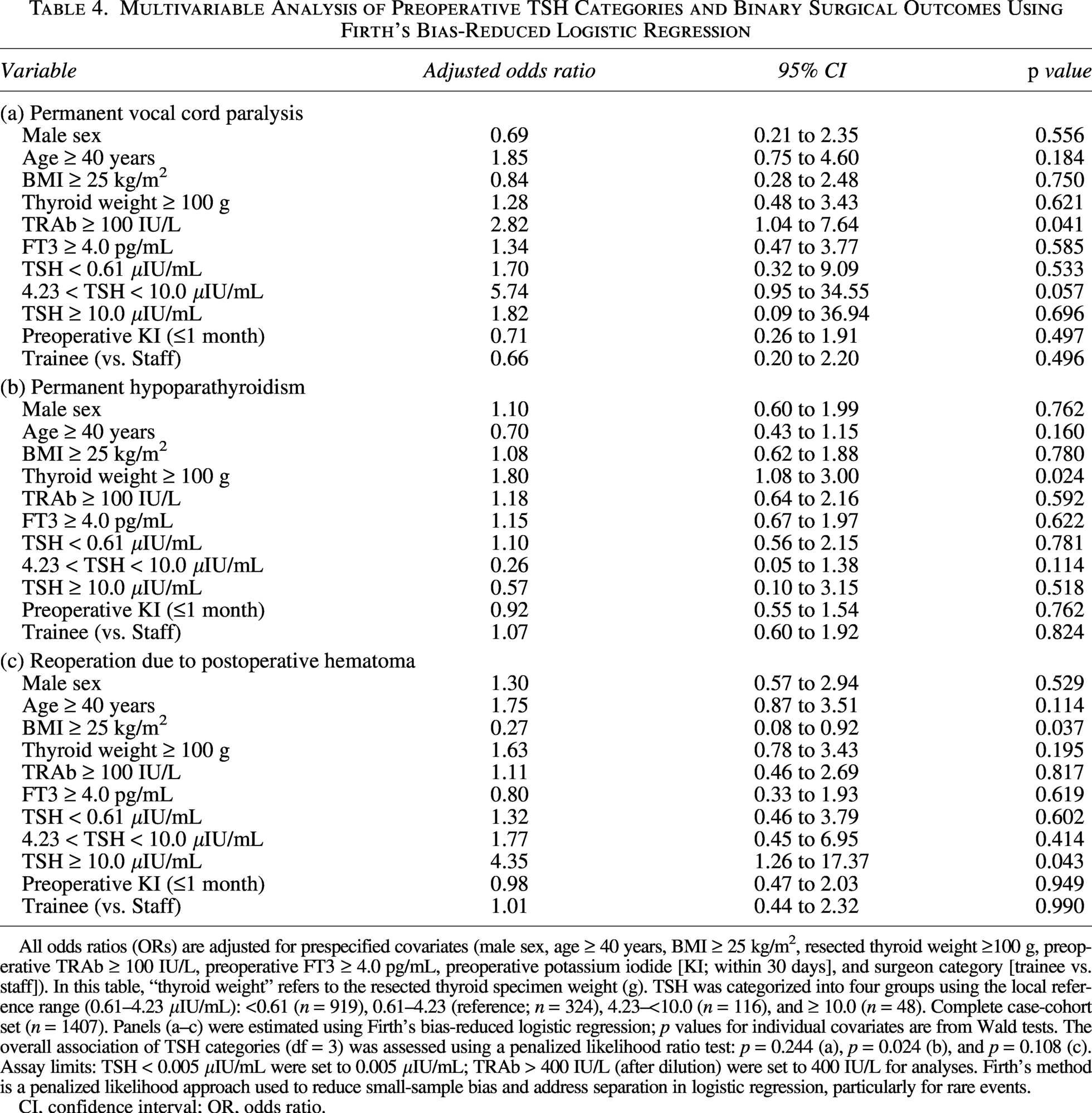
All odds ratios (ORs) are adjusted for prespecified covariates (male sex, age ≥ 40 years, BMI ≥ 25 kg/m², resected thyroid weight ≥100 g, preoperative TRAb ≥ 100 IU/L, preoperative FT3 ≥ 4.0 pg/mL, preoperative potassium iodide [KI; within 30 days], and surgeon category [trainee vs. staff]). In this table, “thyroid weight” refers to the resected thyroid specimen weight (g). TSH was categorized into four groups using the local reference range (0.61–4.23 μIU/mL): <0.61 (n = 919), 0.61–4.23 (reference; n = 324), 4.23–<10.0 (n = 116), and ≥ 10.0 (n = 48). Complete case-cohort set (n = 1407). Panels (a–c) were estimated using Firth’s bias-reduced logistic regression; p values for individual covariates are from Wald tests. The overall association of TSH categories (df = 3) was assessed using a penalized likelihood ratio test: p = 0.244 (a), p = 0.024 (b), and p = 0.108 (c). Assay limits: TSH < 0.005 μIU/mL were set to 0.005 μIU/mL; TRAb > 400 IU/L (after dilution) were set to 400 IU/L for analyses. Firth’s method is a penalized likelihood approach used to reduce small-sample bias and address separation in logistic regression, particularly for rare events.
CI, confidence interval; OR, odds ratio.
Male sex was independently associated with TSH ≥ 10.0 μIU/mL (aOR: 2.47; 95% CI: 1.30–4.71; p = 0.006), whereas preoperative KI (≤1 month) was not (aOR: 0.99; 95% CI: 0.53–1.83; p = 0.962) (Supplementary Table S2).
In receiver-operating characteristic analyses of ER ≥1.1, candidate TSH thresholds showed high specificity and low sensitivity (e.g., sensitivity of 0.050 and specificity of 0.975 at TSH ≥10.0 μIU/mL), with only minimal differences in the Youden index (Supplementary Table S3). The Youden index was highest at a TSH threshold of approximately 7 μIU/mL.
Discussion
In this study, marked preoperative TSH elevation (≥10.0 μIU/mL) was associated with increased operative difficulty during total thyroidectomy for GD. After multivariable adjustment, TSH ≥10.0 remained independently associated with greater intraoperative blood loss and higher ER, whereas the association with operative time was not statistically significant. Consistent results of dichotomized analyses (ER ≥1.1, blood loss ≥200 mL, and operative time ≥120 minutes) and rare event models were observed, indicating an association with reoperation for postoperative hematoma (Table 4; Fig. 2d). Because of the low number of hematoma reoperations and wide CIs, including an unexpected inverse association of BMI ≥25 kg/m2, these findings should be interpreted cautiously and considered hypothesis-generating. Confirmation by independent cohort studies is warranted.
From a clinical perspective, elevated preoperative TSH is unlikely to be a transient perioperative fluctuation; rather, it may represent a phenotype of sustained TSH elevation arising during outpatient antithyroid drug titration despite clinically appropriate biochemical monitoring. This interpretation is consistent with the observed associations between TSH elevation, ER, and intraoperative blood loss.
In the complete case-cohort, LT4 coadministration increased across the four preoperative TSH categories, consistent with dynamic physician-directed adjustments in response to thyroid function. Because details regarding regimens and doses (e.g., block and replace vs. temporary supplementation) were not uniformly retrievable, we could not distinguish treatment strategies. Preoperative glucocorticoids were used infrequently but differed across TSH categories, likely reflecting selective use for refractory cases. Collectively, these patterns underscore that inadvertent TSH overshoot can occur in real-world practice despite structured monitoring and individualized adjustment.
The interval between preadmission and preoperative measurements of TSH levels was generally clinically acceptable, thus arguing against unduly remote preadmission measurements as the primary explanation for marked preoperative TSH elevation. Instead, preadmission TSH was high, and preadmission TSH ≥10.0 μIU/mL was more frequent in the TSH ≥10.0 group, indicating that many patients had TSH elevation earlier during the preoperative preparation period.
Prior reviews have focused on goiter size and patient factors as determinants of bleeding and technical difficulty19–25 but have not evaluated TSH as a preoperative marker. By testing a familiar threshold (≥10.0 μIU/mL) and demonstrating independence from major covariates, we suggest that TSH provides additional information regarding operative conditions. The inclusion of preadmission TSH further supports the concept that earlier elevation (or a sharp increase) may precede interval enlargement (higher ER) and greater blood loss near the time of surgery, emphasizing the value of considering perioperative TSH dynamics rather than a single time point. Although the Youden index was highest at a TSH threshold of approximately 7 μIU/mL, the differences among thresholds of 7, 8, and 10 μIU/mL were minimal. Therefore, we retained the clinically pragmatic cutoff of ≥10.0 μIU/mL for the primary analyses. These findings suggest that even moderately elevated TSH levels may influence operative conditions, highlighting the importance of careful preoperative thyroid function management. Further studies are warranted to determine the optimal TSH threshold for perioperative risk stratification. In the present study, TSH ≥10.0 μIU/mL was used as a pragmatic threshold for elevated TSH, whereas overt and subclinical hypothyroidism were defined based on FT4 levels to ensure consistency with established clinical definitions.
TSH can stimulate follicular cell proliferation and vascular endothelial growth factor-mediated angiogenesis, plausibly linking hypervascularity and interstitial edema to a more hemorrhagic and bulky operative field in patients with GD. The higher blood loss and ER observed with TSH ≥10.0 are consistent with this pathway.10–12,26,27
Our results implied that tracking TSH trends during the preoperative period may identify patients who develop marked TSH elevation (≥10.0 μIU/mL), potentially indicating overtreatment. Clinicians should be cautious about the rapid escalation of antithyroid drugs and extended iodine use in cases that are difficult to control because they may inadvertently precipitate iatrogenic hypothyroidism and TSH overshoot. Additionally, when TSH remains ≥10.0 μIU/mL, the surgical team may anticipate greater hemostatic demands and gland bulk during planning and briefing, thus making this threshold a simple adjunct for perioperative risk communication.28–30 Male sex was independently associated with preoperative TSH ≥10.0 μIU/mL (Supplementary Table S2); however, whether this reflects management-related factors is unclear.
This study had some limitations. Residual confounding and selection bias were possible despite prespecified adjustments. Longitudinal data regarding medication dosing and serial TSH measurements were not uniformly available; in particular, the intent and dosing strategy of LT4 coadministration could not be comprehensively ascertained. Detailed regimen details regarding antithyroid drugs and KI (including treatment days and cumulative dose within 1 month) were not uniformly retrievable. Accordingly, LT4 coadministration and glucocorticoid exposure were modeled as binary variables, and we assumed that the single preoperative TSH value reasonably reflected prior sustained exposure. Ultrasound-based thyroid weight estimates may have included measurement errors despite standardized acquisition and the use of a locally calibrated model. Assay transitions were validated and censoring rules were applied consistently; however, minor systematic differences cannot be fully excluded. Analyses relied on complete case-cohort data without imputation, which may bias results if missingness was not random. Prespecified dichotomization improved clinical usefulness but reduced details and may have misclassified values near thresholds; additionally, receiver-operating characteristic analyses showed limited discrimination of TSH alone, suggesting that TSH is a risk marker rather than a stand-alone screening test (Supplementary Table S3). For rare outcomes, statistical power was limited despite Firth’s correction. Finally, generalizability may have been constrained by the single-center context and standardized surgical techniques.
Conclusion
Preoperative TSH ≥ 10.0 μIU/mL was independently associated with greater intraoperative blood loss and higher ER during total thyroidectomy for GD. Avoiding iatrogenic hypothyroidism and sustained TSH elevation during preoperative titration may improve operative conditions. Prospective multicenter studies are necessary to confirm our findings and clarify causality.
Authors’ Contributions
T.S.: Conceptualization (lead), methodology (lead), formal analysis (lead), writing—original draft (lead), writing—review and editing (equal), and case collection (equal). M.K.: Methodology (equal); supervision (lead), writing—review and editing (equal), and case collection (equal). M.F.: Data curation (lead); writing—review and editing (equal); case collection (equal). H.M.: Writing—review and editing (equal) and case collection (equal). T.H.: Writing—review and editing (equal) and case collection (equal). Y.I.: Writing—review and editing (equal) and case collection (equal). Akihiro M.: Writing—review and editing (equal); case collection (equal). Akira M.: Supervision (equal); writing—review and editing (equal); case collection (equal). T.A.: Writing—review and editing (equal) and endocrinological guidance (lead).
Footnotes
Acknowledgments
The authors would like to thank the clinical staff at Kuma Hospital for their invaluable assistance with patient care and data collection. The authors are especially grateful to Makoto Kawakami for his support with data extraction. The authors also acknowledge the laboratory team for their dedicated quality assurance and performance of thyroid function testing and other relevant laboratory measurements throughout the study period.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
The authors received no financial support for this study.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.