
Abstract
Palliative care (PC) longitudinal curricula are increasingly being recognized as important in Undergraduate Medical Education (UME). They are however, not yet commonplace, and where they do exist may be implemented without a systematic, prospective approach to curriculum evaluation. This paper describes an implementation of a new longitudinal curriculum at the Perelman School of Medicine (PSOM) at the University of Pennsylvania. We used the Context Input Process Product (CIPP) model, a holistic evaluation model, to assess the local environment, design the curriculum, guide the improvement process, and evaluate outcomes. Comprehensive models such as CIPP provide a more robust approach to curriculum evaluation than outcomes-only models and may be of use to other programs who are implementing new curricula or improving upon existing programs.
Keywords
Introduction
CARE-7 Goals and Objectives.
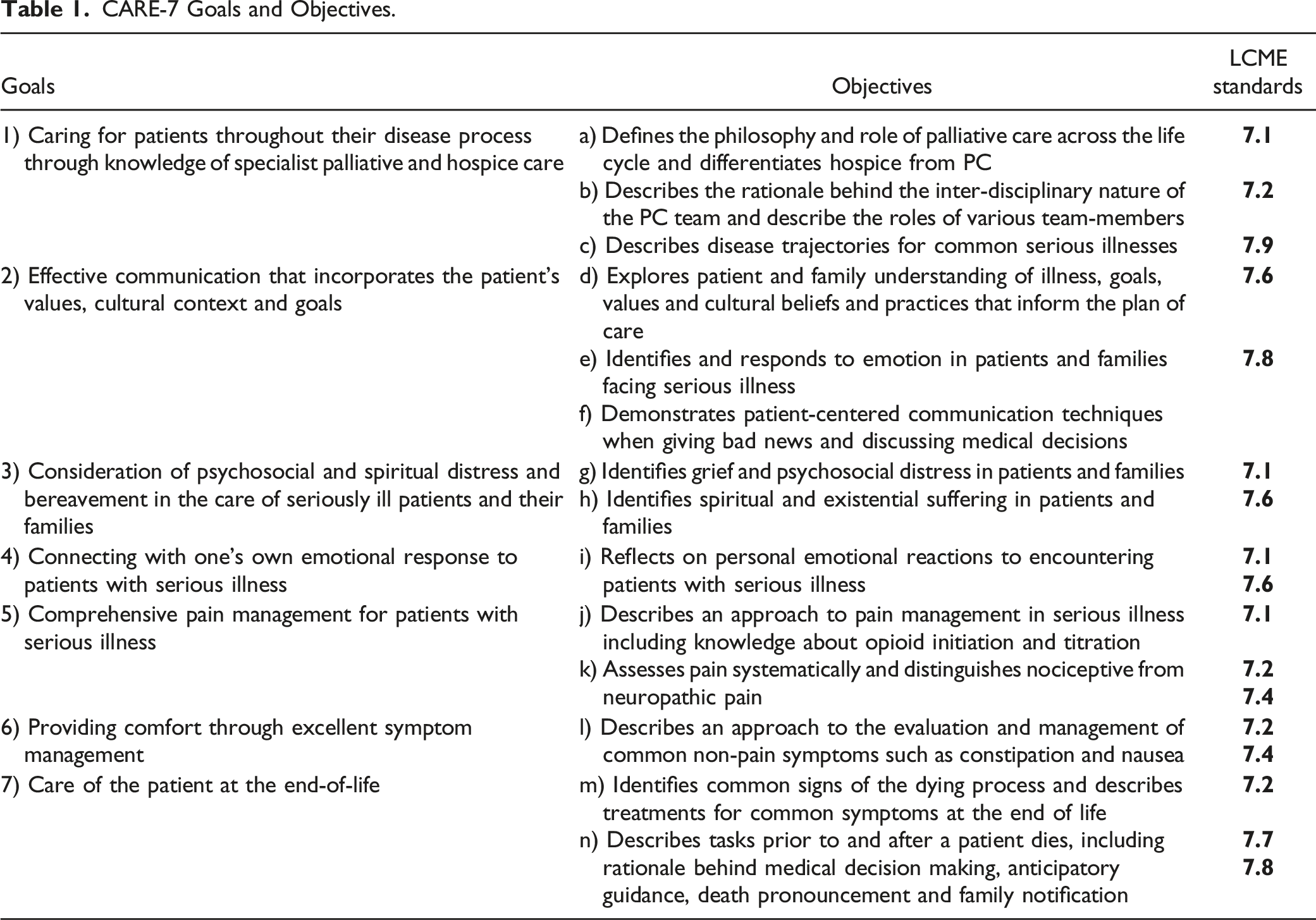
Program History
Prior to the implementation of CARE-7, typical PC content at PSOM was scant, often voluntary, and designed by educators who were not always content experts. The structure of oversight for the PSOM curriculum was changed in July 2019 coincident with the development of a new leadership team in Medical Education under the leadership of a new Senior Vice Dean. At the same time, a new paradigm for the development of longitudinal courses was developed beginning with a list of key curricular topics that needed enhancements. A plan for definitive direction for longitudinal curricular development across the entire curriculum with defined goals, objectives and curricular elements was put into place. In the Spring 2021, 1 of the authors (S.R.) began discussions with an interested donor to support the longitudinal development in PC. Upon development and submission of a CARE-7 curriculum proposal (N.B.), this came to successful fruition. In the Fall of 2021, a curriculum director (A.S.) and co-directors (R.M., J.O.) were named, and a curriculum evaluation committee was assembled. Curriculum directors are board-certified hospice and palliative medicine physicians who practice specialty PC. The curriculum evaluation committee is composed of the CARE-7 directors, school of medicine leadership, PC leadership as well as curriculum evaluation experts.
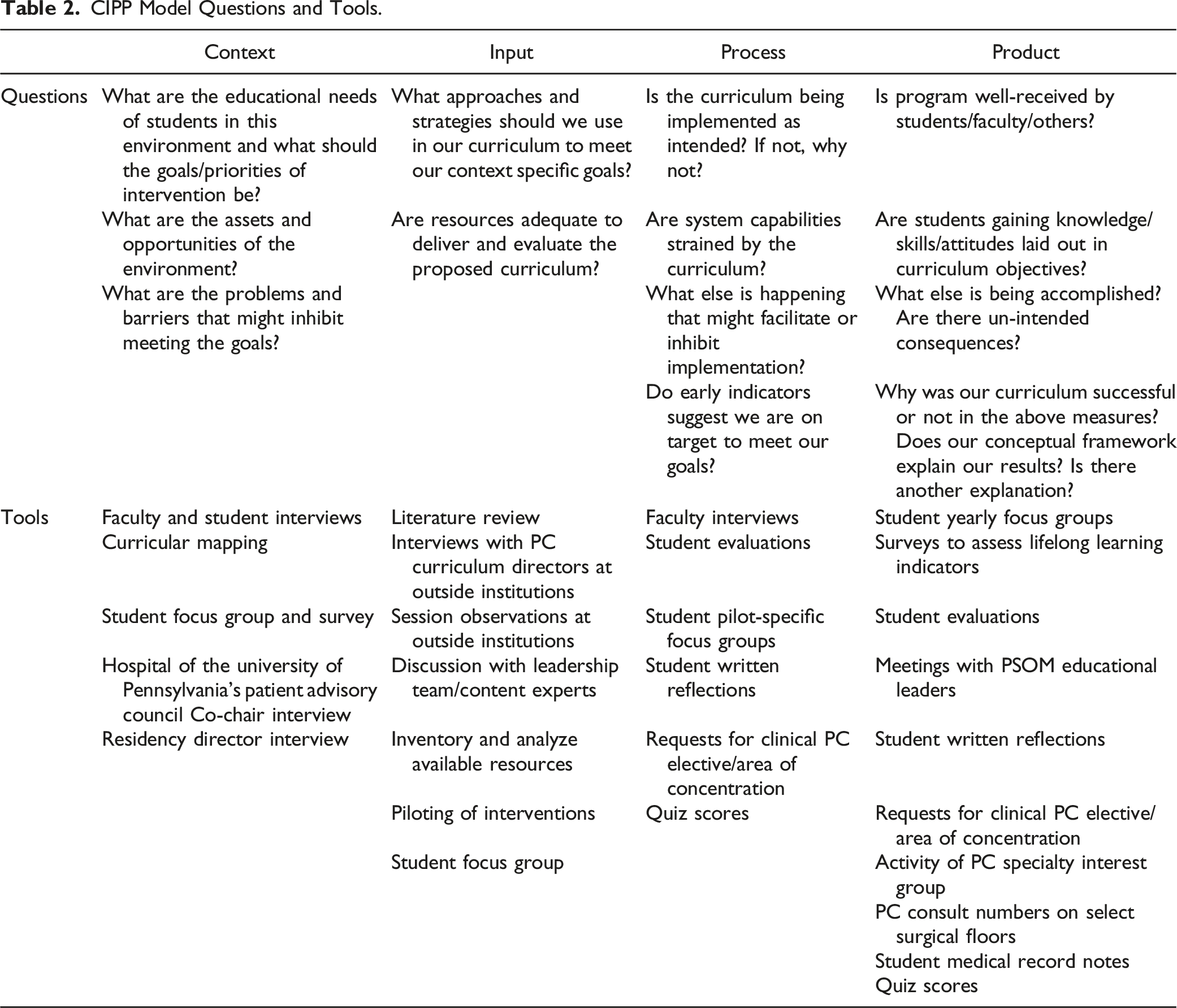
CIPP and the Program Evaluation Model
CIPP Model Questions and Tools.
Context Evaluation
Context evaluation focuses on assessing the needs, problems, and opportunities of the educational environment, acknowledging that a curriculum’s design, implementation, and evaluation process will depend upon contextual factors. Our context evaluation questions centered on educational needs as well as assets/opportunities and barriers. Here, we use the terms context, environment, and environmental context interchangeably.
Context Evaluation Methods
Student Survey.
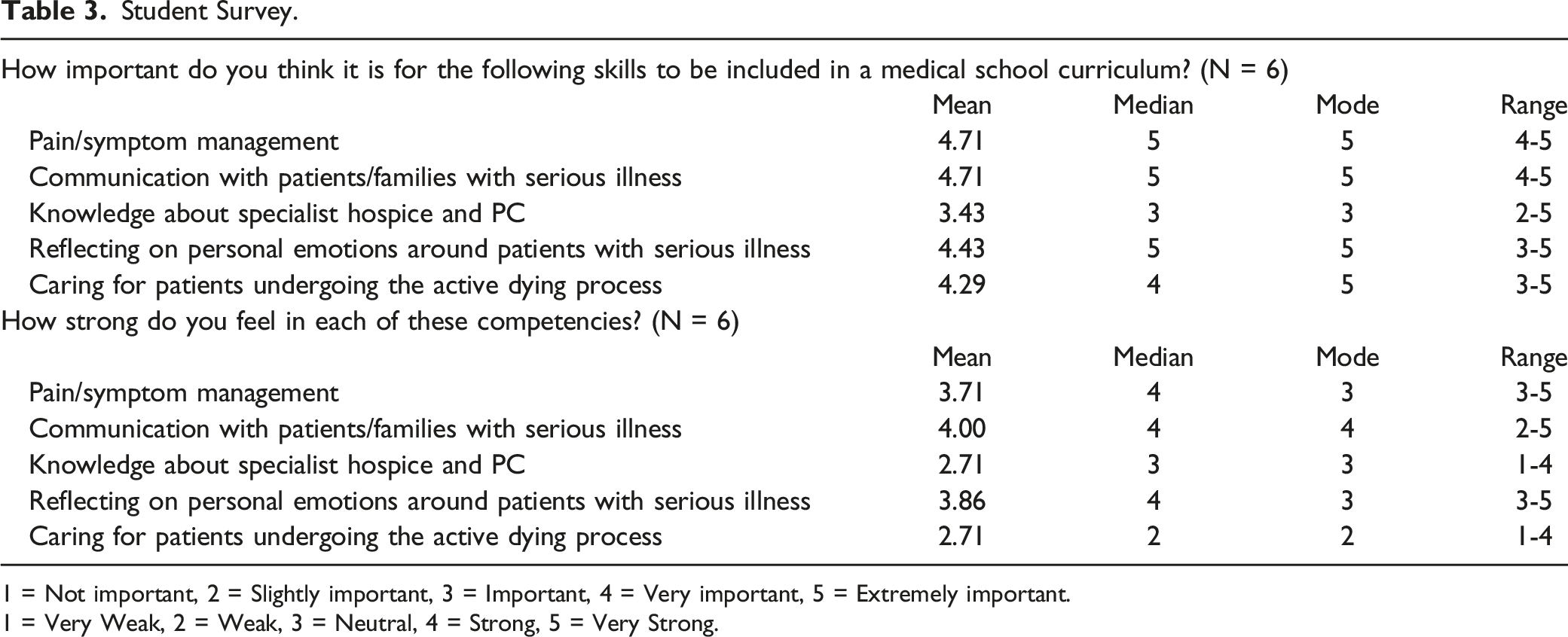
1 = Not important, 2 = Slightly important, 3 = Important, 4 = Very important, 5 = Extremely important.
1 = Very Weak, 2 = Weak, 3 = Neutral, 4 = Strong, 5 = Very Strong.
Context Evaluation Findings
All PSOM stakeholders agreed that communication skill training should be a priority. While some serious illness communication skills training existed, there was no cohesive educational plan with longitudinal integration. Training in pain and symptom management, knowledge of PC and hospice, and mandatory clinical experiences in hospice and palliative medicine with time to debrief these experiences were also identified as curricular needs.
The student survey showed that students considered symptom management and communication with patients and families to be the most critical competencies associated with PC. Knowledge about hospice and PC was considered less important, but students felt relatively weak in their skills in this domain. Students also reported weakness in their ability to care for dying patients, and this was consistent with student reports of lack of exposure to patients near the end of life. Table 2 summarizes these survey results.
We identified many assets and opportunities in the context evaluation dataset, including donor funding which provided for dedicated time for curriculum directors. PSOM had a large network of PC clinical programs with providers who were also skilled educators, and leadership who were supportive of longitudinal PC education. We also identified contextual barriers, such as a need for administrative support and the planned closure of Penn Hospice’s inpatient unit.
While context evaluation tended to validate our own experience of the environment, it elucidated various points. For example, we realized that resources would not allow us to offer a dedicated palliative care clinical rotation; therefore, it was important to provide other opportunities for PC clinical immersion. We also felt empowered to put much of our focus in our ongoing curriculum evaluation on communication skills training, as our stakeholders felt this to be a crucial piece of the curriculum.
Input Evaluation
Input focuses on the implementation and design of interventions based on the environmental context. Our input evaluation questions asked about approaches/strategies to meet curricular goals and key resources.
Input Evaluation Methods
To answer input evaluation questions, we referred to our literature review, 7 interviews with outside curriculum directors and observations of outside programming. Summaries of best practices were collected, and initial curricular design was discussed with PC leadership, content experts and students. Finally, smaller pilots were planned for most parts of the curriculum prior to implementation for all students. Student focus groups and faculty interviews were held after each pilot session to collect feedback along with other data points. For large, single-day teaching interventions, faculty interviews happened directly or soon after the session. For small recurring sessions, faculty group interviews were scheduled once all faculty had a chance to participate. Student focus groups were scheduled in a similar fashion.
Input Evaluation Findings
CARE-7 Core Sessions.
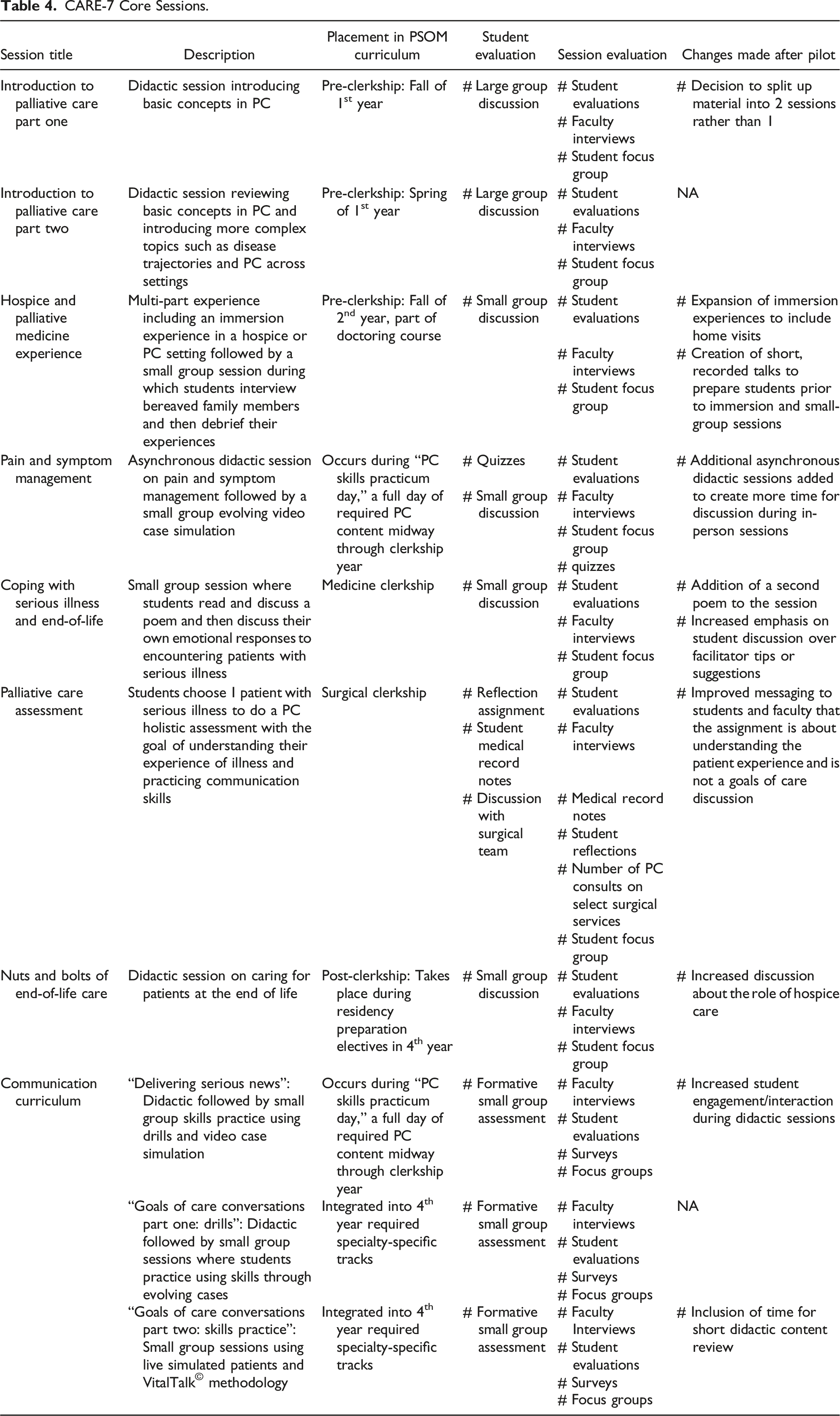
Based on what we learned in the literature review and discussion with outside institutions, we included clinical exposure to patients with PC needs, simulation, and a range of teachers across specialties and disciplines.5,18,25 For communication skills sessions we used methodology from VitalTalk©, a nationally recognized communication skills training program. 26 As other successful curricula have done, 4 we took a step-wise approach to designing the curriculum: pre-clerkship students are introduced to core concepts and skills and exposed to clinical PC; clerkship students then build on these skills by learning more advanced skills and concepts that they are prompted to apply clinically; and post-clerkship students practice advanced skills and have opportunities to pursue additional training through PC clinical electives or a PC area of concentration. CARE-7 coaches mentor students in the PC area of concentration and help teach curricular sessions. Coaches are all faculty members who practice primary palliative care rather than primarily specialist palliative care; this choice was intentional as we were hoping that coaches could model for students the importance of primary palliative care skills regardless of specialty.
Based on our input evaluation we created the following mission statement: “The CARE-7 Curriculum will prepare all medical students, regardless of future specialty, to care for people with serious illness in a multidisciplinary team through simulation and experiential sessions that foster lifelong learning of empathic patient and family-centered communication skills, holistic symptom management and support.” We felt that it was important to include lifelong learning as a principle in our curriculum vision because while students will not be experts in PC skills or topics by the time they graduate, we hope to foster an approach to learning that will help students to continue to develop these skills over their careers.
As with our context evaluation, our input evaluation revealed some unanticipated information. There was variation in expert opinion about the extent to which medical students should be expected to master advanced communication skills such as discussions about goals of care, for example, and whether students should have a mandatory PC rotation. We opted to give students an opportunity to practice having a goals of care conversation. Because our PC and hospice services did not have the bandwidth for a mandatory PC rotation, we created a short early-immersion experience and embedded PC assessment of a patient in an existing clerkship. Furthermore, advice from outside programs that signposting the cohesiveness of a longitudinal curriculum can be difficult led to the creation of a CARE-7 logo.
Process Evaluation
Process evaluation is the observation of how the implementation process is proceeding, noting any areas that diverge from the plan or that require modification. In our process evaluation, we asked if our PC curriculum was being implemented as intended and sought to learn about early indicators of desired outcomes. Given our ambitious roll-out plan, a process evaluation was especially important.
Process Evaluation Methods
A large part of process evaluation focused on faculty interviews, student evaluations and focus groups that took place after session pilots. Detailed notes were taken during these meetings and used in leadership discussions to guide changes for future sessions. One session, called the “PC Assessment,” asks students to perform a comprehensive evaluation of 1 of their patients during Surgical Clerkship and evaluate key PC domains. Students write a note in the medical record, bring pertinent findings back to their team, and write a reflection on their experience. Two CARE-7 team members are currently working on qualitative analysis of electronic medical record (EMR) notes and reflections to identify common themes. At the time of this writing 42 student reflections and EMR notes have been collected and coding is ongoing. A new PC Specialty Interest Group was created in the Fall of 2021, and we are monitoring activity as well as clinical PC elective and area of concentration requests.
Process Evaluation Findings
At the time of this writing 8 out of 10 curricular sessions have been piloted or implemented for all students. Based on the corpus of process evaluation data, curricular sessions have gone as intended and been well-received by students as well as faculty. Reflections and medical record notes show that students are applying knowledge and shifting attitudes in the desired direction. The PC specialty interest group had 7 meetings in its first year and started a program to help hospice patients write a memoir, and multiple students signed up for the PC area of concentration directly after its approval.
All sessions have undergone changes after session pilots (Table 4); changes are tracked and discussed at curriculum director meetings. Some early challenges have included faculty availability to teach sessions and attend faculty development, and logistical hurdles of having pre-clinical medical students spend time in clinical settings.
There are many changes that we made to sessions based on student and faculty input that would have been missed if we had focused on outcomes data alone. For example, we were surprised to learn from students that they valued having evolving video cases to learn communication skills rather than using simulated patient encounters for every session. Another surprise was the interest and engagement of medical students, residents, and fellows in the process of evaluating CARE-7; learners have helped by designing the logo, running focus groups, evaluating reflections and quiz scores and volunteering to help teach sessions. While all planned sessions were given and well-attended, the observation that some students are not able to attend all sessions led to the creation of make-up assignments.
Product Evaluation
Product evaluation refers to the learning outcomes of a curriculum and determines how well it has met the needs of its stakeholders. Our product assessment questions attempt to answer whether sessions are well received, effective in imparting curricular objectives, and to attempt to uncover any un-intended consequences of the curriculum. It also seeks to answer why our curriculum was successful or not in the above measures.
Product Evaluation Methods
Student surveys are being administered at various points in their medical school training to assess student indicators of a lifelong learning approach to communication skill building and to assess the learning environment. Because a growth mindset has been associated with a lifelong learning approach in medical students, surveys include an instrument measuring students’ growth mindset toward communication skills. 27 Yearly student focus groups are planned to assess student’s thoughts about the value of the curriculum, gain insight about their attitudes to learning curricular content, and assess the impact of the hidden curriculum. These yearly focus groups have a broader scope than the pilot-specific focus groups used in process evaluation and will undergo thematic analysis. Bi-annual meetings of PSOM faculty involved in communication skills sessions are planned to ensure integration of CARE-7 communication skills content with other communication skills sessions and to assess the impact of these sessions. Given that 1 of the CARE-7 sessions takes place during the surgical clerkship, palliative care consults to select surgical services will be monitored to assess for any changes to clinical care that might arise. Other tools used in product evaluation are listed in Table 2. Data is collected in a database and qualitative analysis of focus groups and reflections is summarized.
Product Evaluation Findings
At the time of this writing, product evaluation is still in early stages. We are encouraged by initial student enthusiasm for sessions as assessed by session evaluations, focus groups, reflections, and interest in the specialty interest group and area of concentration. Evaluations showed that the “PC Skills Day,” a part of the clerkship year “Practicum Series” was the most highly rated practicum day of the clerkship year. Initial student surveys surrounding communication skills sessions show that students feel sessions create a safe learning environment, and that student indicators of a lifelong learning approach are improved after CARE-7 skills sessions. Quiz scores show that students are learning key concepts. Further data collection as students progress through medical school is needed to understand survey implications and general curricular impact.
Conclusion
Our use of the CIPP model has been invaluable in the process of designing and implementing CARE-7. Because every curriculum will be developed in a context with unique resources, unique barriers and unique stakeholder needs, a one-size-fits-all approach to a PC longitudinal curriculum would be impractical and limiting. No curriculum is a static creation. Ideally, curriculum directors are responsive to the need to change and constantly seek to improve. A successful curriculum will design inputs based upon the context, involve stakeholders in process evaluation and design an outcomes evaluation informed by stakeholder needs. CIPP is a holistic evaluation model that can be applied across contexts and facilitates iterative review of the the curricular processes while paying attention to curricular products.
While longitudinal palliative care curricula are increasingly recognized as critical to medical training, there is a lag in emphasis on robust evaluation to support such curricula. 28 When such curricula are implemented, evaluators often cite prospective program evaluation as a challenge.6,29 To our knowledge, CARE-7 is the first U.S. palliative care UME longitudinal curriculum to describe the use of an evaluation model for prospective program development as well as outcomes assessment. The resulting curriculum is an ambitious program composed of 10 core sessions over 4 years utilizing instructional tools including clinical experiences, various types of simulation, VitalTalk© methodology and interdisciplinary teachers who can role model both primary and specialist palliative care skills.
In our own use of the CIPP framework to evaluate CARE-7 we have identified lessons learned. First, having a curriculum evaluation committee comprised of some members with extensive experience with curriculum evaluation was hugely helpful in guiding our efforts. Next, stakeholder involvement in the process has been helpful both in terms of data collection as well as fostering ongoing stakeholder investment in the project. Finally, we have found that the focus on fostering students primed for lifelong learning has provided further direction to our curriculum evaluation and shaped how we improve upon and evaluate sessions.
In conclusion, the use of a comprehensive program evaluation model such as CIPP can help with the design and implementation of context-specific PC curricula and improve the quality of evaluation. Utilizing the structured approach of the CIPP model allowed us to uncover findings we might not have otherwise and dynamically improve the curriculum, ultimately making the educational experience more relevant and impactful for our students. We look forward to learning more from product evaluation and plan for future scholarship to describe findings in this component of CIPP.
Footnotes
Acknowledgments
The CARE-7 curriculum is generously funded by Barbara M. Jordan, a Penn Medicine Board member and spouse of the late Henry A. Jordan, MD, a Penn alumnus (M’62 from the School of Medicine).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Barbara M. Jordan.