
Abstract
Heart failure (HF) is a chronic, debilitating condition associated with significant morbidity, mortality, and socioeconomic burden. Patients with end-stage HF (ESHF) who are not a candidate for advanced therapies will continue to progress despite standard medical therapy. Thus, the focus of care shifts from prolonging life to controlling symptoms and improving quality of life through palliative care (PC). Because the condition and prognosis of HF patients evolve and can rapidly deteriorate, it is imperative to begin the discussion on end-of-life (EOL) issues early during HF management. These include the completion of an advance directive, do-not-resuscitate orders, and policies on device therapy and discontinuation as part of advance care planning (ACP). ESHF patients who do not have indications for advanced therapies or those who wish not to have a left ventricular assist device (LVAD) or heart transplant (HT) often experience high symptom burden despite adequate medical management. The proper identification and assessment of symptoms such as pain, dyspnea, nausea, depression, and anxiety are essential to the management of ESHF and may be underdiagnosed and undertreated. Psychological support and spiritual care are also crucial to improving the quality of life during EOL. Caregivers of ESHF patients must also be provided supportive care to prevent compassion fatigue and improve resilience in patient care. In this narrative review, we compare the international guidelines and provide an overview of end-of-life and palliative care for patients with ESHF.
Introduction
Heart failure (HF) is a significant healthcare issue due to its high prevalence, mortality, morbidity, and socioeconomic impact. 1 HF has been identified as a contributing factor for 1 in 9 United States (U.S.) deaths, with its prevalence rising steeply with age.2,3 Owing to the aging U.S. population and the development of life-prolonging therapies, the cost of care for patients with HF is projected to remain significant in the future.4,5 The high informal caregiving cost further aggravates this existing socioeconomic burden due to complex care needs brought by aging and co-morbidities in HF patients. 6 Patients with HF have a similar symptom burden as those with cancer; in advanced stages, the number of symptoms exceeds those associated with advanced cancer, with more frequent depression and spiritual malaise. 7 Although the use of Guideline-directed Medical Therapy (GDMT) has been proven to decrease the progression of the disease and improve quality of life (QOL), patients with advanced disease will continue to progress despite therapy, eventually leading to a prolonged terminal disease state with increased symptom burden and poor QOL. 8 For most patients with advanced HF who do not have indications for LVAD or HT, the focus of the goals of care shifts from life-prolonging therapies to symptom management with the addition of palliative care. 9
Palliative care (PC) includes a patient-centered, multidisciplinary approach while continuing appropriate disease-modifying therapies. 9 Evidence suggests that PC improves QOL in HF patients. The Palliative Care in Heart Failure (PAL-HF) trial – a randomized, controlled study by Rogers et al, revealed that interdisciplinary PC intervention in advanced HF patients showed consistently greater benefits in QOL, anxiety, depression, and spiritual well-being compared with usual care alone. 10 In another randomized clinical study by Bekelman et al, the Care to Alleviate Symptoms and Adjust to Illness (CASA) trial concluded that depression and fatigue, improved with the use of collaborative symptom-focused care. 11 With current evidence, most recent guidelines recommend PC for all subsets of HF patients. Unfortunately, it is reported to be received by only a small fraction of these patients. This problem has been attributed to a number of barriers, including the stigma associated with referring patients to PC, the terminology’s perceived inappropriateness, and the HF patients’ excessively variable and unpredictable prognoses. To address these obstacles, cultural shifts and ongoing physician education are required. 7
This narrative review aims to further discuss the concept and components of PC among HF patients, evaluate its benefits, and provide physicians and other healthcare providers with guidance in providing appropriate care for patients in different stages of HF.
The Concept of End-Of-Life and Palliative Care
Palliative Care in Relation to HF
Components of Palliative Care (Adopted from Heidenreich et al, 2022).

Mamas et al. evaluated whether survival rates among patients with ESHF are better than those with cancer diagnosis. 15 They found out that in men, ESHF (reference group; 5-year survival: 55.8%) had worse mortality outcomes than prostate cancer [hazard ratio (HR) .61, 95% confidence interval (CI) .57-.65; 5-year survival: 68.3%], and bladder cancer (HR .88, 95% CI .81-.96; 5-year survival: 57.3%). In women, ESHF (reference group; 5-year survival: 49.5%) had worse mortality outcomes than breast cancer (HR .55, 95% CI .51-.59; 5-year survival 77.7%). 15 The impact of repeated HF hospitalization on mortality was investigated in a large community population with HF. 16 Setoguchi et al used the Health Care Utilization Database to identify patients who had first hospitalization for HF in British Columbia from 2000-2004. Of 14 374 patients hospitalized for HF, 7401 died during the 24 766 person-years of follow-up with mortality dramatically increased after each HF hospitalization. After adjusting for age, sex, and other confounders, the number of HF hospitalizations was a strong predictor of all-cause death. 16 Advanced HF has a waxing and waning course with relapses and improvements, making management and prognostication extremely challenging. For patients and families, it is much more difficult to comprehend and plan for. For this reason, the ACC and AHA recommend the early engagement of Advanced Care Planning in the care of HF patients.
When to Consider EOL Care
Recommendations for Palliative care, Shared Decision-Making, and End-of-Life in Heart Failure Guidelines.
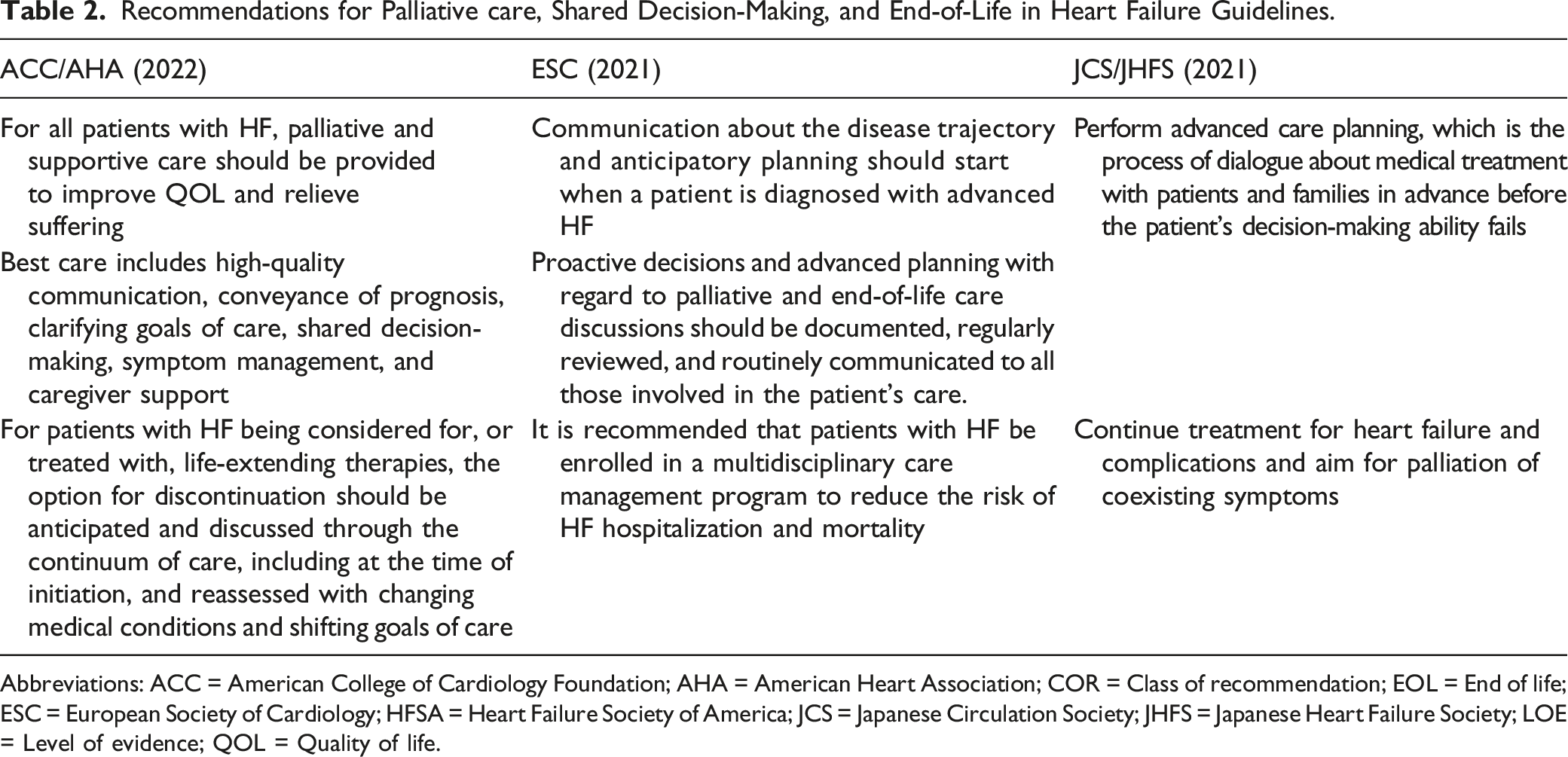
Abbreviations: ACC = American College of Cardiology Foundation; AHA = American Heart Association; COR = Class of recommendation; EOL = End of life; ESC = European Society of Cardiology; HFSA = Heart Failure Society of America; JCS = Japanese Circulation Society; JHFS = Japanese Heart Failure Society; LOE = Level of evidence; QOL = Quality of life.
The declining trajectory of illness in ESHF patients predisposes healthcare providers and family members to determine whether to perform Cardiopulmonary Resuscitation (CPR) in the event of cardiac arrest ahead of time. CPR in ESHF patients poses a prognostic uncertainty, given that CPR generally does not provide a good QOL or a peaceful, dignified death; instead, it prolongs the natural process of dying. 20 Regardless of these bearings, healthcare providers are tasked to discuss CPR with patients and their family members. According to Brunner-La et al, most elderly patients with severe chronic HF valued longevity more than the quality of life, and half wanted to be revived if needed. 21 Furthermore, it was cited that for various cultural, religious, and personal reasons, the symbolic significance of an attempt at CPR might be crucial for certain patients and their families. 22 Hence, EOL for patients with ESHF includes giving personal autonomy and respecting the decision of the patient and their family members regarding CPR, irrespective of the prognosis.
Advance Directives and Care Plan
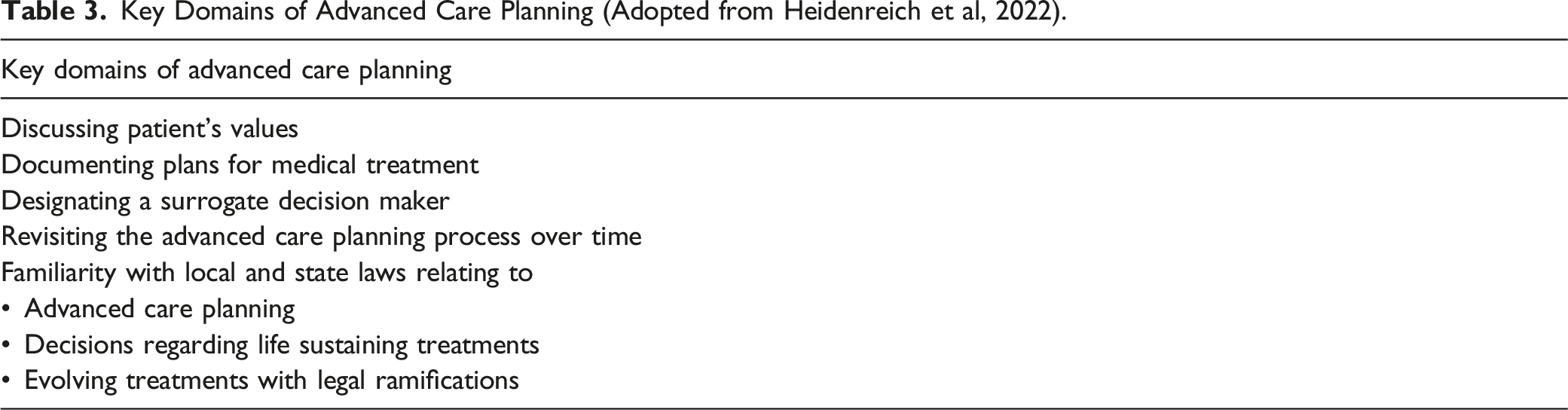
Key Domains of Advanced Care Planning (Adopted from Heidenreich et al, 2022).
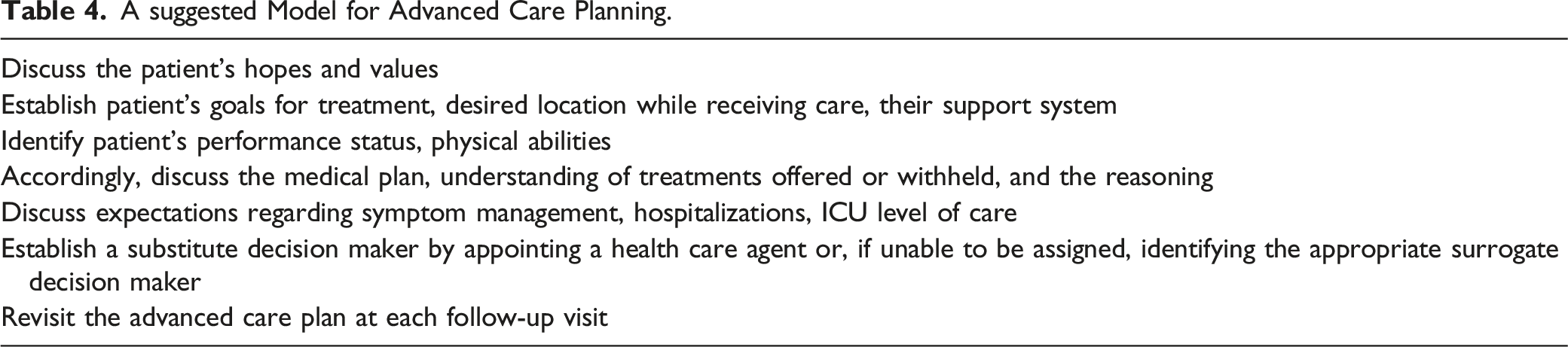
A suggested Model for Advanced Care Planning.
Documentation in Advanced Care Planning.
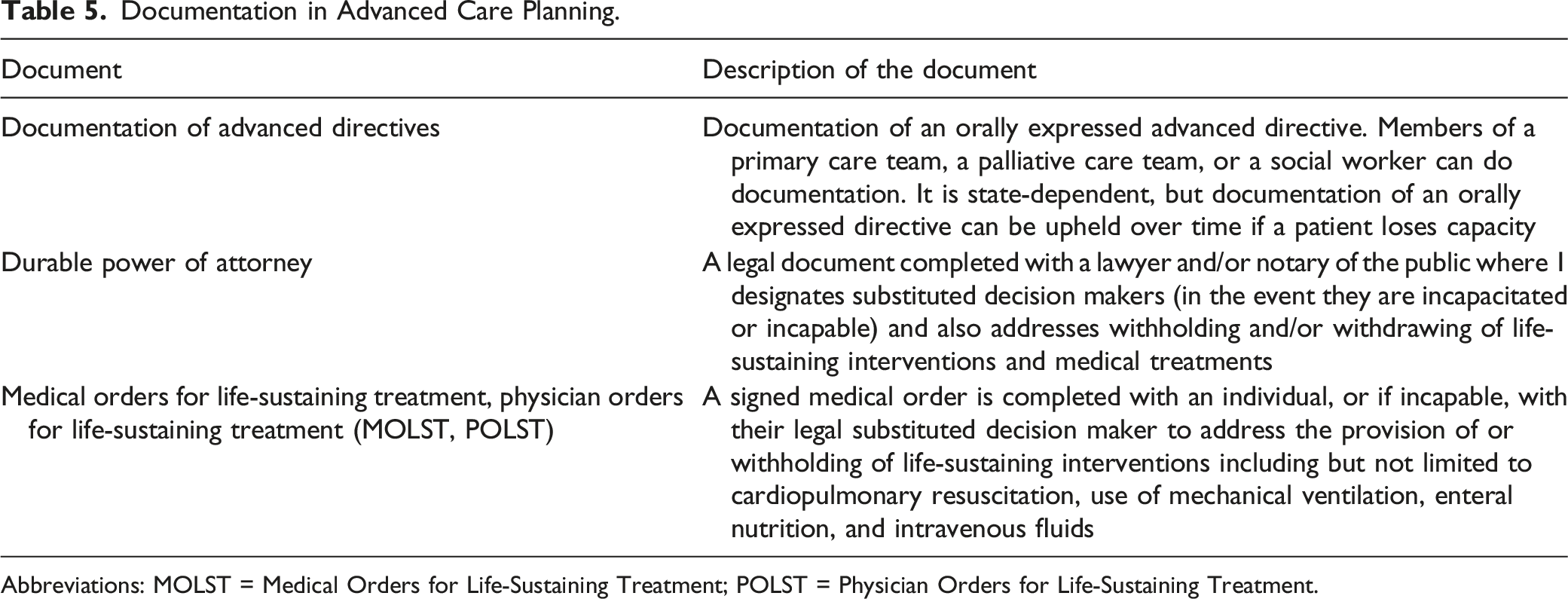
Abbreviations: MOLST = Medical Orders for Life-Sustaining Treatment; POLST = Physician Orders for Life-Sustaining Treatment.
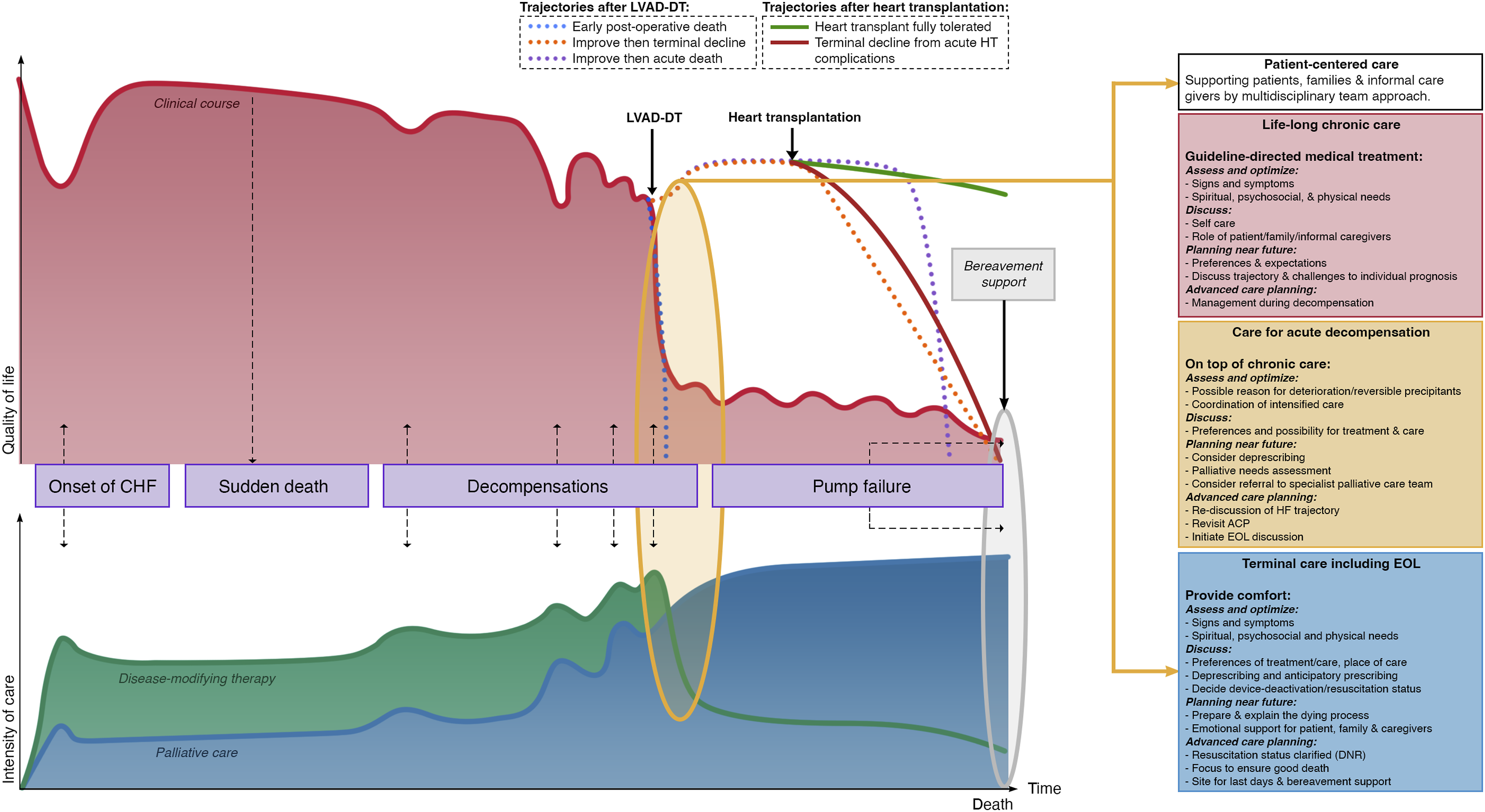
Incorporating palliative and end-of-life care in the course and management of heart failure. The goals are symptom control, quality of life, family support, and caregiver support. Abbreviation: ACP = advanced care planning; CHF = Congestive heart failure; EOL = end-of-life; HT = Heart transplant; LVAD-DT = Left ventricular assist device-device therapy; QOL = Quality of life.
Adjustment of HF Management Plan
As HF progresses, the goals of care may evolve from extending life to controlling symptoms and improving QOL. The role of disease-modifying medications may become less important than other therapies aimed at symptom control. Discontinuation or reduction of these medications should be considered, especially if they cause adverse effects or contribute to impaired quality of life.
17
For instance, medical therapy known to reduce blood pressure can be discontinued in patients with hypotension.
26
Moreover, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers may be discontinued if end-stage patients develop azotemia or worsening renal failure.
27
However, Steinberg (2017) suggested the maintenance and reduction of doses of β-blockers and ACE inhibitors due to their benefits in symptom control and decreasing mortality (Figure 2).
26
Depicts the main presenting symptoms of heart failure patients at the end of life and its proposed mechanisms. Heart failure enters a pro-inflammatory state leading to several pathologic processes, including myopathy and catabolism (with physical deconditioning), responsible for symptoms such as pain and cachexia. The prominent symptom of dyspnea can also be explained by these, but may also be due to associated pulmonary congestion. In totality, patients’ co-morbidities also play a part in the key processes of heart failure symptoms.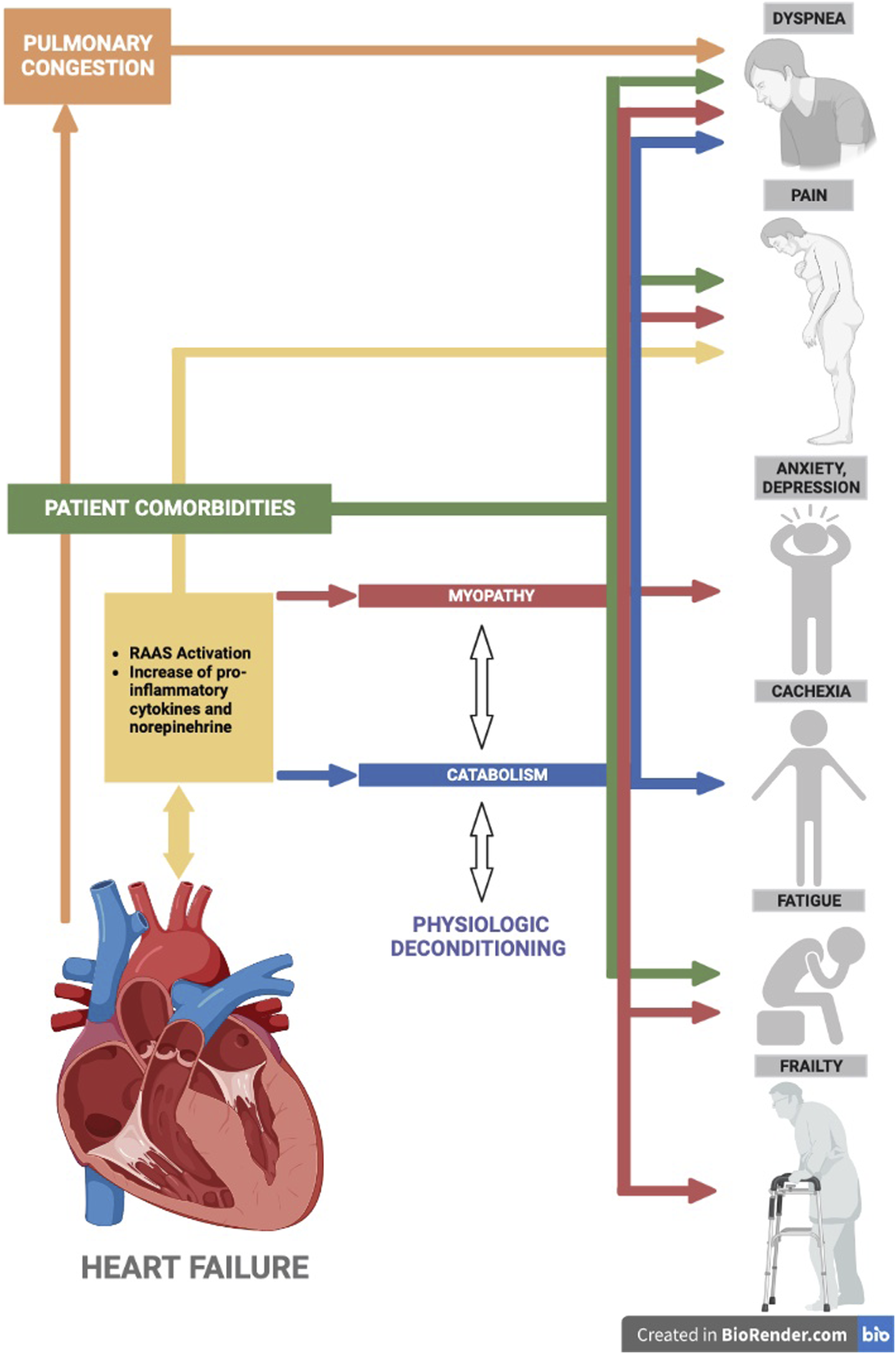
Symptom Assessment and Management
In most clinical settings, patients with ESHF experience a high symptom burden despite receiving adequate medical management. This may be exacerbated by several physiological and psychological factors and is known to progress further as end-of-life approaches. The most experienced symptoms include pain, anxiety, fatigue, shortness of breath, and nausea. Since there is a positive correlation between higher symptom burden and the likelihood of having an adverse event in 1 year, proper identification and assessment of symptoms and their severity are essential in managing patients with ESHF. Common HF symptoms can be assessed and followed using a numeric rating scale, which is simple and easy for patient use. Another useful tool that can provide a more comprehensive assessment includes the Edmonton Symptom Assessment Scale (ESAS). In this self-administered survey, patients are instructed to rate the intensity1-10 of 9 common symptoms they may be experiencing. This scale helps identify some non-classical HF symptoms patients may be experiencing. 28
Pain
Pain is 1 of the most common symptoms of ESHF that contributes to patient suffering. A literature review showed that up to 23-85% of patients with ESHF suffer from pain. 29 Yet it is also known to be frequently unidentified and undertreated for several reasons. 28 It is reported that, more often than not, HF patients fail to recognize the symptoms themselves. 30 Since pain can lower the QOL and bring about many other negative consequences, such as poor medication adherence, depression, and anxiety for patients with ESHF, proper monitoring and management are warranted.
The first step in effectively managing pain includes differentiating the type of pain the patient is experiencing. Physical pain can be subdivided into 2 types, either nociceptive or neuropathic. Based on the analgesic ladder proposed by the World Health Organization, pain should initially be managed using non-opioid analgesics such as nonsteroidal anti-inflammatory drugs (NSAIDs) or acetaminophen. 31 However, long-term use of NSAIDs is contraindicated in patients with ESHF since it can cause further fluid retention, kidney damage, and gastrointestinal bleeding. 27 Opioids are considered when non-opioid medications do not adequately alleviate the patient’s pain. They are also the first line for moderate to severe pain. Opioid medications that are generally considered to be on the safer side effect profile include tramadol, fentanyl, oxycodone, and hydromorphone. 28 Since opioid analgesics are known to cause several side effects, such as constipation, confusion, sedation, and nausea, patients on opioids should be monitored regularly and managed accordingly. 32
Dyspnea
Dyspnea is 1 of the most prevalent symptoms of patients with ESHF, with 85.2% of patients reporting having shortness of breath, 91.1% experiencing it on a constant duration, and 88.6% of patients reporting it to be at the moderate to severe level in terms of symptom severity. 33 Moreover, a significant percentage of patients reported it affecting their QOL. It was also reported that the severity of shortness of breath worsened as the patients approached the end of life, specifically at the last 6 months. 34 Several mechanisms have been proposed to cause dyspnea, the main ones being volume overload and increased left ventricular filling pressures. Awareness, identification of the cause, and direct access to the patient’s HF care team that can provide diuretic adjustments are vital as it helps optimize medical management especially when patient is in fluid overload state necessitating rapid increase in diuresis. As for the use of supplemental oxygen in relieving shortness of breath, there have been inconsistent results as to its effectiveness and reported it to be highly dependent on patient characteristics and hence need to be tailored for each individual. Studies have shown that the feeling of air alleviates dyspnea significantly more than the oxygen itself. 35 Another promising means of rehabilitation for patients with dyspnea, especially those affected by frailty, includes transcutaneous neuromuscular electrical stimulation (NMES). This rehabilitation method has been shown to enhance muscle strength, exercise capacity, and overall health in patients with HF. 36 For intractable dyspnea, low-dose opioids are safe and effective.
Nausea and Vomiting
Intestinal blood flow is known to be reduced in patients with chronic HF. This is associated with several gastrointestinal symptoms, such as nausea, flatulence, and vomiting. 37 Other common causes of nausea include medication side effects, and for patients with renal co-morbidities, uremia can further worsen nausea. These symptoms are known to be at a mild to moderate level of severity in most PC patients but are also frequently undertreated in many. 38 Addressing nausea in patients with HF can be tricky since the commonly used antiemetic medications such as ondansetron, prochlorperazine, or metoclopramide are known to cause QT prolongation. Hence, when used, close monitoring of the QT interval is necessary. Other approaches include removing offending medications, giving agents that do not prolong QT, such as lorazepam, and better management of the cause itself. 28
Fatigue and Frailty
Generalized skeletal muscle wasting in patients with prolonged HF is usually caused by reduced physical activity and metabolic and hormonal derangements that favor a catabolic state that causes cardiac cachexia and protein-calorie malnutrition.28,39 This is 1 of the main reasons behind fatigue in patients with ESHF. Other major causes of fatigue include social and psychological factors such as depressive symptoms and loneliness. 40 Fatigue, despite being a common symptom of HF, is reported to be understudied, and more research is needed to understand its relationship with the causative factors and prognostication. 40 Management of fatigue usually involves behavioral changes that address the underlying cause and good sleep hygiene. When these changes fail to alleviate the symptoms, correcting underlying anemia and giving trazodone or melatonin may be considered. 28
Depression and Anxiety Disorders
In a meta-analysis reported by Moradi et al (2021), the global prevalence of depression among HF patients was 41% and increasing in recent years. It is also reported to be more common in women and countries with low economic income (56.7%). 41 Attributed to the severity of the disease, symptoms, and inability to do activities of daily living, comprehensive screening and prevention programs for ESHF patients are warranted. Regarding pharmacologic therapy, selective serotonin reuptake inhibitors (SSRIs) are the first-line treatment. In the Mood and Mortality in Depressed HF Patients (MOOD-HF) and Sertraline Against Depression and Heart Disease in Chronic Heart Failure (SADHART-CHF) trials, escitalopram and sertraline respectively, led to a significant reduction in depressive symptoms, however no significant difference when compared to placebo. Despite these findings, SSRIs, preferably sertraline, are considered safe to be initiated at low doses and maintained at effective doses. 42
Psychological Support and Spiritual Care
Psychotherapeutic interventions such as cognitive behavioral therapy and family dynamics that are complemented with exercise training programs are shown to enhance cardiac rehabilitation. 43 Moreover, since HF-induced social isolation and depression are reported as independent contributors to adverse HF events, interventions to improve self-care are crucial. Patient empowerment involves patient engagement through self-care. The Motivational Interviewing (MI) to improve self-care in HF patients (MOTIVATE-HF) RCT demonstrated that MI done by trained nurses and caregivers significantly improves self-care maintenance. 44 A Cochrane review (8 studies, 758 total patients, age range 58-79 years) by Poudel et al addresses the positive effect of MI on general self-care behaviors, prevention factors for readmission, QOL, and long-term outcomes related to improved medication adherence. In the mentioned study, MI was performed by any healthcare provider via face-to-face or telephone-based communication. It is well known that PC in the ambulatory setting provides psychosocial support, irrespective of symptom management needs. These patients have better overall survival due to early advanced care planning. 45 Additionally, systematic reviews show that psychosocial support of HF patients is as important an element as that of cancer patients. 46
Symptom Benefit and Discontinuation Effect of Cardiovascular Medications at the End of Life (Adopted from Libby et al. Braunwald’s Heart Disease 12th ed. Elsevier 2021).
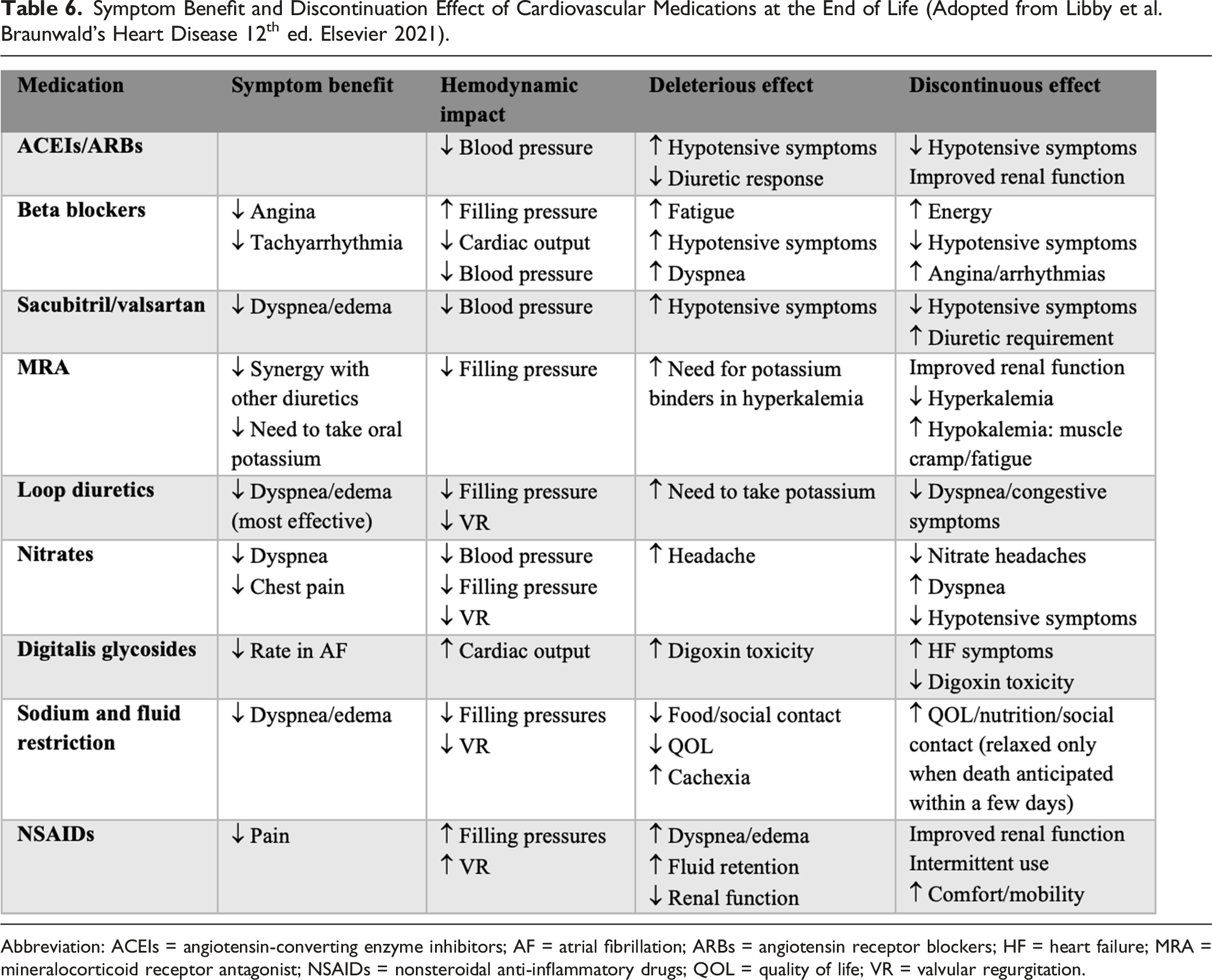
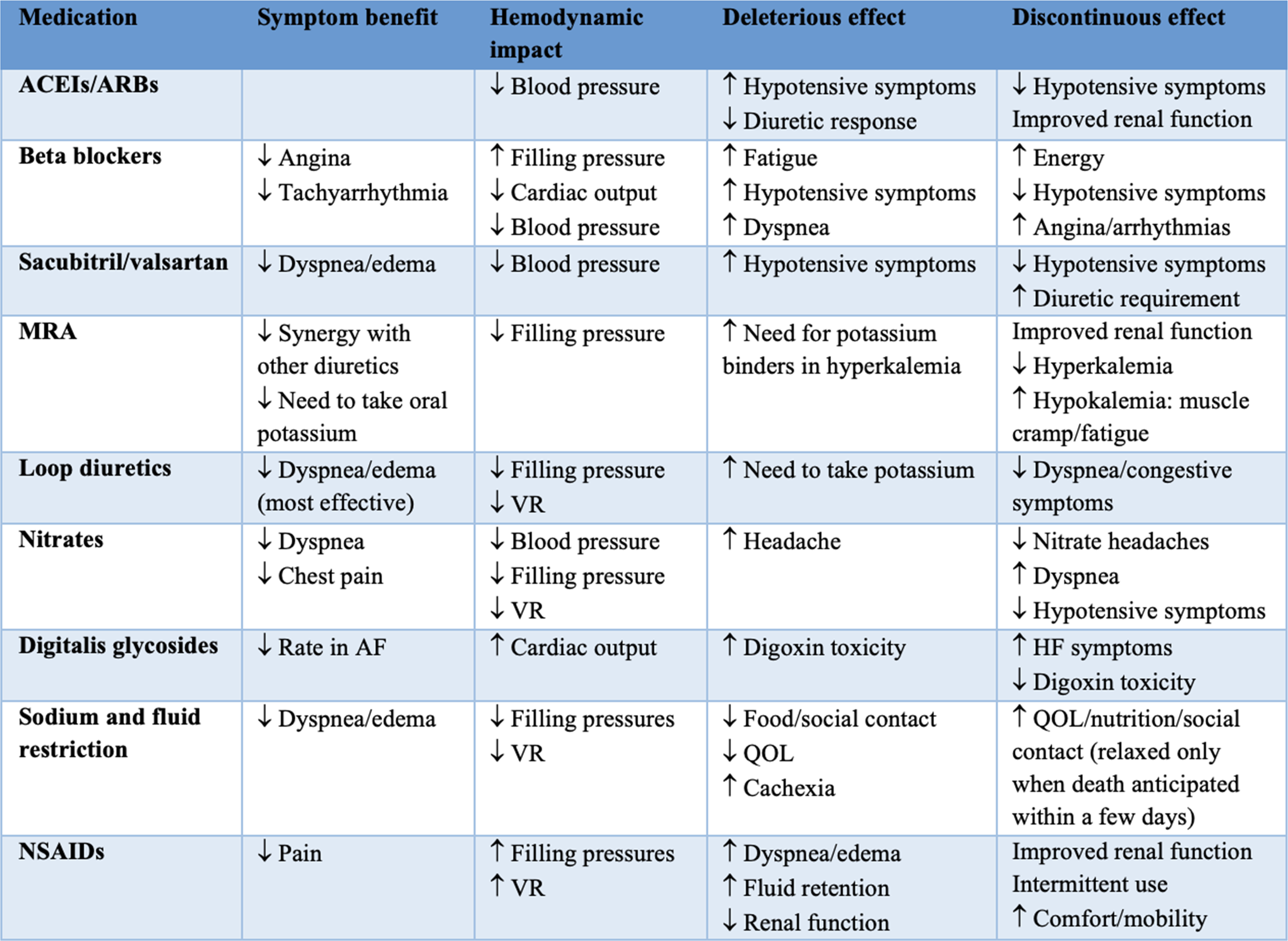
Abbreviation: ACEIs = angiotensin-converting enzyme inhibitors; AF = atrial fibrillation; ARBs = angiotensin receptor blockers; HF = heart failure; MRA = mineralocorticoid receptor antagonist; NSAIDs = nonsteroidal anti-inflammatory drugs; QOL = quality of life; VR = valvular regurgitation.
Caregiver Fatigue
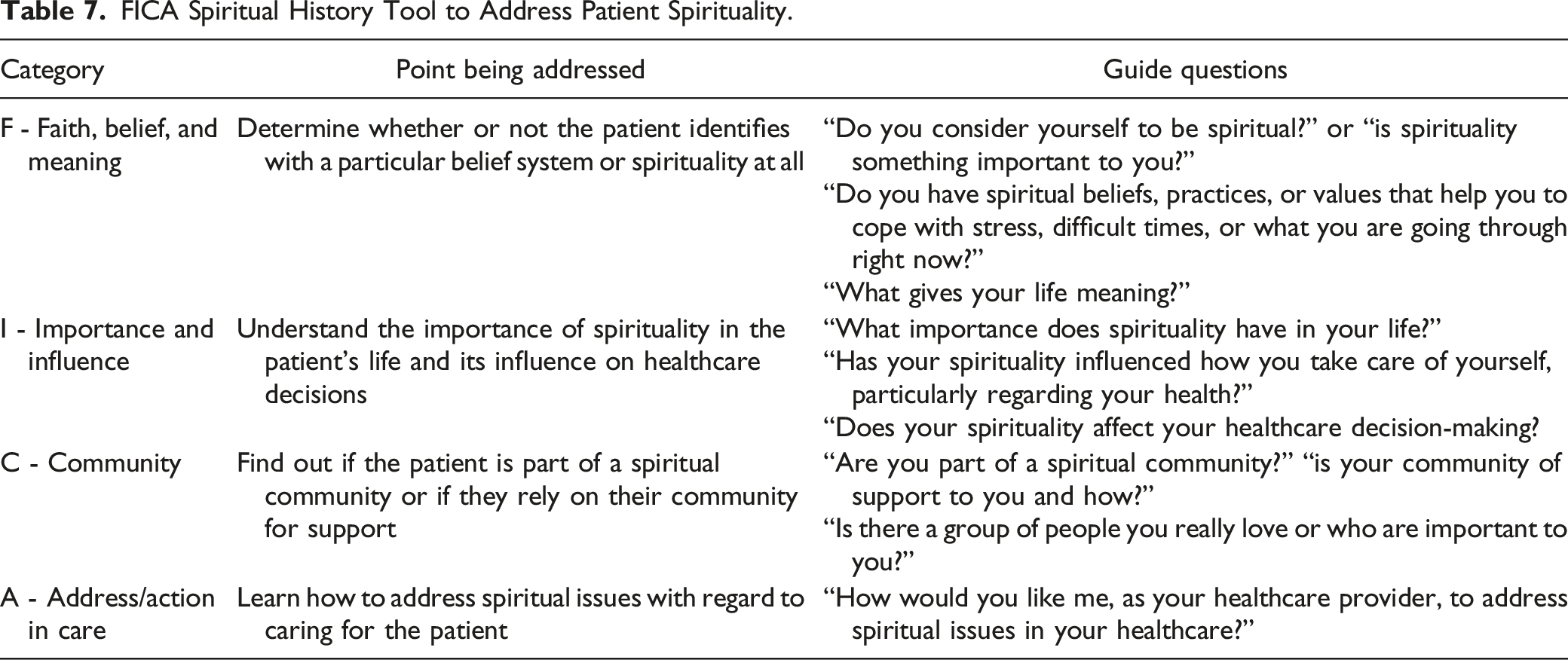
FICA Spiritual History Tool to Address Patient Spirituality.
Special Issues
Implantable Cardioverter Defibrillator
A natural death from cardiac causes characterized by an abrupt loss of consciousness is known as sudden cardiac death. 57 1 of the proven treatments for preventing sudden cardiac death in individuals who are thought to be at high risk for ventricular tachycardia (VT) or ventricular fibrillation (VF), or for those who are resuscitated from prolonged VT/VF is implantable cardioverter-defibrillators (ICDs). 58 According to Pettit et al. (2012), ICDs lower mortality in some chronic heart disease patients, but the prospective benefit is predicted to diminish as HF progresses to the terminal stage. 59 Significant distress due to multiple, frequent, and painful shocks and prolonged pain and death were noted in patients with ESHF; hence, deactivation was recommended as part of EOL care. 22 However, it was noted by Goldstein et al. (2004) that the discussions of deactivating ICDs were not part of the initial advance directives for EOL care but were usually part of the reaction to patient distress nearing EOL. 58 Depending on the knowledge of the procedure and legal and ethical status of ICD deactivation, specialties differ in their experience and comfort with discussions on ICD deactivation. Cardiologists, however, are expected to ensure that the possibility of ICD deactivation is discussed with the patient or surrogate. 60 Currently, there are principles and practice guidelines for ICD deactivation, including a pre-implantation consent and counseling process. A multidisciplinary approach in managing the discussion and decision on ICD deactivation is essential in advance care planning. 61
Left Ventricular Assist Device
Another device treatment used in supporting patients with ESHF and those who are not eligible for a heart transplant (ie, as destination therapy (DT)) is the left ventricular assist device (LVAD). LVADs are said to improve the survival, functional status, and quality of life of patients with ESHF compared to medical therapy. However, stroke, infection, and bleeding are only a few of the serious risks and difficulties associated with LVAD therapy. Given this, another ethical conundrum arises as there are inadequate guidelines for LVAD maintenance and comfort near the EOL. Thus, patients and their families who agree to have DT attend consultations addressing end-of-life preferences, facilitating advance care planning, managing symptoms, and maximizing QOL. 62 This process can also help relieve caregivers of high levels of confusion at EOL care, as seen in the study of McIlvennan et al. 63 When HF is refractory to oral medications, patients who are ineligible for mechanical circulatory support (eg, LVAD) often benefit from continuous cardiac inotrope infusions. Infusions of Milrinone or Dobutamine are used and have been shown to improve quality of life by reducing symptom burden. These infusions are recommended by the AHA/ACC and the Heart Failure Society of America for patients optimized on oral medications with refractory HF as a class IIA indication. 19 Often, these patients are challenged with concurrent hypotension and renal failure and are at elevated risk for arrhythmias. If weaning of inotropes is not successful while hospitalized, these patients may be discharged to the community with ongoing infusions and home-based nursing support from a local hospice agency. 64
Conclusion
ESHF is a chronic illness with limited life expectancy and significant symptom burden. As the patient approaches the EOL, the physician’s role should shift from doing life-prolonging and heroic measures to controlling symptoms and improving QOL. Discussions on EOL and PC should begin early in managing HF, including advanced care planning, hospice referral, device discontinuation, and cardiopulmonary resuscitation discussion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.