
Abstract
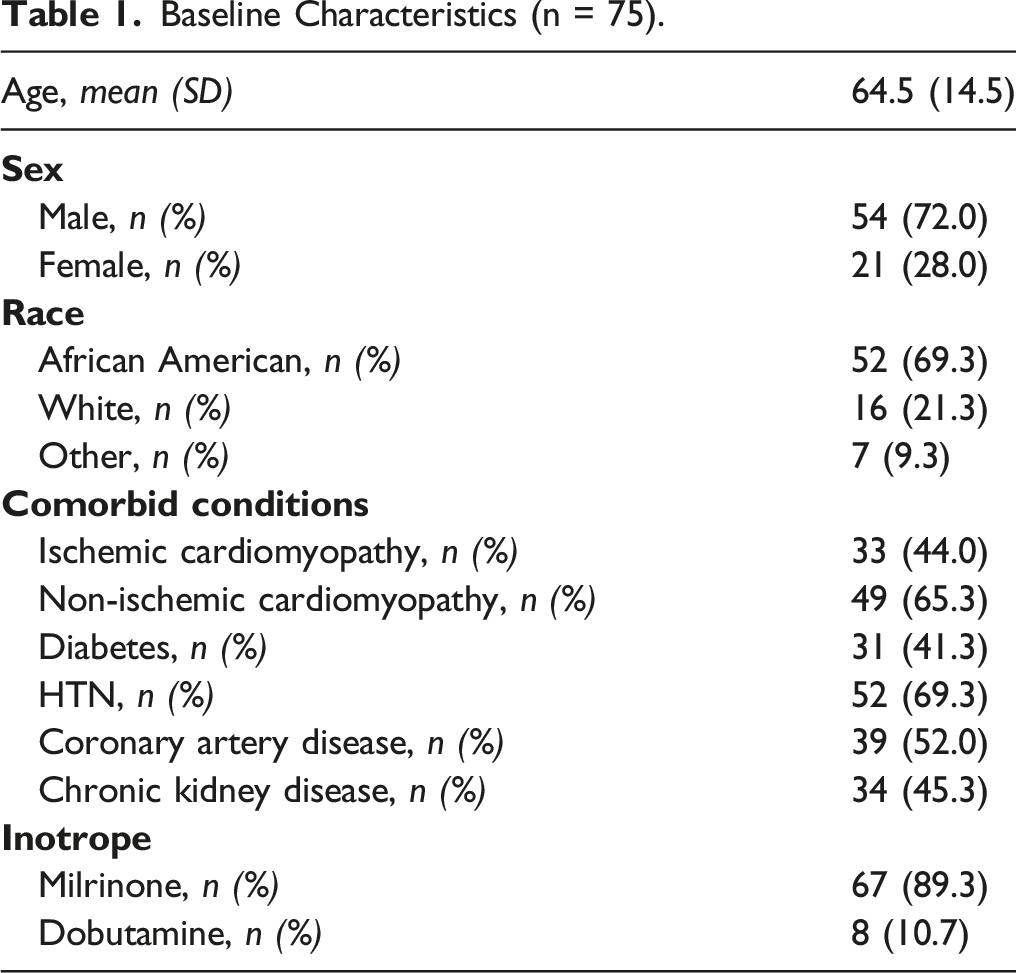
Use of continuous intravenous inotropic support (CIIS) strictly as palliative therapy for patients with ACC/AHA Stage D (end-stage) Heart Failure (HF) has increased significantly. The harms of CIIS therapy may detract from its benefits. To describe benefits (improvement in NYHA functional class) and harms (infection, hospitalization, days-spent-in-hospital) of CIIS as palliative therapy. Methods: Retrospective analysis of patients with end-stage HF initiated on CIIS as palliative therapy at an urban, academic center in the United States between 2014-2016. Clinical outcomes were extracted, and data were analyzed using descriptive statistics. Seventy-five patients, 72% male, 69% African American/Black, with a mean age 64.5 years (SD = 14.5) met study criteria. Mean duration of CIIS was 6.5 months (SD = 7.7). Most patients (69.3%) experienced improvement in NYHA functional class from class IV to class III. Sixty-seven patients (89.3%) were hospitalized during their time on CIIS, with a mean of 2.7 hospitalizations per patient (SD = 3.3). One-third of patients (n = 25) required at least one intensive care unit (ICU) admission while on CIIS therapy. Eleven patients (14.7%) experienced catheter-related blood stream infection. Patients spent an average of 20.6% (SD = 22.8), approximately 40 days, of their time on CIIS admitted to the study institution. Patients on CIIS as palliative therapy report improvement in functional class, survive 6.5 months following initiation, but spend a significant number of days in the hospital. Prospective studies quantifying the symptomatic benefit and the direct and indirect harms of CIIS as palliative therapy are warranted.
Introduction
Heart Failure (HF) is a chronic, progressive disease that affects more than 6.5 million individuals in the United States and is a leading cause of death. 1 The incidence of HF has been rising over the past decade with nearly 1 million new cases of HF diagnosed annually. 2 The prevalence of HF is projected to surpass 8 million Americans by the year 2030. 3 Despite advancements in guideline directed medical and device therapies (GDMDT), some patients progress to end-stage HF (American College of Cardiology/American Heart Association Classification (ACC/AHA) Stage D), which is frequently associated with dyspnea at rest or with minimal exertion, exertional fatigue, and functional deterioration. Management options for patients who have progressed to Stage D HF include Left Ventricular Assist Device (LVAD), Heart Transplantation (HT), and continuous intravenous inotropic support (CIIS) as palliative therapy or as bridge to surgical therapy. 2 The 2022 ACC/AHA HF guidelines provide a Class IIb recommendation for CIIS as palliative therapy (Level of Evidence B), with intention of improving patient’s symptoms, functional status, and quality of life. 4
The use of CIIS as palliative therapy has increased significantly in recent years, with a 44-63% increase in the number of Medicare beneficiaries receiving home inotropes. 5 CIIS has been shown to improve New York Heart Association (NYHA) functional class and health-related quality of life when compared to patients receiving usual HF care.6,7 Though studies examining impact on survival are limited, heterogeneous in their inclusion and exclusion criteria, and of variable design, overall survival is not significantly different for patients on inotropes compared to controls. 6 One important caveat to the survival result reported in the meta-analysis by Nizamic and colleagues is that very few studies on inotropes included patients with a low cardiac output/index.6,8 Patients with a low cardiac output/index and evidence of end-organ dysfunction at outset of consideration of CIIS may experience both a short-term and long-term survival benefit, though this has not been assessed, to date, in a randomized, controlled trial. 8 Moreover, CIIS therapy also carries a risk of complications, such as catheter-related bloodstream infections (CRBSI) and arrythmias.6,9
Among the 4000 patients per year who are treated with CIIS, around two thirds receive CIIS as palliative therapy; the intention of therapy is to palliate symptoms related to end-stage HF, without expectation of life-prolongation or cure.7,10 CIIS may be considered when patients have refractory symptoms (particularly, dyspnea at rest or exertional dyspnea and fatigue) despite maximal palliative therapies such as diuretics, nitrates, opioids, benzodiazepines, and oxygen. 11 Patients on CIIS as palliative therapy have a prognosis of around 6 months, on average, though with a large standard deviation of 6.6 months, suggestive of significant variability in treatment response. 12 Given that most patients are prescribed CIIS as palliative therapy in the last year of life, it is important to understand outcomes of this therapy to inform shared decision making and promote goal concordant care. Palliative care consultation has an established role in supporting patients on CIIS and collaborations between Advanced Heart Failure cardiologists and Palliative Care specialists are growing. 13 The purpose of this study was to examine a cohort of patients receiving CIIS strictly as palliative therapy at a single high-volume center.
Methods
This investigation was conducted with approval from the institutional review board (IRB) from the MedStar Health Research Institute. We conducted a retrospective cohort study of all patients with ACC/AHA Stage D heart failure who were initiated on CIIS as palliative therapy between 2014 and 2016 at an urban, tertiary-care, academic institution. Patients were identified at discharge from their index hospitalization when they were initiated on CIIS. Follow-up data were subsequently gathered by study investigators from the electronic health record. Inclusion criteria included the diagnosis of ACC/AHA Stage D HF, need for inotrope initiation as determined by a HF specialist, and discharge from the hospital with a plan for long-term administration of inotropes. Exclusion criteria included age <18 and patients initiated on CIIS as bridge to left ventricular assist device (LVAD) or orthotopic heart transplant (OHT). Additional descriptions of the methodology used to categorize patients into “palliative” and “bridge” intentions of therapy were published previously. 14
Electronic health record review was performed to collect data on patient demographics, comorbidities, type of inotrope (dobutamine or milrinone), duration of CIIS therapy, change in NYHA functional class at first clinic appointment, typically 2–4 weeks following hospital discharge, and clinical outcomes while on CIIS [eg, implantable cardioverter defibrillator (ICD) shocks, infections, type of infection, hospitalizations, emergency department (ED) visits, intensive care unit (ICU) admissions]. Reasons for inotrope discontinuation included death, worsening clinical status, or improved hemodynamics. One patient remained on CIIS through the end of the study period (8/31/2020).
Data were analyzed using SPSS 28. Descriptive statistics for interval/ratio level data were mean and standard deviation; descriptive statistics for nominal data included frequency distributions and percentages. Some outcomes were converted into 100-person-months as patients were in the study for differing lengths of time. Person-time is an estimate of the actual time a person is at risk for an outcome in a study.
Results
Demographics
Baseline Characteristics (n = 75).
NYHA Functional Class
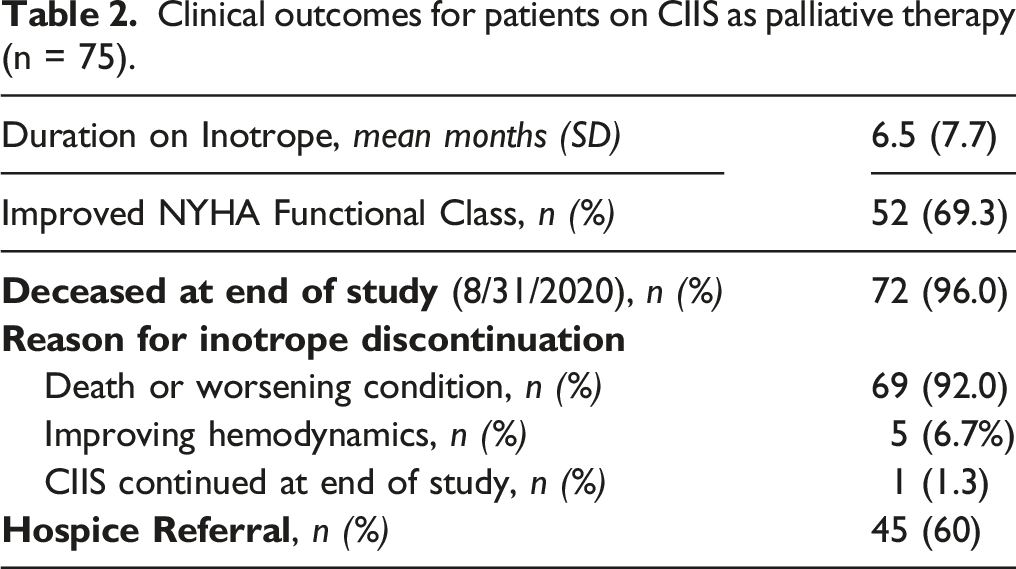
Clinical outcomes for patients on CIIS as palliative therapy (n = 75).
Clinical Outcomes
Patients in this study received CIIS for an average of 6.5 months (SD 7.7) (median 3.3 months, IQR 9.0 months). Nearly all (n = 72; 96%) of the patients who received CIIS as palliative therapy were deceased by the end of the study. Death or worsening clinical condition prompting consideration of hospice was the primary reason for stopping CIIS in 69 (92%) patients. Forty-five (60%) patients were ultimately referred to hospice (Table 2).
CIIS associated harms
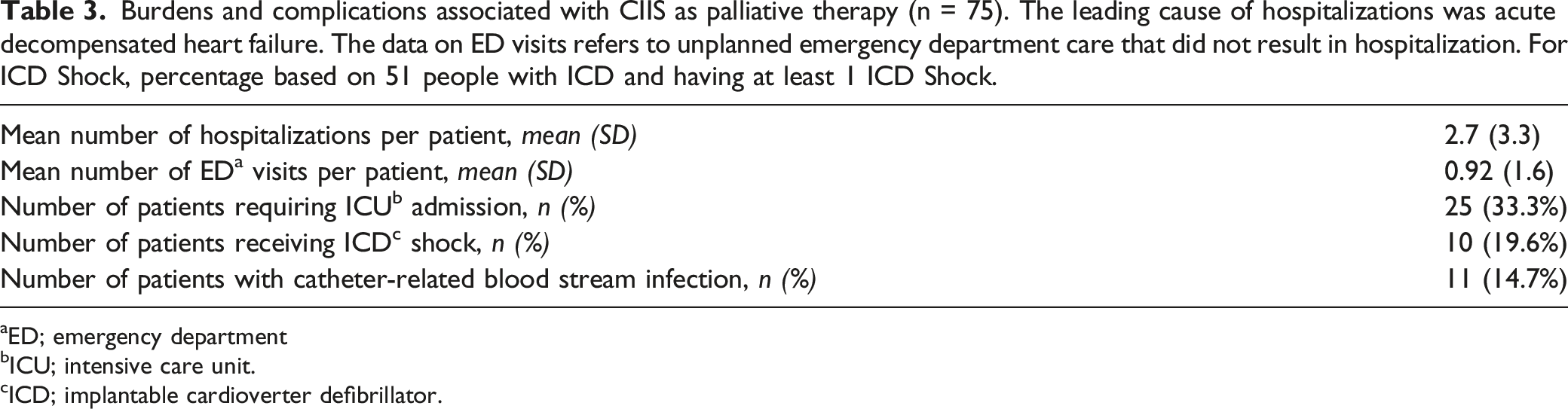
Sixty-seven patients (89.3%) were hospitalized during their time on CIIS, with a mean of 2.7 hospitalizations per patient (SD = 3.3). This equates to a rate of hospitalization of 29.1 per 100-person-months of CIIS therapy. Patients spent an average of 20.6% (SD = 22.8%) of their days on CIIS admitted to the study institution, approximately 40 days per patient. The leading cause of hospitalization was acute decompensated heart failure, affecting 56 patients (74.7%) in the cohort. In addition, patients experienced a mean of 0.92 emergency department (ED) visits that did not result in a hospitalization during their time on CIIS.
Burdens and complications associated with CIIS as palliative therapy (n = 75). The leading cause of hospitalizations was acute decompensated heart failure. The data on ED visits refers to unplanned emergency department care that did not result in hospitalization. For ICD Shock, percentage based on 51 people with ICD and having at least 1 ICD Shock.
aED; emergency department
bICU; intensive care unit.
cICD; implantable cardioverter defibrillator.
Discussion
In this single-center retrospective cohort study of a contemporary cohort of patients with end-stage HF, we demonstrate that the majority of patients on CIIS as palliative therapy experience an improvement in their NYHA functional class with some notable harms that may detract from the quality-of-life improvement afforded by the therapy. The use of CIIS in the management of patients with HF has evolved over time. Initially indicated in patients with chronic HF refractory to standard therapy, the role of CIIS now includes palliative symptomatic relief to improve functional class and quality of life. 15 The increasing use of CIIS as palliative therapy in patients with end-stage HF underscores the need for detailed study of the harms and benefits of CIIS to guide shared decision making with patients and families. To our knowledge, this is the first report of a cohort of patients receiving CIIS for an exclusive palliative indication detailing both the benefits and harms associated with CIIS.
We demonstrate a clinically significant initial improvement in NYHA functional class in our cohort. Few medical options are efficacious for patients who are ineligible for LVAD or OHT and are facing refractory symptoms associated with end-stage HF. Diuretics are the mainstay for managing dyspnea and edema related to end-stage HF. However, end-stage HF is often associated with renal impairment due to cardio-renal syndrome, resulting in progressive diuretic resistance and rendering these medications less effective. 11 Breathlessness is common in these patients and often prompts consideration of low-dose opioid therapy. 16 However, the use of opioid therapy carries its own drawbacks, such as constipation, nausea, drowsiness, dizziness, and a risk of opioid-use disorder. 16 Exertional fatigue related to low cardiac output is yet another distressing symptom that is difficult to ameliorate with standard palliative therapies. In this context, our finding that the majority of patients on CIIS as palliative therapy experienced an improvement in their functional status represents an important and clinically meaningful result, especially considering that this symptomatic benefit is often noted in the last year of life.
While many patients experience improvement in functional class, patients also face harms related to CIIS, such as catheter-related bloodstream infections (CRBSI), and challenges concurrent to CIIS therapy (not necessarily causally linked), such as hospitalizations for acute decompensated heart failure (ADHF) or ICD shocks. Notably, patients in our population spent on average 20.6% (median 16.2%) of their time on inotropes, approximately one in five days, hospitalized at the study institution. This represents an underestimate of their total days out-of-home given we did not collect data on days at rehabilitation or skilled nursing facilities or days admitted to hospitals outside of the study institution. In the absence of a randomized, placebo-controlled trial or a propensity-matched cohort, it is not possible to know how our population of patients on CIIS as palliative therapy would have compared to a similar cohort of patients who were not initiated on CIIS. Nevertheless, the high proportion of days spent out-of-home serves as a notable reminder of the burdens associated with end-stage HF.
In a meta-analysis of 15 studies, the pooled rate of all-cause hospitalization was 22.2 per 100-person-months of follow-up. 6 We find a slightly higher rate of all-cause hospitalization of 29.1 per 100-person-months, which equates to roughly 2 hospitalizations per average patient’s duration on CIIS. The leading cause of rehospitalization in our study was ADHF. Other reasons for hospitalization included catheter-related bloodstream infections (CRBSI) and ICD shocks. We report a similar incidence of ICD shocks as compared to previously published literature. Of the 51 patients with an ICD, 15.7% experienced at least one ICD shock. Given the lack of access to ICD interrogation reports, we were unable to determine the appropriateness of shocks delivered. In a retrospective analysis of 197 patients on CIIS as palliative therapy, Acharya and colleagues 9 report a 17% incidence of ICD shock, 82% of which were appropriate shocks for ventricular tachycardia or ventricular fibrillation, 9% inappropriate shocks, and 9% experienced both appropriate and inappropriate shocks. One third of our patients required admission to the ICU at some point during their treatment course with CIIS, underscoring the significant harms that can accompany CIIS as palliative therapy.
CIIS as palliative therapy is complex and requires consideration of numerous factors. Some patients may not have the social support, insurance coverage, or cognitive function to manage a continuous infusion pump and a central line. Others may have comorbidities that increase harms associated with CIIS (for example, ESRD, advanced malignancy receiving chemotherapy). Patients who present for consideration of CIIS too late in their disease course may have had such deterioration in their functional status that the benefits of CIIS as palliative therapy may be negligible and outweighed by the harms. Regardless of the clinical situation, a firm understanding of the clinical course of patients on CIIS as palliative therapy is necessary to engage in shared decision making with patients and families regarding the pros and cons of this treatment modality. For these reasons, most patients at the study institution who are contemplating CIIS receive an inpatient palliative care consultation. These patients are subsequently followed by outpatient palliative care teams, either in person or by telehealth.
Furthermore, initiation of CIIS as palliative therapy may herald a more medically complex end-of-life (EOL) course for patients with end-stage HF compared to patients who elect to continue GDMDT as tolerated and to transition to hospice care when appropriate. At minimum, patients are living with and managing an indwelling central line and a medication infusion pump. At the study institution, patients on CIIS as palliative therapy have weekly blood work drawn to assess electrolytes and kidney function, though practice patterns may differ at other institutions. Some patients experience catheter-related blood stream infections, which can range from mild to life-threatening, but almost always require acute care hospitalization. Although as a palliative intervention, CIIS appears aligned with hospice philosophy of care, hospice organizations do not consistently enroll patients with end-stage HF who wish to continue receiving CIIS, perhaps due to organizational financial constraints or due to lack of familiarity with the intervention.10,17 Some patients and families feel reluctant to wean CIIS, even when there may no longer be an appreciable symptomatic benefit and there may be escalating harms as patients near EOL. 18 Lastly, weaning off CIIS at the end-of-life results in reversion of the patients’ physiology to their underlying cardiogenic shock state. This may result in a high symptom burden that can best be managed at an acute care hospital or at inpatient hospice, forcing some patients to leave their home in the final days-to-weeks of life. 18 There are regional variations in the use of dobutamine as opposed to milrinone, with higher use in the West than the Northeast. 19 Given the lower cost of dobutamine compared to milrinone, it is possible that certain regions have more hospice agencies that provide CIIS. 15 The contemporary practice of most hospices in the Washington DC metropolitan area is to accept patients once they are weaned off CIIS or with clear intention to wean off CIIS within days-weeks of hospice admission. The patients in our cohort who were referred to hospice (n = 45; 60%) were likely referred towards the end of their treatment course with CIIS. Referral to hospice was likely delayed and length-of-stay in hospice was likely shortened due to these factors. This delicate harm-benefit calculus makes CIIS as palliative therapy an ideal opportunity for shared decision making between patients, families, and specialists from Advanced Heart Failure Cardiology and Palliative Care.
Limitations of this study include a small-retrospective study design with patients from a single center. Compared to previously published studies, our study population represents a more racially diverse population (67.7% African American) than typically presented in patients with HF. There may be heterogeneity in the study population that was not considered in our analysis. For example, we were unable to control the analyses for specific medications patients were on, hemodynamic measurements, or comorbid conditions. Additionally, aside from a subjective assessment of the patient’s NYHA functional class, we were not able to assess the impact of CIIS on health-related quality of life. Future studies on CIIS as palliative therapy should consider serial evaluation of NYHA functional class, quality-of-life indicators, symptom trajectory, and the cost-benefit analysis of the therapy.
Conclusions
Patients and families considering CIIS as palliative therapy must weigh the symptomatic benefit against the harms associated with the therapy, such as risk of infection, ICD shocks, and rehospitalization. We provide some data herein that can inform shared decision-making conversations between patients, families, and their HF and palliative care clinicians. Prospective studies of individual patient experiences are required to understand the benefits and harms of CIIS compared to patients on medical therapies alone.
Footnotes
Acknowledgments
The study authors thank Dr Selma Mohammed and Dr Mark Hofmeyer for their contributions to study design and data acquisition.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.