
Abstract
Background
Patients with advanced cancer commonly involve family caregivers in decision-making for palliative care. However, how patients with advanced cancer and family caregivers accommodate each other in decision-making is unclear.
Methods
A qualitative study in advanced cancer was conducted with 14 patients and 19 family caregivers recruited from two hospices comprising a large regional specialist palliative care service in Ireland. Data comprised semi-structured interviews with participants. The data were analyzed using grounded theory coding procedures.
Results
Most patients preferred to make care decisions with their family caregiver or at least involve their family caregiver in care discussions. Patients engaged in shared decision-making because they felt they benefited from caregiver support. Patients accommodated family caregiver preferences out of concern for that person and because they trusted them. Family caregivers accommodated patient preferences because they wanted to honor the patient’s wishes and felt a responsibility to protect patient autonomy when they had a close relationship with the patient. Prior conflict between the patient and family caregiver was a barrier to mutual accommodation. Although concealment was used as a mechanism to support accommodation between the patient and family caregiver, both sought to communicate openly with other family members to negate potential conflict between each other and the wider family.
Conclusion
Patients with advanced cancer and family caregivers in specialist palliative care support one another by accommodating each other’s preferences for patient care. Patients with advanced cancer and family caregivers accommodate one another in decision-making out of a sense of responsibility to one another.
Keywords
Introduction
Decision-making can be challenging for patients with advanced cancer and family caregivers,1,2 particularly when patients experience heavy symptom burden and when end of life approaches. 2 Whilst some patients make decisions about care independently, 3 many make decisions while involving their family caregiver. 4 When engaging in shared decision-making, patients and their family caregivers may have different opinions regarding symptom management, advance care planning, and end-of-life care. 5
Multiple studies have investigated differences between patients with advanced cancer and family caregivers in care preferences.6-9 However, few studies in advanced cancer have described how patients and family caregivers manage discordance and what motivates them to accommodate each other in decision-making. Understanding what motivates patients and family caregivers to accommodate one another is important because discordance between the patient and family caregiver can be distressing for both parties. 5 Moreover, family caregiver perceived burden can be a function of increasing family caregiver responsibility for decision-making. 10
In this paper, we report findings from a study in specialist palliative care conducted in Ireland on supportive relationships between patients with advanced illness and family caregivers including in decision-making. The Irish health system is a hybrid of both public and private healthcare, but palliative care is delivered predominantly by the public and voluntary sectors. Specialist palliative care is provided in a range of settings including home, hospital, hospice, and residential care. Here, we explain how patients with advanced cancer and family caregivers receiving palliative care can accommodate each other in decision-making for patient care.
Methods
Study Design
We used a grounded theory approach 11 for this study, a systematic set of techniques and procedures for generating concepts via constant comparison between data to explain psycho-social processes in the data. 11 We used this approach because our focus was to decipher key psycho-social processes – in our case, how participants acted and behaved in both similar and different contexts that impacted on decision-making. We referred to the Standards for Reporting Qualitative Research (SRQR) 12 to report this study.
Study Setting
The recruitment setting was a large regional specialist palliative care service in Ireland comprising two hospice sites which combined cover a catchment area of circa 14% of the national population. The regional specialist palliative care service provides a mixture of inpatient hospice, outpatient hospice, and community-based care.
Inclusion/Exclusion Criteria
Inclusion criteria for patient participants were that they be ≥ 18 years old and in receipt of palliative care. Inclusion criteria for family caregivers were that they were also ≥ 18 years old and were a relative, partner, or friend who was considered by a patient in receipt of palliative care to be an informal caregiver to them.
Sampling Procedures and Participants
Description of Participants.
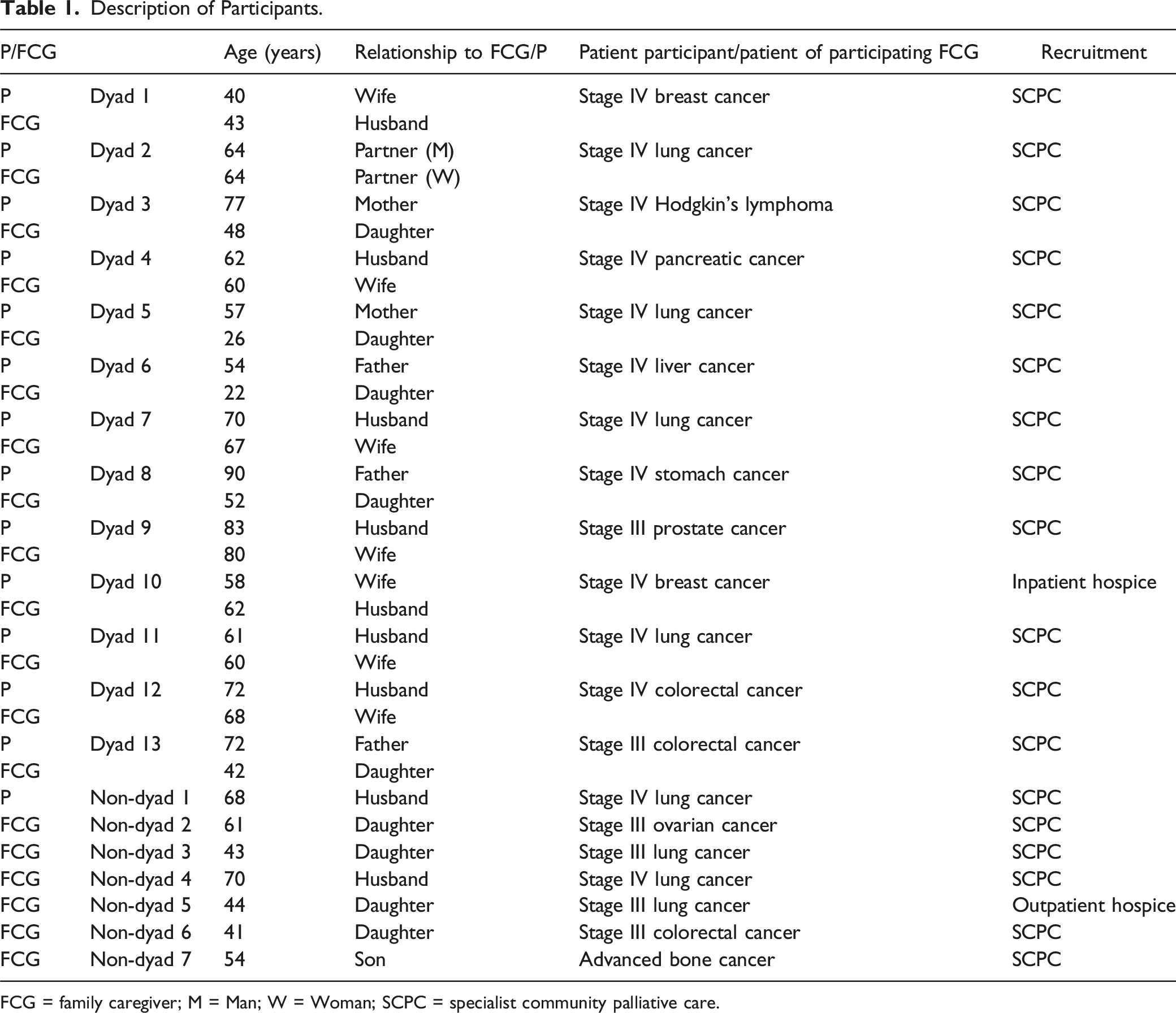
FCG = family caregiver; M = Man; W = Woman; SCPC = specialist community palliative care.
Data Collection
Data collection comprised 28 semi-structured interviews with participants focused on the topic. Interviews were conducted with 8 of the 13 dyads separately (i.e., the patient and family caregiver each interviewed on their own) [16 interviews], and the remaining 5 dyads with each member of the dyad together (i.e., dyadic interview - both patient and family caregiver in one interview) [five interviews]. All other participants were interviewed on their own. Semi-structured interview schedules were formulated consistent with the broader focus of the study on supportive relationships between patients and family caregivers including in decision-making. Tables 2, 3 and 4 (supplemental material) outlines open-ended questions asked of patients and family caregivers when interviewed alone and when interviews were dyadic. Interviews were digitally recorded, transcribed verbatim, and member checked with participants. Member checking was conducted through clarification and verification during the interviews and by providing participants with their transcript prior to the analysis to check that the data generated from them was an accurate representation of their viewpoint. No participants requested alteration to their data. Of the 28 interviews, 24 were conducted by phone, two conducted via Zoom 15 and the remainder were in-person. The interviews were carried out between July 2021 and May 2022 and the average duration of interviews was 44 minutes.
Data Analysis
The dataset (transcribed interviews) was analyzed using grounded theory coding procedures. 11 The data were first open coded which involved breaking down the data and labelling key segments of data that pointed to key incidents, behaviours, and patterns suggestive of participant intent to be supportive. We then coded the data for conceptual saturation 11 by looking for connections (relationships) between concepts to decipher key conditions and consequences of participants’ actions and interactions when deciding about care. The final stage of coding involved a theoretical integration 11 of the data to fully account for how patients and family caregivers sought to be supportive in decision-making. All stages of the analysis involved comparison between data. NVivo qualitative data analysis software was used as a tool to organize and code the data. The second author coded the data and the first author checked the coded data and cross-interpreted the data with the second author as the data were generated and analyzed. We also ensured rigor in procedures by memoing during the analysis. The final narrative was agreed by all authors. All extracts (i.e., participants’ quotes) used in the next section to illustrate the findings are pseudonymized by replacing names with participants’ ID codes as listed in Table 1.
Ethical Approval
Ethical approval was obtained from the Faculty of Health Sciences Research Ethics Committee at Trinity College Dublin (re 191002) and from the Research Ethics Committee of St. Francis Hospice Dublin. Participants provided written and informed consent to participate.
Results
The following subsections of the results explain patient and family caregiver accommodation of one another in decision-making. We report why patients sought family caregiver involvement in decision-making and why family caregivers were satisfied to be involved. We then explain how patients and family caregivers accommodated each other’s preferences and how the quality of their reported relationship impacted both patient and family caregiver ability to accommodate.
Family Caregiver Involvement in Decision-Making
Most patients preferred to involve their family caregiver directly in decision-making about their care. One of two main reasons for involving their family caregiver in decision-making was patients feeling they needed and benefited from their caregiver’s support in decision-making. Patients frequently communicated how they depended on their family caregiver when making decisions about care: I completely rely on him [family caregiver] just 100%. I completely rely on him for everything including decisions. He's just been an absolute rock to me. (P, dyad 1)
The second main reason behind patients involving family caregivers in decision-making was to alleviate any concerns that their family caregiver might feel if they were not involved in decision-making. For example, another patient communicated: Every time I got chemo … I’d have to think of [family caregiver] because it would affect her in the long run … without consulting. (P, dyad 12)
Family caregivers expressed satisfaction about having an active role in the decision-making process. However, they were also conscious not to overly persuade or dissuade the patient in decision-making out of respect to the patient’s own choices: I suppose any of the suggestions that have been put to us or any changes … upcoming medical appointments and things like that … It's my role to respect exactly how she [patient] wants to go about things as well. I can't say ‘well I think you should do this’ if she doesn't want to do it. We can talk about it and maybe I’d have a little bit more of a voice on certain things but as I say I have to support and I have to respect the decisions that she wants to make. (FCG, dyad 1)
Both patients and family caregivers were conscious of other family members’ opinions about the patient’s care, particularly if other family members’ opinions had potential to cause conflict between the patient and family caregiver. In these situations, patients and family caregivers acted by communicating openly with other family members to negate possibility of conflict between each other and the wider family. For example, participants recounting their efforts to avoid conflict, communicated: I can see the signs [of argument] and it didn't come to that … what I done was I put them all together … Just to take the family unit, treat the family unit right and the rest will work out. (P, dyad 4) After he has made his decisions, I will then support, whether I like them or not … I will go to my extended family, my brothers and I’ll even talk to my husband and kids then and say what Dad has chosen to do and highlight that his decision must be respected and they then agree. (FCG, dyad 13)
Patient and Family Caregiver Accommodating Each Other’s Preferences
Family caregivers accommodated patient preferences when they were sensitive to patient distress. In these cases, and even if family caregivers disagreed with the patient, they proceeded to conceal their differences from the patient to avoid exacerbation of the patient’s distress. A family caregiver explained: He's [patient] got very finicky [difficult to please] since he got the cancer. Normally, he's always in great form, he's happy go lucky guy … [but] now I would have to bite my lip, walk out to the hall, take few deep breaths, and walk back in, you can imagine. But it's not him, it's the pain. (FCG3, dyad 2)
In most cases, family caregivers were motivated to honor the patient’s wishes for their care because they felt they had a responsibility to do so given the support they themselves had received in the past from their now ill family member. For example, a family caregiver communicated: I would love to be here for my mam you know but obviously like it's her choice. I wouldn't be happy with her going to the hospice but it's her choice … she's done so much for us as a single parent … [so] obviously it's her decision. (FCG, dyad 5)
Patients sometimes agreed with their family caregivers out of a sense of responsibility to them. In doing so, patients also sought to conceal their preferences – in their case, to help their family caregiver navigate their own needs. For example, a patient whose preference was to limit caregiving from his family caregiver voiced: I know she’s wound up about the whole thing [providing care] and unless she was there, she wouldn't be happy. So, I let her go along. And she's happy to go with that and she's looking around to do different things all the time … At the moment, it’s more for her than me. (P, dyad 13)
However, patient accommodation of family caregivers’ preferences was not only because they felt obliged to do so. Patients also placed trust in family caregivers to make the best decision for them when they viewed them more capable than themselves in a decision-making role: If he's [patient] going to hospital appointments, he'll always say to me, ‘Are you taking me to it?’ because ‘you know everything regarding the medication and what's happening to me’. (FCG, non-dyad 3)
In some cases, patients’ trust in family caregivers resulted in patients rendering responsibility for decision-making to a family caregiver: I would trust [family caregiver] to make the best decision for me … I trust him deeply, that you [speaking to caregiver] know, if you're saying that this is going to do me good. I trust you completely on that. (P, dyad 1)
Quality of Relationship Between Patient and Family Caregiver
There was variation among participants in terms of the quality of the relationship they reported with their respective other. Participants who reported prior conflict in their relationship struggled to accommodate their respective other. For example, a family caregiver who had reported long-standing conflict with his parent [patient] shared: She [patient] always has been quite a difficult person to live with … [Now] she's horrified by the idea of having to use a commode … [Whilst] that kind of thing I would find difficult to deal with … but it’s necessary, absolutely necessary. (FCG, non-dyad 7)
However, patients and family caregivers who felt they had a strong relationship with the other were more willing to accommodate each other in decision-making. A family caregiver who had already reported a strong bond between her and her mother [patient] disclosed: When it came to her chemotherapy … she was the only one who could decide if she wanted to keep going even though it wasn't going to help her, it was going to make her sick … She kept saying ‘No, I'm going to take it, I'm going to pay for it’ and I said ‘Okay, it’s your body if you want to do it’ and then she decided no, she wouldn't do it. (FCG, dyad 3)
The family caregiver’s tendency to accommodate the patient’s preference (when they reported a close relationship with the patient) was explained by them valuing the patient’s autonomy in deciding on matters relating to their own (i.e., patient’s) care: We [family] have to make sure that no matter what's happening with [patient], he is the one who is most involved, that we make sure that he understands and that he gets a chance to say what he wants. (FCG, dyad 7)
Discussion
Our findings pertaining to patients’ wish to include family caregivers in decision-making resonate with other studies of people with cancer and their family caregivers, 16 including in palliative care. 17 Family caregivers’ willingness to be actively involved in and/or in some cases, lead on decision-making, is also consistent with other palliative care studies which have investigated family caregiver preferences in a caregiving role for people with advanced cancer.18-20 However, in our study, we identified some concealment between patients and family caregivers of their preferences for care even when patients and family caregivers sought to participate collectively in decision-making. Concealment between patients and family caregivers manifested when they felt that an otherwise explicit account of their differences might cause more distress for the other. Concealment in situations where both the patient and family caregiver actively encourage the other in a decision-making role is to the best of our knowledge an under-reported dimension of patient and family shared decision-making in palliative care. We found that patient and family caregiver concealment was intended to be mutually supportive and assisted them to accommodate preferences of the other.
As reported, family caregivers felt a responsibility to honor the patient’s wishes in return for the support they had already received from their ill family member. We found that family caregivers felt such actions and behaviours constituted a form of reciprocal support between them and the patient, and this was the case for both intra- and inter-generational based relationships between patients and family caregivers. A systematic review of mutual support between patients and family caregivers in palliative care found that patients and family caregivers do reciprocate in supportive roles. 21 Our findings point to what can motivate family caregivers to reciprocate.
We identified that having trust in their family caregiver was important for patients because it alleviated concerns around decision-making particularly in situations where patients felt they had become increasingly dependent on their family caregiver for their care needs. Trust as a feature of decision-making in palliative care is commonly reported in studies focused on patient relationships with healthcare professionals.22,23 In our study, we found patient trust in their family caregiver meant that patients felt able to make decisions about their care but also in some cases, able to render control to the family caregiver. Patient trust in their family caregiver as a catalyst for both exerting and rendering control expands our current understandings of how trust and control function for patients with advanced cancer in palliative care.24-26
A key finding in our study was family caregivers’ wish to protect patient autonomy in decision-making, particularly when family caregivers reported a close relationship with the patient. Family caregivers’ desire to protect autonomy of the patient resonates with other studies in the field.27,28 Importantly, we identified that the patient approach to decision-making was modulated not only by their own needs but also by those of their family caregiver. Hence, our findings support the argument that autonomy in palliative care be understood as relational autonomy.29-31 This means that people with serious illness do not make decisions about their care based only on their own preferences, but rather factor in preferences of others close to them.
A primary strength of our study is that we have identified how patients with advanced cancer and family caregivers receiving palliative care can accommodate each other in decision-making. A limitation is that recruitment was limited to one (albeit large) regional specialist palliative care service in Ireland. In addition, a minority of the sample (n = 7) participated on their own which means that their data were less contextualized to their respective other. Lastly, the sample were patients and family caregivers who were willing to discuss aspects of supportive relationships between them. Hence, the sample might not be fully representative of all patients with advanced cancer and their family caregivers.
Conclusion
We have identified how patients with advanced cancer and their family caregivers in palliative care can accommodate each other in decision-making. From a research perspective, future multi-center studies on this topic and which incorporate advanced illness beyond cancer are needed to expand on the findings. Studies which include the healthcare professional perspective with a focus on how they impact patient and family caregiver accommodation of each other in decision-making would be useful to further our understanding of relational autonomy in palliative care. From a practice perspective, the findings are important for healthcare professionals in the field who seek to support patient and family caregiver understanding of each other’s needs. Interventions in palliative care that focus on helping the patient and family caregiver to understand what motivates them to accommodate each other may be particularly beneficial to support both the patient with advanced illness and family caregiver in decision-making.
Supplemental Material
Supplemental Material - How do Patients With Advanced Cancer and Family Caregivers Accommodate One Another in Decision-Making? Findings From a Qualitative Study in Specialist Palliative Care
Supplemental Material for How do Patients With Advanced Cancer and Family Caregivers Accommodate One Another in Decision-Making? Findings From a Qualitative Study in Specialist Palliative Care by Geraldine Foley, Rachel McCauley, Regina McQuillan, Karen Ryan in American Journal of Hospice and Palliative Medicine®
Footnotes
Acknowledgments
The authors wish to thank all participants for their time and for sharing their experiences and perspective with us. We also thank personnel at each recruitment site who assisted with participant recruitment.
Author Contributions
The first author (GF) designed the study, obtained funding to conduct the study, supervised the study, interpreted the data, and wrote the manuscript. The second author (RMcC) recruited participants, collected the data, transcribed the interviews, analyzed and interpreted the data, and made critical contributions to the manuscript. The third author (RMcQ) and fourth author (KR) advised on recruitment strategies and data collection methods and made critical contributions to the manuscript. All authors approved the final draft of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Trinity College Dublin Provost’s Project Award.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.