
Abstract
This research, a descriptive qualitative analysis of self-defined serious illness goals, expands the knowledge of what goals are important beyond the physical—making existing disease-specific guidelines more holistic. Integration of goals of care discussions and documentation is standard for quality palliative care but not consistently executed into general and specialty practice. Over 14 months, lay health-care workers (care guides) provided monthly supportive visits for 160 patients with advanced heart failure, cancer, and dementia expected to die in 2 to 3 years. Care guides explored what was most important to patients and documented their self-defined goals on a medical record flow sheet. Using definitions of an expanded set of whole-person domains adapted from the National Consensus Project (NCP) Clinical Practice Guidelines for Quality Palliative Care, 999 goals and their associated plans were deductively coded and examined. Four themes were identified—medical, nonmedical, multiple, and global. Forty percent of goals were coded into the medical domain; 40% were coded to nonmedical domains—social (9%), ethical (7%), family (6%), financial/legal (5%), psychological (5%), housing (3%), legacy/bereavement (3%), spiritual (1%), and end-of-life care (1%). Sixteen percent of the goals were complex and reflected a mix of medical and nonmedical domains, “multiple” goals. The remaining goals (4%) were too global to attribute to an NCP domain. Self-defined serious illness goals express experiences beyond physical health and extend into all aspects of whole person. It is feasible to elicit and record serious illness goals. This approach to goals can support meaningful person-centered care, decision-making, and planning that accords with individual preferences of late life.
Keywords
Introduction
People are living longer with multiple medical conditions, 1 causing functional, social, and emotional stresses that threaten an individual’s independence and quality of life. 2 Multiple comorbidities become serious illness in the presence of disease progression, complications with high mortality, disabling physical and cognitive decline, and significant disease burden that affects daily life, eventually leading to death. 3,4 Disease management practices and guidelines rely on biomarkers 5 and typically do not account for whole-person needs and individual preferences. 6,7 Over the experience of a changing disease trajectory, personal preferences may proceed over a spectrum from desiring to cure, to living longer, to prioritizing meaning, and quality over quantity of life. 8,9 This discordance between individual preferences and disease-specific guidelines makes it difficult to match care to desired preferences.
Person-centered, person-directed care 10,11 can create challenges for providers in adhering to medical guidelines. 12 Goal-oriented care better supports the health and well-being of chronic illness and end-of-life (EOL) care and recommends parting from problem-oriented medical care that focuses on diagnosing, treating, and fixing. 13 Goal-oriented care 14 promotes the use of self-defined health goals in decision-making and assists providers in managing multiple often conflicting, disease-specific guidelines and an individual’s ideal state of health. 15 Palliative Care guidelines, 16 preferred practices, 17 and a recent Institute of Medicine report 18 call for incorporation of earlier practices that include ongoing goals of care discussions and advance care planning (ACP). Research suggests substantial gaps remain between the type of care patients receive at the EOL and care they would prefer to receive, 19,20 indicating a need to understand individual goals beyond physical, disease-specific medical care.
There is less understanding of care goals for patients with serious illness in the last years of life than for those who are sick enough to die within weeks or months. 21 Most EOL goals focus on life-sustaining treatment options, whereas other goals are described in terms of varied and diverse outcomes of maintaining physical function and independence, relief from pain, symptoms, suffering, and longer survival. 8,22 Current tools (eg, disease-specific guidelines and advance directives) designed to address medical needs and preferences are not well suited to individualized care of patient’s psychosocial nonmedical needs. 23 Strategies to move palliative care upstream from traditional models of delivery suggest a shift to person-centered individualized care beyond the EOL experience. 24 Whole-person planning could best be accomplished when self-identified physical and psychosocial goals have been elicited and shared.
Poor completion of advance directives and stated EOL concerns of Americans 25 makes it difficult to know whether patients received desired care throughout the serious illness experience upstream from EOL preferences. To ensure care desired matches care received, we first need to expand our knowledge of what kind of goals are important beyond the physical domain and EOL planning—making goals of care discussions and disease-specific guidelines more holistic. This research is a descriptive analysis that examined whole-person goals of patients with serious illness identified during their last 2 to 3 years of life. The qualitative results should help to better understand whole-person priorities that could be missing from existing clinical assessments, disease-specific guidelines, decision-making, and care planning.
Methods
The current research is part of a 4-year late life supportive care study within a large Midwestern metropolitan health-care system in the United States. An upstream community-based palliative care approach, called LifeCourse, provided whole-person, patient-centered support alongside existing care services for patients and families with advanced medical conditions expected to be in the last 2 to 3 years of life. Intervention activities were expected to show positive results in quality of life, patient experience, 26 and total cost of care. Trained lay health-care workers (care guides [CGs]) visited monthly and collaborated with the patients’ primary care team members. The CGs were supported by an interdisciplinary team that included nurses, social workers, a chaplain, a family therapist, and a pharmacist. 27 Each CG supported patients through a set of palliative care activities, assessment tools, 28 –33 a whole-person conversation guide, and specific visits. 34,35 This approach allowed the CG to provide a person-centered approach driven by self-defined goals, linking patients and families to existing health-care services and community resources. Subsequent to the research, CGs are being integrated into high-risk care management populations, primary and specialty care, and a federally qualified health center.
The present analysis was an initial inquiry to describe self-defined goals patients living with advanced heart failure, cancer, and dementia shared with their CG. The CGs entered goals into an electronic health record (EHR) flow sheet using direct quotes or patient-validated statements. A major focus of the CG work was to help patients’ articulate goals by identifying what was most important at the time. Each monthly visit utilized a framework that began with questions like, “What is most important to you?” and “What are you willing to work on?” The CGs used broad, uniform, open-ended questions to encourage identification of whole-person goals beyond illness and physical health. The CGs were trained in motivational interviewing to standardize the variability in individual approaches and encouraged exploration of patient-stated goals. This study was approved by the relevant institutional review boards. Patients consented to take part in the study, making their EHR data available for research purposes.
Researchers exhaustively sampled 160 patients, who enrolled during the first 17 months of the larger study period between November 7, 2012, and March 25, 2014 (Table 1). Researchers analyzed the contents of individual goals’ flow sheets, accommodating up to 30 goals that changed or were carried forward over time. Data were drawn from the “description” and “plan” flow sheet fields. Medical record documentation of goals available for the broader care team to review were automatically populated into the CG visit notes (Figure 1).
Characteristics of 160 Participants at Baseline.
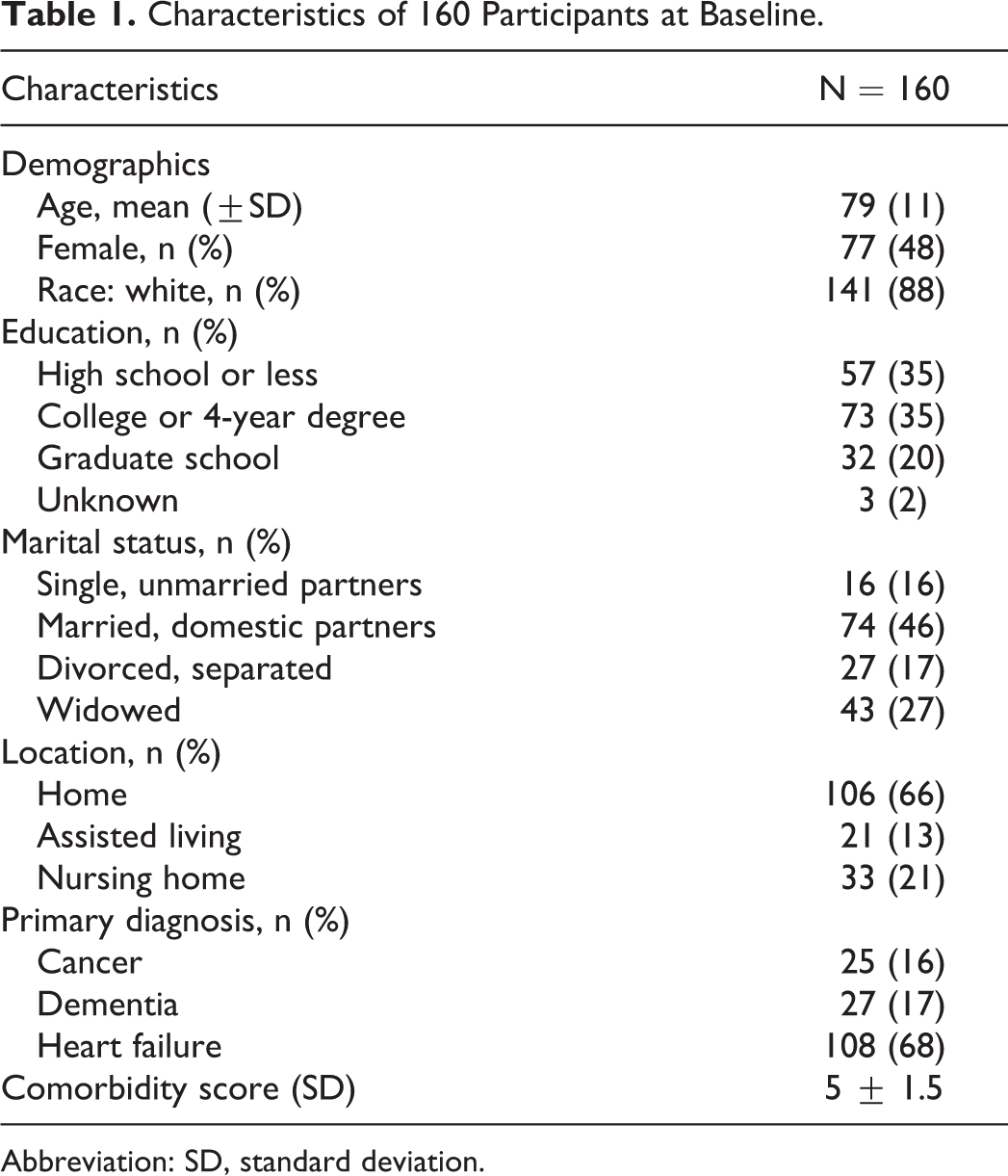
Abbreviation: SD, standard deviation.
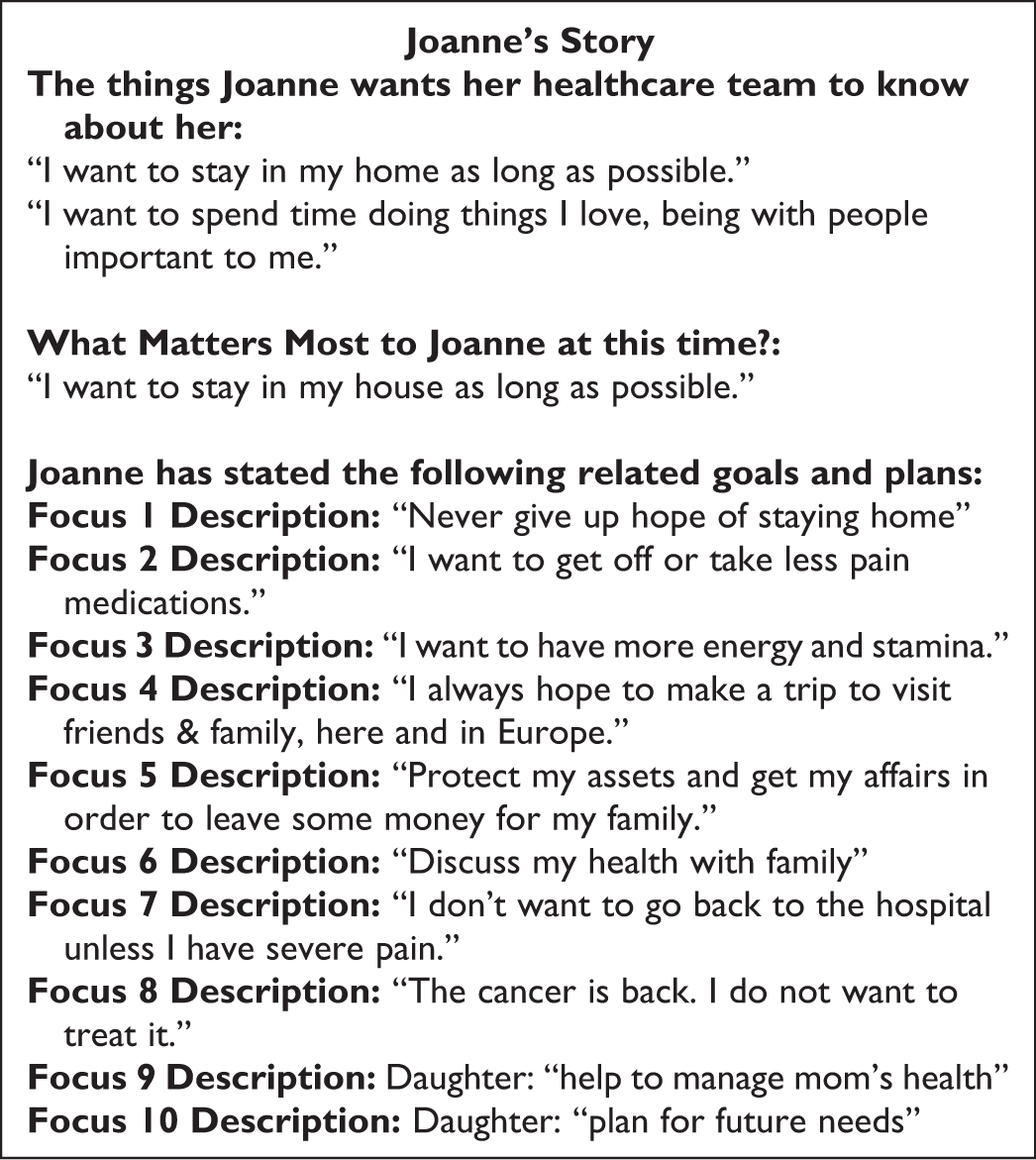
Example of serious illness goals documentation in the medical record.
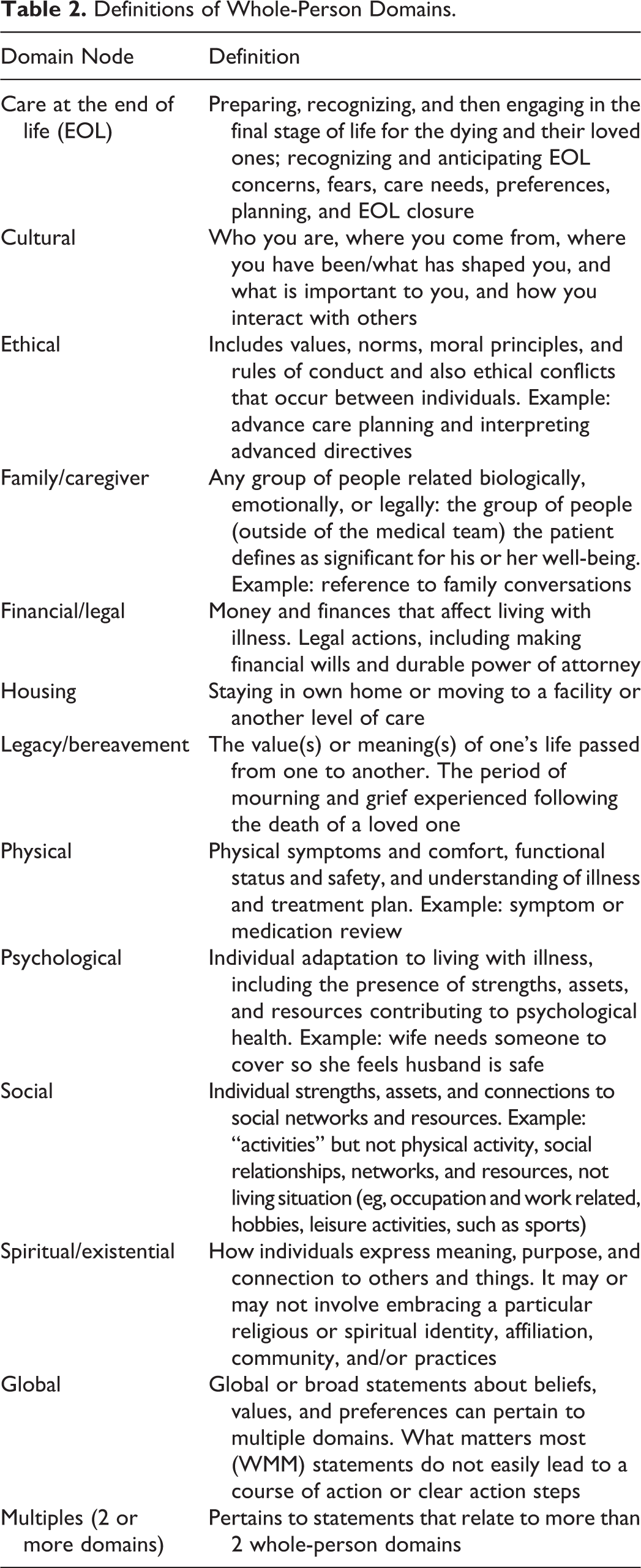
The overarching analytic strategy for this research was a fundamental qualitative descriptive approach aimed to describe the content of patient goals in everyday language. 36 Deductive analysis and coding were conducted according to the methods outlined by Saldana 37 and based upon an expanded set of whole-person domains of the National Consensus Project (NCP) Guidelines for Quality Palliative Care. 16 The NCP presented 8 whole-person domains, physical, social, ethical, and other aspects of care, which LifeCourse expanded by adding family/caregiver, financial/legal, and legacy/bereavement domains during development of the broader intervention. The NCP domain “structures and processes of care” did not focus on individualized planning and was not used for this analysis.
The first part of the analysis sought to operationalize the whole-person domains by developing code definitions. First, each researcher independently coded 25% of the data and developed a definition for each code based upon their review. All researchers compared coding associated with each domain until consensus on definitions for each code was achieved.
Second, 2 researchers (S.E.S. and E.W.A.) independently coded 100% of the data using the established code definitions and met to resolve discrepancies. The primary source of information examined for coding was the “description” field in the flow sheet. The “plan” field was used when “description” did not include enough information to enable coding to a specific domain(s). While resolving discrepancies, researchers identified 3 additional domains that resulted in 13 unique definitions and domains (Table 2). Ten domains described aspects of whole person. Simultaneous coding was avoided. 37 Goals reflecting 2 or more whole-person domains were coded as “multiple.” An additional domain identified as “housing” was derived using an eclectic coding 37 approach that reflected complex meanings expressed by patients about a strong desire or a sense of importance about where, how, and with whom patients wanted to live. Finally, we identified broad goals or aspirations, coded as “global.” Each domain was then categorized and grouped according to themes.
Definitions of Whole-Person Domains.
Results
This data set included 999 goal entries. Some goals were repeated over time, averaging 1.83 occurrences per unique goal. Patients expressed a range of 1 to 16 goals each, with an average of 4.2 and a median of 4 goals. We found some goals were repeated with little change to the wording or plan over time, so it was difficult to determine when a goal transitioned to a new focus. Analysis revealed a variety of goal statements categorized into 4 broad themes—medical, nonmedical, multiple, and global. The distribution of goal statements by broad theme was 40% medical goals, 40% nonmedical goals, 16% were a mixture of “multiple” domain goals, and 4% global statements (Figure 2).
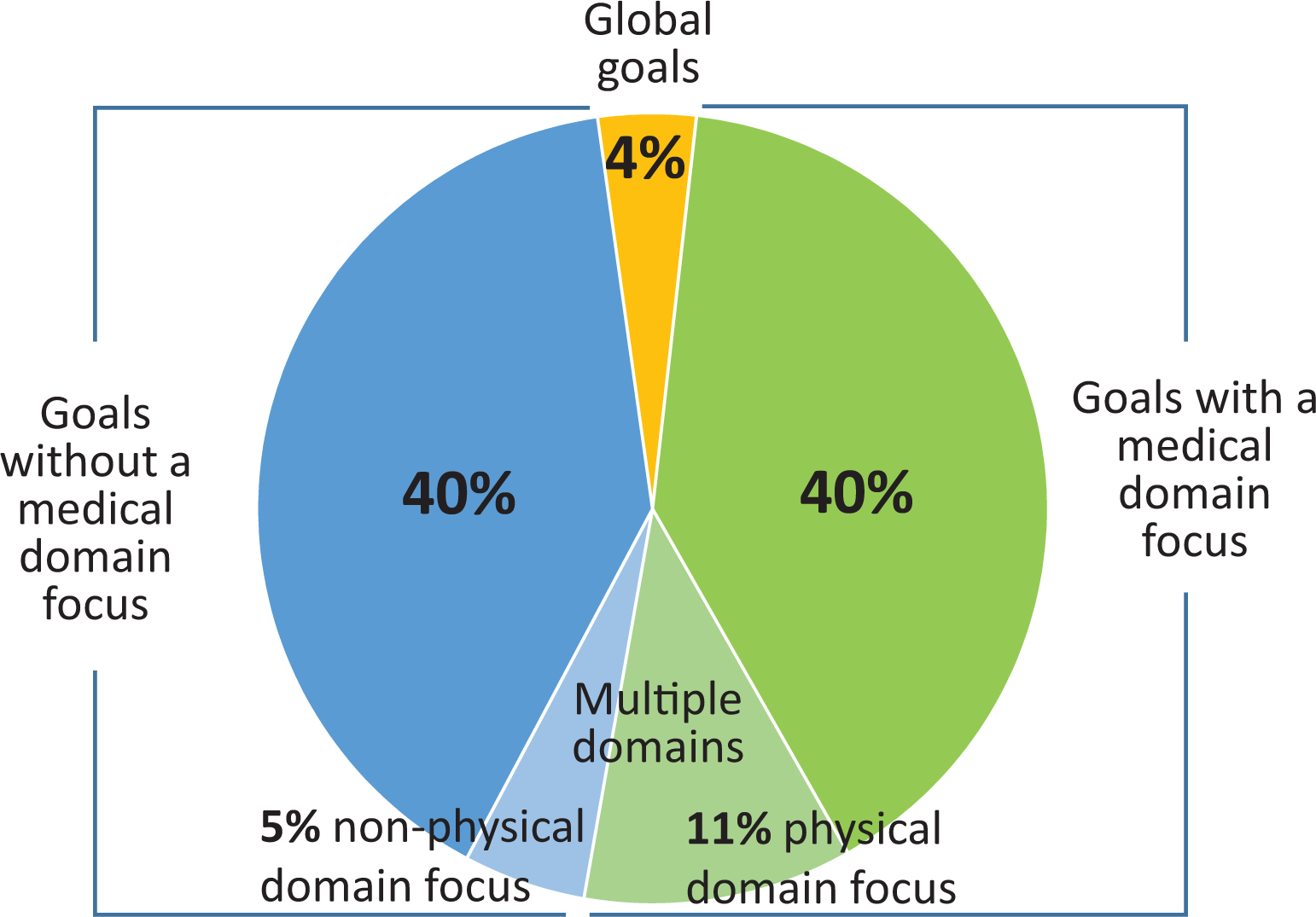
Distribution of 999 serious illness goals by theme.
Medical goals
Medical goals described activities that promoted change in physical and cognitive well-being or health. Medical goals such as “get through chemotherapy,” “take less medications,” and “manage my blood sugar” were attributed to the physical domain and reflected desires for completing treatment plans to cure or arrest a medical condition. Some goals, such as “reduce Hemoglobin A1c and lower my high blood pressure,” were very specific to controlling and managing medical conditions. Goals related to symptom reduction, such as “I want to breathe better without oxygen,” “resolve facial edema,” and “get rid of the tingling in my arm” revealed patients’ desires to feel better and reduce symptoms. Goals to reduce and/or improve physical or cognitive limitations included “get stronger,” “walk without a cane,” “avoid being in a wheelchair,” and “be less forgetful.” Some medical goals had 2 physical foci; for example, “I want to lose weight so I can breathe better” and “I want to improve my appetite, eat more so I can take chemo.”
Nonmedical goals
There were almost as many nonmedical goals as physical goals. Nonmedical goals reflected other aspects of whole person and were coded in terms of the following domains—social (9%), ethical (7%), family/caregiver (6%), financial/legal (5%), psychological (5%), housing (3%), legacy/bereavement (3%), care at the EOL (1%), spiritual (1%), and culture (0%). Although these goals were not individually as prevalent as medical goals, each domain ended up having specific themes identified. The following analysis includes the findings within each nonmedical domain node.
Social goals included activities focused on connecting to others (eg, “getting Internet to email,” “get a phone in my room,” and “go on a fishing trip in Canada”); giving back to others (eg, “volunteer for AARP [American Association of Retired Persons]” and “volunteer for others with heart failure”); maintaining vocational activities and hobbies (eg, writing, woodworking, quilting, and sewing); and accessing resources and support (eg, “get medications and food delivered” and “apply for metro mobility”).
Ethical goal statements reflected ACP activities, such as completing a health-care directive and changing health-care agent, “I’d like to have a health-care directive.” Family/caregiver goals focused on getting support and resources for family/caregivers (eg, “My daughter and I need some support”) and managing relationships (eg, “I want to spend time with family” and “I want to reconcile with my son”).
Financial/legal goals reflected statements about financial security, preparing paperwork for family, and paying for current care needs, such as “have enough money while I am alive and after I die,” “I want to get my affairs in order,” “I want to create a will,” and “pay for medications at a lower cost.” Psychological goal statements focused on activities to change the state of emotional and mental health, such as “I want to keep a positive mental attitude,” “acupuncture for relaxation,” and “I need emotional support to deal with my illness and other concerns.”
Although few, housing goals reflected desires about where, how, and with whom patients wanted to live and the location and type of care for the purpose of preserving independence (eg, “to stay in my home,” “find new housing so…only one more move required”). Housing goals also reflected a desire to live with others and reduce financial and family burden of care (eg, “to decide on a new place to live with my son David” and “…move to a place where there are increasing levels of care…when I need it”).
Legacy/bereavement goals focused on the donation of time and talents, reflection of personal life values and beliefs, and worries or concerns about grief and loss, for example, “I want to complete my novel,” “organize my stuff for my family,” and “I worry about my family being sad after I die.”
The care at the EOL, spiritual, and cultural goals contained the fewest self-defined goals. The EOL goals focused on care options and preparation for the EOL (eg, “explore hospice options and plan for funeral” and “die peacefully—die in my sleep”). Goals reflecting spiritual activities were about staying connected to a spiritual community and counseling to support spiritual needs, such as “go to church every week” and “talk with pastor about experience with dementia.” There were no cultural domain goals.
Multiple domain goals were complex and not easily attributed to a single domain leaving 16% coded to 2 or more domains. The majority (11%) of multiple domain goals were coded into the “physical” and to 1 or more nonmedical domains (Figure 2). For example, “I’m hoping to continue feeling well so I can continue playing golf, doing art, attending church, and seeing friends” was coded into both “physical and social” domains. In another example, a patient’s goal focused on physical activities to stay healthy, so he could enjoy life with his wife. The corresponding plan for this goal included additional domains of “family/caregiver, global, and housing” domains (eg, “John (a fictionalized patient name) is, while struggling with his illness, acting as a care giver for his wife who has early stages of dementia.…He is hopeful to continue to live well enough to enjoy life and is prepared to make measured steps…to accommodate that (ie, nursing home, etc).”
The remaining 5% of multiple domain goals reflected a mix of nonmedical goals beyond the “physical” domain and expressed a combination of issues specific to all other domains. For example, the goal “I want to visit my daughter in Chicago” was coded to the “family/caregiver” domain, and because the “plan” for this goal included arranging for dialysis in Chicago and setting up affordable transportation, it was also coded into the “physical, financial/legal, and social” domains. Some “multiple” domain goals included more than 1 focus making it difficult to target a single domain. Goals of this type were coded to all domains represented in both goals (eg, “I want to walk and be more independent to avoid moving to assisted living” was coded into the “physical, global, and housing” domains).
The fourth theme, “global,” included aspirational statements that often conveyed emotions, hope, or meaning and purpose in relation to something bigger than an individual aspect of self (eg, “I want to stay alive” and “I want to see my grandchildren grow up”). Global statements usually had no desired plan or identified actions attached to them (eg, “I want to wake up and breathe”). In the absence of an attached plan, “global” goals described a broader sense of meaning and hope, such as “I want to feel alive every day.” “Global” statements focused on living a healthy lifestyle, living longer, emotional or spiritual well-being, relationships, “being normal,” and independence.
Discussion
Movement from problem-oriented disease-specific care implying a desire to be fixed toward goal-oriented care based upon individual desires of health within all aspects of whole person has potential to improve or maintain quality of life when physical decline is inevitable. 13 Research results demonstrate that patients express a diverse range of goals related to global aspirations and many facets of the whole person, which patients identify nonmedical goals as often as medical goals. Identification and consideration of medical, nonmedical, multiple, and global goals of serious illness presents an opportunity to individualize assessments and care planning processes. 38 Whole-person assessments realign disease-specific goals with views of well-being beyond physical health 39 that have been shown to support broader psychosocial needs. 7 Care planning and goals of care discussions including self-defined goals can assist in individualizing and setting context to established disease-specific guidelines and assist decision-making that more fully reflect current health status and psychosocial spiritual aspects of patients’ lives. 7,40
Integrating nonmedical day-to-day living goals 41 is especially relevant for serious illness to sustain a sense of hope and healing when physical decline, cure, or controlling a disease is no longer possible. 42,43 Research participants were less likely to identify goals specific to EOL and few had global aspirational goals. Serious illness discussions will miss the psychosocial and emotional issues that help individualize care if providers fail to acknowledge whole-person goals before embarking on disease-specific medical plans and advance directive life-sustaining treatment options. Expanding EOL discussions to include a whole-person approach which includes nonmedical goals may help increase understanding about what is at the heart of patient wishes and individualized care needs.
Advance directive completion is a gold standard to documenting patient goals. The physical decline expected in serious illness increases the potential for goals to change, indicating a need for ongoing conversations which advance directive completion alone cannot support. 44,45 This research indicates that it is possible to review and document patient goals beyond ACP and disease-specific interventions and could enable systems that support individualized serious illness care. 38 Research findings demonstrated goals articulated by a patient in discussions can be documented in the medical record and made available to other clinicians.
This analysis is a first step to exploring the expressed goals of patients with serious illness and offers a platform for how self-defined goals may be collected and evaluated in generalized palliative care approaches. The results are relevant to a primarily Caucasian group of patients with heart failure, cancer, and dementia, likely in their final 2 to 3 years of life, who received care within a Midwest Health System. These results can inform future research about the goals of a more representative population of patients with serious illness and how patient-defined goals may be collected and used by clinicians.
Patient self-defined goals reveal a rich mix of preferences attributed to medical, nonmedical, multiple, and global goals. When patients living with serious illness are asked what they feel is most important to them, most goals reveal deeper wishes and desires beyond physical needs and express a host of social, ethical, family, psychological, financial, and bereavement needs. Looking further into the relationship between particular goals and more global aspirations may help us better understand what is at the heart of our patients’ wishes in order to receive an individualized care approach.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: From the Robina Foundation.