
Abstract
Background
Healthcare professionals in specialist palliative care have a key role in conducting end-of-life care discussions with patients and their family caregivers. We aimed to identify key barriers and facilitators for healthcare professionals in specialist palliative care to support patients and their family caregivers in decision-making for patient end-of-life care.
Methods
Twenty-two healthcare professionals from different healthcare professions were recruited from a large regional specialist palliative care service in Ireland comprising 2 hospice sites. Five focus groups were conducted with participants. Data were member checked and analyzed using thematic analysis.
Results
Open communication and trusting relationships with patients and family caregivers combined with sufficient time for early and phased exploration of the patient’s preferences for end-of-life care, were key facilitators for participants. Family caregivers keeping information from the patient, family misunderstanding about who is responsible for decision-making, and a lack of involvement of other specialties in end-of-life care discussions were perceived by participants as key barriers. Although participants indicated they had sufficient expertise to support patients in end-of-life care decision-making, they felt that end-of-life care discussions were not solely the responsibility of specialist palliative care services.
Conclusion
Open communication with patients in end-of-life care decision-making can be of central importance for healthcare professionals in specialist palliative care. Further research is needed to understand the role of healthcare professionals outside of specialist palliative care in end-of-life care discussions and decision-making.
Keywords
Introduction
Healthcare professionals in palliative care negotiate complex decisions with patients and family caregivers about patient end-of-life care. 1 Facilitating patients and their family caregivers in end-of-life discussions can have a positive effect on patient mental health and help family caregivers cope with bereavement. 2 A lack of information from healthcare professionals about end-of-life issues can make patients and family caregivers feel uncertain about end-of-life care.3,4
End-of-life care decisions that healthcare professionals typically advise patients and family caregivers about include for example, pharmacological interventions, artificial nutrition and hydration, cardiopulmonary resuscitation, transfer to acute and/or home care, and optimal timing of hospice care.5,6 Providing sufficient information to patients and family caregivers about specific interventions and understanding patients’ expressed wishes are of key importance. 7 Healthcare professionals also consider the effect of family caregivers on the decision-making process including family caregiver views on the patient’s expressed wishes. 8 The emotional impact of decision-making on both patient and family caregiver can be significant.9,10
Differences between patients’ and family caregivers’ approach to decision-making about patient end-of-life care 11 means that healthcare professionals need to be sensitive to the viewpoint of both the patient and family caregiver. Healthcare professionals themselves may differ from patients and family caregivers in terms of their preferences for patient end-of-life care. 12 We already know that healthcare professionals’ capacity to effectively facilitate patients and family caregivers in decision-making about end-of-life care can be constrained by their reluctance to discuss prognostic uncertainty. 13 Inadequate communication skills on the part of healthcare professionals, their personal convictions, and concerns they have about medicolegal repercussions of their communications with patients and family caregivers may also limit their ability to fully support the patient and family caregiver in decision-making about end-of-life care. 14 There may be other factors which limit healthcare professionals’ support to patients and family caregivers in end-of-life care decision-making. Evidence on the effectiveness of healthcare professionals in conducting end-of-life discussions is limited. 15
Specialist palliative care is understood as care provided by healthcare professionals whose core activity is providing palliative care including end-of-life care. We aimed to ascertain barriers and facilitators for healthcare professionals in specialist palliative care to support patients and family caregivers in the decision-making process for patient end-of-life care.
Methods
Study Design
We used a qualitative design16-18 because we were inductive in our approach to interpret participants’ viewpoint and we were focused on the meanings participants attached to their experiences. The Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist 19 was used while developing, conducting, and reporting this study.
Ethics Approval
The study was approved by the Research Ethics Committee of St. Francis Hospice, Ireland in February 2023 (reference no: 230 194), and by the School of Medicine Research Ethics Committee of Trinity College Dublin, Ireland in April 2023 (reference no: 2426). Written informed consent to participate in the study was provided by each participant.
Eligibility Criteria
The eligibility criteria for participants were that they were healthcare professionals working in specialist palliative care, had a minimum of 1 year’s clinical experience in specialist palliative care, and had direct patient and family caregiver contact in their practice. We set a criterion of minimum 1 year’s experience working in specialist palliative care so that participants would have sufficient experience working in the field.
Setting and Recruitment
Between August 2023 and April 2024, 22 healthcare professionals were recruited from a large regional specialist palliative care service in Ireland which comprises 2 hospice sites serving a population of approximately 700,000 people (circa 14% of the national population). The regional specialist palliative care service provides a mixture of inpatient, outpatient and day services, and community (ie, home-based) care. A letter of invitation was circulated to those who were eligible to participate by a non-healthcare professional who was not involved in the delivery of services. A recruitment poster was also displayed in common areas in the 2 hospice sites of the regional service.
Sampling and Participants
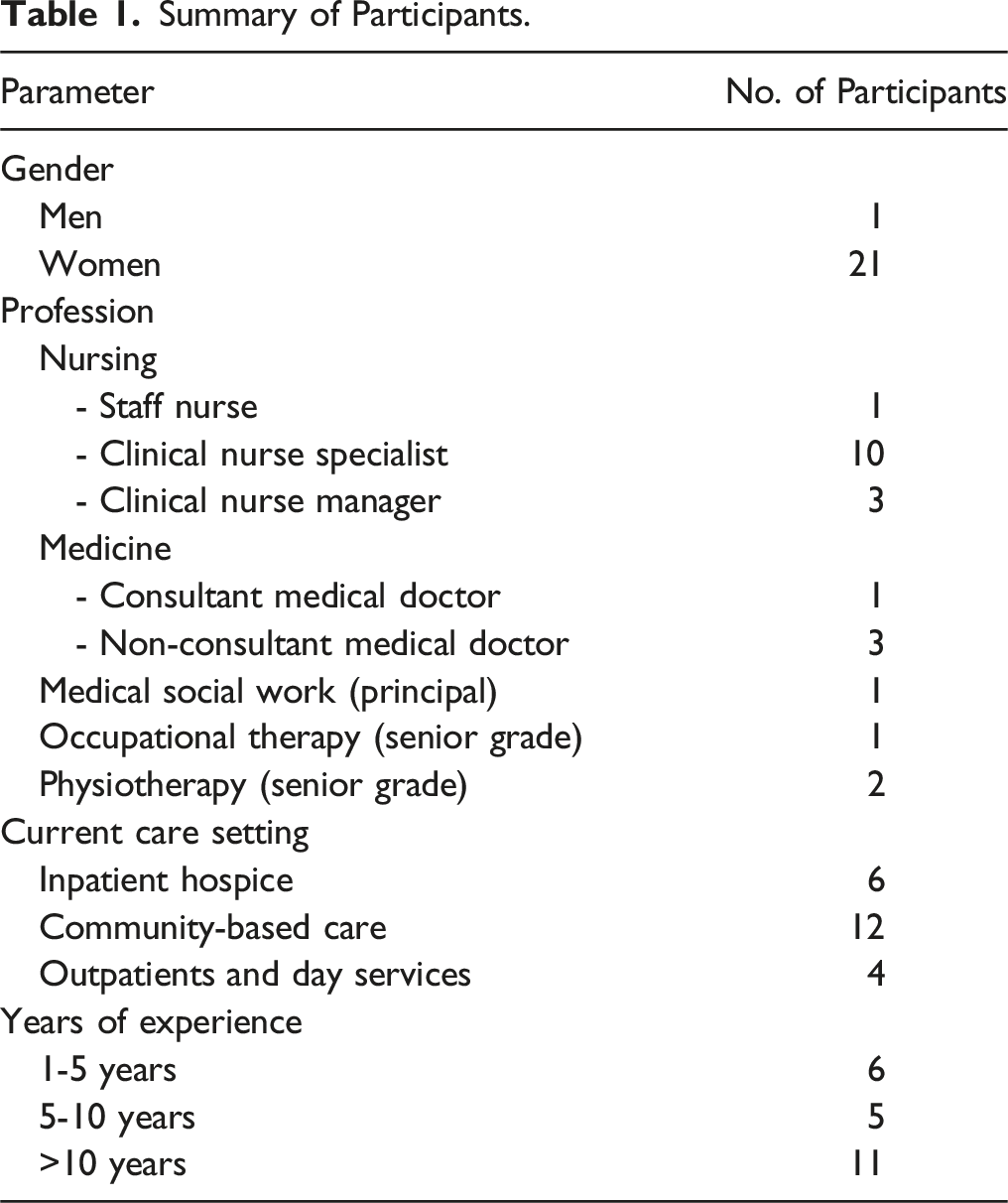
Participants were purposively sampled for variation in healthcare profession (eg, nursing, medical, and allied health professionals), care setting (eg, inpatient units, outpatients and day services, and community-based care), professional grade, and in amount of experience working in specialist palliative care. Thirteen healthcare professionals who had initially indicated interest to participate did not participate in the study citing time constraints.
Summary of Participants.
Data Collection
Focus Group-Based Questions.
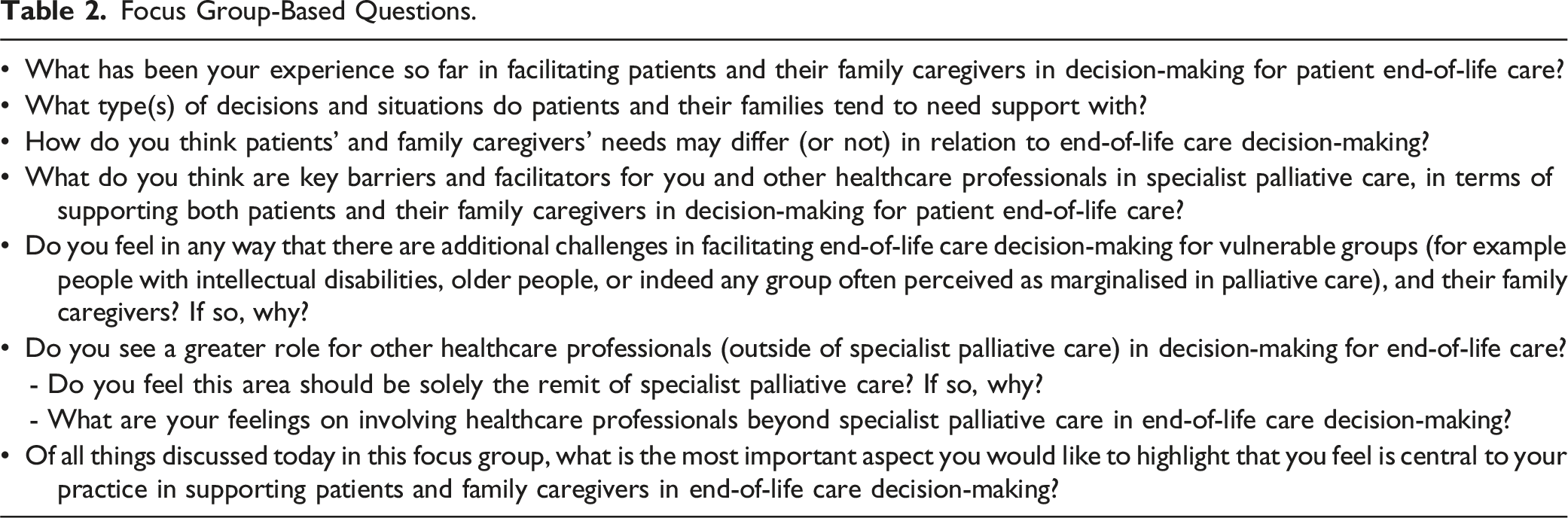
The focus groups were conducted by the first author. The third author took field notes in the first focus group. For all other focus groups, field notes were documented immediately after the focus group by the first author. The field notes were used to record similarities and anomalies between participants’ accounts in a focus group. Duration of focus groups ranged between 46 and 78 minutes, and the mean duration was 65 minutes. Four of the focus groups were conducted in-person. The remaining focus group was conducted using the video conferencing platform Zoom 22 to accommodate for a wide geographical location of participants. Participant member-checking 23 was performed by confirming the interviewer’s interpretation with participants during their focus group and by summarizing their contributions toward the end of their focus group.
All focus groups were digitally-audio recorded and transcribed verbatim. The transcripts were then pseudonymized in storage whereby any information that could identify a participant in a transcript was replaced with non-identifying descriptors. All procedures for data management including protection of participant confidentiality were fully compliant with General Data Protection Regulation (GDPR) (EU) 2016/679. All participant data were stored in encrypted files on a password-accessed computer which only the researchers had access to. The key that linked each participant’s real name to their pseudonym and data was stored in an encrypted file separate to the encrypted file containing their pseudonym and data.
Data Analysis
We analyzed the data using Braun and Clarke’s framework for thematic analysis.17,18 The first step involved reading and re-reading the focus group transcripts to be fully familiar with the data. The next step involved generating codes from each transcript and labelling them in a way that described the content of each code. Similar data were merged into the same code and similar codes were aggregated to form developing themes. We then refocused the analysis across the dataset at the level of developing themes rather than at the code level to ensure all relevant codes were coded appropriately to a developing theme. The final stage of analysis constituted a full description and refinement of each theme.17,18 We reached data saturation after analyzing data from 22 participants (ie, when data from the fifth focus group did not result in any significant new findings). Microsoft Excel was used as a tool to organize and manage the data during coding. Rigor in the analysis was ensured by the third author examining data coded by the first author at each stage of analysis and by their agreement on codes and themes.
Results
In this paper, we report themes which depict the main facilitators and barriers for participants in terms of supporting patients and family caregivers in decision-making for patient end-of-life care. The data extracts are tagged with a unique identifier with ‘P#’ indicating a participant and their number.
Key Facilitators
Relationship Building
Participants emphasized the importance of establishing a strong relationship with the patient and family caregiver. This they felt enabled them to understand what underpinned patients’ and family caregivers’ preferences: Working in the inpatient unit … we tend to get to build a nice relationship with the patient, with the family … and [then] have a very good sense of what their values are to try and help support them in decision-making. (P13, focus group 3)
Participants deemed that trusting relationships with patients and family caregivers were important to establish at an individual level because trust established at the micro-level could then benefit patients and family caregivers when interacting with the wider palliative care service. For example, P1 (focus group 1) commented: Trust and [then] the work has been put in place. And then they have a trust in not only the nurses but the service also.
Transparency in Communication. Participants valued transparency in communication with patients and their family caregivers: It’s our role to try to make sure that decisions that are made … are done with as much honest information [as possible]. (P8, focus group 2)
Participants felt that open communication gave patients an opportunity to make informed decisions about end-of-life care, even if participants themselves disagreed with their decisions. For instance, P18 (focus group 4) shared: It’s the informed decision. And that’s what we do well, make sure that it’s informed … even if we think it is a bit bonkers [unwise].
They also judged that open communication promoted cohesion in decision-making between the patient and family caregiver because it aided family caregivers to gain insight into the patient’s preferences for care: Very often we are having these conversations with patients when their family are there. I suppose because they are privy to that information at the time, and they can hear what’s been discussed, and they can hear what preferences their loved one has voiced. (P5, focus group 1)
Early Exploration of Care Preferences
There was general agreement among participants that early exploration of the patient’s preferences was beneficial because it enabled healthcare professionals to be clear about patients’ preferences: If you’ve done that spade work [identify care preferences], we know what their wishes are, that they want to die at home or in the hospice, or if they want to go to the hospital. (P2, focus group 1).
However, participants indicated that early exploration of patients’ preferences also needed to factor in the time required by patients to decide about care. In this respect, participants felt early discussion of care preferences necessitated phased interactions with patients and family caregivers: This might be, firstly, an information sharing opportunity, then providing time for the patient and the family or their appointed caregivers or appointed decision-makers to have time to do their own piece of research and to have discussion … and then maybe to have a follow up, that might be sometimes a more realistic way of approaching the situation. (P11, focus group 3)
Less Competing Needs in Specialist Palliative Care
Participants perceived that working solely in specialist palliative care enabled them to be effective in end-of-life discussions. They recognized that healthcare professionals outside of the specialist palliative care setting had additional and competing priorities beyond end-of-life discussions: I think the hospital [general care], they have different experiences than we do because they are very busy, they see and treat loads of patients … They don’t have time for these [end-of-life care] conversations like we do. (P5, focus group 1)
Participants were confident that their experience gained from frequent engagement in end-of-life discussions enabled them to effectively support patients and family caregivers in decision-making. For example, P20 (focus group 5) communicated: I think the experience of doing it repetitively or watching other people having those conversations, and then building up your own way of approaching it ... That’s the only way of getting a better understanding of how to approach it.
Key Barriers
Family Misunderstandings
A key barrier to supporting both the patient and family caregiver in decision-making for patient end-of-life care was family caregivers’ misunderstandings about who was responsible for making decisions about the patient’s care. Participants recounted that decisions which typically fall under the responsibility of the medical team (eg, pharmacological agents or do not attempt resuscitation) or which are ordinarily the patient’s choice (eg, refusal of treatment including resuscitation), were often misinterpreted by family caregivers as decisions that they (ie, the family caregiver) were responsible for. Participants reported that family caregivers themselves often felt an obligation to decide about a treatment or intervention: They [family] feel [incorrectly] that the onus is on them to actually decide when we can introduce the pharmacological management at end of life. (P12, focus group 3)
Participants felt that family caregivers’ misconceptions about who was primarily responsible for decisions about the patient’s care could inadvertently make family caregivers feel more burdened and make bereavement more difficult for family caregivers: The biggest one [family misconception] that I would have come across particularly when I worked in the inpatient unit was families [being] absolutely distraught, thinking they have made decisions around DNR [Do not attempt resuscitation]. Which is never their decision … We see it in bereavement, the family is wracked with guilt about stuff that was never their decision. (P15, focus group 4)
Family Collusion
Participants frequently highlighted the importance of protecting patient autonomy in decision-making. However, they recounted situations where family caregivers withheld information from the patient. They reported that family reasoning for doing so was based on their opinion that their ill family member would have difficulties understanding the information that they had already discussed with a healthcare professional about the patient. P17 (focus group 4) shared: I’ve seen families who feel that their loved one who is cognitively impaired or has a disability, won’t be able to have those conversations and will shield them strictly and firmly away from having it [conversation].
Participants also reported incidences where healthcare professionals beyond palliative care could be persuaded by family caregivers to withhold information from the patient and which could undermine participants’ own communication with the patient and family caregiver: I can think of a case recently [which was problematic for us] whereby the family were told all about the diagnosis and it was up to them whether they were going to tell the patient, and they were saying no, and the healthcare team were going to go along with it. (P15, focus group 4)
Over Reliance on Specialist Palliative Care
Participants reported they had sufficient expertise to facilitate patients and family caregivers in end-of-life care decision-making. However, they also felt that end-of-life care discussions with patients and family caregivers could be interpreted incorrectly by other disciplines as being solely under the remit of specialist palliative care. Participants reported that poorly timed referral of patients to specialist palliative care combined with a lack of collaborative input from other services in end-of-life care decision-making was problematic. P14 (focus group 3) communicated: I really worry that it may become a natural position that when a person wants to have decisions about their future ‘who can we get to do that? Let’s ask specialist palliative care.’ And we know that we are not the appropriate people if you have never met the patient before … We struggle to get general practitioners to engage in formal documentation of DNR status.
Participants felt a spectrum of medical specialities beyond palliative care should also support patients and family caregivers in end-of-life care decision-making: Not only your oncology and your cardiology but you know right across especially intellectual disability, all the different disciplines … I think we are only a little part of the decision-making. (P8, focus group 2)
Discussion
From the perspective of healthcare professionals in specialist palliative care, we have identified that open communication and building trust with patients and family caregivers aids them to support patients and family caregivers in end-of-life care decision-making. An early but phased approach to eliciting patients’ preferences may also assist end-of-life care discussions with patients and family caregivers. However, family efforts to conceal coupled with family misunderstanding of their (ie, family) remit in the decision-making process operate as potential barriers for healthcare professionals in specialist palliative care. Healthcare professionals in specialist palliative care value their own expertise in discussing end-of-life care with patients and their family caregivers, but also feel that end-of-life care discussions are not solely their responsibility.
We know that open communication, 23 trust, 24 and early assessment of patient preferences 25 are important for patients in end-of-life care discussions. In our study, we identified that healthcare professionals also felt that the above were of central importance. Cases of concealment and of family caregiver misunderstandings in decision-making have been reported elsewhere in palliative care.26,27 Healthcare professionals have been known to withhold information from patients at the end of life 28 and patients and their caregivers have concealed their preferences for care from each other to alleviate each other’s distress.29,30 In our study, participants reported that they did not conceal. However, they had concerns about pressure placed by family caregivers on healthcare professionals to withhold information from patients. Our findings highlight the importance for healthcare professionals in palliative care to adhere to decision-making protocols that best protect patient autonomy in decision-making for end-of-life care. 31
We identified incongruity in participants’ views on healthcare professional roles and responsibilities in end-of-life care decision-making. Participants were sensitive to the demands on other healthcare services beyond end-of-life care 32 and reported that their own skills in this domain were the result of working in a specialist palliative care setting. However, they still considered that end-of-life care discussions were also the responsibility of other services. Further research across different health systems to delineate the main commonalities in practice between specialist palliative care and other specialties for end-of-life care decision-making, would be beneficial to conduct.
A primary strength of our study is that we have identified key factors that enable and restrict healthcare professionals in specialist palliative care to support patients and family caregivers in end-of-life care decision-making. A limitation of the study is that it was conducted in 1 regional specialist palliative care service in Ireland albeit the regional service covers a large and diverse population across different care settings. Recruitment was limited to 5 healthcare professions. Moreover, sampling procedures in this study (ie, purposive) means that the findings might not be representative of all healthcare professionals working in specialist palliative care.
Conclusions
Healthcare professionals in specialist palliative care agreed that end-of-life care decision-making with patients and their family caregivers was a key feature of their work but one which can be demanding because of the onus on them to take primary responsibility to conduct end-of-life care discussions. Our findings point to the importance of open communication for healthcare professionals when discussing options for patient end-of-life care with patients and family caregivers. Open communication helps healthcare professionals in specialist palliative care ensure that patient autonomy remains central in the decision-making process for patient end-of-life care.
Footnotes
Acknowledgments
The authors sincerely thank all participants for participating in this study.
Author Contributions
HJF and GF designed the study. HJF recruited participants, collected, and analyzed the data. GF guided HJF in the analysis. HJF and GF wrote the manuscript. RMcQ supported HJF in participant recruitment and made critical contributions to the manuscript. All authors agreed on the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Trinity College Dublin.